

Abstract
Being held responsible for our actions strongly determines our moral judgements and decisions. This study examined whether responsibility also influences our affective reaction to others' emotions. We conducted two experiments in order to assess the effect of responsibility and of a sense of agency (the conscious feeling of controlling an action) on the empathic response to pain. In both experiments, participants were presented with video clips showing an actor's facial expression of pain of varying intensity. The empathic response was assessed with behavioural (pain intensity estimation from facial expressions and unpleasantness for the observer ratings) and electrophysiological measures (facial electromyography). Experiment 1 showed enhanced empathic response (increased unpleasantness for the observer and facial electromyography responses) as participants' degree of responsibility for the actor's pain increased. This effect was mainly accounted for by the decisional component of responsibility (compared with the execution component). In addition, experiment 2 found that participants' unpleasantness rating also increased when they had a sense of agency over the pain, while controlling for decision and execution processes. The findings suggest that increased empathy induced by responsibility and a sense of agency may play a role in regulating our moral conduct.
Keywords: responsibility, sense of agency, empathy, pain perception, electrophysiological measurements, moral sense
1. Introduction
Being held responsible for our own actions and for their effects on others determines our moral sense and conduct. Our moral judgements regarding an individual's action depend not only on its effects on others (e.g. pleasant or unpleasant consequences), but also on the individual's degree of responsibility. An individual is held responsible when he or she executes an action that has direct consequences for others, and even more so when that action is perceived as intentional (i.e. if a decision about the action was also made). It has been shown that intentional actions that have unpleasant effects on others are judged as being more wrong than accidental actions even though the consequences are identical [1–3]. Likewise, our moral decisions are also affected when our personal responsibility is involved. Moral reasoning studies have shown that we make different decisions regarding harmful conduct when we imagine being personally involved compared with imagining what a third party would do [4,5].
Watching harmful conduct that causes pain in an individual not only has some implications for our moral judgements and decisions, but can also elicit an affective reaction from the observer. Yet it is not known whether our responsibility for another's pain also affects our affective reaction to that pain. Observing another's pain will likely elicit an empathic response in the observer [6]. Empathy has been defined as an affective vicarious response, isomorphic to the emotion that provoked it [7,8]. In other words, empathy is the ability to feel what the other feels [8]. Regarding empathy for pain, this would refer to the unpleasant feeling that one experiences when observing a person in pain. Another component of the empathic response, the cognitive component of empathy [9], refers to the ability to understand or evaluate how much pain a person is in [8].
There is evidence that individuals' responsibility for another's pain modulates pain perception and the brain's responses associated with it [10–12]. Akitsuki & Decety [10] have shown that the intensity of a pain caused intentionally by another agent is rated higher than the intensity of a pain caused accidentally, and that brain activity increased in regions involved in representing social interaction and emotion regulation. Koban et al. [12] showed that unintentional personal involvement in another's pain (i.e. when participants erroneously caused pain) induced an enhanced haemodynamic response in the insular cortex, which is part of the affective component of the pain matrix [13]. However, no research to date has established an explicit relationship between the empathic response (i.e. the vicarious unpleasant feeling experienced by the observer) and the personal responsibility (intentional involvement) for that pain.
In this study, we analysed whether personal responsibility for another's pain affects the empathic response to that pain. Responsibility for an action strongly depends on the intentional nature of that action. Intentional actions involve decisional processes about what action to select, and when to act [14], as well as processes of action control to carry out the action selected. Furthermore, the actions that we are responsible for are often accompanied by a sense of agency, the conscious experience of controlling one's own actions and their consequences [15,16]. Therefore, we determined which components of responsibility (the decision about the action, the execution of the action and/or the sense of agency over the action) would affect empathy. We developed two original experiments in which the empathic response to another's pain was measured in conditions that differed in the participants' degree of responsibility for pain. The first experiment assessed whether decision and/or execution processes affect the empathic response to pain. In the second experiment, we examined whether the sense of agency affects that response while controlling for decision and execution processes.
These two experiments were designed so that participants believed that they were participating in a clinical trial testing a new painful treatment in which another volunteer was actually receiving the treatment. They were shown some video clips showing the volunteer's face expressing different intensities of pain (among four pain intensities). In the first experiment, the participants' degree of responsibility for the pain was modulated by manipulating their intentional actions at the decision or the execution level. Either participants were passive observers or they were required to apply the painful treatment (‘execute’ condition), or they had to make a decision about what action to select (select one intensity among four treatment intensities) and execute the action (‘decide and execute’ condition). In the second experiment, the participants' sense of agency was manipulated in addition, by adapting the sense of agency paradigm in which the origin of an action (self or externally generated) was made ambiguous [17]. This allowed us to assess whether the conscious feeling of controlling an action also affected the empathic response. In both experiments, participants' vicarious affective experience of pain was assessed with behavioural and electrophysiological measurements. Behavioural measures included pain intensity ratings (i.e. how intense is the pain observed?) and unpleasantness ratings (i.e. how unpleasant is it for the observer?) in order to assess the cognitive and affective components of empathy, respectively. Electrophysiological measures included facial electromyography (EMG) and heart rate variability (HRV). These metrics are known to correlate with negative affect and empathic response. Facial expression in response to an other's pain expression appears to be a reliable indicator of empathic response. Lamm et al. [18] showed that frowning increased when presented with videos of patients’ faces expressing pain. In addition, the facial muscle, orbicularis oculi, involved in the typical cheek raising and tightening of the orbits of painful expression, was specifically contracted when participants had to put themselves in the patients' position. HRV can be considered as ‘an index of regulated emotional responding’ [19]. The neurovisceral integration model [20] proposes that high frequencies (HFs) of the HRV signal, an index of cardiac vagal tone, are associated with emotion reappraisal and coping with unpleasant stimulation. As real-life social interactions are demanding in terms of emotion regulation, and especially social situations such as harmful conduct in which a person must overcome his/her moral beliefs to accomplish a task, we posited that HF-HRV would be modulated by the degree of responsibility in such social interactions.
