

Abstract
Background:
A common type of Humerus fractures is about proximal. This study aimed to compare the results of surgical and non-surgical methods in treatment the Fracture of Proximal Humerus for decisions based on high-performance and less side effect.
Materials and Methods:
This prospective clinical trial study was done on 114 patients 30-80 years old with proximal humerus fracture referred to the Isfahan hospital universities (Ayatollah Kashani and Al Zahra hospitals) in 2007-2012. They were divided into two groups of 57 and treated surgically or non-surgically. The self provided questionnaires were used to assess the consequences of the side effects. The patients returned for trial check up during 6 weeks, 3 months, 6 months and one year after intervention.
Result:
In two parts fracture with displacement, nonsurgical treatment had lead to more complications rather than surgical treatment. In three-parts fracture non-union was seen in nonsurgical method in 6 weeks and in surgical method in 3, 6 months and one year after treatment, malunion was seen more in nonsurgical method rather than surgical method. In four-part fracture none-union results was seen more in nonsurgical method in 6 weeks, 3 months and one year and in surgical method in 6 months after treatment, mal union was seen more in nonsurgical method rather than surgical method.
Conclusion:
The surgery in three and four parts fractures had fewer complications in the patients under 50 but not in the elders.
Keywords: Closed reduction, fracture of proximal humerus, internal fixation, open reduction
INTRODUCTION
Humerus proximal fracture is the most common type of Humerus fractures. These types of fractures contain 4 to 5% of the total fractures.[1]
The ratio of this type of fracture is two in females but one in males. It is going to be increased in the elders and it is uncommon in less than 40 years old people. There are many differences between age and gender in the incidence. In ¾ of the cases, the fracture happens in non dominant Humerus.[2,3]
The treatment of this lesion depends on the conditions like the patient's age, degree of fracture displacement, the amount of damage to the soft tissue, last systematic diseases; fractured bone resulted of pathology, degree of bone damages and experience of surgeon. It might be chosen from surgical or nonsurgical treatment.[2,3,4,5] Surgical treatment causes more side effects and complications like nonunion, delayed union, neurovascular problems, osteo necrosis, joints stiffness, arthritis, infection, loss of fixation, decreasing of ROM. In opposite nonsurgical methods have been associated with less problems, in some circumstances the outcomes is not reliable.[2]
Although different indications for different types of treatment choices are represented, choosing the intervention type is challenging all the time.
This study have been compared the surgical and non-surgical methods of treatment in proximal Humerus fractures. The result of this study based on the objective outcomes can be helpful for surgeons to choose the best way with less complication.
MATERIALS AND METHODS
This study was based on prospective clinical trial, observational - Cohort studying.
Totally 114 subjects had been chosen from the patients with proximal Humerus Fracture referred to the hospital universities in Isfahan (Ayatollah Kashani and Al Zahra hospitals) during 2007-2012. They were at first divided into two groups based on treatment method (57 with surgical and 57 with non surgical) with the age range of 30-80 years old.
These patients were similarized and uniformed as per the age, gender, underline diseases, and 2, 3, 4 parts fractures. The patients with Pathologic fractures proceeds because of any reasons like metastasis, underline diseases, tumor and infection, death during surgery or in 6 months later, disable to be followed for any reason like unavailability or not referring for check up, non complete information registered by surgeon, last Humerus surgery, Humerus proximal fracture with dislocation were excluded and finally the patients in each group were divided in 3 subgroups of 19 members based on the 2, 3, 4 parts fractures. They have been analyzed with the results of surgical or nonsurgical methods of treatments [Figure 1].
Figure 1.
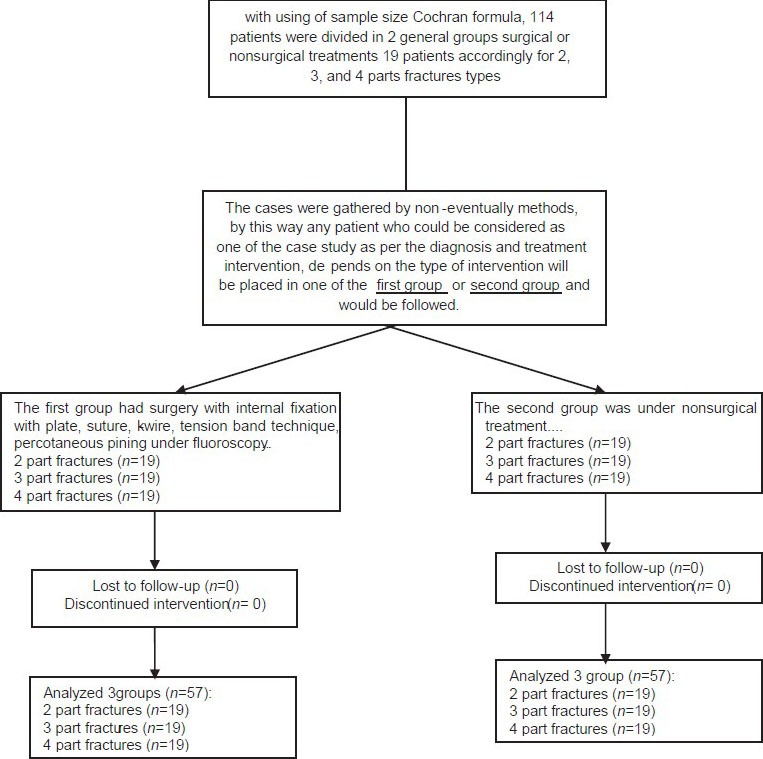
The Consort Flowchart
The cases were gathered by non-eventually methods, by this way; any patient could be considered as one of the case study as per the diagnosis and treatment intervention. Depending on the type of intervention; and each one placed in one of the first group or second group and was followed.
