

Neuroendocrine tumors (NETs) are mostly found in the gastrointestinal tract and the pancreas. The World Health Organization (WHO) classification (2010) has been widely used to categorize NETs [1]. In the digestive system, NETs including those found within the bile ducts, are classed as NET G1 (carcinoid, mitotic count of <2 per 10 high-power fields (HPF) and/or ≤2% Ki-67 index), NET G2 (mitotic count 2–20 per 10 HPF and/or 3%–20% Ki-67 index), NET G3 (neuroendocrine carcinoma, mitotic count of >20 per 10 HPF and/or >20% Ki-67 index), and mixed adenoneuroendocrine carcinoma (MANEC) [1]. NETs arising from the bile duct are rare, accounting for only 1.8% of gastroenteropancreatic NETs [2]. MANECs of the common bile ducts (CBDs) are extremely rare, and only a few cases have been reported thus far [3-5].
In this study, we report a case of MANEC arising from the mid CBD.
CASE REPORT
A 75-year-old man was admitted to the hospital with painless jaundice that had begun the previous week. He had undergone laparoscopic cholecystectomy four months previously due to gallbladder empyema. He had a history of prostate cancer which had been cured after radical prostatectomy 10 years prior. The patient was taking antihypertensive medication. He was neither a drinker nor a smoker and did not have any specific family history of any other diseases.
Physical examinations on admission were unremarkable, except for icteric scleras. Laboratory tests showed abnormal liver function tests with aspartate aminotransferase 196 U/L, alanine transaminase 428 U/L, total bilirubin 4.62 mg/dL, direct bilirubin 3.62 mg/dL, and gamma glutamyl transpeptidase 946 IU/L. The cancer antigen 19-9 level was 68.89 U/mL.
A abdominal computed tomography revealed intrahepatic duct dilatation and luminal narrowing of the mid CBD with diffuse wall thickening and enhancement (Fig. 1A). Upon endoscopic retrograde cholangiopancreatography (ERCP), there was a luminal narrowing (2 cm in length) in the proximal CBD with proximal ductal dilatation (Fig. 1B). Biopsy with forcep and brush cytology during ERCP revealed a few atypical cells with ulcer detritus that were suggestive of adenocarcinoma (Fig. 1C). On positron emission tomography, no significant abnormal fludeoxyglucose uptake was seen (Fig. 1D).
Fig. 1.
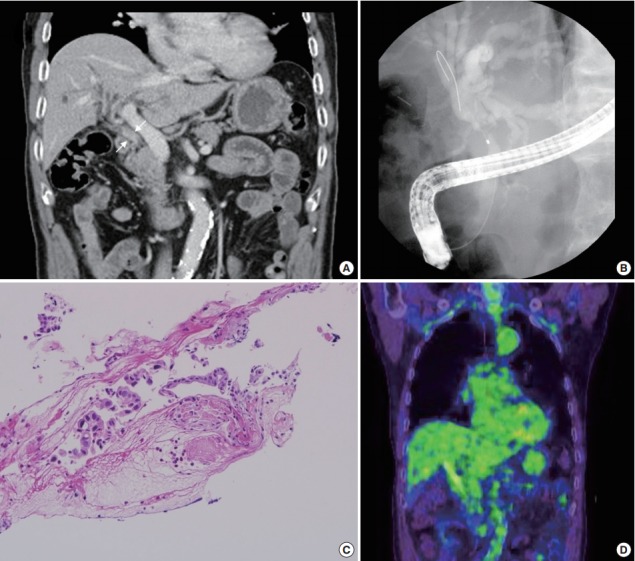
Study findings before surgery. (A) A portal phase image of a dynamic computed tomography scan shows luminal narrowing of the mid common bile duct (CBD) with diffuse wall thickening and enhancement (white arrows). (B) A filling defect in the CBD with proximal dilatation is noted upon endoscopic retrograde cholangiopancreatography (ERCP). (C) ERCP biopsy of the tumor reveals a few atypical cells with ulcer detritus, suggestive of adenocarcinoma. (D) Positron emission tomography shows no significant abnormal uptake.
