

Abstract
The current study adopted the trauma film paradigm to examine potential moderators affecting heart rate (HR) as an indicator of peritraumatic psychological states and as a predictor of intrusive memories. We replicated previous findings that perifilm HR decreases predicted the development of intrusive images and further showed this effect to be specific to images rather than thoughts, and to detail rather than gist recognition memory. Moreover, a group of individuals showing both an atypical sudden reduction in HR after a startle stimulus and higher trait dissociation was identified. Only among these individuals was lower perifilm HR found to indicate higher state dissociation, fear, and anxiety, along with reduced vividness of intrusions. The current findings emphasize how peritraumatic physiological responses relate to emotional reactions and intrusive memory. The moderating role of individual difference in stress defense style was highlighted.
Keywords: Startle, Heart rate, Trauma, Memory
Intrusive memories are a hallmark of posttraumatic stress disorder (PTSD; American Psychiatric Association [APA], 1994) but little is known of what causes them. Previous research has suggested heart rate (HR) falls during the encoding of trauma stimuli that later return as intrusive memories (Holmes, Brewin, & Hennessy, 2004). The current study sought to replicate and extend this finding by distinguishing between images and thoughts, by assessing risk factors such as trait dissociation, and by investigating psychophysiological moderators of this effect.
Heart Rate as an Index of Response to Trauma
In studies of PTSD, HR has been used as an objective measure of reactions to trauma-related stimuli. Most studies have shown a positive association between PTSD severity and HR increases when trauma memories were involuntarily triggered by reminders (e.g., Adenauer, Catani, Keil, Aichinger, & Neuner, 2010; Ehlers et al., 2010; Hetzel-Riggin, 2010). However, studies investigating voluntary retrieval of trauma memory have found reduced HR response among PTSD patients relative to trauma survivors without PTSD (e.g., Halligan, Michael, Wilhelm, Clark, & Ehlers, 2006). Cognitive characteristics commonly seen in PTSD patients such as dissociation and rumination have been related to the above findings of physiological inhibition (e.g., Halligan et al., 2006; Hetzel-Riggin, 2010; Koopman et al., 2004). For example, in a study involving rape victims (Griffin, Resick, & Mechanic, 1997), lower HR during verbal recollection of the trauma was found among individuals with high, compared to those with low peritraumatic dissociation. These results indicated the existence of important individual differences in the psychological and physiological reactions to trauma-related stimuli.
Additionally, HR has been investigated at time points close to traumatic accidents. Studies assessing HR at the time when victims arrived at hospital and onwards (e.g., before discharge) have found associations between higher HR and greater posttraumatic symptoms afterwards (e.g., Bryant, Creamer, O'Donnell, Silove, & McFarlane, 2008; De Young, Kenardy, & Spence, 2007; Kraemer, Mörgeli, Roth, Hepp, & Schnyder, 2008). However, when HR was examined at time points closer to the accidents (e.g., at the accident sites or during ambulance transport), victims later developing more severe PTSD symptoms have sometimes been found to have lower HR (Blanchard, Hickling, Galovski, & Veazey, 2002; O'Donnell, Creamer, Elliott, & Bryant, 2007; for nonsignificant findings, see also Buckley et al., 2004; Ostrowski, Christopher, & Delahanty, 2007). In sum, there is evidence to suggest that the relationship between HR and PTSD may be different at the time when trauma is encoded versus subsequently.
To model the processes underlying the encoding of trauma memories and better control for variability, the trauma film paradigm (reviewed by Holmes & Bourne, 2008) has been widely adopted with healthy volunteers. A previous study (Holmes et al., 2004) adopting this paradigm has found decreases in HR during film viewing, with a greater reduction associated with an increased number of subsequent intrusive images of the film. Moreover, the mean HR during the film sequences matching the contents of intrusions was found to be significantly lower than the sequences that did not intrude. The HR reduction was linked with fear bradycardia and freezing response commonly found in animals in the face of overwhelming threats. However, an alternative explanation of the HR reduction, increased orienting (Adenauer et al., 2010; Sokolov, 1960; Turpin, 1979), has not been ruled out. The current study sought to investigate in more detail the relationship between dissociation, HR, and intrusive memories.
Dual Representation Theory of PTSD
Differences have been proposed between the cognitive mechanisms involved in a resilient versus a pathological memory process. According to the dual representation theory (DRT) of PTSD (Brewin, Dalgleish, & Joseph, 1996; Brewin, Gregory, Lipton, & Burgess, 2010), traumatic events are encoded via two different pathways and give rise to two types of representations with different properties. First, contextualized representations (C-reps) involve focused attention and high-level cognitive processing supported by medial temporal lobe structures including the hippocampus. They contain viewpoint-independent contextual information and “gist” representations (e.g., when, where, how, who) of an event, which are crucial for the formation of episodic memory and abstract meanings. These properties also enable the trauma representations to integrate with personal semantic and autobiographical memory, making them available for verbal thoughts and appraisals. In contrast, sensory-bound representations (S-reps) are processed with the support of lower level sensory cortices. S-reps are viewpoint-dependent and inflexibly depictive of the original sensory details (e.g., images, sound, smell), physiological reactions (e.g., heart pounding, palm sweating), and feelings (e.g., fear, anger) occurring during the event. It is thought that in ordinary situations S-reps decay soon after the events. However, when formed under extreme levels of emotion, S-reps become enduring and intrusive sensory memories thus arise (Brewin et al., 2010).
Supporting the diverse memory representations and processes proposed in the DRT, a previous study (Hagenaars, Brewin, van Minnen, Holmes, & Hoogduin, 2010) has shown that the processes underlying intrusive sensory images are likely different to those underlying intrusive verbal thoughts. Despite being a form of intrusion, the semantic nature of intrusive thoughts suggests the involvement of higher-level cognitive functions and a more prominent involvement of C-reps (Hagenaars et al., 2010). Moreover, a study adopting the trauma film paradigm showed that participants focusing on sensory details during and after the film viewing reported more PTSD-like symptoms compared to those focusing on conceptual information and ideas (Kindt, van den Hout, Arntz, & Drost, 2008). Further, peritraumatic dissociation, which involves a reduction in consciousness, has been hypothesized to lead to weaker C-reps and to impede the normal integration of S-reps and C-reps (Brewin et al., 2010). Agreeing with this argument, peritraumatic dissociation has been found to impair memory performance (Brewin, Ma, & Colson, 2013; Brewin & Mersaditabari, 2013) and to reliably predict PTSD symptoms (Ozer, Best, Lipsey, & Weiss, 2003).
Startle Response and Stress Defense Styles
According to the defense cascade model (Bradley & Lang, 2000), the proximity of a threat elicits an orienting response characterized by cardiac deceleration and information gathering. At the second stage, an immediate threat may elicit an active defense (fight or flight), a reaction associated with the activation of the sympathetic nervous system and increased HR. However, when escape is perceived as impossible, a passive defense mode featured by physical deactivations such as freezing or bradycardia is more likely to be observed (Kaada, 1987).
In human studies, neurobiological characteristics associated with different stress defense behaviors and styles have been explored. For example, exaggerated startle is indicative of hyperexcitable fear circuits (Rosen & Schulkin, 1998; Vaidyanathan, Patrick, & Cuthbert, 2009) and has been observed in PTSD patients (e.g., Cuthbert et al., 2003; Ladwig et al., 2002). On the other hand, reduced startle has also been found among individuals with chronic exposure to trauma (Medina, Mejia, Schell, Dawson, & Margolin, 2001) and prolonged PTSD symptoms (Morgan & Grillon, 1998). A subgroup of PTSD patients with physiological suppression, instead of heightened reactivity, and a tendency to adopt passive stress coping behaviors has thus been suggested (Medina et al., 2001). The current study adopted the trauma film paradigm to examine the effect of individual difference in startle heart rate (sHR) response on the process and development of intrusive traumatic memory.
The Current Study
The current study included healthy adult participants and involved two types of HR measurement and two forms of memory assessment. The sHR response to an auditory startle trigger was assessed followed by examination of HR and psychological states before, during, and after viewing a trauma film. A diary was kept for 7 days to record intrusive memories of the film, and a recognition memory test was introduced after one week.