The first group had surgery with internal fixation with plate, suture, k-wire, tension band technique, percotaneous pining under fluoroscopy. In this method the patients were ruled under general anesthesia or local supraclavicular anesthesia after preoperational procedures, then operation has been done by 1- delto pectoral 2- deltoid splitting 3- posterior, then internal fixation was fixed, irrigation has been done and then hemovac drain was placed and layer by layer suture was done and the operation place was reformed.
The second group was under nonsurgical treatment; in this method the Humerus was splinted by sling and swath or velpeau bandage and caused the better union by bone un-movement which resulted in better union.
Since we had considered the fractures in three groups of two, three, and four-parts fractures, with using the Cochran sample size formula 114 patients were divided in two general groups of surgical or nonsurgical treatments with three subgroups of 19 patients based on 2, 3, and 4 parts fractures types. For ensuring of matching, it has been tried to choose the patients in the same range of sex and age for each group.
After completing the cases for each group the Confounding Factors were reviewed. The complications check list was completed through examination according to the schedule (6 weeks, 3 month, 6 months and one year) by a resident cooperated in the project and under the related professor supervision. Occurrence of each side effect was considered as a complication during one year of intervention.
Finally the data were gathered and analyzed in order to compare the surgical and nonsurgical treatments outcomes for Humerus proximal fracture in SPSS software (version 17), with fisher exact test, Chi-square test, independent sample T test (P < 0.05).
This clinical trial study has been registered in WWW.IRCT.IR with the code of IRCT 2013052313435N1.
RESULT
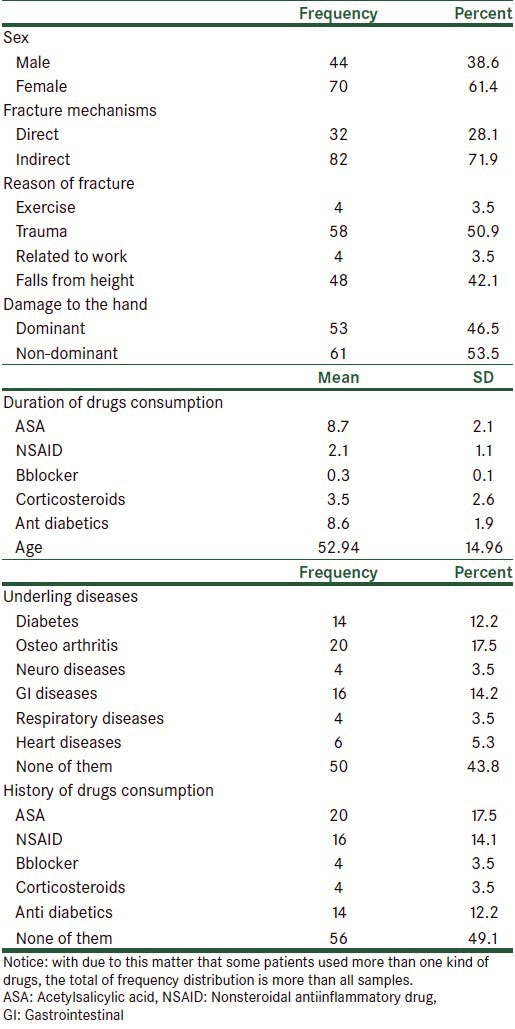
The studied population was consisted of 70 females (61.4%) and 44 males (38.6%). The average age was generally 52.94 ± 14.96. There was 82 indirect fractures (71.9%) and 32 direct fractures (28.1%) with the most common causes of falling in 48 cases (42%) and accidents in 58 cases (50.9%). The injury to non dominant Humerus was reported as 61 cases (53.5%) and to the dominant Humerus were 53 cases (46.5%).