The patient underwent CBD resection with Roux-en Y choledocojejunostomy and liver wedge resection. On the gross-section after fixation, an infiltrative, whitish tumor was noted at the CBD (Fig. 2A). Microscopically, the surface of the tumor was composed of moderately differentiated adenocarcinoma (Fig. 2B). In contrast, the tumor cells in the deep portion showed an infiltrative growth pattern and were composed of small round cells with hyperchromatic nuclei and scant cytoplasm (Fig. 2C). These infiltrative tumor cells stained positive for chromogranin A (Fig. 2D), synaptophysin (Fig. 2E), and CD56 (Fig. 2F), the markers for NET. Both adenocarcinoma and NET components occupied more than 30% of the tumor volume. The final diagnosis of the patient was MANEC (composite of moderately differentiated adenocarcinoma and small cell carcinoma). There was no lymphatic or vascular invasion.
Fig. 2.
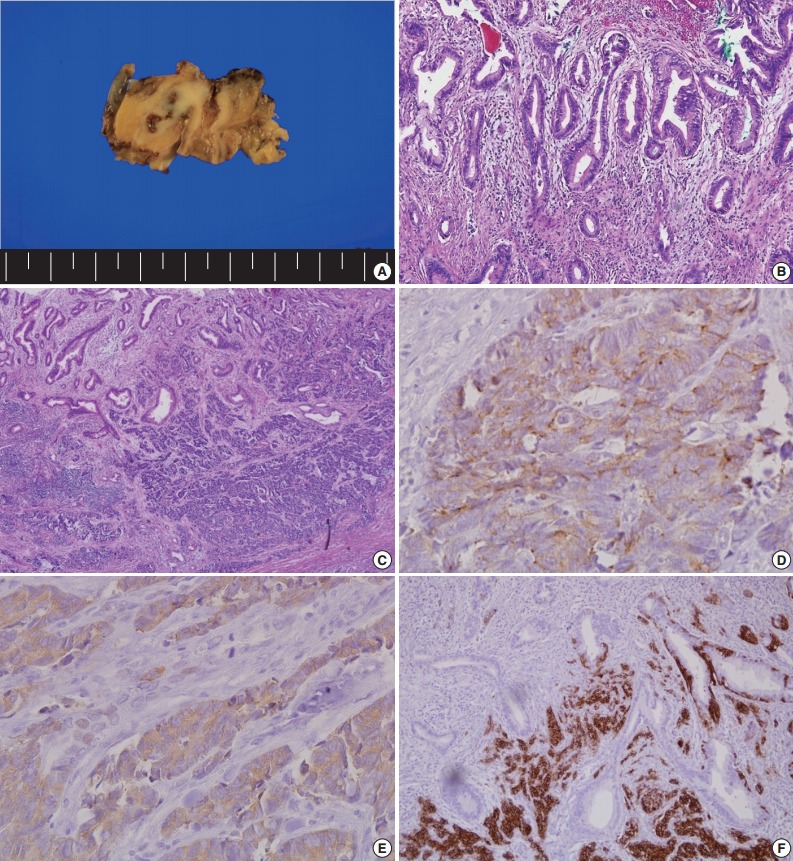
Pathologic findings after surgery. (A) Gross cross-sectional view of the tumor after fixation. (B) On the surface of the tumor, the tumor cells are composed of moderately differentiated adenocarcinoma. (C) The infiltrative tumor cells are small and round with hyperchromatic nuclei and scant cytoplasm. Immunohistochemical analysis for chromogranin (D), synaptophysin (E), and CD56 (F).
Five months after the procedure, the patient was readmitted to the hospital due to recurrent liver abscess. After percutaneous abscess drainage and antibiotic therapy, his condition improved. He continues to be followed-up and has shown no evidence of recurrence for 11 months after the operation.
DISCUSSION
MANEC is a subtype of NET that contains both gland-forming epithelial tumor cells and neuroendocrine cells [1]. By definition, both components must represent at least 30% of the tumor [1]. NETs that arise from the extrahepatic bile duct are very rare, occupying less than 1% of all NETs [6-8]. MANECs arising from the extrahepatic bile duct are extremely rare [7,8]. These types of tumor have a characteristic histology that includes an adenocarcinoma component at the surface and a neuroendocrine component in the areas of vascular and perineural invasion [3-5,9].
Because of their rarity and complexity, most MANECs of the bile duct are initially thought to be adenocarcinomas or NETs [3-5]. Our patient was also first diagnosed with cholangiocarcinoma by biopsy via ERCP, and the adenocarcinoma components were localized in the superficial layer.
