

Abstract
Background
Preclinical models show that an antiangiogenic regimen at low-dose daily (metronomic) dosing may be effective against chemotherapy-resistant tumors. We undertook a prospective, open-label, single-arm, multi-institutional phase II study to evaluate the efficacy of a “5-drug” oral regimen in children with recurrent or progressive cancer.
Procedure
Patients ≤21 years old with recurrent or progressive tumors were eligible. Treatment consisted of continuous oral celecoxib, thalidomide, and fenofibrate, with alternating 21-day cycles of low-dose cyclophosphamide and etoposide. Primary endpoint was to assess, within eight disease strata, activity of the 5-drug regimen over 27 weeks. Blood and urine angiogenesis markers were assessed.
Results
One hundred one patients were enrolled; 97 began treatment. Median age was 10 years (range: 191 days–21 years); 47 (49%) were female. Disease strata included high-grade glioma (HGG, 21 patients), ependymoma (19), low-grade glioma (LGG, 12), bone tumors (12), medulloblastoma/primitive neuroectodermal tumor (PNET, 8), leukemia (4), neuroblastoma (3), and miscellaneous tumors (18). Treatment was generally well tolerated; most common toxicities were hematologic. Twenty-four (25%) patients completed 27 weeks therapy without progression, including HGG: 1 (5%), ependymoma: 7 (37%), LGG: 7 (58%), medulloblastoma/PNET: 1, neuroblastoma: 1, and miscellaneous tumors: 7 (39%). Best response was complete response (one patient with medulloblastoma), partial response (12), stable disease (36), progressive disease (47), and inevaluable (1). Baseline serum thrombospondin levels were significantly higher in patients successfully completing therapy than in those who progressed (P = 0.009).
Conclusion
The 5-drug regimen was well tolerated. Clinical activity was demonstrated in some but not all tumor strata. Pediatric Blood Cancer 2014;61:636–642. © 2013 The Authors Pediatric Blood & Cancer Published by Wiley Periodicals, Inc.
Keywords: angiogenesis, drug resistance, pediatric oncology, phase II clinical trials
INTRODUCTION
The propensity of malignant cells to develop drug resistance is one of the major problems confronting cytotoxic strategies 1. Over 40 years ago, Judah Folkman proposed antiangiogenic therapy as an alternative approach to cancer treatment 2. Essentially all tissue growth is angiogenesis-dependent 3, and the genomic stability of host endothelial and vascular-progenitor cells targeted by antiangiogenic therapy should theoretically limit acquired resistance 4. In contrast to conventional cytotoxic therapy, which is classically given in an interval dose-intensive fashion to maximize cell kill and minimize resistance 5, sustained suppression of endothelial cell proliferation requires a low continuous (metronomic) dosing 6,7. Browder et al. 6 demonstrated that cyclophosphamide-resistant tumors can be killed in vivo by metronomic dosing of the same agent, and that this activity is attributable to antiangiogenesis. These findings have been replicated with other agents 7,8. An antiangiogenic strategy thus offers the possibility of greater long-term efficacy and tolerability than conventional cytotoxic therapy 9.
The mechanisms and pathways involved in new blood vessel recruitment are multiple and redundant. Opportunity exists for a malignancy to exploit these redundancies and bypass a unimodal antiangiogenic strategy 10,11. Combination antiangiogenic therapy, targeting non-overlapping aspects of neovascularization, may be a more effective means of overcoming treatment resistance.
We previously reported a pilot study that demonstrated feasibility and tolerability of an oral antiangiogenic regimen including thalidomide, celecoxib, and alternating 21 day cycles of low-dose oral cyclophosphamide and etoposide 12. We subsequently demonstrated that the PPAR-alpha agonist fenofibrate has antiangiogenic anti-tumor activity, and that the antiangiogenic effects of PPAR modulation are synergistic with COX2 inhibition and metronomic cytotoxic therapy in a preclinical model 8. Given the synergistic activity of fenofibrate without added toxicity in vivo, and in view of the poor prognosis and limited options in children with progressive disease, it was proposed that fenofibrate be added to the 4-drug regimen for the successor study. A single arm trial was proposed to assess the activity of this 5-drug combination.
We now report the results of the multi-center open-label prospective two-stage phase II trial of a multi-agent oral antiangiogenic/metronomic “5-drug” regimen for children with recurrent or progressive cancer. Treatment consisted of alternating 21-day cycles of low-dose oral cyclophosphamide and etoposide, with continuous oral thalidomide, celecoxib, and fenofibrate. The primary objective of the study was to assess the efficacy of this oral antiangiogenic/metronomic regimen within eight different disease strata in children with recurrent disease.