Diabetes was the mostly underline disease seen in the samples with 14 cases (12.2%), 16 cases of Gastrointestinal diseases (14.2%) and 20 cases (17.5%) had osteoarthritis but the fewest underline disease was respiratory and neurological diseases in 4 cases (3.5%).
The most prescribed drugs according to the underline disease were Anti diabetic, NSAIDs and ASA while they had also the longest time of usage [Table 1].
Table 1.
Descriptive specifications of the patients with fracture of proximal Humerus
In review of the relations between fracture parts and treatment; it revealed that surgical treatment were more required as the number of fracture parts increased.
In two-parts fracture, methods of surgery was mostly percutaneous pins, suture, k-wire, tension band technique and in three and four-parts fractures, the methods of locking plates and Buttress plates have been used. In nonsurgical treatment, two methods of velpeau bandage and sling and sawath have been used; statistically the method of treatment (surgical or nonsurgical) had been directly related to the number of the fracture parts (P < 0.05) [Figure 2].
Figure 2.
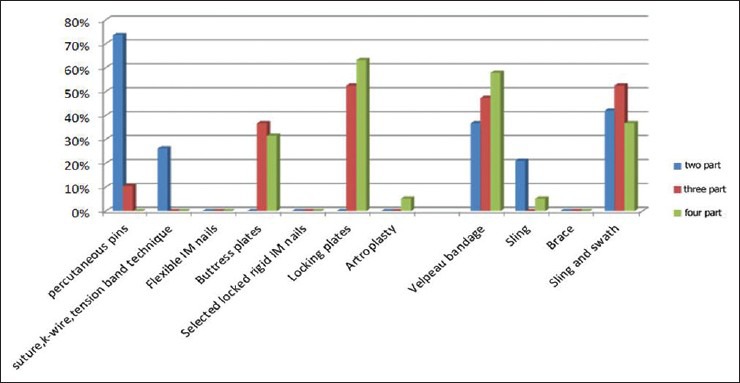
Rod graph of the treatment frequency percents with consideration of fracture parts in fracture of proximal Humerus patients
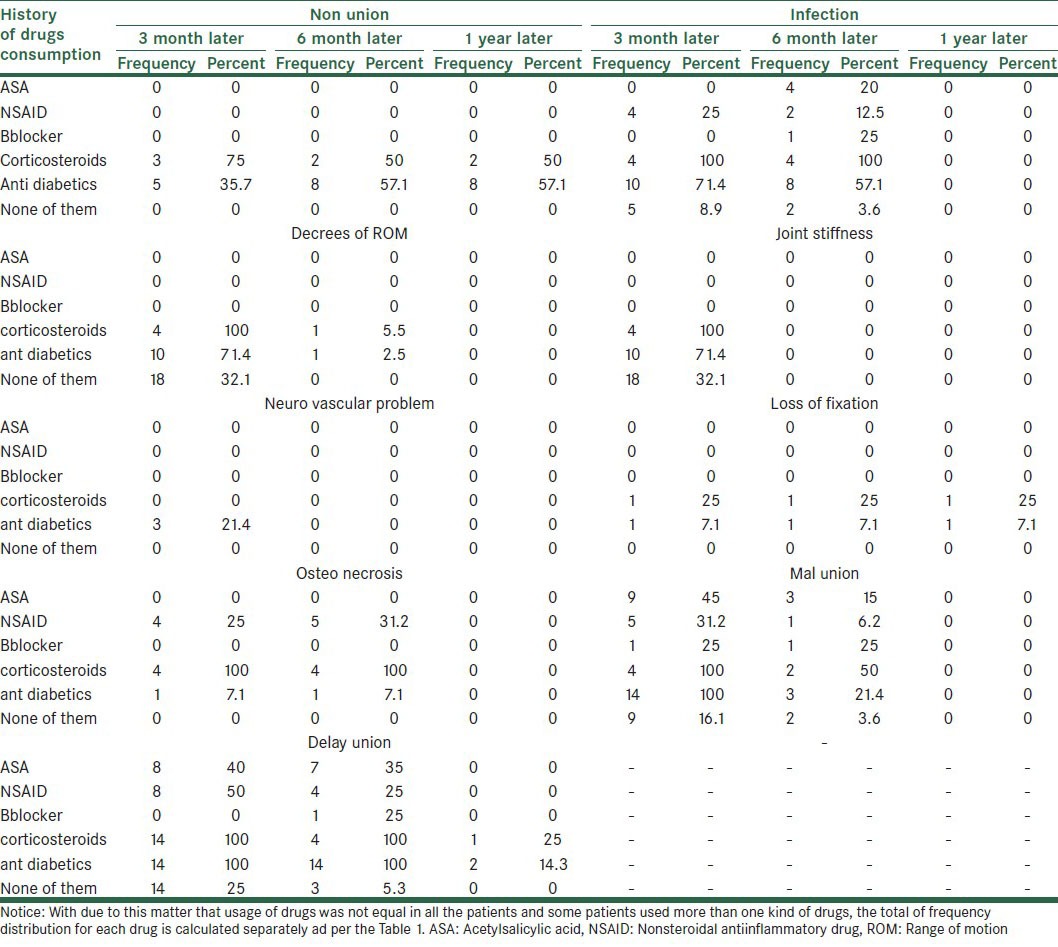
One of the factors which could affect on complication is acquisition of the above mentioned drugs. For example corticosteroids and anti diabetic drugs could be resulted to the infection, loss of fixation, delayed union and nonunion, also NSAID and corticosteroids could be lead to osteo necrosis [Table 2].