The first aim of the study was to examine the association between HR and the psychological and memory measures. Low absolute levels of HR have been found to predict the development of PTSD (Blanchard et al., 2002; O'Donnell et al., 2007) and to be associated with peritraumatic dissociation (Griffin et al., 1997). Therefore, we examined the relationships between absolute levels of HR, dissociation, and other psychological states at the memory encoding (perifilm) phase, predicting that lower HR would be correlated with higher dissociation. Additionally, following Holmes et al. (2004), we examined perifilm HR change relative to baseline, as well as during sequences of the film that later became intrusive compared to those that did not intrude. We predicted that greater decreases in both HR measures would be associated with more frequent intrusive memories. The vividness of these images was also assessed given its clinical importance. Further, considering the important theoretical differences between intrusions taking the form of abstract thoughts and sensory images (Hagenaars et al., 2010), and between processes underlying gist and detail memory (Adolphs, Tranel, & Buchanan, 2005), these were assessed separately.
Next, we investigated the role of an exaggerated or diminished startle response: first, whether individuals with different levels of sHR varied in pre-existing anxiety and dissociation levels, as well as in intrusive memories for the trauma film. Second, the role of sHR in the relationships between HR and different psychological responses was examined. As exaggerated startle has been suggested to indicate hyperexcitable fear circuits (Rosen & Schulkin, 1998; Vaidyanathan et al., 2009), individuals with a higher sHR response were predicted to have greater anxiety. In contrast, as a reduced startle response has been associated with passive defense (Medina et al., 2001), those with a diminished sHR response were predicted to have a greater tendency to dissociation. Their lower levels of HR during the trauma film were expected to be a sign of dissociation, and greater reductions in perifilm HR were expected to be predictive of the development of more involuntary memories of the film.
Method
Participants
The current study was approved by the Research Ethics Committee at University College London. Nonsmoking, healthy native English speakers aged between 18 and 40 with a body mass index (BMI) range of 17.5 to 30 were recruited. Volunteers with a history of cardiovascular illness, any other significant physiological illness, or currently taking any medication including contraceptives were excluded. Because the materials in this study contained graphic footages from car accidents, those who had experienced/witnessed serious road traffic accidents, had close others seriously injured/killed in road traffic accidents, and individuals with a history of any mental disorder were excluded. Eighty-seven participants passed the inclusion and exclusion criteria and completed the study. They were paid £15 as a reward for their participation.
The data from 10 participants were excluded due to a high number of artifacts in the electrocardiographic (ECG) data (i.e., more than 3% corrected R-R intervals; Hodson, Harnden, Roberts, Dennis, & Frayn, 2010; Vaile et al., 2001). Another 13 participants were excluded because of procedural issues (e.g., failed to keep the intrusion diary at the end of each day, experienced actual traumatic or stressful events between the two study sessions, errors in the volume setting of the auditory startle trigger in the psychophysiological reactivity test). This resulted in a final sample size of 64 (male = 33). Subgroups were defined at the data analysis stage based on sHR patterns in the psychophysiological reactivity test. See Results section for details regarding the classification approach.
Psychophysiological Data Acquisition
The Actiwave Cardio system (Camntech, Cambridge, UK) was used in the current study to collect ECG signals. Signals were sampled continuously at 512 Hz, with resolution 9 bits and no notch filter. Two disposable electrodes (Blue Sensor SP, Ambu, Denmark) were attached to the participants' chest to record the signals.
Psychophysiological Reactivity Test
A psychophysiological reactivity test was conducted at the beginning of the study to assess sHR response. Participants were told that the aim of this task was to examine the effect of sound on relaxation, and, therefore, they might encounter an unexpected loud noise. However, the only thing they needed to do was to try to be relaxed. After the instruction, a 6-min resting period was given with a white noise (500-ms, 110 dB, and instantaneous rise time) presented through a set of headphones at the end and followed by an ECG recording of 80 s.
Trauma Film Viewing
A 13-min 40-s trauma film used in previous studies (e.g., Holmes et al., 2004) was presented to participants on a 28.5 × 40 cm computer monitor. The sound was played through headphones. The film consists of five scenes of different real-life car accidents containing horrific images of emergency service personnel working to extract trapped victims and move dead bodies, injured individuals screaming, and body parts among vehicle wreckage. Before each scene, there is a brief narration (voiceover without images) introducing the context of the accident and background of the victims involved. Participants were asked to watch the film as closely as possible, and imagine themselves being present and witnessing the events firsthand. ECG signals were recorded throughout the whole film, the prefilm, and postfilm resting periods.
Materials: Symptom Check, Trait and State Measurements
Posttraumatic Stress Diagnostic Scale.
The Posttraumatic Stress Diagnostic Scale (PDS: Foa, 1995) is a 49-item self-report measure of traumatic experiences and related PTSD symptoms. The first section presents a short checklist identifying potential traumatic events experienced by respondents. The second section asks respondents to indicate one of these events that has troubled them the most at the time of answering the questionnaire. They then identify the elapsed time and rate Criterion A for PTSD in DSM-IV (APA, 1994) based on the aftermath caused by the specified event. In the third and fourth sections, Criteria B, C, D, and E for PTSD are also rated according to the event picked out in section two. PTSD symptom severity is indicated by the sum of all the items for Criteria B, C, and D. The scores range between 0 and 51, with the higher scores indicating greater severity. The validity of the PDS (Foa, Cashman, Jaycox, & Perry, 1997) has been supported by good diagnostic agreement with the Structured Clinical Interview for DSM-IV (Spitzer, Williams, Gibbon, & First, 1990). Satisfactory reliability was found in the current sample (Cronbach's α = .86).
State-Trait Anxiety Inventory.
The State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983) is a widely used self-report scale for anxiety. The first subscale measures state, whereas the second subscale measures trait anxiety. They each have 20 items, and the anxiety levels are indicated by the sum of all items in the corresponding subscale. The scores range between 20 and 80 with higher scores indicating greater anxiety. The validity of the STAI has been supported by its ability to discriminate high versus low stress situations and its agreement with other anxiety assessment tools (Metzger, 1976; Spielberger, 1989). Satisfactory reliability was found in the current sample (Cronbach's α ranged between .94 and .96).
Dissociative Experiences Scale.
The Dissociative Experiences Scale (DES-II; Carlson & Putnam, 1993) is a 28-item questionnaire designed to examine trait dissociation. It is composed of three aspects of dissociation: amnesia (e.g., finding oneself in a place and having no idea how he or she got there), depersonalization-derealization (e.g., feeling one's body does not seem to belong to him or herself), and absorption (e.g., finding oneself so involved in a fantasy or daydream that it feels as though it were really happening). For each item, participants are required to indicate the percentage of time when they have a given experience in daily life (range between 0 and 100%). A tendency toward dissociation is indicated by averaging the percentage scores with higher scores indicating more frequent occurrence of dissociation. Evidence suggesting good validity of the DES has been reviewed by Dubester and Braun (1995). Satisfactory reliability was found in the current sample (Cronbach's α = .94).
Dissociative State Scale.
The Dissociative State Scale (DSS; adapted from Bremner et al., 1998) is a 19-item self-report measurement for state dissociation. The covered areas include depersonalization, derealization, and amnesia. For each item, participants are required to rate on a five-point scale anchored with 0 (not at all) and 4 (extremely) based on their feeling at the particular moment in time when they are given the measure. The level of state dissociation was indicated by the sum of all items. The scores ranged between 0 and 76, with higher scores indicating greater levels. Satisfactory reliability was found in the current sample (Cronbach's α ranged between .86 and .92). Validity has been supported by the findings that healthy participants scored lower than PTSD patients (Bremner et al., 1998).
Mood rating scales.
Two 11-point visual analogue scales (anchored with 0 = not at all and 10 = extremely) were used to assess participants' state of fear and calm.
Materials: Memory Measures
Intrusion diary.
A tabular diary was used to record intrusions for 7 days after viewing the trauma film. Intrusion was defined as “unintended and spontaneous, rather than deliberate, memories/thoughts/images about the film that easily capture attention and may interfere with ongoing activities.” Participants were asked to note the timing of every intrusion, describe its contents, and to specify whether it took the form of an image, a thought, or a mixture of both. The vividness level (0 = not at all, 10 = extremely) was rated for the imagery and mixture, but not for thought intrusions. The frequency of intrusive images was calculated by summing the number of times when imagery intrusions and those consisting of a mixture of both images and thoughts occurred over the week. Similarly, the frequency of intrusive thoughts was the number of times when thought intrusions occurred over the week. The vividness of intrusion was derived from averaging the vividness ratings of the occurrences that were mainly images or a mixture of both images and thoughts. Cases with no qualifying intrusions did not receive a score for vividness.