METHODS
The study was initiated at 11 centers in the United States. Institutional Review Board approval was obtained at all participating institutions. A data-safety monitoring committee oversaw the conduct of the study. Eligible patients were ≤21 years with evaluable recurrent or progressive tumors for which no curative therapy remained, Karnofsky/Lansky performance status ≥50, estimated life expectancy >2 months, no significant underlying organ disease, and adequate organ function, defined as serum creatinine <1.5 mg/dl, total bilirubin ≤1.5 mg/dl, transaminases and alkaline phosphatase ≤3 times normal, hemoglobin ≥8.0 g/dl, platelets >75,000/mm3, and absolute neutrophil count >1,000/mm3. Patients could not receive concurrent radiation or chemotherapy, nor could they have received prior oral low-dose etoposide or cyclophosphamide. Use of prior standard-dose intravenous etoposide/cyclophosphamide was permitted. Patients with non-progressive refractory disease were not eligible.
Treatment
Treatment consisted of daily oral thalidomide and fenofibrate, twice-daily oral celecoxib, and alternating 21-day cycles of low-dose oral etoposide and cyclophosphamide (Table1). Thalidomide was initiated at a lower dose to allow acclimatization to sedative effects; this was not related to a dose-finding study. Planned treatment duration was 27 weeks. Continuation of treatment beyond 27 weeks in patients with responsive or stable disease was permitted at the discretion of the treating institution; data regarding treatment continuation beyond 27 weeks was not uniformly collected. Dose reductions or interruptions were permitted at the individual investigator's discretion for clinically significant toxicities. Patients with clinically significant grade 3 or 4 toxicities that did not resolve with dose adjustment were removed from study. Following termination of study therapy, patients were followed for survival and disease status.
Table I.
5-Drug Oral Regimen: Dosing Schedule
| Medication | Dosing schedule |
|---|---|
| Continuous | |
| Thalidomide | Start at 3 mg/kg (rounded to nearest 50 mg) daily |
| Increase dose weekly by 50 mg as tolerated to 24 mg/kg (max 1,000 mg) daily | |
| Celecoxib | <20 kg: 100 mg twice daily |
| 20–50 kg: 200 mg twice daily | |
| >50 kg: 400 mg twice daily | |
| Fenofibrate | 90 mg/m2 (max 200 mg) daily |
| Alternating 21 day cycles | |
| Etoposide | 50 mg/m2 daily for 21 days |
| Cyclophosphamide | 2.5 mg/kg (max 100 mg) daily for 21 days |
Patients with history of significant myelosuppression with prior therapy initiated etoposide at 35 mg/m2 day and escalated to 50 mg/m2 as tolerated.
Disease Evaluation
As appropriate for tumor type and location, gadolinium-enhanced MRI and other imaging modalities were performed at study entry, every 9 weeks during therapy, and at study termination. Best response was regarded as best response at any single assessment. Response was defined as follows: complete resolution of all demonstrable tumor, complete response (CR); ≥50% decrease in the product of the two maximum perpendicular diameters relative to the baseline evaluation, partial response (PR); <50% decrease and <25% increase in product of diameters, stable disease (SD); and ≥25% increase in product of diameters, development of new areas of disease, or disease-attributable clinical deterioration or death, progressive disease (PD). For patients with leukemia PD was defined as ≥25% or ≥5,000 cells/mm3 increase in number of circulating cells, development of extramedullary disease, or other clinical evidence of progression.
Statistical Design
Patients were accrued to one of seven disease strata: leukemia/lymphoma, bone tumors, neuroblastoma, high-grade glioma, low-grade glioma, ependymoma, and medulloblastoma/PNET. Patients whose disease did not fall within these strata were accrued to an eighth “miscellaneous” stratum. The primary endpoint of the study was to assess, within each stratum, the activity of the 5-drug regimen given over a 27-week period. A favorable outcome was defined as completion of 27 weeks therapy without tumor progression. A two-stage design was implemented for each stratum. If none of the first 10 subjects in a stratum were able to complete 27 weeks therapy without disease progression, enrollment to that stratum was terminated. If at least one patient successfully completed 27 weeks of therapy, up to 10 additional patients were allowed to be accrued to the stratum. Three or more patients completing 27 weeks of treatment without disease progression was defined as a favorable outcome. With this design, the probability of a favorable outcome given a true success rate of 30% was 0.95, and 0.07 given a true rate of 5%. Secondary endpoints included objective response rate; overall survival (OS), defined as time from date of treatment initiation to date of death from any cause; and progression-free survival (PFS), defined as time from date of treatment initiation to date of either death from any cause or disease progression, whichever occurred first. Patients were censored at date of last known contact for OS, and date of last disease assessment for PFS. Patients who started a new regimen in absence of PD were censored at time of changing treatment for estimation of PFS.
