

Abstract
Insufficiency fracture occurs when normal or physiological stress applied to weakened bone with demineralization and decreased elastic resistance. Recently, many studies reported the development of IF after radiation therapy (RT) in gynecological cancer, prostate cancer, anal cancer and rectal cancer. The RT-induced insufficiency fracture is a common complication during the follow-up using modern imaging studies. The clinical suspicion and knowledge the characteristic imaging patterns of insufficiency fracture is essential to differentiate it from metastatic bone lesions, because it sometimes cause severe pain, and it may be confused with bone metastasis.
Keywords: Radiation therapy, Adverse effects, Fracture, Stress
Introduction
Insufficiency fracture (IF) is a type of stress fracture, which occurs when normal or physiological stress applied to weakened bone with demineralization and decreased elastic resistance. It is sometimes confused with fatigue fracture, another type of stress fracture, which occurs with abnormal stress on normal bone [1]. The various conditions can weaken bone strength. The osteoporosis is the most frequently associated with IF [2], and the long-term use of steroid or bisphosphonate and rheumatoid arthritis are known to be risk factors for IF [3,4]. Recently, many studies reported the development of IF after radiation therapy (RT) in gynecological cancer [5,6,7,8,9,10,11,12], prostate cancer [13], anal cancer [11], and rectal cancer [11,14,15]. The Surveillance, Epidemiology, and End Results (SEER) data also showed that the RT can substantially increase the risk of fracture [11]. Clinically, the development of IF after RT is sometimes the cause of severe pain, and it may be confused with the bone metastasis during the follow-up in cancer patients.
The purpose of the review is to describe the clinical characteristics of IF and illustrate various imaging features. The pathophysiology and management will be also discussed.
Incidence
The actual incidence of IF after RT is unknown, although it has been regarded as rare complication in the era of megavoltage equipment. The various factors in patients (e.g., the gender, menopausal state, age, body weight, and comorbidity) and treatment parameters (e.g., RT volume, dose per fraction, total dose, RT technique, and the use of chemotherapy) also affect the development of IF, thus RT effect to bone damage cannot be solely evaluated. Nevertheless, recent study showed that RT substantially increases the fracture risk by hazard ratio of 1.65 to 3.16 [11]. In addition, several studies reported the cumulative incidence of IF after RT as 8.2% to 45.2% in cervical cancer [5,6,8,10], 9.0% to 11.2% in rectal cancer [11,14], and 6.8% in prostate cancer [13] (Table 1). The wide use of imaging modalities, such as computed tomography (CT), magnetic resonance imaging (MRI), and bone scintigraphy, during the follow-up may increase detection of the asymptomatic IF. Imaging studies to detect the IF also affect the incidence of IF after RT. One study reported 89% of patients had findings compatible with IF after RT using MRI [16], while another study reported 34% using bone scintigraphy [17].
Table 1.
Recently reported studies for radiation-induced insufficiency fracture
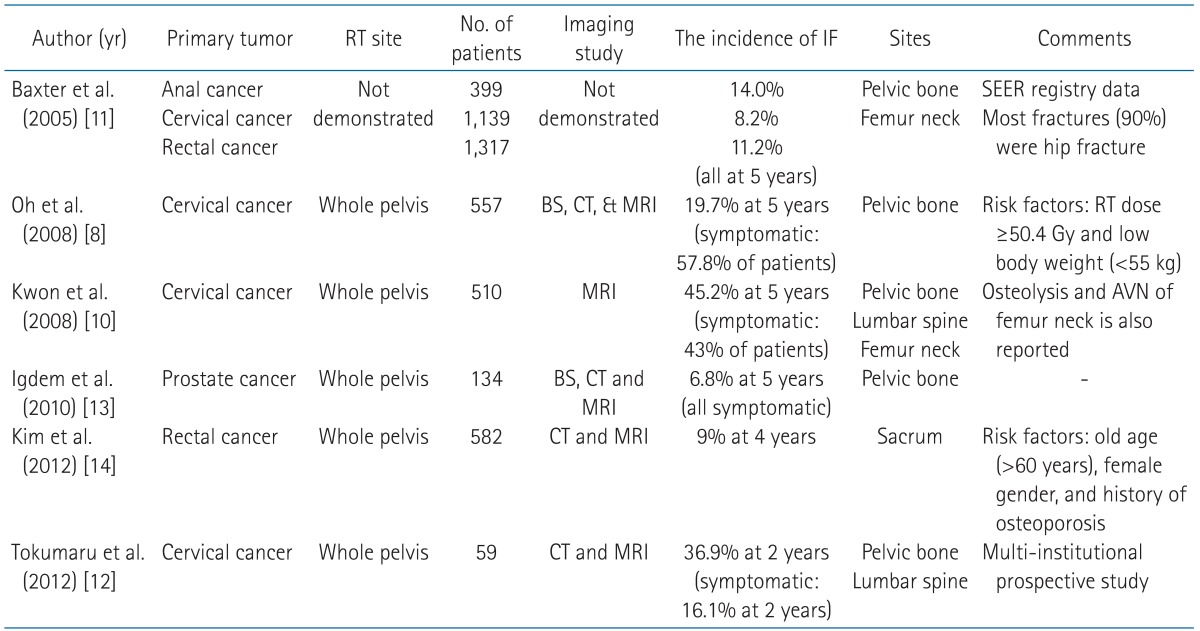
RT, radiation therapy; IF, insufficiency fracture; BS, bone scintigraphy; CT; computed tomography; MRI, magnetic resonance imaging; SEER, The Surveillance, Epidemiology, and End Results; AVN, avascular necrosis.