Recognition task.
In order to separately assess contextualized and sensory-bound memory (Brewin et al., 2010) for the trauma film, the questionnaire developed in a previous study (Bisby, Brewin, Leitz, & Curran, 2009) aiming to assess gist versus detail information in the trauma film was used. This questionnaire involved 30 multiple-choice questions with one correct and three plausible choices. For each scene in the film, six questions were asked. Three of these questions tapped gist recognition memory such as the context and causes of the incidents (e.g., where/how the collisions occurred). The remaining three tapped detail recognition memory such as the sensory elements in the scenes (e.g., the color of the shirt that a victim wore).
Identification task.
Based on the description given by participants in their intrusion diaries, the parts of the film where intrusive images were likely to be from were replayed. Participants were asked whether the replayed parts of the film were the sources of their intrusive images. After agreement was reached, they were then asked to identify the exact sections, namely, the beginning and the ending seconds in the film corresponding to their intrusions. This task was used to locate the intrusive and nonintrusive sequences of the film for each participant.
Procedure
All participants were asked to be free of caffeine, alcohol, and medication 24 h before testing to avoid the effects of these substances. As shown in Figure 1, PTSD symptom and the trait measures (i.e., anxiety and dissociation) were given at the beginning. Next, participants were fitted with the ECG electrodes and given the psychophysiological reactivity test, after which they were reassured that no more sudden noise would be delivered. Another 6-min prefilm resting period was then introduced with no task other than resting given in the first 2 min, and the prefilm psychological state measures (i.e., anxiety, dissociation, fear, and calmness) given at the third minute. The trauma film was then shown to the participants with a 10-min postfilm resting period. The perifilm psychological state measures were given at the very beginning of this period and finished within the first 4 min, leaving the next 6 min pure rest. The postfilm psychological state measures were given at the end of this resting period. Participants were instructed in the usage of the intrusion diary and asked to keep it for 7 days at the end of the first session. A text message was sent at 9 p.m. each day to remind the participants to check the completion of the diary for that particular day. In the follow-up session on the 8th day, the diary was returned and participants carried out the recognition and identification task.
Figure 1.
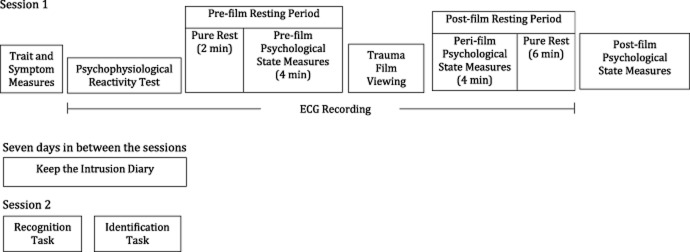
Timeline of the procedures.
Analytic Strategy
All statistical analyses were performed with SPSS version 18 (SPSS Inc., Chicago, IL). Scores greater than 3 standard deviations above the mean were changed to one unit larger than the greatest nonextreme score in the given variable, whereas scores smaller than 3 standard deviations below the mean were changed to one unit smaller than the smallest nonextreme score (Tabachnick & Fidell, 1996). For example, an outlying score of 27.0 would be changed to 11.5 if the highest nonextreme score was 10.5. The variables and number of cases with such changes were: trait dissociation (2 cases); prefilm anxiety (1 case); pre- (2 cases), peri- (2 cases) and postfilm dissociation (1 case); frequency of intrusive images (2 cases); and prefilm HR (1 case). Normality of distributions was examined by dividing the absolute values of skewness by the standard error of skewness. For variables with values larger than 3 from this calculation, square root transformation was performed.
The ECG data were examined using VivoSense software (VivoNoetics, San Diego, CA). Artifacts in the data due to misdetected R-waves were easily recognized as outliers from the average HR curve and were manually deleted and interpolated using the facility of the software (Halligan et al., 2006). Next, the average HR pre-, peri-, and postfilm were calculated. The calculation of pre- and postfilm HR excluded periods when the participants were filling in questionnaires and therefore only included HR in the first 2 min of the prefilm and the last 6 min of the postfilm resting period. Perifilm HR was calculated by averaging HR during the whole film. Among those who had at least one imagery intrusion and were able to identify the film sequences that later intruded (n = 54), HR was averaged during these sequences and the sequences that did not intrude, respectively. Two forms of HR change were calculated: The “overall perifilm HR change” was estimated by subtracting the prefilm HR from the perifilm HR. To calculate the “intrusive sequence HR change,” the mean HR in the nonintrusive sequences was first subtracted from the mean HR in the intrusive sequences of the film. In order to control for the overall amount of variation caused by the film, this HR difference score was then divided by the absolute value of the overall perifilm HR change.
Given the extensive literature linking dissociation to lower HR, as well as the lower HR found during intrusive sequences by Holmes et al. (2004), one-tailed t tests were applied to examine the differences between pre- and perifilm HR, as well as between HR during the intrusive and nonintrusive sequences. Pearson's correlations were used to examine the association between HR and psychological states at the corresponding phases (e.g., prefilm HR with prefilm anxiety, perifilm HR with perifilm fear). Pearson's correlations were also performed to examine whether the overall perifilm HR change and/or intrusive sequence HR change were predictive of the measures of intrusive and recognition memory (i.e., intrusive thoughts and images, gist and detail recognition memory). Further, the relationships between these memory measures were examined by Pearson's correlations.
Next, to classify participants by their sHR, Ward's hierarchical cluster analysis was adopted. This method has been used in previous studies (López, Poy, Pastor, Segarra, & Moltó, 2009; Milligan & Isaac, 1980) for its ability to produce clusters with similar numbers in small data sets. Following López et al. (2009), the variables used in this analysis were the second-by-second HR changes during the first 10 s after the onset of the white noise in the psychophysiological reactivity test (relative to the mean HR in the 15-s prestimulus period). One-way analyses of variance (ANOVAs) and a chi-square test were conducted initially to establish the demographic, physiological, and psychological characteristics of the three groups. To examine the effects of the trauma film on different groups, a two-way (Group × Time) mixed design ANOVA was performed on HR, and one-way ANOVAs were used to examine group differences in memories for the trauma film. Given the multiple levels on the group and time factors as well as the specific design of the study, tests of linear and quadratic effects replaced tests of main effects. For all of the F tests, linear and quadratic effects were examined. Homogeneity of variance was assessed by Levene's statistic, while sphericity was examined with Mauchly's test. When the assumption of sphericity was not met, the uncorrected degrees of freedom, epsilon (Greenhouse-Geisser), corrected F, and corrected p values were reported. Finally, to investigate the moderating effects of sHR on the relationships between HR, psychological states, and intrusive memories, multiple regressions were used.
A few exploratory analyses were performed. First, two-tailed t tests were used to compare the frequency of intrusive thoughts versus images, the performance in gist versus detail recognition memory, and recognition memory for the scenes that later became intrusive versus those that did not. Second, two-way (Group × Time) mixed design ANOVAs were used to examine the effect of the film on psychological states and individual differences in such reactions. Similar to the two-way mixed design ANOVA on HR, tests of linear and quadratic effects replaced main effects.
Results
Relationships Between HR, Psychological State, and Memory in the Overall Sample
Descriptive data for HR, psychological states, and memory measures are summarized in Table 1. None of the correlations between HR and psychological states at the corresponding phases was significant (largest r = −.18, p = .16). Comparisons of HR levels at different phases with one-tailed t tests showed that the difference between the pre- and perifilm HR, t(63) = 1.27, p = .21, was not significant, but that the drop in HR associated with intrusive versus nonintrusive sequences was significant, t(53) = −2.33, p < .05.
Table 1.