An initial pathologic diagnosis of malignant biliary stricture is frequently made following a biopsy of the site. However, due to the limitation involved with obtaining adequate biopsy specimens, ERCP may fail to reach the neuroendocrine component, which is embedded in a deeper portion of the tumor. Therefore, the pathologic diagnosis of MANEC using a surgically resected specimen with immunohistochemical stainining for neuroendocrine markers (chromogranin, synaptophysin, and CD56) may be useful for the correct diagnosis [3].
Even in surgical specimens of biliary tract cancer, NETs and MANECs may be hidden inside the adenocarcinomatous components. A previous study examined 274 cases of surgically resected biliary tract cancer specimens and reported that 13 of 53 extrahepatic bile duct cancer cases contained neuroendocrine cells and two were newly diagnosed as MANEC [9]. Therefore careful attention and thorough examinations are needed for pathologists to accurately diagnose surgically resected biliary tumors, even when the tumor has been initially determined to be a cholangiocarcinoma via ERCP biopsy.
In general, the prognosis of biliary MANEC is poor. While the five-year survival rates of NET G1 and NET G2 of the gastroenteropancreatic tract are greater than 70%, the same survival rate of MANEC is about 40% [2]. Disease-related causes of death are most commonly located in the biliary tract (62.2%), while the rarest arise in the rectum (5.2%) [2].
The treatment algorithm of MANEC is not well established. As with other types of cancer, surgery may be the mainstay of the treatment of MANEC, and adjunctive therapy with chemotherapy, radiotherapy and somatostatin analogues can be considered according to the NEC type. It is also reasonable to treat MANEC in accordance with a more aggressive histology of the tumor [10]. For example, treat like adenocarcinoma in a MANEC with a well differentiated neuroendocrine component and an adenocarcinomatous component, and treat as poorly differentiated NET in a MANEC with poorly differentiated neuroendocrine component [10].
In conclusion, we present a case of MANEC of the CBD. Most MANEC cases, including this one, are initially diagnosed as cholangiocarcinoma. Therefore, the acquisition of a surgical specimen and thorough investigations by the pathologist are crucial to make the correct diagnosis in order to determine the best treatment and estimate the prognosis in extra-hepatic bile duct cancer.
Footnotes
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1.Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC Press; 2010. [Google Scholar]
- 2.Gastrointestinal Pathology Study Group of Korean Society of Pathologists. Cho MY, Kim JM, et al. Current trends of the incidence and pathological diagnosis of gastroenteropancreatic neuroendocrine tumors (GEP-NETs) in Korea 2000-2009: multicenter study. Cancer Res Treat. 2012;44:157–65. doi: 10.4143/crt.2012.44.3.157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Linder R, Dorfman T, Ben-Ishay O, Kakiashvili E, Velodavsky E, Kluger Y. Mixed neuroendocrine tumor of the common bile duct. JOP. 2013;14:71–3. doi: 10.6092/1590-8577/1225. [DOI] [PubMed] [Google Scholar]
- 4.Kim J, Lee WJ, Lee SH, et al. Clinical features of 20 patients with curatively resected biliary neuroendocrine tumours. Dig Liver Dis. 2011;43:965–70. doi: 10.1016/j.dld.2011.07.010. [DOI] [PubMed] [Google Scholar]
- 5.Baek IY, Chung YJ, Park MK, et al. A case of mixed adenoneuroendocrine carcinoma in common bile duct. Korean J Pancreas Biliary Tract. 2012;17:56–60. [Google Scholar]
- 6.Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer. 2003;97:934–59. doi: 10.1002/cncr.11105. [DOI] [PubMed] [Google Scholar]
- 7.Chamberlain RS, Blumgart LH. Carcinoid tumors of the extrahepatic bile duct: a rare cause of malignant biliary obstruction. Cancer. 1999;86:1959–65. [PubMed] [Google Scholar]
- 8.Sato K, Waseda R, Tatsuzawa Y, et al. Composite large cell neuroendocrine carcinoma and adenocarcinoma of the common bile duct. J Clin Pathol. 2006;59:105–7. doi: 10.1136/jcp.2005.028019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Harada K, Sato Y, Ikeda H, et al. Clinicopathologic study of mixed adenoneuroendocrine carcinomas of hepatobiliary organs. Virchows Arch. 2012;460:281–9. doi: 10.1007/s00428-012-1212-4. [DOI] [PubMed] [Google Scholar]
- 10.Hervieu V, Scoazec JY. Mixed endocrine tumors. Ann Pathol. 2005;25:511–28. doi: 10.1016/s0242-6498(05)86164-4. [DOI] [PubMed] [Google Scholar]