Clinical Features
The clinical presentation is diverse, from asymptomatic to severe pain which needs hospitalization. Most patients have no or minor trauma history [4,18,19]. On the physical examination, tenderness over the sacral area [19] may be present, but there are generally no specific findings that allow a specific diagnosis to be made [4,18]. The time to development of IF after RT is usually several months but variable ranging from 5 to 44 months [8]. About 50% of patients who were detected by various imaging studies are symptomatic [8,12]. Extent of lesions may correlate with severity of symptoms. A few patients have severe pain and they may be associated with multiple site fractures [8]. Blomlie et al. [16] showed that smaller lesions (<1 cm2) on MRI might be not painful.
IF associated with RT can be developed anywhere within RT field. The sacral fracture by pelvic RT is most frequently reported in the literatures, because the development of IF is associated with weight-bearing. The sacrum, sacroiliac joints, and medial parts of the iliac bones are the major weight-bearing structures of the body. The pubic bone or acetabulum fractures can be accompanied with sacral fracture (Fig. 1), but they rarely present with solitary lesion [8], because initial mechanical fracture of the sacrum usually causes other subsequent other pelvic bone fractures [16,20]. Femur neck or sub-trochanteric fracture is infrequently reported [10,21]. Actually, the vertebral body fracture is the most common clinical presentation of IF associated with osteoporosis, but in association with RT, it is mostly presented with pathologic fracture rather than IF. After pelvic RT, low lumbar spines are often involved (Fig. 2) and non-traumatic vertebral fracture after RT in patients with esophageal cancer was reported [22].
Fig. 1.

Insufficiency fractures in multiple sites in 79-year-old woman who had undergone radiation therapy for cervical carcinoma with stage IIIB 17 months ago. Bone scintigraphy shows increased uptake in both sacral alae and pubic bone (small arrow) and there is fracture in pubic bone on plain X-ray (long arrow) and computed tomography.
Fig. 2.

Insufficiency fracture in low lumbar spine in 49-year-old woman who received pelvic irradiation with extended filed of para-aortic lymph nodes 19 months ago for cervical cancer. Bone scintigraphy shows increased uptake in lower lumbar spines (long arrow) and right sacral alae (short arrow) after radiation therapy.
Pathophysiology
The direct effect of radiation on mature bone is damage to osteoblast cells which result in osteopenia by decrease of collagen production and alkaline phosphatase activity [23,24]. The threshold for these changes is known to be 30 Gy, with cell death occurring at 50 Gy with conventional fractionation [25]. The indirect effect of radiation, generally late effect, is the RT-induced vascular injury [23,24]. These combined radiation effects ultimately result in the structural weakness of the mature bone which is susceptible to stress fracture following a normal or physiological stress (Fig. 3). A tolerance dose (TD5/5-TD50/5) of mature bone is reported as 60-77 Gy for radioosteonecrosis of mandible [26], however, there have been no data for IF.
Fig. 3.

The development of insufficiency fracture.