Mean and Standard Deviations of All Variables by Phase and Group
| Overall sample | High startle group | Medium startle group | Low startle group | |||||
|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
| Biological and background characteristics | ||||||||
| Age | 64 | 24.98 (4.71) | 14 | 23.07 (3.50) | 31 | 25.45 (5.20) | 19 | 25.63 (4.49) |
| Years of education | 64 | 16.86 (2.09) | 14 | 16.38 (1.56) | 31 | 17.06 (2.14) | 19 | 16.84 (2.36) |
| BMI (kg/m2) | 64 | 22.19 (3.04) | 14 | 21.88 (3.34) | 31 | 22.28 (3.07) | 19 | 22.27 (2.92) |
| Psychological traits | ||||||||
| Trait anxiety (20–80) | 64 | 39.02 (10.36) | 14 | 36.43 (7.61) | 31 | 39.77 (12.14) | 19 | 39.72 (8.93) |
| Trait dissociation (%) | 64 | 14.69 (10.52) | 14 | 9.30 (6.77) | 31 | 14.81 (11.03) | 19 | 18.46 (10.65) |
| PTSD symptom (0–51)a | 51 | 4.56 (5.46) | 10 | 2.00 (1.94) | 25 | 5.68 (6.04) | 16 | 5.63 (6.52) |
| Heart rate | ||||||||
| Prefilm | 64 | 77.92 (9.56) | 14 | 74.83 (9.39) | 31 | 77.05 (9.59) | 19 | 81.46 (6.97) |
| Perifilm | 64 | 77.32 (9.46) | 14 | 74.48 (9.89) | 31 | 76.46 (10.18) | 19 | 80.12 (7.20) |
| Postfilm | 64 | 78.35 (9.21) | 14 | 74.65 (9.68) | 31 | 77.94 (9.42) | 19 | 81.73 (7.64) |
| Psychological states | ||||||||
| State anxiety (20–80) | ||||||||
| Prefilm | 64 | 35.95 (9.54) | 14 | 35.14 (9.79) | 31 | 36.55 (9.70) | 19 | 35.58 (9.55) |
| Perifilm | 64 | 49.20 (11.51) | 14 | 48.00 (12.30) | 31 | 49.90 (10.98) | 19 | 48.95 (12.30) |
| Postfilm | 64 | 41.67 (11.84) | 14 | 38.21 (10.45) | 31 | 43.23 (11.44) | 19 | 41.68 (13.41) |
| State dissociation (0–76) | ||||||||
| Prefilm | 64 | 4.95 (5.08) | 14 | 3.36 (2.90) | 31 | 6.19 (5.82) | 19 | 4.11 (4.71) |
| Perifilm | 64 | 7.39 (7.60) | 14 | 4.86 (4.15) | 31 | 8.29 (9.09) | 19 | 7.79 (6.75) |
| Postfilm | 64 | 5.52 (6.74) | 14 | 4.07 (4.46) | 31 | 6.06 (8.33) | 19 | 5.68 (5.20) |
| Fear (0–10) | ||||||||
| Prefilm | 64 | 1.37 (1.75) | 14 | 1.07 (1.38) | 31 | 1.65 (1.99) | 19 | 1.16 (1.57) |
| Perifilm | 64 | 3.34 (2.85) | 14 | 3.93 (2.92) | 31 | 3.26 (2.61) | 19 | 3.05 (3.24) |
| Postfilm | 64 | 1.33 (1.95) | 14 | 0.86 (1.46) | 31 | 1.52 (2.06) | 19 | 1.37 (2.11) |
| Calmness (0–10) | ||||||||
| Prefilm | 64 | 6.25 (2.61) | 14 | 6.57 (2.10) | 31 | 6.03 (2.69) | 19 | 6.37 (2.89) |
| Perifilm | 64 | 4.08 (2.72) | 14 | 3.86 (2.96) | 31 | 3.77 (2.47) | 19 | 4.74 (2.98) |
| Postfilm | 64 | 5.59 (2.66) | 14 | 6.07 (2.64) | 31 | 5.26 (2.48) | 19 | 5.80 (3.01) |
| Memory measures | ||||||||
| Intrusive memory | ||||||||
| Frequency_image | 64 | 3.94 (2.79) | 14 | 3.50 (4.33) | 31 | 3.97 (2.63) | 19 | 4.79 (3.65) |
| Frequency_thought | 64 | 0.92 (1.26) | 14 | 0.71 (1.07) | 31 | 1.06 (1.26) | 19 | 0.84 (1.43) |
| Vividness_image (1–10)b | 56 | 4.76 (2.18) | 10 | 5.38 (1.84) | 27 | 4.64 (2.17) | 17 | 4.60 (2.42) |
| Recognition memory | ||||||||
| Gist (0–15) | 64 | 11.92 (1.77) | 14 | 11.36 (1.74) | 31 | 12.03 (1.92) | 19 | 12.16 (1.50) |
| Detail (0–15) | 64 | 6.64 (1.80) | 14 | 6.79 (1.31) | 31 | 6.52 (1.84) | 19 | 6.74 (2.10) |
Note. BMI = body mass index; Frequency_image = frequency of intrusive images; Frequency_thought = frequency of intrusive thoughts; Vividness_image = vividness of intrusive images.
Only the participants who had had at least one traumatic experience answered this questionnaire.
Only the participants who had had at least one intrusive image answered this question.
The intrusive sequences in the film were readily identified by most of the participants, except for two whose intrusive images were too vague and difficult to specify. On average, materials from 2.08 (SD = 1.23) scenes in the trauma film intruded. The overall duration of the intrusive sequences reported by each participant ranged between 2 to 173 s (M = 47.09; SD = 40.40). T tests showed that intrusive images were significantly more frequently reported than thoughts, t(63) = 7.97, p < .001. Gist information was recognized significantly better than details, t(63) = 20.01, p < .001. Detail recognition memory was better for the scenes that intruded than those that did not, t(53) = 2.79, p < .01. However, the performance of gist recognition memory was not significantly different, t(53) = 1.49, p = .14. As for the relationships between the memory measures (see Table 2), the frequency of imagery intrusions was significantly positively correlated with detail, but not with gist recognition memory. A marginally significant partial correlation was found between the frequency of imagery intrusions and detail recognition memory after controlling for gist (r = .24, p = .06). Frequency of thought intrusion was not significantly correlated with either type of recognition memory.
Table 2.
Pearson's Correlation Coefficients Between Memory Measures and Heart Rate Changes
| Intrusive memory | Recognition memory | ||||||
|---|---|---|---|---|---|---|---|
| Frequency_image | Frequency_thought | Vividness_image | Gist | Detail | |||
| Intrusive memory | Frequency_image | – | – | – | – | – | |
| Frequency_thought | −.05 (64) | – | – | – | – | ||
| Vividness_image | .00 (56) | −.12 (56) | – | – | – | ||
| Recognition memory | Gist | .15 (64) | −.04 (64) | .18 (56) | – | – | |
| Detail | .27 (64)* | −.14 (64) | .16 (56) | .31 (64)* | – | ||
| ΔHR | Overall perifilm ΔHR | .08 (64) | −.17 (64) | .07 (56) | .07 (64) | −.02 (64) | |
| Intrusive sequence ΔHRa | −.35 (54)* | −.04 (54) | −.01 (54) | .05 (54) | −.40 (54)** | ||
Note. Numbers in the brackets indicate sample sizes. Frequency_image = frequency of intrusive images; Frequency_thought = frequency of intrusive thoughts; Vividness_image = vividness of intrusive images; ΔHR = HR change.
Only the participants who had had at least one intrusive image and were able to identify the intrusive sequence(s) in the trauma film were included in this analysis.
p < .05.
p < .01.
The overall perifilm HR change did not show any significant correlations with the memory measures (see Table 2). However, intrusive sequence HR change significantly and negatively correlated with frequency of imagery intrusion and detail recognition memory. The more reduction in HR during the intrusive relative to the nonintrusive sequences, the greater frequency of imagery intrusions and better recognition of details were. The correlation between intrusive sequence HR change and frequency of intrusive images was marginally significant after controlling for vividness level and frequency of intrusive thoughts (r = −.32, p = .05). The partial correlation between intrusive sequence HR change and detail recognition memory remained significant after controlling for gist recognition memory (r = −.42, p < .01).