Table 2.
Double side frequency distribution for using oral drugs background and their results
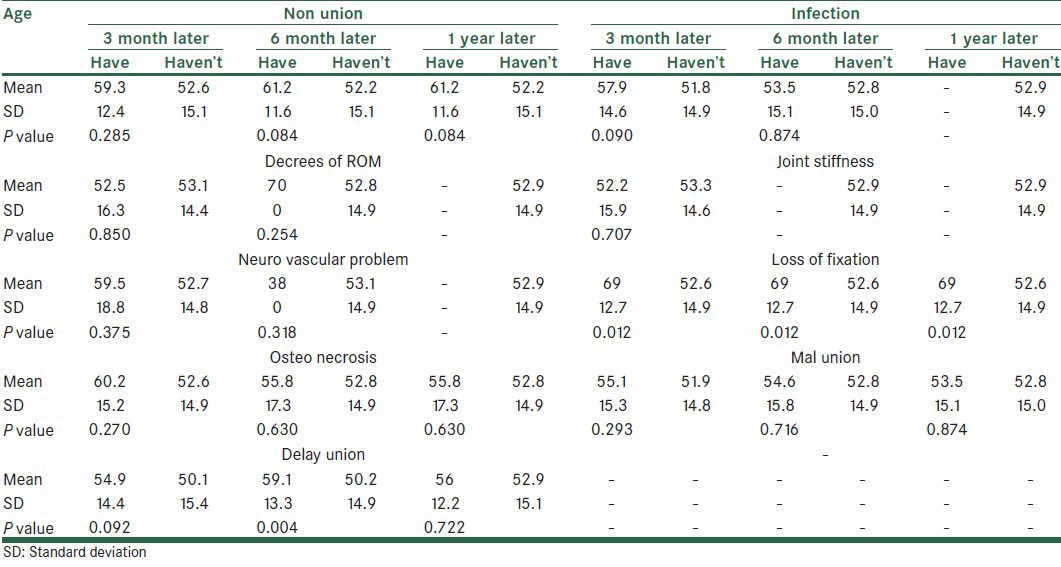
Among the studied side effects, the nonunion, limited ROM, infection, neurovascular problems, joints stiffness, osteo necrosis, and loss of fixation, delayed union and mal union are also memorable. In determination and comparing the relations between age and side effects, the T test was used, loss of fixation was seen in 3 and 6 months and one year after treatment, delayed union was seen in 6 months after treatment (P < 0.05). In other word the older patients had more side effects than Youngers [Table 3].
Table 3.
Determination and comparing of the affect of the age factor on treatment complications in fracture of proximal Humerus patients
In comparing and determination of the relation between gender and side effects, the Chi-square test was used and it has been cleared that there was no direct relation between them (P > 0.05), therefore the gender had no adverse effects.
In two parts fracture with dislocation, non union and mal union were remarkable in none surgical treatment so; surgical treatment was recommended.
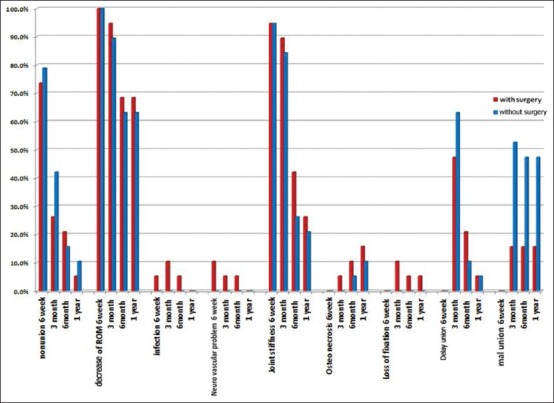
But some complications like decreasing of ROM, infection, delayed union, joints stiffness, osteo necrosis, loss of fixation, was more remarkable in surgical method but because of very small differences and diversity resulted as per the Fisher exact test there was no approved meaningful relation between them (P > 0.05) [Figure 3].