Patient baseline characteristics were summarized as number (percentage) of patients for categorical endpoints and median (range) for continuous endpoints. Exact two-stage binomial 90% confidence intervals (CI) were reported. Comparisons between groups were performed using Fisher's exact test for binary endpoints and Wilcoxon rank sum test for continuous endpoints. A repeated measurement analysis using mixed models was performed to evaluate the tempo of changes in correlative markers of angiogenesis. The Kaplan–Meier method was used to estimate time-to-event secondary endpoints. All P values are two-sided. Statistical analyses were performed using SAS statistical software (version 9.2, SAS Institute, Inc., Cary, NC).
Surrogate Marker Analysis
Blood and urine samples were requested before therapy and every ninth week. VEGF, bFGF, endostatin, and thrombospondin-1 levels were evaluated from serum, plasma, and urine using commercially available ELISA kits (VEGF and bFGF: R&D Systems, Minneapolis, MN; endostatin and thrombospondin: CytImmune Sciences, Inc., College Park, MD) in accordance with the manufacturers' recommended methodology.
RESULTS
The study was open to accrual from January 7, 2005 through March 6, 2009, and enrolled 101 patients; 97 began treatment. Accrual goals were met for the high-grade glioma stratum. In low-grade glioma, ependymoma, and miscellaneous tumors strata the number of responses allowed criteria for positive activity to be met before 20 patients had been enrolled; the statistical team therefore allowed early study completion. Accrual to the bone tumor stratum was terminated after the first stage due to lack of efficacy in the first 10 patients; two additional patients were enrolled while response assessment for the first stage was still ongoing. Accrual to leukemia/lymphoma, neuroblastoma, and medulloblastoma/PNET strata was limited due to prominent competing trials for these diseases during the study time-period. Patient characteristics are summarized in Table2.
Table II.
Patient Characteristics
| Characteristic | Frequency (%) |
|---|---|
| Gender | |
| Male | 50 (51.5%) |
| Female | 47 (48.5%) |
| Age (years) | |
| Median | 10 |
| Range | (191 days–21 years) |
| Disease strata/diagnosis | |
| Leukemia/lymphoma | 4 |
| ALL | 2 |
| AML | 2 |
| Bone tumor | 12 |
| Osteosarcoma | 8 |
| Ewing sarcoma | 4 |
| Neuroblastoma | 3 |
| High grade glioma | 21 |
| Diffuse pontine glioma | 6 |
| Glioblastoma | 9 |
| Anaplastic astrocytoma | 3 |
| Anaplastic oligodendroglioma | 3 |
| Low grade glioma | 12 |
| Optic pathway/hypothalamic glioma | 8 |
| Oligodendroglioma | 1 |
| Other low grade glioma | 3 |
| Ependymoma | 19 |
| Medulloblastoma/PNET | 8 |
| Medulloblastoma | 6 |
| Pineoblastoma | 1 |
| Supratentorial PNET | 1 |
| Miscellaneous tumors | 18 |
| CNS | |
| Choroid plexus carcinoma | 2 |
| Atypical teratoid/rhabdoid tumor | 2 |
| Neurocytoma | 1 |
| Anaplastic glioneuronal tumor | 1 |
| Chordoma | 1 |
| Atypical meningioma | 1 |
| Non-germinomatous germ cell tumor | 1 |
| Non-CNS | |
| Wilms tumor | 3 |
| Hepatocellular carcinoma | 2 |
| Rhabdomyosarcoma | 2 |
| Epithelioid sarcoma | 1 |
| Lymphangioma | 1 |
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; PNET, primitive neuro-ectodermal tumor; CNS, central nervous system.
Clinical Outcome
Twenty-four subjects (25%, [90% CI 18%, 33%]) successfully completed 27 weeks of the 5-drug regimen without PD or significant toxicity. Sixty-five (67%, [90% CI 58%, 75%]) discontinued therapy due to PD, including three who died of disease while on study. One patient died due to complications of acute infection. Two (2%, [90% CI 0%, 6%]) discontinued therapy due to toxicity. Five (5%, [90% CI 2%, 11%]) withdrew consent due to patient/family preference. Reasons for treatment discontinuation by strata are shown in Supplementary Table I. The 27-week OS was 60% (90% CI 52%, 68%). Best response was CR (1), PR (12), SD (36), PD (47), and not evaluable (1). Favorable outcome was seen in ependymoma, low-grade glioma, and miscellaneous tumors strata (Table3).
Table III.