Classification of Startle Groups
To categorize participants by sHR response, both two- and three-cluster solutions were applied in Ward's hierarchical cluster analysis. The former resulted in nonequivalent sample sizes (50 participants with sHR response and 13 without). The latter resulted in a group with exaggerated and long-lasting sHR (n = 14), a group with medium (n = 31), and a group with restricted sHR (n = 19). They were termed high startle group (HSG), medium startle group (MSG), and low startle group (LSG), respectively (see Figure 2) and were used in the following analyses. A 3 (Group) × 11 (Time: the 0- to 10-s interval after the white noise onset) mixed design ANOVA showed a significant Time × Group interaction, Greenhouse-Geisser (20, 610) = 14.57, p < .001, and main effects of time, Greenhouse-Geisser (10, 610) = 17.08, p < .001, and group, F(2,61) = 113.10, p < .001. The results indicated a significant distinction between the three groups in HR over the first 10 s after the startle probe.
Figure 2.
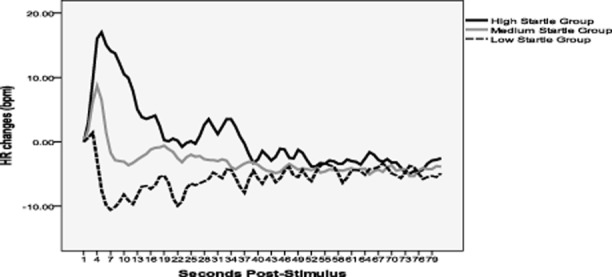
Startle heart rate response by group.
No significant difference was found between the three groups in gender (HSG: male = 4, female = 10; MSG: male = 20, female = 11; LSG: male = 9, female = 10, χ2(2) = 5.18, p = .08), age, F(2,61) = 1.51, p = .23, years of education, F(2,60) = .48, p = .62, BMI, F(2,61) = .09, p = .92, trait anxiety, F(2,60) = .55, p = .58, or PTSD symptoms, F(2,48) = 1.34, p = .27; See Table 1 for descriptive data. There were significant linear effects of group in baseline (i.e., prefilm) HR, F(1,61) = 4.03, p < .05, and trait dissociation, F(1,61) = 7.29, p < .01, with the LSG having higher baseline HR and reporting more trait dissociation than the HSG.
Group Differences in HR, Psychological States, and Memory
A 3 (Group) × 3 (Time: pre-, peri-, and postfilm) mixed design ANOVA on HR showed a significant quadratic effect of time, F(1,60) = 4.53, p < .05, with postfilm HR significantly higher than perifilm (p < .05). A significant linear effect of group was also found with the LSG presenting significantly higher HR than HSG (p < .05). The interaction between group and time was nonsignificant (F(4,120) = .59, p = .67). For the psychological states, all the quadratic effects of time were significant, F(1,61) = 81.48, p < .001 for state anxiety; F(1,61) = 19.27, p < .001 for state dissociation; F(1,61) = 49.83, p < .001 for fear; and F(1,61) = 46.12, p < .001 for calmness. Perifilm dissociation was significantly higher than pre- (p < .01) and postfilm (p < .001); perifilm calmness was significantly lower than pre- and postfilm (p < .001 for both). In contrast, perifilm fear was greater than pre- and postfilm (p < .001 for both). Perifilm anxiety was significantly higher than post- and prefilm (p < .001 for both). Moreover, postfilm anxiety was significantly greater than prefilm (p < .001). On the other hand, there were no significant linear effects of group or Group × Time interactions on any of these state measures (largest Greenhouse-Geisser (4, 122) = 2.01, p = .11). Scores on the memory measures were not significantly different between the three groups (largest F(2,61) = 1.41, p = .33; See Table 1 for descriptive data).
Moderating Role of sHR in the Relationship Between HR and Psychological States
To examine the moderating role of sHR, perifilm HR and group (i.e., dummy variables comparing either HSG or LSG with the other two groups) were entered in the first step, followed by their interactions in the second step to predict the different psychological states perifilm.1 As shown in Table 3, the interaction terms significantly increased the variance of perifilm anxiety, fear, and calmness explained by the model. In predicting perifilm dissociation, the second model as a whole did not significantly increase the variability accounted for. However, the interaction between perifilm HR and LSG (compared with the HSG and MSG) significantly contributed to the prediction of perifilm dissociation as well as all the other psychological states (i.e., anxiety, fear, and calmness). Additionally, both perifilm HR and its interaction with HSG (compared with the LSG and MSG) showed significant effects on predicting perifilm anxiety.
Table 3.
Multiple Regressions with Perifilm Psychological States as Dependent Variables and Perifilm Heart Rate, Group, and their Interaction as Independent Variables
| B | SE B | β | |
|---|---|---|---|
| Dependent variable: Perifilm anxiety | |||
| Step 1: R2 = .01, p = .94, df1 = 3, df2 = 60 | |||
| Constant | 49.96 | 2.12 | |
| Perifilm heart rate | .61 | 1.64 | .05 |
| Low startle group | −1.15 | 3.46 | −.05 |
| High startle group | −1.76 | 3.81 | −.06 |
| Step 2: ΔR2 = .13, p < .05, df1 = 2, df2 = 58 | |||
| Constant | 50.27 | 2.01 | |
| Perifilm heart rate | 4.36 | 2.03 | .35* |
| Low startle group | .14 | 3.37 | .01 |
| High startle group | −3.43 | 3.74 | −.12 |
| Perifilm heart rate × Low startle group | −10.72 | 4.26 | −.36* |
| Perifilm heart rate × High startle group | −7.99 | 3.79 | −.32* |
| Dependent variable: Perifilm dissociation | |||
| Step 1: R2 = .02, p = .76, df1 = 3, df2 = 60 | |||
| Constant | 2.26 | .29 | |
| Perifilm heart rate | .17 | .22 | .10 |
| Low startle group | .09 | .47 | .03 |
| High startle group | −.24 | .52 | −.06 |
| Step 2: ΔR2 = .09, p = .07, df1 = 2, df2 = 58 | |||
| Constant | 2.29 | .28 | |
| Perifilm heart rate | .53 | .28 | .31 |
| Low startle group | .30 | .47 | .09 |
| High startle group | −.31 | .52 | −.08 |
| Perifilm heart rate × Low startle group | −1.40 | .59 | −.35* |
| Perifilm heart rate × High startle group | −.49 | .53 | −.14 |
| Dependent variable: Perifilm fear | |||
| Step 1: R2 = .02, p = .72, df1 = 3, df2 = 60 | |||
| Constant | 32.83 | 5.19 | |
| Perifilm heart rate | 2.93 | 4.03 | .10 |
| Low startle group | −2.98 | 8.50 | −.05 |
| High startle group | 7.39 | 9.34 | .11 |
| Step 2: ΔR2 = .15, p < .01, df1 = 2, df2 = 58 | |||
| Constant | 33.44 | 4.88 | |
| Perifilm heart rate | 10.14 | 4.93 | .33* |
| Low startle group | 2.32 | 8.17 | .04 |
| High startle group | 7.05 | 9.07 | .10 |
| Perifilm heart rate × Low startle group | −32.86 | 10.33 | −.45** |
| Perifilm heart rate × High startle group | −6.35 | 9.21 | −.10 |
| Dependent variable: Perifilm calmness | |||
| Step 1: R2 = .03, p = .63, df1 = 3, df2 = 60 | |||
| Constant | 37.89 | 4.96 | |
| Perifilm heart rate | 1.75 | 3.85 | .06 |
| Low startle group | 9.07 | 8.12 | .15 |
| High startle group | 1.24 | 8.92 | .02 |
| Step 2: ΔR2 = .10, p < .05, df1 = 2, df2 = 58 | |||
| Constant | 37.22 | 4.78 | |
| Perifilm heart rate | −6.19 | 4.82 | −.21 |
| Low startle group | 6.42 | 8.00 | .11 |
| High startle group | 4.85 | 8.88 | .07 |
| Perifilm heart rate × Low startle group | 22.36 | 10.12 | .32* |
| Perifilm heart rate × High startle group | 17.14 | 9.02 | .29 |
Note. Low startle group = the low startle group compared against the high and medium startle group; High startle group = the high startle group compared against the low and medium startle group.
p < .05.
p < .01.