Figure 3.
Rode graph of the treatment complications in 2 parts fractures with dislocation
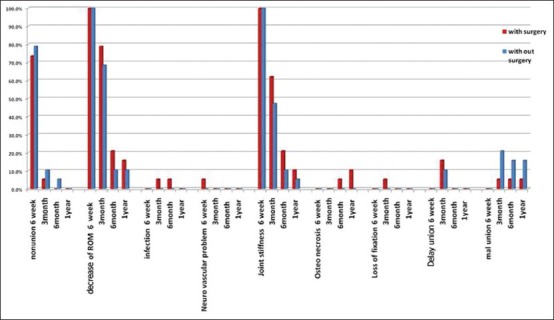
In three-parts fracture, none-union was seen in nonsurgical method in 6 weeks after treatment and mal union was more in none surgical treatment so the surgical method was better than nonsurgical, but some complications like decreasing of ROM, infection, delayed union, neurovascular problems, joints stiffness, osteo necrosis, loss of fixation, was more significant in surgical method than nonsurgical, statically as per the Fisher exact test there was only a meaningful relation in mal union in one year after treatment (P < 0.05) [Figure 4].
Figure 4.
Rode graph of the treatment complications in 3 parts fractures with dislocation
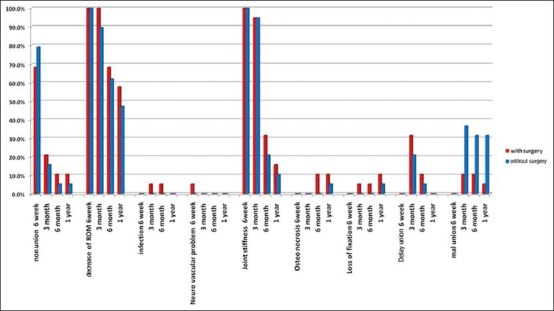
In four-parts fracture none-union was mostly seen in nonsurgical method in 6 weeks and 3 months and one year and delayed union was seen in 3 month after treatment, so the surgical method was better than nonsurgical, but some complications like decreasing of ROM, infection, neurovascular problems, joints stiffness, osteo necrosis, delayed union and non-union in 6 months after treatment and loss of fixation was more notable in surgical method than nonsurgical treatment, statically as per the Fisher exact test there was only a meaningful relation in mal union in 3 and 6 months and one year after treatment (P < 0.05) [Figure 5].
Figure 5.
Rode graph of the treatment complications in 4 parts fractures with dislocation
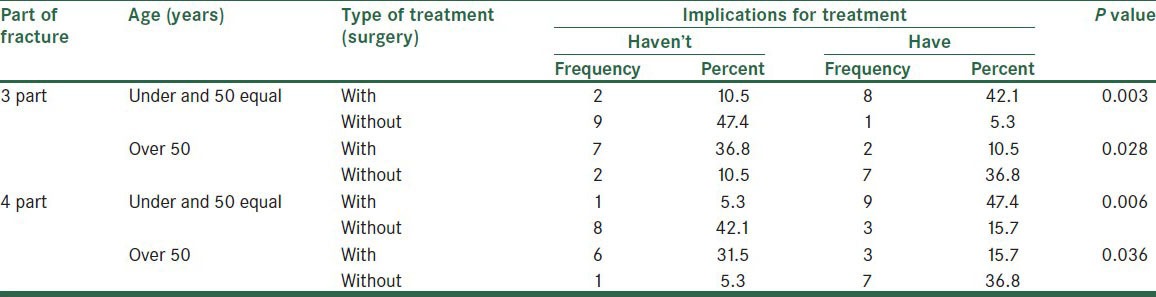
Although the surgical treatment had more complications considering of some basic factors like age, in three and four parts fracture, surgical treatment was better and had less complications in under 50 (years old) patients. Vice versa in above 50 (years old) patients, the surgical treatment had more side effects and nonsurgical treatment had better results (P < 0.05) [Table 4].
Table 4.
Reviewing of the treatment type in all kind of fractures with considering of the age factor and their result for treatment complications
DISCUSSION
Due to this matter that the Humerus proximal fracture is the most common type of arm fractures and it includes 4 to 5% of total fractures and also its treatment depends on some factors like (age, fracture displacement measure, last systematic disease, fractured bone resulted of pathology, soft tissue injury degree, bone injury and surgeon experience) the treatment would be selected among total way of surgical or nonsurgical treatments. Finding a way with less complication for the patients is very important and memorable.
Recent studies indicated that it is not so important if Humerus fracture had a union with a little mal-alignment because the appearance and function of the arm would not be changed after union. Accepting some mal-alignment is better than some complications which may happen after surgery, the operation procedure is opening reduction and internal fixation in this method that allow the patient to move his arm and shoulder normally one day after operation.