Risk Factors
The various risk factors of osteoporosis are closely associated with the development of IF, which include low body weight, female gender, current smoking, old age, rheumatoid arthritis, diabetes mellitus, hyperthyroidism, and corticosteroid therapy [3,4,5,6,15,27]. The treatment-related risk factors, such as the higher dose of RT [8,28], pelvic RT technique (the 4-field box vs. the AP/PA parallel opposing technique) [8,12], and the use of chemotherapy [29], were also reported despite these associations have not always been statistically significant.
Imaging Study
1. Plain radiography
Plain radiographs of pelvis, sacrum and lumbar spines showed sclerotic bands, cortical disruptions and fracture lines (Fig. 4), however the subtle changes are not usually seen [4,30] or sometimes an aggressive appearance of bone healing mimicking malignancy may be seen [18].
Fig. 4.

Plain X-ray of pelvic insufficiency fracture: sclerotic changes of sacral alae in 54-year-old woman who had received radiation therapy for cervical carcinoma with stage IVA 6 months ago (A) and in 61-year-old woman who had received radiation therapy for cervical carcinoma with stage IIIA 42 months ago (B).
2. Bone scintigraphy
Bone scintigraphy is sensitive to detect IF. The fractures usually show increased uptake on bone scintigraphy. The typical appearance of pelvic IF is called the butterfly or Honda sign (H-sign), which means the fractures of both sacral alae and sacral body (Fig. 5). The H-sign is often absent. Finiels et al. [4] reported that it was documented in just 40%. Oh et al. [8] also reported that 46.8% of patients who developed IF have unilateral lesions of the sacroiliac joints.
Fig. 5.

Butterfly or H-sign in 57-year-old woman who had received radiation therapy for cervical carcinoma with stage IIA 13 months ago. There are increased uptakes in both sacral alae (long arrow) and sacral body (short arrow) on bone scintigraphy.
3. MRI
MRI is highly sensitive to detect IF with these abnormal marrow changes during the follow-up after RT [16,31]. The irradiated bone has bone marrow changes from the cellular bone components to fat, which shows high signal intensity on T1-weighted images, except an initial reactive marrow changes during the first 2 weeks of RT [32]. When fracture occurs, the diffuse reactive bone marrow changes with fracture line is noted on MRI, which shows reversed signal intensity with low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. Linear areas with this abnormal signal intensity indicate the fracture line. The contrast-enhanced T1-weighted image is sometimes helpful to detect the fracture line (Fig. 6). IF can be diagnosed when these abnormal bone marrow signal with linear fracture line in the typical locations associated with IF. MRI is helpful to distinguish IF from the metastatic bone lesion. MRI is very useful tool to detect the soft-tissue component, thus the absence of focal or discrete mass lesion on MRI around fracture sites is important finding to distinguish it from metastatic bone lesion.
Fig. 6.

Sacral insufficiency fracture on magnetic resonance imaging (MRI) in 57-year-old woman who had received radiation therapy for cervical carcinoma with stage IIB 9 months ago. MRI shows low signal intensity on T1-weighted image (A), high signal intensity on T2-weighted image (B), and fracture line on contrast-enhanced T1-weighted image (C).
4. 18F FDG-PET or PET/CT
18F-fluorodeoxyglucose-positron emission tomography (FDG-PET) has been used as an important imaging tool for the evaluation of patients with cancer, but there have been only a few reports describing the findings of FDG-PET scanning in patients with IF [33,34,35,36]. The FDG-PET shows a variable degree of uptake depending on the stages of fracture (Fig. 7), sometimes it shows prolonged uptake. The standardized uptake value has a trend toward lower in the benign than in malignant lesions [37], but it is not a good indicator of a malignant lesion [36]. Many factors, such as the interval between the PET and the development of a fracture, the age of the patients, the stability of the fracture, and the site of the fracture, are associated with the intensity of FDG uptake [37].
Fig. 7.

FDG-PET findings of insufficiency fracture. (A) In 64-year-old woman who had received concurrent chemoradiotherapy for cervical carcinoma with stage IVA 21 months ago, FDG-PET shows diffuse vertical FDG-uptake (SUVmax = 3.8) in left sacral ala. (B) The FDG-uptake is decreased (SUVmax = 2.0) 6 months later. (C) In 49-year-old woman who had received postoperative radiotherapy for cervical carcinoma with stage IIB 12 months ago, FDG-PET/CT images show increased FDG-uptake in both sacral alae (SUVmax = 2.7). FDG-PET, fluorodeoxyglucose-positron emission tomography; SUVmax, the maximum of standardized uptake values.