Overall, because accidentally causing pain to an individual enhances our empathic response [12], we hypothesized that increasing participants' degree of responsibility for another's pain would increase the empathic response. This effect may be explained by one or several components of responsibility, the decision about the action, the execution of the action and/or the sense of agency over the action.
2. Common procedure in the two experiments
Assessing the impact of responsibility on the empathic response for pain required that participants believe that they could inflict pain on another person. For this purpose, we used a plausible scenario describing a situation in which the inflicting physical suffering on others was morally acceptable. Participants were informed that the research experiment on pain perception for which they had volunteered was taking advantage of another clinical trial testing a new treatment for pain that was taking place at the same time in an adjacent room. They were told that the clinical trial involved one volunteer (in reality a professional actress) who had received the treatment for pain in order to assess her ability to feel the pain stimuli. They were told that the volunteer would be filmed and that they would observe her face while the painful stimuli were applied. Participants were informed that sometimes the clinician running the clinical study would repeatedly apply an electric current (with one intensity varying among four intensities) to the volunteer's hand, through electrodes placed on the back of her hand, whereas at other times, they themselves would trigger the electrical current. To familiarize participants with the experimental procedure and make the scenario more realistic to them, participants were shown other video clips with two professional actors playing the roles of the clinician and the volunteer and they were required to perform practice trials (see the electronic supplementary material: familiarizing participants with the experiment).
The stimuli consisted of video clips of a professional actress making facial expressions of pain with different intensities (low, moderate, intense, very intense). Each 2 s video clip started with a neutral facial expression for 500 ms, which then evolved to a painful expression for 1500 ms (see the electronic supplementary material for detailed stimuli preparation and validation for experiments 1 and 2). Physiological data (EMG and electrocardiogram, ECG) were continuously recorded from the beginning of the experiment.
Forty-four healthy volunteers were recruited for the two experiments; four of them were later excluded from the study because of inappropriate compliance with the experimental procedures. In the end, 21 volunteers took part in experiment 1 (24.8 ± 5.5 years old, 12 women) and 19 volunteers in experiment 2 (23.7 ± 4.2 years old, nine women). None of the participants had a history of psychiatric or neurological disease. Written informed consent was obtained from all the participants. The study conformed to the Code of Ethics of the World Medical Association (Declaration of Helsinki), and the protocol experiment was approved by the local Committee for the Protection of Human Subjects (no. 1-10-29).
3. Experiment 1
(a). Material and methods
Experiment 1 consisted of three conditions that differed in the participants' degree of responsibility for the actress's pain (figure 1). In the ‘observe’ condition, participants passively observed the actress's facial pain expression; they had neither to select an intensity of current nor to trigger the electric current. In the ‘execute’ condition, participants had to press a button to trigger the electric shock and they were told the intensity of the shock in advance. In the ‘decide and execute’ condition, participants had to select one intensity current among four possible intensities (low, moderate, intense, very intense) and trigger the current. The degree of the participants' responsibility for the actress's pain increased from the ‘observe’ condition to the ‘execute’ condition and from the ‘execute’ condition to the ‘decide and execute’ condition. The order of conditions was pseudo-randomized across participants, so that each condition was presented an equal number of times in the first, second and third position. All conditions were grouped into two sessions. In one session, participants evaluated their feeling of unpleasantness, induced by observing the actress's pain (unpleasantness rating). In another session, they had to evaluate the intensity of the observed pain (pain intensity rating). These ratings were given on a visual analogue scale (VAS) ranging from not painful/unpleasant to extremely painful/unpleasant. Each condition was repeated twice within each session. The order of these sessions was counterbalanced across participants, and each session lasted at least 4 min (including the instruction screens) and consisted of 20 trials of 10 s each (five trials per intensity level). A short break was offered every two sessions. At the end of the experiment, a 10 min rest session was additionally recorded for baseline ECG.
Figure 1.