Yuksel et al., in a study on 18 patients between 39-90 years old in 2011 revealed that the result of nonsurgical method has been better in 3-4 parts fractures in older patients.[6,7,8] Also in our study the surgical method was associated with more complications in the patients above 50 and nonsurgical one was done with more success (P < 0.05).
In a study by Kayalar et al., on 18 patients between 18-89 years old revealed that the result of percotaneous pining has been better in 2-3 parts fractures in the younger patients. This kind of treatment was resulted to loss of fixation in above 60 years old patients.[9] The results of this study showed that surgical method was better with less complications in younger than 50 years patients (P < 0.05).
In Motison et al., study in 2010 and Neviaser et al., study in 2010 it was revealed that some surgical methods like Percutaneous pins, Suture, k-wire, tension band technique, Flexible IM nails, selected locked rigid IM nails, locking plates, Buttress plates associated with some complications like delayed union, non union, neurovascular problems, osteo necrosis, joints stiffness, infection and loss of fixation[1,10,11] as in our study.
In studies by Monga et al., in 2009, it was showed that internal fixation locking plate's surgery in 3 parts fracture treatment has been along with good performance in 18 male and 2 female patients between 29-46 years old. Also the vascular complications represent 5 to 6% of total complications and injury occurrences will be increased in the elders because of loss of vessel wall elasticity.[12]
In some prospective studies by Esen, Monga, Yang et al., in 2009-2011, they found that brachial plexus injury occurs at 6% of the cases; especially Axillary nerve injury is common in proximal Humerus fracture dislocation. Osteo necrosis is common in 3 to 4% of three-parts Humerus proximal fracture, 13-14% of four-parts of this kind of fractures and it contains a vast surface of anatomical neck of the arm. Nonunion can be resulted from high tensile fracture fragments, inadequate fixation of fracture fragments and infection, one of the other complications is mal-union which is lead to restriction of shoulder movement, also in reviewing of 64 patients in 25 months they revealed that locking plates treatment in 4 parts fractured in some cases resulted to osteo necrosis complication.[12,13] According to the results of this study we can say that locking plate surgical method can be more applied in four parts fractures and the complications such as Limited range of motion and Joint stiffness increase with fracture parts.
The study of Brorson et al., in 2009, on 62 patients with 4 parts fractures in one year revealed that using of locking plates is one of the best fixations and the most advantageous method in improving the situation, especially Osteoporotic fractures in elders, that leading to an early movement.[14,15]
As per Kilic et al., studied in 2008 on 13 males (between 35-83 years) with 2,3 and 4 parts fracture they noticed that locking plates will lead to better union in proximal Humerus fracture.[16]
Woo-bin et al., in 2013 evaluated 62 patients including 42 females and 20 males with 2 and 3 parts fractures (between 18-92 years old) and noticed that treatment with suture k-wire, tension band technique, and locking plates would have better quality after surgery.[4] In our study we have focused on this important point that generally it was not advised to use surgical method in the elders and it is better to use nonsurgical method for them.
Esen, Yunus et al., had studied 2 part fractures of 16 cadaver arm frozen in the age group of 70-80 years in 2011 showed that due to a complication of percutaneous pining move the pin from surgery to the thorax, mediastinal and abdominal with using multiplaner fixation with Suture and k-wire, tension band technique would be used to prevent the pin from the surgical site.[17]
Yildis et al., found in their studies in 2010 that fixation should be used with considering of the bone quality with less offensive methods.[18]
In some prospective studies by Fallatah et al., in 2008, it has been assumed that only 20% of proximal Humerus fractures needed to surgery and in their study on 45 patients (between 46-95 years) with acute fracture of proximal Humerus showed that the soft tissue situation and surgery technique play very important roles in amount of the pain and movement after surgery.[19] We have not mentioned to this matter in our study.
Orlando et al., in 2010 studied 50 patients (between 55-93 years) with 2 parts fracture and revealed that using of locking plated has very good results in these patients.[20] In opposite of this study we didn’t use the locking plated method in two parts fractures at all.
Martinez et al., found in their studies in 2009 on 58 patients with 3 -4 parts fractures that locking plates has very good results in all fractures except one case leads to mal union in 4 parts fracture.[21] According to our results the most applicable method in four parts fractures is locking plate with the rare malunion complication.
Gerhard et al., in a study on 211 patients with 3 parts fracture showed that experience of surgeon is more important than choosing of the implant type in 3 parts fracture of Humerus for a better successful surgery.[22] In this study the physician should make the final decision about the type of surgery.