Differential Diagnosis and Management
IF can be diagnosed if the radiologic fracture line is present in typical locations and there is no definite soft-tissue lesion indicating the metastatic disease. The clinical suspicion to rule out metastatic disease is important for preventing inappropriate treatment. Biopsy should be avoided for differential diagnosis from metastatic bone lesion, because of the high risk of osteonecrosis and low diagnostic yield [20,38,39]. Furthermore, sometime the histologic findings of the healing bone can mimic malignancy [18].
Most symptomatic patients were fully resolved after conservative treatment using analgesics and rest [5,6,7,8,9,10,13,15,18,19,30], but some patients needs narcotics or hospitalization because of severe pain and disability those who generally have multiple sites of fracture [8] or larger lesions [16]. Pentoxifylline may be effective in recovering symptoms [40]. CT-guided sacroplasty for sacral IF was reported to be helpful in patients with pain resistant to conservative treatment [41].
Conclusion
The RT-induced IF is a common complication during the follow-up using modern imaging study. The clinical suspicion and knowledge the characteristic imaging patterns of IF is essential to differentiate it from metastatic bone lesions, thus avoid inappropriate further management.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA. 1964;187:1001–1004. doi: 10.1001/jama.1964.03060260029006. [DOI] [PubMed] [Google Scholar]
- 2.Cooper KL, Beabout JW, Swee RG. Insufficiency fractures of the sacrum. Radiology. 1985;156:15–20. doi: 10.1148/radiology.156.1.4001403. [DOI] [PubMed] [Google Scholar]
- 3.Peh WC, Gough AK, Sheeran T, Evans NS, Emery P. Pelvic insufficiency fractures in rheumatoid arthritis. Br J Rheumatol. 1993;32:319–324. doi: 10.1093/rheumatology/32.4.319. [DOI] [PubMed] [Google Scholar]
- 4.Finiels H, Finiels PJ, Jacquot JM, Strubel D. Fractures of the sacrum caused by bone insufficiency, meta-analysis of 508 cases. Presse Med. 1997;26:1568–1573. [PubMed] [Google Scholar]
- 5.Ikushima H, Osaki K, Furutani S, et al. Pelvic bone complications following radiation therapy of gynecologic malignancies: clinical evaluation of radiation-induced pelvic insufficiency fractures. Gynecol Oncol. 2006;103:1100–1104. doi: 10.1016/j.ygyno.2006.06.038. [DOI] [PubMed] [Google Scholar]
- 6.Ogino I, Okamoto N, Ono Y, Kitamura T, Nakayama H. Pelvic insufficiency fractures in postmenopausal woman with advanced cervical cancer treated by radiotherapy. Radiother Oncol. 2003;68:61–67. doi: 10.1016/s0167-8140(03)00128-2. [DOI] [PubMed] [Google Scholar]
- 7.Park SH, Kim JC, Lee JE, Park IK. Pelvic insufficiency fracture after radiotherapy in patients with cervical cancer in the era of PET/CT. Radiat Oncol J. 2011;29:269–276. doi: 10.3857/roj.2011.29.4.269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Oh D, Huh SJ, Nam H, et al. Pelvic insufficiency fracture after pelvic radiotherapy for cervical cancer: analysis of risk factors. Int J Radiat Oncol Biol Phys. 2008;70:1183–1188. doi: 10.1016/j.ijrobp.2007.08.005. [DOI] [PubMed] [Google Scholar]
- 9.Uezono H, Tsujino K, Moriki K, et al. Pelvic insufficiency fracture after definitive radiotherapy for uterine cervical cancer: retrospective analysis of risk factors. J Radiat Res. 2013;54:1102–1109. doi: 10.1093/jrr/rrt055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kwon JW, Huh SJ, Yoon YC, et al. Pelvic bone complications after radiation therapy of uterine cervical cancer: evaluation with MRI. AJR Am J Roentgenol. 2008;191:987–994. doi: 10.2214/AJR.07.3634. [DOI] [PubMed] [Google Scholar]