To clarify the above significant findings, the relationships between perifilm HR and psychological states were examined separately in different groups. As shown in Figure 3, while a trend level negative correlation between perifilm HR and dissociation was shown in the LSG (r = −.41, p = .08), the other two groups did not show the same pattern (r = .04, p = .90 for the HSG; r = .29, p = .11 for the MSG). In contrast, perifilm HR was significantly positively associated with anxiety among the MSG (r = .40, p < .05), but the associations in the HSG (r = −.29, p = .32) and LSG (r = −.36, p = .13) were in the opposite direction. In the LSG, perifilm HR was significantly negatively associated with fear (r = −.49, p < .05). However, a significant positive correlation between the two variables was found in the MSG (r = .39, p < .05), and the HSG (r = .13, p = .67) did not show a clear association. Finally, the patterns of correlation between perifilm HR and calmness in the HSG (r = .36, p = .21) and LSG (r = .38, p = .11) were found to be opposite to the MSG (r = −.25, p = .17; see Figure 3).
Figure 3.

Relationships between perifilm psychological states and heart rate by group.
Moderating Role of sHR in the Relationship between HR Changes and Intrusive Memories
Similar analyses were used to examine the effect of sHR in the relationship between overall perifilm HR change and the intrusive memory measures (i.e., frequency of intrusive images and thoughts, vividness of intrusive images). The second step significantly increased the variance in vividness of intrusive images explained by the model (ΔR2 = .18, p < .01) with the interaction between overall perifilm HR change and the LSG (compared with the HSG and MSG) being the significant predictor (β = .47, p < .01). For the LSG, a greater HR decrease perifilm was associated with less vivid intrusive images (r = .64, p < .01), whereas for the HSG (r = −.27, p = .45) and MSG (r = −.19, p = .35) significant correlations were not found (see Figure 4). No moderating effects of sHR were found in the relationships between overall perifilm HR change and both intrusion frequency measures (largest ΔR2 of the second step = .05, p = .44).
Figure 4.
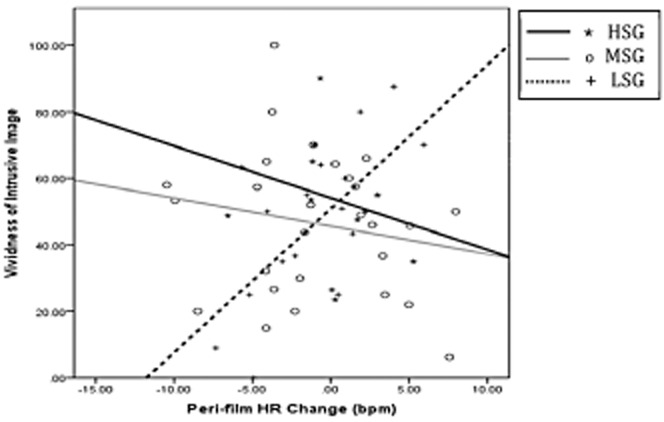
Relationships between vividness of intrusive image and overall perifilm heart rate change by group.
Discussion
The current study assessed sHR as a biological trait and adopted the trauma film paradigm to examine the role of sHR in the relationships between HR, psychological states, and memory. Overall, a significant correlation between decreased HR and increased intrusive trauma memory was found. A group of individuals showing suppressed, rather than increased, HR after a startle probe was identified. This individual difference in sHR was further shown to relate to diverse correlations between peritraumatic HR, psychological states, and intrusive memory.
Trauma Memory and Peritraumatic HR Reduction
Adopting the same paradigm and similar methodology, our data provide the first replication of an important previous finding (Holmes et al., 2004)—HR during the encoding phase of the intrusive film sequences is lower than it is during the nonintrusive sequences. Further, we showed for the first time that the extent of HR reduction during intrusive sequences correlated with the frequency of intrusive images and also with recognition memory for details. Consistent with the DRT, which distinguishes between detail memory linked to viewpoint-dependent images (S-reps) and gist memory linked to contextualized episodic memories (C-reps), the positive associations between HR reduction during intrusive sequences, frequency of intrusive images, and detail memory were independent of gist memory. Moreover, our results also support the notion that the correlates of intrusive images and thoughts tend to be different (cf. Hagenaars et al., 2010). Specifically, while the correlations between the frequency of intrusive images, HR, and detail recognition memory were significant, the correlations between intrusive thoughts and these variables were not significant. Additionally, two parameters of intrusions, namely, frequency and vividness, were examined separately in the current study. Interestingly, the correlation between the two was not significant, and they were related in different ways to changes in HR. The results add to recent evidence (Brewin & Langley, 2013) that the cognitive processes underlying the two parameters are different.
The current study failed to replicate Holmes et al.'s (2004) finding of a significant relationship between overall perifilm HR change and intrusion frequency. This may be due to the relatively smaller mean HR reduction (0.45 bpm) in the current study compared to the previous one (4.24 bpm). A factor contributing to the smaller HR reduction is likely to be the lower baseline HR (77.83 bpm) in the current study relative to the 81.94 bpm reported by Holmes et al. (2004). Presentation of the initial startle probe may have caused participants to be in a watchful state, resulting in this lowered baseline HR.
Individual Differences in sHR, Psychological States, and Trauma Memory
The current study assessed sHR as a physiological trait indicating different stress defense styles. For the first time, a group of individuals (the LSG) has been identified who react to an unexpected threat with an inhibited cardiovascular response instead of the typical startle response characterized by a sharp HR increase. These individual differences echo the dual defensive behaviors observed in animal threat responses (Bradley & Lang, 2000; Kaada, 1987) and the reduced startle response of women suffering from chronic interpersonal violence (Medina et al., 2001). Accordingly, the LSG may represent individuals tending to adopt a passive stress coping strategy. Our finding that the LSG reported higher trait dissociation supports this hypothesis. Interestingly, we found higher overall HR among the LSG than HSG, despite their suppressive sympathetic response to threat (the startle probe). This finding is consistent with previous studies showing more severe hyperarousal symptoms among people with a dissociative subtype of PTSD (Ginzburg et al., 2006), as well as a positive association between acute dissociative symptoms and salivary cortisol level in PTSD patients (Koopman et al., 2003). The implication is that increased basal stress responses coexist with inhibition of reactive stress responses.
Although the groups did not differ in their psychological responses to the trauma film, individual differences were found in the relationship between perifilm HR and the psychological states. Agreeing with the existing literature, a high level of HR in the MSG correlated with increased fear and anxiety, implying a readiness to take active defensive actions in a threatening situation (Graham & Clifton, 1966), whereas a low level of HR correlated with a relatively calmer state. In contrast, for the LSG, it is lower HR that is suggestive of greater subjective distress. The lower these individuals' HR, the more anxious, fearful, and dissociative they are. Accordingly, for the MSG, lower HR may be a sign of orientation and information gathering similar to the cognitive activities happening at the second stage of the defense cascade model (Bradley & Lang, 2000). However, for the LSG, low HR during the film viewing may indicate passive defense behavior that can be found in the final stage of the model when predators have arrived and active coping is perceived as unavailable or useless (Bradley & Lang, 2000). In contrast, the HSG group did not show a consistent pattern of response.
The patterns of sHR did not relate to diverse phenomena of intrusion or moderate their relationships with HR. An unexpected finding was that greater overall perifilm HR reduction in the LSG was associated with lower vividness of intrusive images. Given the finding of negative correlation between HR and dissociation in the LSG, this result suggests a link between greater dissociation and lower vividness among these individuals. It may be related to the study by Ginzburg and colleagues (2006), which included adult female survivors of childhood sexual abuse and found a group of individuals who were less bothered by intrusive memories but suffered from greater dissociation symptoms.
Limitations
There are a number of limitations in the current study. As discussed earlier, presentation of the startle stimulus may have affected the prefilm baseline HR and led to the differences with previous work (e.g., Holmes et al., 2004). However, as all participants had gone through the same procedures, its impact on the group effect and Group × Time interaction should be relatively small. Reliance on self-report diary measures entails some loss of accuracy. However, considering the fact that the average compliance rating in the current sample is satisfactory (9.3 on a 0–10 scale), this approach arguably has advantages over retrospective reports that average over longer periods such as a week. The sample size was small, especially after being separated into the three groups. Replication with bigger sample sizes is needed.