Dietmar et al., in 2011 found in their studies on 64 patients with 4 parts fractures in 25 months that locking plates would be along with some complications like infection and Osteo Necrosis.[23,24] Which is in accordance with our study.
In our study, the average age of patients with humerus proximal fracture was generally 52.94 ± 14.96 and the number of fracture parts increased with age.
The measure of direct fracture was more in males than females and indirect fracture was seen more in females.
In Direct fracture, the injury was more to the dominant arm and the injury was seen more to the non-dominant arm in indirect fracture.
We also found that drugs can be one of the effective factors in treatment, for example; corticosteroids and Anti diabetic drugs had more frequency effects in infection, non union, loss of fixation and delayed union also NSAIDs and corticosteroids had more frequency effects in Osteo necrosis occurrences.
In multi-parts fractures, with increasing of fracture parts, the urgency and requirement to the surgery was felt more, in two-parts fracture two kind of technique were used, K-wire and tension band technique but in three and four-parts fracture mostly locking plates and Buttress plate were used, in nonsurgical method, sling and sawath and velpeau bandages were used for all the parts, statistically there was a direct relation between selection of the treatment method (surgical or nonsurgical) and extent number of fracture parts while the gender was not an effective factor for choosing the treatment method.
The limitation of our study was the lack of patients’ intention to follow up or unanswered calls to gather the information in some cases.
CONCLUSION
As per the result of this study, in two parts fracture with displacement in non surgical treatment, nonunion and mal union were remarkable so surgical treatment was recommended.
In four-part fracture nonunion results was seen more in nonsurgical method.
Although the surgical treatment had more complications but with considering of some basic factors like age, in three and four parts fracture, surgical treatment was better and had less complications in fewer than 50 (years old) patients. Vice versa in above 50 (years old) patients, the surgical treatment had more side effects and nonsurgical treatment had better results.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gupta AK, Gupta M, Sengar G, Nath R. Functional outcome of closed fractures of proximal humerus managed by Joshi's external stabilizing system. Indian J Orthop. 2012;46:216–20. doi: 10.4103/0019-5413.93679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Egol KA, Koval KJ. 7th ed. Chapter 2. Philadelphia: Lippincott Williams; 2010. Fractures of the proximal humerus in: Rockwood and Green's Fracture in Adult; p. 1039. [Google Scholar]
- 3.Terrycanale S, Jamesh B. 12th ed. Chapter 57. Memphis: Edward A Perez; 2013. Fractures of the shoulder/arm/for in: Campbell's operative orthopaedics; pp. 2832–56. [Google Scholar]
- 4.Jung WB, Moon ES, Kim SK, Kovacevic D, Kim MS. Does medial support decrease major complications of unstable proximal humerus fractures treated with locking plate? BMC Musculoskelet Disord. 2013;14:102. doi: 10.1186/1471-2474-14-102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Esen E, Doğramaci Y, Kömürcü M, Kanatli U, Bölükbaşi S, Atahan AO. Biomechanical comparison of fixation of two-part osteoporotic neck fracture of the proximal humerus using uni-planar and multi-planar Kirschner wire. Eklem Hastalik Cerrahisi. 2009;20:114–8. [PubMed] [Google Scholar]
- 6.Yüksel HY, Ylmaz S, Akşahin E, Celebi L, Muratl HH, Biçimoğlu A. Results of Nonoperative treatment for Three- and Four-Part Fractures of the Proximal humerus in Low-Demand Patients. J Orthop Trauma. 2011;25:588–95. doi: 10.1097/BOT.0b013e318210ea56. [DOI] [PubMed] [Google Scholar]
- 7.Modi CS, Nnene CO, Godsiff SP, Esler CN. Axillary artery injury secondary to displaced proximal humeral fractures: A report of two cases. J Orthop Surg (Hong Kong) 2008;16:243–6. doi: 10.1177/230949900801600223. [DOI] [PubMed] [Google Scholar]
- 8.Bicknell RT, DeLude JA, Kedgley AE, Ferreira LM, Dunning CE, King GJ, et al. Early experience with computer-assisted shoulder hemiarthroplasty for fractures of the proximal humerus: Development of a novel technique and an in vitro comparison with traditional methods. J Shoulder Elbow Surg. 2007;16:S117–25. doi: 10.1016/j.jse.2006.08.007. [DOI] [PubMed] [Google Scholar]