- 11.Baxter NN, Habermann EB, Tepper JE, Durham SB, Virnig BA. Risk of pelvic fractures in older women following pelvic irradiation. JAMA. 2005;294:2587–2593. doi: 10.1001/jama.294.20.2587. [DOI] [PubMed] [Google Scholar]
- 12.Tokumaru S, Toita T, Oguchi M, et al. Insufficiency fractures after pelvic radiation therapy for uterine cervical cancer: an analysis of subjects in a prospective multi-institutional trial, and cooperative study of the Japan Radiation Oncology Group (JAROG) and Japanese Radiation Oncology Study Group (JROSG) Int J Radiat Oncol Biol Phys. 2012;84:e195–e200. doi: 10.1016/j.ijrobp.2012.03.042. [DOI] [PubMed] [Google Scholar]
- 13.Igdem S, Alco G, Ercan T, et al. Insufficiency fractures after pelvic radiotherapy in patients with prostate cancer. Int J Radiat Oncol Biol Phys. 2010;77:818–823. doi: 10.1016/j.ijrobp.2009.05.059. [DOI] [PubMed] [Google Scholar]
- 14.Kim HJ, Boland PJ, Meredith DS, et al. Fractures of the sacrum after chemoradiation for rectal carcinoma: incidence, risk factors, and radiographic evaluation. Int J Radiat Oncol Biol Phys. 2012;84:694–699. doi: 10.1016/j.ijrobp.2012.01.021. [DOI] [PubMed] [Google Scholar]
- 15.Herman MP, Kopetz S, Bhosale PR, et al. Sacral insufficiency fractures after preoperative chemoradiation for rectal cancer: incidence, risk factors, and clinical course. Int J Radiat Oncol Biol Phys. 2009;74:818–823. doi: 10.1016/j.ijrobp.2008.08.054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Blomlie V, Rofstad EK, Talle K, Sundfor K, Winderen M, Lien HH. Incidence of radiation-induced insufficiency fractures of the female pelvis: evaluation with MR imaging. AJR Am J Roentgenol. 1996;167:1205–1210. doi: 10.2214/ajr.167.5.8911181. [DOI] [PubMed] [Google Scholar]
- 17.Abe H, Nakamura M, Takahashi S, Maruoka S, Ogawa Y, Sakamoto K. Radiation-induced insufficiency fractures of the pelvis: evaluation with 99mTc-methylene diphosphonate scintigraphy. AJR Am J Roentgenol. 1992;158:599–602. doi: 10.2214/ajr.158.3.1739002. [DOI] [PubMed] [Google Scholar]
- 18.Peh WC, Khong PL, Yin Y, et al. Imaging of pelvic insufficiency fractures. Radiographics. 1996;16:335–348. doi: 10.1148/radiographics.16.2.8966291. [DOI] [PubMed] [Google Scholar]
- 19.Lin J, Lachmann E, Nagler W. Sacral insufficiency fractures: a report of two cases and a review of the literature. J Womens Health Gend Based Med. 2001;10:699–705. doi: 10.1089/15246090152563588. [DOI] [PubMed] [Google Scholar]
- 20.De Smet AA, Neff JR. Pubic and sacral insufficiency fractures: clinical course and radiologic findings. AJR Am J Roentgenol. 1985;145:601–606. doi: 10.2214/ajr.145.3.601. [DOI] [PubMed] [Google Scholar]
- 21.Epps HR, Brinker MR, O'Connor DP. Bilateral femoral neck fractures after pelvic irradiation. Am J Orthop (Belle Mead NJ) 2004;33:457–460. [PubMed] [Google Scholar]
- 22.McKean H, Miller RC, Jatoi A. Non-traumatic vertebral fractures in patients with locally advanced esophageal cancer: a previously unreported, unrecognized problem. Dis Esophagus. 2007;20:102–106. doi: 10.1111/j.1442-2050.2007.00645.x. [DOI] [PubMed] [Google Scholar]
- 23.Howland WJ, Loeffler RK, Starchman DE, Johnson RG. Postirradiation atrophic changes of bone and related complications. Radiology. 1975;117(3 Pt 1):677–685. doi: 10.1148/117.3.677. [DOI] [PubMed] [Google Scholar]