Perhaps the main issue is the adaptation of an analogue stimulus, the trauma film, and a nonclinical sample. This limitation may relate to the nonsignificant findings for group differences in memory and psychological state. For example, the nonsignificant difference in intrusion frequency, fear, and state dissociation between groups may be partly due to a floor effect. However, the use of a trauma film does fulfill diagnostic criteria A1 and A2 for PTSD in DSM-IV (APA, 1994) as the participants witnessed actual death and reported significant distress after viewing it. Moreover, it has been well established that the nature, amplifiers, and attenuators of intrusive memories for the trauma film are in line with those of intrusions that resulted from real traumas (see review by Holmes & Bourne, 2008). Because of these and the other advantages of the trauma film paradigm, such as enabling the investigation of peritraumatic phenomena and offering laboratory control, it has been recognized as a valid approach to studying trauma and PTSD (Holmes & Bourne, 2008). Nevertheless, future studies involving survivors of real-life traumatic events are needed before generalization of the findings can be made with greater confidence.
Footnotes
Multiple regressions with overall perifilm HR change and group entered in the first step, followed by their interactions in the second step, were also performed, but did not significantly predict the different psychological states perifilm. Detailed statistical results are available from the authors upon request.
References
- Adenauer H, Catani C, Keil J, Aichinger H. Neuner F. Is freezing an adaptive reaction to threat? Evidence from heart rate reactivity to emotional pictures in victims of war and torture. Psychophysiology. 2010;47:315–322. doi: 10.1111/j.1469-8986.2009.00940.x. doi: 10.1111/j.1469-8986.2009.00940.x. [DOI] [PubMed] [Google Scholar]
- Adolphs R, Tranel D. Buchanan TW. Amygdala damage impairs emotional memory for gist but not details of complex stimuli. Nature Neuroscience. 2005;8:512–518. doi: 10.1038/nn1413. doi: 10.1038/nn1413. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: Author; 1994. [Google Scholar]
- Bisby JA, Brewin CR, Leitz JR. Curran HV. Acute effect of alcohol on the development of intrusive memories. Psychopharmacology. 2009;204:655–666. doi: 10.1007/s00213-009-1496-5. doi: 10.1007/s00213-009-1496-5. [DOI] [PubMed] [Google Scholar]
- Blanchard EB, Hickling EJ, Galovski T. Veazey C. Emergency room vital signs and PTSD in a treatment seeking sample of motor vehicle accident survivors. Journal of Traumatic Stress. 2002;15:199–204. doi: 10.1023/A:1015299126858. [DOI] [PubMed] [Google Scholar]
- Bradley MM. Lang PJ. Measuring emotion: Behavior, feeling, and physiology. In: Nadel L, editor; Lane R, editor. Cognitive neuroscience of emotion. New York, NY: Oxford University Press; 2000. pp. 242–276. [Google Scholar]
- Bremner JD, Krystal JH, Putnam FW, Southwick SM, Marmar C, Charney DS. Mazure CM. Measurement of dissociative states with the clinician-administered dissociative states scale (CADSS) Journal of Traumatic Stress. 1998;11:125–136. doi: 10.1023/A:1024465317902. doi: 10.1023/A:1024465317902. [DOI] [PubMed] [Google Scholar]
- Brewin CR, Dalgleish T. Joseph S. A dual representation theory of posttraumatic stress disorder. Psychological Review. 1996;103:670–686. doi: 10.1037/0033-295x.103.4.670. [DOI] [PubMed] [Google Scholar]
- Brewin CR, Gregory JD, Lipton M. Burgess N. Intrusive images in psychological disorders: Characteristics, neural mechanisms, and treatment implications. Psychological Review. 2010;117:210–232. doi: 10.1037/a0018113. doi: 10.1037/a0018113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewin CR. Langley K. The contribution of involuntary memory to voluntary recall of emotional pictures. Manuscript submitted for publication; 2013. [Google Scholar]
- Brewin CR, Ma BYT. Colson J. Effects of experimentally induced dissociation on attention and memory. Consciousness and Cognition. 2013;22:315–323. doi: 10.1016/j.concog.2012.08.005. doi: 10.1016/j.concog.2012.08.005. [DOI] [PubMed] [Google Scholar]
- Brewin CR. Mersaditabari N. Experimentally-induced dissociation impairs visual memory. Consciousness and Cognition. 2013;22:1189–1194. doi: 10.1016/j.concog.2013.07.007. doi: 10.1016/j.concog.2013.07.007. [DOI] [PubMed] [Google Scholar]
- Bryant RA, Creamer M, O'Donnell M, Silove D. McFarlane AC. A multisite study of initial respiration rate and heart rate as predictors of posttraumatic stress disorder. Journal of Clinical Psychiatry. 2008;69:1694–1701. doi: 10.4088/jcp.v69n1104. doi: 10.4088/JCP.v69n1104. [DOI] [PubMed] [Google Scholar]
- Buckley B, Nugent N, Sledjeski E, Raimonde AJ, Spoonster E, Bogart LM. Delahanty DL. Evaluation of initial posttrauma cardiovascular levels in association with acute PTSD symptoms following a serious motor vehicle accident. Journal of Traumatic Stress. 2004;17:317–324. doi: 10.1023/B:JOTS.0000038480.87290.4a. doi: 10.1023/B:JOTS.0000038479.30903.ed. [DOI] [PubMed] [Google Scholar]
- Carlson EB. Putnam FW. An update on the dissociative experiences scale. Dissociation. 1993;6:16–27. [Google Scholar]
- Cuthbert BN, Lang PJ, Strauss C, Drobes D, Patrick CJ. Bradley MM. The psychophysiology of anxiety disorder: Fear memory imagery. Psychophysiology. 2003;40:407–422. doi: 10.1111/1469-8986.00043. doi: 10.1111/1469-8986.00043. [DOI] [PubMed] [Google Scholar]
- De Young AC, Kenardy JA. Spence SH. Elevated heart rate as a predictor of PTSD six months following accidental pediatric injury. Journal of Traumatic Stress. 2007;20:751–756. doi: 10.1002/jts.20235. doi: 10.1002/jts.20235. [DOI] [PubMed] [Google Scholar]
- Dubester KA. Braun BG. Psychometric properties of the dissociative experiences scale. Journal of Nervous and Mental Disease. 1995;183:231–235. doi: 10.1097/00005053-199504000-00008. doi: 10.1097/00005053-199504000-00008. [DOI] [PubMed] [Google Scholar]
- Ehlers A, Sündermann O, Böllinghaus I, Vossbeck-Elsebusch A, Gamer M, Briddon E. Glucksman E. Heart rate responses to standardized trauma-related pictures in acute posttraumatic stress disorder. International Journal of Psychophysiology. 2010;78:27–34. doi: 10.1016/j.ijpsycho.2010.04.009. doi: 10.1016/j.ijpsycho.2010.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foa EB. Posttraumatic stress diagnostic scale manual. Minneapolis, MN: National Computer Systems; 1995. [Google Scholar]
- Foa EB, Cashman L, Jaycox L. Perry K. The validation of a self-report measure of posttraumatic stress disorder: The posttraumatic diagnostic scale. Psychological Assessment. 1997;9:445–451. doi: 10.1037/1040-3590.9.4.445. [Google Scholar]
- Ginzburg K, Koopman C, Butler LD, Palesh O, Kraemer HC, Classen CC. Spiegel D. Evidence for a dissociative subtype of post-traumatic stress disorder among help-seeking childhood sexual abuse survivors. Journal of Trauma & Dissociation. 2006;7:7–27. doi: 10.1300/J229v07n02_02. doi: 10.1300/J229v07n02_02. [DOI] [PubMed] [Google Scholar]
- Graham FK. Clifton RK. Heart rate change as a component of the orienting response. Psychological Bulletin. 1966;65:305–320. doi: 10.1037/h0023258. doi: 10.1037/h0023258. [DOI] [PubMed] [Google Scholar]