Clinical Outcomes by Disease Strata
| Best response | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Stratum | N | CR | PR | SD | PD | NE | Completed 27 weeks therapy | ||
| High grade glioma | 21 | — | 1 | 7 | 13 | — | 1 (5%) | ||
| Ependymoma | 19 | — | 2 | 10 | 7 | — | 7 (37%) | ||
| Low grade glioma | 12 | — | 4 | 5 | 3 | — | 7 (58%) | ||
| Bone tumors | 12 | — | — | 1 | 10 | 1 | — | ||
| Medulloblastoma/PNET | 8 | 1 | 1 | 1 | 5 | — | 1 (13%) | ||
| Leukemia | 4 | — | — | 1 | 3 | — | — | ||
| Neuroblastoma | 3 | — | — | 2 | 1 | — | 1 (33%) | ||
| Miscellaneous | 18 | — | 4 | 9 | 5 | — | 7 (39%) | ||
| Miscellaneous CNS Tumors | 9 | — | 3 | 5 | 1 | — | 5(56%) | ||
| Miscellaneous non-CNS tumors | 9 | — | 1 | 4 | 4 | — | 2(22%) | ||
CNS, central nervous system; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; NE, not evaluable. One patient with anaplastic glioneuronal tumor (miscellaneous CNS tumors strata) and best response SD sustained a CR during continuation therapy.
Nine (47%) ependymoma patients had metastatic disease at time of enrollment. Primary tumor location was supratentorial (N = 3), infratentorial (N = 13), and spinal (N = 3). All had received at least one prior course of radiation, and a median of 1 prior course of chemotherapy. Seven (37% [90% CI 19%, 58%]) completed therapy with SD or better. Two-year PFS and OS for patients with ependymoma were 34% (90% CI 16%, 52%) and 43% (90% CI 23%, 61%) (Fig. 1). Long-term (>3 year) survivors included two with metastatic disease.
Figure 1.
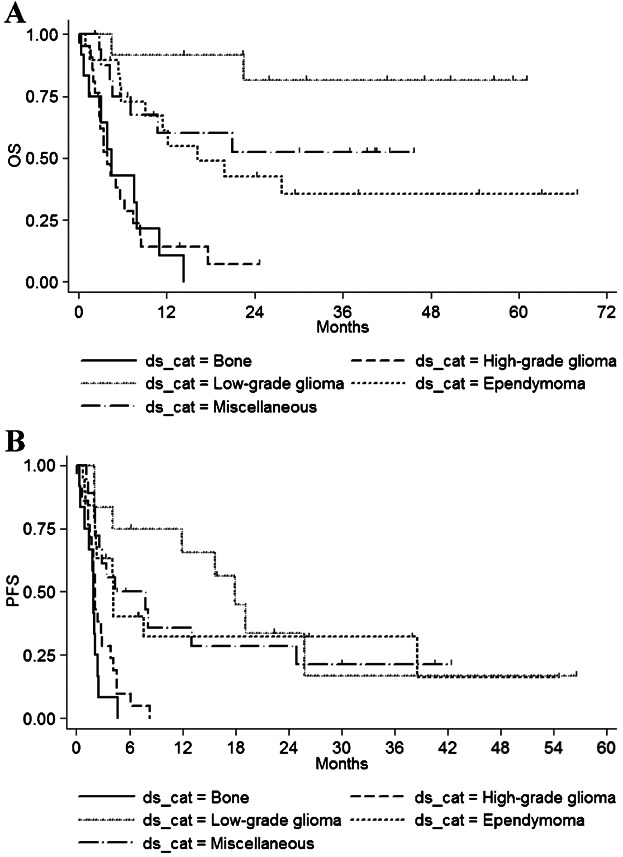
Overall survival (A) and progression free survival (B) by disease strata.
Low-grade glioma patients had received a median of 2 prior chemotherapy regimens. Four (33%) had received prior irradiation. Prior chemotherapy included one or more carboplatin-containing regimens (N = 10), temozolomide (N = 7), procarbazine and nitrosourea-containing regimens (N = 5), and vinblastine (N = 2). Three patients (25%) experienced PD within the first 9 weeks of study. The remaining nine patients (75%) had best response of SD or better. Two came off study before 27 weeks with SD, because of toxicity (N = 1) or to undergo surgical debulking of residual stable tumor (N = 1). The remaining 7 (58% [90% CI 32%, 82%]) completed therapy without PD. Two-year PFS and OS for patients with low-grade glioma were 33% (90% CI 11%, 57%) and 83% (90% CI 54%, 94%) (Fig. 1).
Responses among patients in the miscellaneous stratum included one patient with anaplastic glioneuronal tumor who completed study therapy with SD and demonstrated a subsequent sustained CR. One patient each with neurocytoma and chordoma completed therapy with PR. One patient each with mixed malignant germ cell tumor, meningioma, hepatocellular carcinoma, and lymphangioma completed therapy with SD. In addition, one patient with choroid plexus carcinoma demonstrated a PR, but came off study before 27 weeks due to patient/family preference.
Response rate was unfavorable in high-grade glioma and bone tumor strata (Table3 and Fig. 1). Of 21 evaluable patients with high-grade glioma, one patient (5%, [90% CI 0–21%]) with secondary GBM and a prior history of medulloblastoma completed 27-week study therapy with SD. Eleven of 12 bone tumor patients were evaluable for disease response. All, including three with Ewing sarcoma and eight with osteosarcoma, had metastatic disease with pulmonary involvement at the time of enrollment. All experienced PD during the treatment period, most (91%) within the first 9 weeks of therapy.