- 24.Hopewell JW. Radiation-therapy effects on bone density. Med Pediatr Oncol. 2003;41:208–211. doi: 10.1002/mpo.10338. [DOI] [PubMed] [Google Scholar]
- 25.Williams HJ, Davies AM. The effect of X-rays on bone: a pictorial review. Eur Radiol. 2006;16:619–633. doi: 10.1007/s00330-005-0010-7. [DOI] [PubMed] [Google Scholar]
- 26.Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys. 1991;21:109–122. doi: 10.1016/0360-3016(91)90171-y. [DOI] [PubMed] [Google Scholar]
- 27.Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med. 1998;338:736–746. doi: 10.1056/NEJM199803123381107. [DOI] [PubMed] [Google Scholar]
- 28.Fu AL, Greven KM, Maruyama Y. Radiation osteitis and insufficiency fractures after pelvic irradiation for gynecologic malignancies. Am J Clin Oncol. 1994;17:248–254. doi: 10.1097/00000421-199406000-00015. [DOI] [PubMed] [Google Scholar]
- 29.Jenkins PJ, Montefiore DJ, Arnott SJ. Hip complications following chemoradiotherapy. Clin Oncol (R Coll Radiol) 1995;7:123–126. doi: 10.1016/s0936-6555(05)80815-5. [DOI] [PubMed] [Google Scholar]
- 30.Newhouse KE, el-Khoury GY, Buckwalter JA. Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am. 1992;74:1472–1477. [PubMed] [Google Scholar]
- 31.Mammone JF, Schweitzer ME. MRI of occult sacral insufficiency fractures following radiotherapy. Skeletal Radiol. 1995;24:101–104. doi: 10.1007/BF00198070. [DOI] [PubMed] [Google Scholar]
- 32.Stevens SK, Moore SG, Kaplan ID. Early and late bone-marrow changes after irradiation: MR evaluation. AJR Am J Roentgenol. 1990;154:745–750. doi: 10.2214/ajr.154.4.2107669. [DOI] [PubMed] [Google Scholar]
- 33.Fayad LM, Cohade C, Wahl RL, Fishman EK. Sacral fractures: a potential pitfall of FDG positron emission tomography. AJR Am J Roentgenol. 2003;181:1239–1243. doi: 10.2214/ajr.181.5.1811239. [DOI] [PubMed] [Google Scholar]
- 34.Ravenel JG, Gordon LL, Pope TL, Reed CE. FDG-PET uptake in occult acute pelvic fracture. Skeletal Radiol. 2004;33:99–101. doi: 10.1007/s00256-003-0711-4. [DOI] [PubMed] [Google Scholar]
- 35.Tsuchida T, Kosaka N, Sugimoto K, Itoh H. Sacral insufficiency fracture detected by FDG-PET/CT: report of 2 cases. Ann Nucl Med. 2006;20:445–448. doi: 10.1007/BF03027382. [DOI] [PubMed] [Google Scholar]
- 36.Oh D, Huh SJ, Lee SJ, Kwon JW. Variation in FDG uptake on PET in patients with radiation-induced pelvic insufficiency fractures: a review of 10 cases. Ann Nucl Med. 2009;23:511–516. doi: 10.1007/s12149-009-0267-z. [DOI] [PubMed] [Google Scholar]
- 37.Kato K, Aoki J, Endo K. Utility of FDG-PET in differential diagnosis of benign and malignant fractures in acute to subacute phase. Ann Nucl Med. 2003;17:41–46. doi: 10.1007/BF02988257. [DOI] [PubMed] [Google Scholar]
- 38.Casey D, Mirra J, Staple TW. Parasymphyseal insufficiency fractures of the os pubis. AJR Am J Roentgenol. 1984;142:581–586. doi: 10.2214/ajr.142.3.581. [DOI] [PubMed] [Google Scholar]
- 39.Hall FM, Goldberg RP, Kasdon EJ, Glick H. Post-traumatic osteolysis of the pubic bone simulating a malignant lesion. J Bone Joint Surg Am. 1984;66:121–126. [PubMed] [Google Scholar]
- 40.Base NS, Ozguroglu M, Kamberoglu K, Karahasanoglu T, Ober A. Pentoxifylline in the treatment of radiation-related pelvic insufficiency fractures of bone. Radiat Med. 2003;21:223–227. [PubMed] [Google Scholar]
- 41.Heron J, Connell DA, James SL. CT-guided sacroplasty for the treatment of sacral insufficiency fractures. Clin Radiol. 2007;62:1094–1103. doi: 10.1016/j.crad.2007.04.017. [DOI] [PubMed] [Google Scholar]