- Griffin MG, Resick P. Mechanic M. Objective assessment of peritraumatic dissociation: Psychophysiological indicators. American Journal of Psychiatry. 1997;154:1081–1088. doi: 10.1176/ajp.154.8.1081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagenaars MA, Brewin CR, van Minnen A, Holmes EA. Hoogduin KAL. Intrusive images and intrusive thoughts as different phenomena: Two experimental studies. Memory. 2010;18:76–84. doi: 10.1080/09658210903476522. doi: 10.1080/09658210903476522. [DOI] [PubMed] [Google Scholar]
- Halligan SL, Michael T, Wilhelm FH, Clark DM. Ehlers A. Reduced heart rate responding to trauma reliving in trauma survivors with PTSD: Correlates and consequences. Journal of Traumatic Stress. 2006;19:721–734. doi: 10.1002/jts.20167. doi: 10.1002/jts.20167. [DOI] [PubMed] [Google Scholar]
- Hetzel-Riggin MD. Peritraumatic dissociation and PTSD effects on physiological response patterns in sexual assault victims. Psychological Trauma: Theory, Research, Practice and Policy. 2010;2:192–200. doi: 10.1037/a0019892. [Google Scholar]
- Hodson L, Harnden KE, Roberts R, Dennis AL. Frayn KN. Does the DASH diet lower blood pressure by altering peripheral vascular function? Journal of Human Hypertension. 2010;24:312–319. doi: 10.1038/jhh.2009.65. doi: 10.1038/jhh.2009.65. [DOI] [PubMed] [Google Scholar]
- Holmes EA. Bourne C. Inducing and modulating intrusive emotional memories: A review of the trauma film paradigm. Acta Psychologica. 2008;127:553–566. doi: 10.1016/j.actpsy.2007.11.002. doi: 10.1016/j.actpsy.2007.11.002. [DOI] [PubMed] [Google Scholar]
- Holmes EA, Brewin CR. Hennessy RG. Trauma films, information processing, and intrusive memory development. Journal of Experimental Psychology: General. 2004;133:3–22. doi: 10.1037/0096-3445.133.1.3. doi: 10.1037/0096-3445.133.1.3. [DOI] [PubMed] [Google Scholar]
- Kaada B. The sudden infant death syndrome induced by “the fear paralysis reflex”? Medical Hypotheses. 1987;22:347–356. doi: 10.1016/0306-9877(87)90029-6. [DOI] [PubMed] [Google Scholar]
- Kindt M, van den Hout M, Arntz A. Drost J. The influence of data-driven versus conceptually-driven processing on the development of PTSD-like symptoms. Journal of Behavior Therapy and Experimental Psychiatry. 2008;39:546–557. doi: 10.1016/j.jbtep.2007.12.003. doi: 10.1016/j.jbtep.2007.12.003. [DOI] [PubMed] [Google Scholar]
- Koopman C, Carrion V, Butler LD, Sudhakar S, Palmer L. Steiner H. Relationships of dissociation and childhood abuse and neglect with heart rate in delinquent adolescents. Journal of Traumatic Stress. 2004;17:47–54. doi: 10.1023/B:JOTS.0000014676.83722.35. doi: 10.1023/B:JOTS.0000014676.83722.35. [DOI] [PubMed] [Google Scholar]
- Koopman C, Sephton S, Abercrombie HC, Classen C, Butler LD, Gore-Felton C. Spiegel D. Dissociation symptoms and cortisol responses to recounting traumatic experiences among childhood sexual abuse survivors with PTSD. Journal of Trauma and Dissociation. 2003;4:29–46. doi: 10.1300/J229v04n04_03. [Google Scholar]
- Kraemer B, Mörgeli H, Roth H, Hepp U. Schnyder U. Contribution of initial heart rate to the prediction of posttraumatic stress symptom level in accident victims. Journal of Psychiatric Research. 2008;42:158–162. doi: 10.1016/j.jpsychires.2006.11.005. doi: 10.1016/j.jpsychires.2006.11.005. [DOI] [PubMed] [Google Scholar]
- Ladwig KH, Marten-Mittag B, Deisenhofer I, Hofmann B, Schapperer J, Weyerbrock S. Schmitt C. Psychophysiological correlates of peritraumatic dissociative responses in survivors of life-threatening cardiac events. Psychopathology. 2002;35:241–248. doi: 10.1159/000063825. doi: 10.1159/000063825. [DOI] [PubMed] [Google Scholar]
- López R, Poy R, Pastor MC, Segarra P. Moltó J. Cardiac defense response as a predictor of fear learning. International Journal of Psychophysiology. 2009;74:229–235. doi: 10.1016/j.ijpsycho.2009.09.006. doi: 10.1016/j.ijpsycho.2009.09.006. [DOI] [PubMed] [Google Scholar]
- Medina AM, Mejia VY, Schell AM, Dawson ME. Margolin G. Startle reactivity and PTSD symptoms in a community sample of women. Psychiatry Research. 2001;101:157–169. doi: 10.1016/s0165-1781(01)00221-9. [DOI] [PubMed] [Google Scholar]
- Metzger RL. A reliability and validity study of the State-Trait Anxiety Inventory. Journal of Clinical Psychology. 1976;32:276–278. doi: 10.1002/1097-4679(197604)32:2<276::AID-JCLP2270320215>3.0.CO:2-G. [Google Scholar]
- Milligan GW. Isaac PD. The validation of four ultrametric clustering algorithms. Pattern Recognition. 1980;12:41–50. [Google Scholar]
- Morgan CA. Grillon C. Acoustic startle in individuals with posttraumatic stress disorder. Psychiatric Annals. 1998;28:430–434. [Google Scholar]
- O'Donnell ML, Creamer M, Elliott P. Bryant RA. Tonic and phasic heart rate as predictors of posttraumatic stress disorder. Psychosomatic Medicine. 2007;69:256–261. doi: 10.1097/PSY.0b013e3180417d04. doi: 10.1097/PSY.0b013e3180417d04. [DOI] [PubMed] [Google Scholar]
- Ostrowski S, Christopher NC. Delahanty DL. Parental posttraumatic stress symptoms as a moderator of child's acute biological response and subsequent posttraumatic stress symptoms in pediatric injury patients. Journal of Pediatric Psychology. 2007;32:309–318. doi: 10.1093/jpepsy/jsl005. doi: 10.1093/jpepsy/jsl005. [DOI] [PubMed] [Google Scholar]
- Ozer EJ, Best SR, Lipsey TL. Weiss DS. Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin. 2003;129:52–73. doi: 10.1037/0033-2909.129.1.52. doi: 10.1037/1942-9681.S.1.3. [DOI] [PubMed] [Google Scholar]
- Rosen JB. Schulkin J. From normal fear to pathological anxiety. Psychological Review. 1998;105:325–350. doi: 10.1037/0033-295x.105.2.325. doi: 10.1037/0033-295X.105.2.325. [DOI] [PubMed] [Google Scholar]
- Sokolov EN. Neuronal models and the orienting reflex. In: Brazier MAB, editor. The central nervous system and behavior. New York, NY: Josiah Macy Jr. Foundation; 1960. pp. 187–276. [Google Scholar]
- Spielberger CD. State-Trait Anxiety Inventory: Bibliography. 2. Palo Alto, CA: Consulting Psychologists Press; 1989. [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene R, Vagg PR. Jacobs GA. Manual for the State-Trait Anxiety Inventory Form Y. Palo Alto, CA: Consulting Psychologists Press; 1983. [Google Scholar]
- Spitzer RL, Williams JBW, Gibbon M. First MB. Structured Clinical Interview for DSM-III-R Patient ed. Washington, DC: American Psychiatric Press; 1990. [Google Scholar]
- Tabachnick BG. Fidell LS. Using multivariate statistics. 3. New York, NY: Harper Collins; 1996. [Google Scholar]
- Turpin G. A psychobiological approach to the differentiation of orienting and defense responses. In: Kimmel HD, editor. The orienting reflex in humans. New York, NY: Erlbaum; 1979. pp. 259–267. [Google Scholar]
- Vaidyanathan U, Patrick CJ. Cuthbert BN. Linking dimensional models of internalizing psychopathology to neurobiological systems: Affect-modulated startle as an indicator of fear and distress disorders and affiliated traits. Psychological Bulletin. 2009;135:909–942. doi: 10.1037/a0017222. doi: 10.1037/a0017222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaile JC, Chowdhary S, Osman F, Ross HF, Fletcher J, Littler WA. Townend JN. Effects of angiotensin II (AT1) receptor blockade on cardiac vagal control in heart failure. Clinical Science. 2001;101:559–566. [PubMed] [Google Scholar]