Accrual to three disease strata—medulloblastoma/PNET, leukemia/lymphoma, and neuroblastoma—was inadequate for response assessment. Three of four leukemia patients experienced disease progression shortly after initiating therapy. No lymphoma patients were enrolled. Eight patients in the PNET/medulloblastoma stratum included six patients with medulloblastoma; three medulloblastoma patients had best response of SD or better, including one who demonstrated a CR. Of three patients with neuroblastoma, one completed therapy with SD.
Toxicities
Treatment was well tolerated overall in the majority of patients. The most common toxicities were hematologic: 32% developed grade 4 neutropenia (ANC <500/mm3), 22% developed grade 3–4 anemia (hemoglobin <8 g/dL), and 5% developed grade 4 thrombocytopenia (platelets <25,000/mm3). Febrile neutropenia occurred in 11%. Neutropenia incidence was similar across strata. Dose reductions or interruptions were permitted at the individual investigator's discretion. Interruption of one or more drugs due to toxicity occurred at least once in 43 patients (44%). Toxicities and dose interruptions are summarized in Supplementary Tables II and III. There was one toxic death: a patient with recurrent Ewing sarcoma developed Enterococcus faecalis bacteremia with neutropenia in the fourth week of therapy, suffered progressive clinical deterioration with acute respiratory distress syndrome, and subsequently expired. Two other patients came off study due to toxicity: one with neutropenia and transaminase elevation during the second week of therapy, and one with rash. In both cases, toxicity resolved upon discontinuation of therapy.
The study did not include uniform assessment of long-term toxicities. One second malignancy has been reported in an ependymoma patient treated with the 5-drug regimen for 21 months, who developed t(8;21) acute myelogenous leukemia (AML) 26 months after study entry. No other second malignancies have been reported.
Correlative Studies
Markers of angiogenesis were obtained in a patient subset. Baseline serum TSP-1 levels were available for 52 patients (54%), including 17 who completed therapy and 35 with PD. Serum TSP-1 levels were significantly higher in patients who completed therapy than in non-completers (median 9,163 ng/mL vs. 4,299 ng/mL, P = 0.009). Baseline VEGF, bFGF, and endostatin levels were not significantly different in study completers compared to non-completers (Supplementary Table IV). A significant difference was seen in the slope of urine endostatin level over time: level remained stable in patients who completed therapy, but decreased over time in non-completers (P = 0.03, repeated measures model). Analysis of correlative findings was limited by intra-patient variability.
DISCUSSION
Metronomic therapy is defined as sustained low-dose administration of chemotherapeutic agents 13. Its development as a therapeutic modality was prompted by the in vivo observation that tumors resistant to dose-intense therapy would respond to the same agents at low continuous dosing 6. The concentrations achieved by metronomic dosing are typically well below concentrations required for direct tumor-cell kill. Instead, metronomic therapy exerts its primary effect on the host cells of the tumor microenvironment, including pericytes, endothelium, mesenchymal cells, and inflammatory cells 13. While several mechanisms of action have been proposed and may play a role, antiangiogenesis is believed to be the most important 6–8.
VEGF blockade as a unimodal antiangiogenic strategy has resulted in only modest clinical success. This can be explained in part by the multiplicity and redundancy of mechanisms involved in tumor-induced angiogenesis 11. Simultaneous inhibition of multiple pro-angiogenic pathways may be a more effective strategy.
Several small pilot studies have evaluated the feasibility of various antiangiogenic multi-drug combinations 12,14–16 The rationale for the combination of thalidomide, celecoxib, and low-dose etoposide and cyclophosphamide has previously been described 12. The inclusion of the PPAR-alpha agonist fenofibrate was prompted by the preclinical observation that PPAR modulation acts synergistically with COX-2 inhibition and low-dose etoposide to inhibit antiangiogenesis 8. In a clinical trial of retinoids in patients with cutaneous T cell lymphoma, it was incidentally noted that response rate in patients who received concurrent fenofibrate to control hyperlipidemia was 90%, compared to 48% in those treated without fenofibrate 17. PPAR ligands are involved in lipid metabolism 18, but also inhibit VEGF-mediated migration of endothelial cells 19 and decrease microvessel density within intimal tissues in animals 20. We have previously demonstrated that fenofibrate's antitumor activity is attributable to its antiangiogenic effect 21.
The 5-drug regimen was well tolerated in this heavily pre-treated population. There was one non-disease-related death, in a patient with neutropenia, bacteremia, and multi-organ failure. Overall, the cumulative incidence of severe neutropenia, the most common toxicity, compared favorably to that seen in other low-intensity regimens 22,23. Seven percent of patients came off study either due to toxicity (2%) or patient/family preference (5%).