- 9.Kayalar M, Toros T, Bal E, Ozaksar K, Gürbüz Y, Ademoğlu Y. The importance of patient selection for the treatment of proximal humerus fractures with percutaneous technique. Acta Orthop Traumatol Turc. 2009;43:35–41. doi: 10.3944/AOTT.2009.035. [DOI] [PubMed] [Google Scholar]
- 10.Neviaser AS, Hettrich CM, Beamer BS, Dines JS, Lorich DG. Endosteal Strut Augment Reduces Complications Associated With Proximal Humeral Locking Plates. Clin Orthop Relat Res. 2011;469:3300–6. doi: 10.1007/s11999-011-1949-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mathison C, Chaudhary R, Beaupre L, Reynolds M, Adeeb S, Bouliane M. Biomechanical analysis of proximal humeral fixation using locking plate fixation with an intramedullary fibular allograft. Clin Biomech (Bristol, Avon) 2010;25:642–6. doi: 10.1016/j.clinbiomech.2010.04.006. [DOI] [PubMed] [Google Scholar]
- 12.Monga P, Verma R, Sharma VK. Closed reduction and external fixation for displaced proximal humeral fractures. J Orthop Surg (Hong Kong) 2009;17:142–5. doi: 10.1177/230949900901700203. [DOI] [PubMed] [Google Scholar]
- 13.Yang H, Li Z, Zhou F, Wang D, Zhong B. A prospective clinical study of proximal humerus fractures treated with a locking proximal humerus plate. J Orthop Trauma. 2011;25:11–7. doi: 10.1097/BOT.0b013e3181d2d04c. [DOI] [PubMed] [Google Scholar]
- 14.Brorson S, Olsen BS, Frich LH, Jensen SL, Johannsen HV, Sørensen AK, et al. Effect of osteosynthesis, primary hemiarthroplasty, and non-surgical management for displaced four-part fractures of the proximal in humeruselderly: A multi-centre, randomised clinical trial. Trials. 2009;10:51. doi: 10.1186/1745-6215-10-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Leonard M, Mokotedi L, Alao U, Glynn A, Dolan M, Fleming P. The use of locking plates in proximal humeral fractures: Comparison of outcome by patient age and fracture pattern. Int J Shoulder Surg. 2009;3:85–9. doi: 10.4103/0973-6042.63214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kiliç B, Uysal M, Cinar BM, Ozkoç G, Demirörs H, Akpinar S. Early results of treatment of proximal humerus fractures with the PHILOS locking plate. Acta Orthop Traumatol Turc. 2008;42:149–53. doi: 10.3944/aott.2008.149. [DOI] [PubMed] [Google Scholar]
- 17.Esen E, Doğramaci Y, Kömürcü M, Kanatli U, Bölükbaşi S, Atahan AO. Biomechanical comparison of fixation of two-part osteoporotic neck fracture of the proximal humerus using uni-planar and multi-planar Kirschner. Eklem Hastalik Cerrahisi. 2009;20:114–8. [PubMed] [Google Scholar]
- 18.Yildiz C, Kürklü M, Ozkan H, Bilgiç S, Sehirlioğlu A, Yurttaş Y, et al. AO tension band technique application in proximal humerus fractures. Eklem Hastalik Cerrahisi. 2010;21:62–7. [PubMed] [Google Scholar]
- 19.Fallatah S, Dervin GF, Brunet JA, Conway AF, Hrushowy H. Functional outcome after proximal humeral fractures treated with hemiarthroplasty. Can J Surg. 2008;51:361–5. [PMC free article] [PubMed] [Google Scholar]
- 20.Olerud P, Ahrengart L, Söderqvist A, Saving J, Tidermark J. Quality of life and functional outcome after a 2-part proximal humeral fracture: A prospective cohort study on 50 patients treated with a locking plate September. J Shoulder Elbow Surg. 2010;19:814–22. doi: 10.1016/j.jse.2009.11.046. [DOI] [PubMed] [Google Scholar]
- 21.Martinez AA, Cuenca J, Herrera A. Philos plate fixation for proximal humeral fractures. J Orthop Surg (Hong Kong) 2009;17:10–4. doi: 10.1177/230949900901700103. [DOI] [PubMed] [Google Scholar]
- 22.Konrad G, Audigé L, Lambert S, Hertel R, Südkamp NP. Similar Outcomes for Nail versus Plate Fixation of Three-part Proximal Humeral Fractures. Clin Orthop Relat Res. 2012;470:602–9. doi: 10.1007/s11999-011-2056-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yang H, Li Z, Zhou F, Wang D, Zhong B. A Prospective Clinical Study of Proximal Hummers Fractures Treated with a Locking Proximal humerus Plate. J Orthop Trauma. 2011;25:11–7. doi: 10.1097/BOT.0b013e3181d2d04c. [DOI] [PubMed] [Google Scholar]
- 24.Krappinger D, Roth T, Gschwentner M, Suckert A, Blauth M, Hengg C, et al. Preoperative assessment of the cancellous bone mineral density of the proximal humerus using CT data. Skeletal Radiol. 2012;41:299–304. doi: 10.1007/s00256-011-1174-7. [DOI] [PubMed] [Google Scholar]