One previously irradiated patient who received the 5-drug regimen for nearly 2 years developed AML characterized by a t(8;21) translocation within months of treatment completion. The t(8;21) translocation is primarily associated with de novo AML and associated with a favorable prognosis. Therapy-associated t(8;21) AML has been reported as a rare event, with a median latency of 37 months 24. The incidence of second malignancy after prolonged low-dose topoisomerase or alkylator therapy is not well defined.
Clinical benefit, including PR or sustained stabilization of previously progressive disease, was seen for both ependymoma and low-grade glioma. This confirms observations in the pilot feasibility study testing a similar (4-drug) regimen. That study, which primarily evaluated toxicity and was not powered for disease-specific efficacy evaluation, included one patient with low grade glioma who demonstrated a PR, and five patients with ependymoma who demonstrated PR (2), SD (2), and PD (1) 12. Other reports of favorable outcome for recurrent low-grade glioma treated with metronomic vinblastine 22 or with bevacizumab and irinotecan 25 and responses in some cases of recurrent ependymoma treated with low-dose oral etoposide 26 support the validity of an antiangiogenic strategy in these diseases. The miscellaneous tumors disease stratum also showed a favorable outcome. Individual diseases showing PR and/or sustained SD included both CNS tumors (anaplastic glioneuronal tumor, neurocytoma, chordoma, germ cell tumor, meningioma, choroid plexus carcinoma) and non-CNS tumors (hepatocellular carcinoma, lymphangioma). Further investigation for these diseases may be warranted. Accrual to leukemia, neuroblastoma, and medulloblastoma/PNET strata was limited, primarily due to prominent competing trials for these diseases during the study time-period. Rapid progression in three leukemia patients suggests that this is not a viable strategy for leukemia. Favorable outcomes in individual patients with medulloblastoma and neuroblastoma are intriguing. Sustained responses in a majority of medulloblastoma patients treated with the 5-drug regimen and concurrent intravenous bevacizumab and intrathecal therapy were recently reported in a pilot study 27
The 5-drug regimen was not effective in the treatment of high-grade glioma: only 1 of 21 subjects with high-grade glioma completed 27 weeks therapy without PD. Outcome in the treatment of bone tumors was likewise unpromising: none of 12 subjects with bone tumors completed study therapy. Interpretability of findings is limited by the heterogeneity of this stratum, which included eight subjects with osteosarcoma and only three evaluable patients with Ewing sarcoma, all of whom had advanced disease with significant tumor burden.
We chose tumor non-progression rather than response as the primary endpoint for this study. This reflects the unique mechanism of action and intended effect of a metronomic strategy, as well as a conceptual shift in goal for many currently incurable malignancies: away from cancer eradication, and towards the effective redefinition of cancer as a chronic disease 28. We chose 27 weeks as the minimum treatment duration. This reflects what we suggest is a minimum interval required, in the setting of active measurable disease progression at the time of treatment initiation, to differentiate disease stabilization from continued slow progression, especially in typically slow-growing tumors such as low-grade glioma.
Baseline serum TSP-1 was higher in patients who successfully completed therapy than in patients with PD. This replicates previous findings12. TSP-1 is a modulator of angiogenesis, induces endothelial cell apoptosis in vivo 29 and may play a role in mediating the antiangiogenic activity of metronomic chemotherapy 30. We hypothesize that TSP-1 elevation may be associated with increased tumor susceptibility to antiangiogenic therapy. Variability in response to antiangiogenic regimens suggests the existence of distinct angiogenic subtypes. Prospective systematic incorporation of imaging and tissue evaluation into future trials may facilitate better understanding of antiangiogenic resistance, and ultimately open the possibility of biologically tailored (“personalized”) antiangiogenic strategies.
Limitations of this study included lack of central review of imaging or pathology. In addition, toxicities were recorded only during the 27 weeks of study therapy. Systematic monitoring of late toxicities and incorporation of comparative quality-of-life metrics will be an important component of future disease-specific trials.
Comparison of the 5-drug regimen with other historical options was not an objective of this study. For most pediatric malignancies, including ependymoma, no effective salvage regimen has been previously established. Several chemotherapeutic approaches have shown benefit for progressive low-grade glioma, although none is curative and all involve intravenous drug administration. Further evaluation, ideally in a randomized large two-arm phase III setting, is needed to establish comparative disease-specific efficacy. Strategies combining this multi-drug anti-angiogenic with conventional cytotoxic or newer biologic regimens will also be an important focus of future research. Encouraging results were seen in a recent multicenter European study that tested a multi-drug oral and intravenous anti-angiogenic regimen in combination with retinoic acid 31.
In conclusion, this phase II study showed that the 5-drug oral antiangiogenic regimen was feasible, with a favorable toxicity profile. Clinical benefit was seen in patients with low-grade glioma and ependymoma, as well as in a miscellaneous tumors stratum. Further evaluation in disease-specific trials is planned.
Acknowledgments
We would like to thank Alex's Lemonade Stand Foundation for Childhood Cancer, the Stop & Shop Pediatric Brain Tumor Research Fund, and the Pediatric Brain Tumor Research and Clinical Fund for their generous support. Additional support for data management was provided by Celgene Pharmaceutical Corporation. Participating institutions included NYU Langone Medical Center, New York; Lurie Children's Hospital, Chicago; St. Louis Children's Hospital, St. Louis; Connecticut Children's Medical Center, Hartford; UMDNJ-Robert Wood Johnson University Hospital, New Brunswick; Miami Children's Hospital, Miami; Penn State Hershey Children's Hospital, Hershey; Children's Hospital and Clinics of Minnesota, Minneapolis/St. Paul; Hasbro Children's Hospital, Providence; Maine Medical Center, Portland; and Dana-Farber/Children's Hospital Cancer Center, Boston.
Supporting Information
Additional Supporting Information may be found in the online version of this article at the publisher's web-site.
REFERENCES
- 1.Al-Lazikani B, Banerji U, Workman P. Combinatorial drug therapy for cancer in the post-genomic era. Nat Biotechnol. 2012;30:679–692. doi: 10.1038/nbt.2284. [DOI] [PubMed] [Google Scholar]
- 2.Folkman J. Tumor angiogenesis: Therapeutic implications. N Engl J Med. 1971;285:1182–1186. doi: 10.1056/NEJM197111182852108. [DOI] [PubMed] [Google Scholar]
- 3.Folkman J. How is blood vessel growth regulated in normal and neoplastic tissue? G.H.A. Clowes memorial Award lecture. Cancer Res. 1986;46:467–473. [PubMed] [Google Scholar]
- 4.Rich JN, Bigner DD. Development of novel targeted therapies in the treatment of malignant glioma. Nat Rev Drug Discov. 2004;3:430–446. doi: 10.1038/nrd1380. [DOI] [PubMed] [Google Scholar]
- 5.Doolittle ND, Anderson CP, Bleyer WA, et al. Importance of dose intensity in neuro-oncology clinical trials: Summary report of the Sixth Annual Meeting of the Blood–Brain Barrier Disruption Consortium; Neuro Oncol; 2001. pp. 46–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Browder T, Butterfield CE, Kräling BM, et al. Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res. 2000;60:1878–1886. [PubMed] [Google Scholar]
- 7.Klement G, Baruchel S, Rak J, et al. Continuous low-dose therapy with vinblastine and VEGF receptor-2 antibody induces sustained tumor regression without overt toxicity. J Clin Invest. 2000;105:R15–R24. doi: 10.1172/JCI8829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Panigrahy D, Kaipainen A, Butterfield CE, et al. Inhibition of tumor angiogenesis by oral etoposide. Exp Ther Med. 2010;1:739–746. doi: 10.3892/etm.2010.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bottsford-Miller JN, Coleman RL, Sood AK. Resistance and escape from antiangiogenesis therapy: Clinical implications and future strategies. J Clin Oncol. 2012;30:4026–4034. doi: 10.1200/JCO.2012.41.9242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Manley PW, Martiny-Baron G, Schlaeppi J-M, et al. Therapies directed at vascular endothelial growth factor. Expert Opin Investig Drugs. 2002;11:1715–1736. doi: 10.1517/13543784.11.12.1715. [DOI] [PubMed] [Google Scholar]
- 11.Kerbel RS. Reappraising antiangiogenic therapy for breast cancer. Breast. 2011;20:S56–S60. doi: 10.1016/S0960-9776(11)70295-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kieran MW, Turner CD, Rubin JB, et al. A feasibility trial of antiangiogenic (metronomic) chemotherapy in pediatric patients with recurrent or progressive cancer. J Pediatr Hematol Oncol. 2005;27:573–581. doi: 10.1097/01.mph.0000183863.10792.d4. [DOI] [PubMed] [Google Scholar]
- 13.Pasquier E, Kavallaris M, André N. Metronomic chemotherapy: New rationale for new directions. Nat Rev Clin Oncol. 2010;7:455–465. doi: 10.1038/nrclinonc.2010.82. [DOI] [PubMed] [Google Scholar]
- 14.Stempak D, Gammon J, Halton J, et al. A pilot pharmacokinetic and antiangiogenic biomarker study of celecoxib and low-dose metronomic vinblastine or cyclophosphamide in pediatric recurrent solid tumors. J Pediatr Hematol Oncol. 2006;28:720–728. doi: 10.1097/01.mph.0000243657.64056.c3. [DOI] [PubMed] [Google Scholar]
- 15.André N, Rome A, Coze C, et al. Metronomic etoposide/cyclophosphamide/celecoxib regimen given to children and adolescents with refractory cancer: A preliminary monocentric study. Clin Ther. 2008;30:1336–1340. doi: 10.1016/s0149-2918(08)80059-8. [DOI] [PubMed] [Google Scholar]
- 16.Fousseyni T, Diawara M, Pasquier E, et al. Children treated with metronomic chemotherapy in a low-income country: METRO-MALI-01. J Pediatr Hematol Oncol. 2011;33:31–34. doi: 10.1097/MPH.0b013e3182018ab8. [DOI] [PubMed] [Google Scholar]
- 17.Talpur R, Ward S, Apisarnthanarax N, et al. Optimizing bexarotene therapy for cutaneous T-cell lymphoma. J Am Acad Dermatol. 2002;47:672–684. doi: 10.1067/mjd.2002.124607. [DOI] [PubMed] [Google Scholar]
- 18.Stienstra R, Duval C, Müller M, et al. PPARs, obesity, and inflammation. PPAR Res. 2007;2007:95974. doi: 10.1155/2007/95974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Goetze S, Eilers F, Bungenstock A, et al. PPAR activators inhibit endothelial cell migration by targeting Akt. Biochem Biophys Res Commun. 2002;293:1431–11437. doi: 10.1016/S0006-291X(02)00385-6. [DOI] [PubMed] [Google Scholar]
- 20.Libby P. Current concepts of the pathogenesis of the acute coronary syndromes. Circulation. 2001;104:365–372. doi: 10.1161/01.cir.104.3.365. [DOI] [PubMed] [Google Scholar]
- 21.Panigrahy D, Kaipainen A, Huang S, et al. PPARalpha agonist fenofibrate suppresses tumor growth through direct,indirect angiogenesis inhibition. Proc Natl Acad Sci USA. 2008;105:985–990. doi: 10.1073/pnas.0711281105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bouffet E, Jakacki R, Goldman S, et al. Phase II study of weekly vinblastine in recurrent or refractory pediatric low-grade glioma. J Clin Oncol. 2012;30:1358–1363. doi: 10.1200/JCO.2011.34.5843. [DOI] [PubMed] [Google Scholar]
- 23.Ater JL, Zhou T, Holmes E, et al. Randomized study of two chemotherapy regimens for treatment of low-grade glioma in young children: A report from the Children's Oncology Group. J Clin Oncol. 2012;30:2641–2647. doi: 10.1200/JCO.2011.36.6054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gustafson SA, Lin P, Chen SS, et al. Therapy-related acute myeloid leukemia with t(8;21) (q22;q22) shares many features with de novo acute myeloid leukemia with t(8;21)(q22;q22) but does not have a favorable outcome. Am J Clin Pathol. 2009;131:647–655. doi: 10.1309/AJCP5ETHDXO6NCGZ. [DOI] [PubMed] [Google Scholar]
- 25.Packer RJ, Jakacki R, Horn M, et al. Objective response of multiply recurrent low-grade gliomas to bevacizumab and irinotecan. Pediatr Blood Cancer. 2009;52:791–795. doi: 10.1002/pbc.21935. [DOI] [PubMed] [Google Scholar]
- 26.Chamberlain MC. Recurrent intracranial ependymoma in children: Salvage therapy with oral etoposide. Pediatr Neurol. 2001;24:117–121. doi: 10.1016/s0887-8994(00)00249-6. [DOI] [PubMed] [Google Scholar]
- 27.Peyrl A, Chocholous M, Kieran MW, et al. Antiangiogenic metronomic therapy for children with recurrent embryonal brain tumors. Pediatr Blood Cancer. 2012;59:511–517. doi: 10.1002/pbc.24006. [DOI] [PubMed] [Google Scholar]
- 28.Gately S, Kerbel R. Antiangiogenic scheduling of lower dose cancer chemotherapy. Cancer J. 2001;7:427–436. [PubMed] [Google Scholar]
- 29.Jiménez B, Volpert OV, Crawford SE, et al. Signals leading to apoptosis-dependent inhibition of neovascularization by thrombospondin-1. Nat Med. 2000;6:41–48. doi: 10.1038/71517. [DOI] [PubMed] [Google Scholar]
- 30.Bocci G, Francia G, Man S, et al. Thrombospondin 1,a mediator of the antiangiogenic effects of low-dose metronomic chemotherapy. Proc Natl Acad Sci USA. 2003;100:12917–12922. doi: 10.1073/pnas.2135406100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zapletalova D, André N, Deak L, et al. Metronomic chemotherapy with the COMBAT regimen in advanced pediatric malignancies: A multicenter experience. Oncology. 2012;82:249–260. doi: 10.1159/000336483. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.