Experimental design. In experiment 1, each session consisted of one passive condition (‘observe’) and two responsibility conditions (‘execute’ and ‘decide and execute’). In the conditions ‘observe’ and ‘execute’, the pain intensity was indicated in green on the instruction screen. In the condition ‘decide’, all the intensities appeared in green to let the participants choose between the four possible intensities. In experiment 2, participants had to choose the pain intensity and their sense of agency was made ambiguous by showing them a facial expression of pain corresponding either to their chosen intensity or to a different intensity. Participants then made an agency judgement by indicating whether they had triggered the pain. For both experiments and for each condition, participants' unpleasantness rating ‘Is it unpleasant?’ (for themselves) and pain rating ‘Is it painful?’ (for the other person) were assessed in separate sessions using a visual analogue scale.
(b). Analyses and results
(i). Participants' involvement in the task
Participants were questioned about their belief in the realism of the experiment using a five-point scale (1, did not believe; 2, seriously doubted; 3, could not say; 4, a slight doubt; and 5, no doubt). The debriefing analyses revealed that participants were indeed well involved in the task, because 90% of them strongly believed in the realism of the experimental context (scores 4 and 5) or had a doubt (scores 2 and 3), but still believed it could be real. All the participants, including those who did not believe, asserted that they behaved as if they had no doubt. In addition, participants more frequently chose lower intensities when they had to decide on the pain level, although they were asked to select all pain intensities an equal number of times (see debriefing and table S1 in the electronic supplementary material, table S1, for more details about the debriefing).
(ii). Pain intensity and unpleasantness ratings
Participants rated the intensity of the observed pain and their feeling of unpleasantness by moving a cursor with a mouse on the VAS. The locations of the cursor on the scale were then converted to a 0–100 scale. Pain intensity and unpleasantness ratings were compared across conditions of degree of responsibility (‘observe’, ‘execute’, ‘decide and execute’) and intensity levels (low, moderate, intense, very intense) using a 2 (response type) × 3 (degree of responsibility) × 4 (intensity level) multivariate analysis of variance (MANOVA). The data revealed a significant main effect of participants’ responsibility (F2,17 = 3.88, p = 0.04, partial η2 = 0.16). The significant interaction between responsibility and the dependent variables further showed that increased responsibility enhanced unpleasantness for the observer, but not pain intensity ratings (F2,17 = 3.87, p = 0.041, partial η2 = 0.18). Post hoc Tukey's tests confirmed that unpleasantness was rated higher when participants had to both select an intensity level and trigger the current (‘decide and execute’ condition) than when they had to passively observe the actress's pain (‘observe’ condition; p = 0.002, figure 2). The difference between the two other conditions was not significant (‘execute’ versus ‘observe’: p = 0.40; ‘execute’ versus ‘decide and execute’: p = 0.20).
Figure 2.
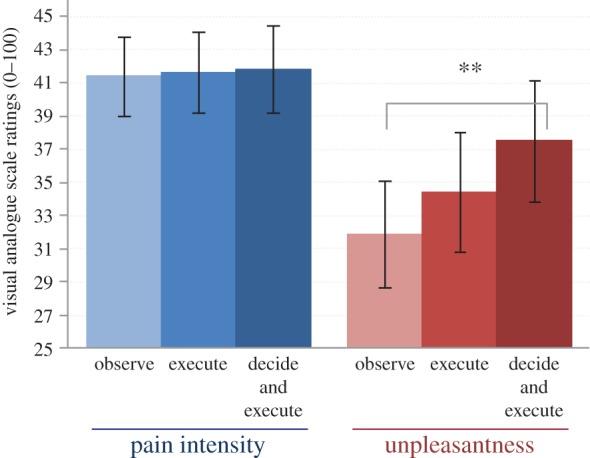
Behavioural results of experiment 1. Unpleasantness rating (red) refers to participants’ evaluation of their feeling of unpleasantness induced by observing the actress's pain. Pain intensity rating (blue) refers to the evaluation of the intensity of the observed pain (i.e. the actress's pain). Participants' unpleasantness ratings increased when they decided and executed the action that induced the pain, compared with the ‘observe’ condition. However, pain ratings were not modified by increased responsibility. Reported values are mean ± s.e.m. **0.01 ≤ p > 0.001. (Online version in colour.)
As expected, both pain intensity and unpleasantness were rated higher for higher intensity levels, as revealed by the significant main effect of intensity level (F3,54 = 324.59, p < 0.001, partial η2 = 0.95). The intensity level affected the two ratings differently, as shown by the significant interaction with the dependent variable (interaction effect: F2,17 = 3.87, p = 0.041, partial η2 = 0.18). The pain intensity rating increased more than the unpleasantness rating when the highest intensity levels (3 and 4) were selected (p ≤ 0.001; figure 2). The intensity level did not, however, interact with the degree of responsibility.
(iii). Physiological measurements
An effect of responsibility was also found on the two physiological responses associated with observing facial pain expressions. Facial EMG was recorded over the regions of the orbicularis oculi and the corrugator supercilii, the muscles involved in the facial expression of pain [21]. The EMG response was scored as the ratio of the signal during the 2 s video clips with the signal during the 1 s baseline period preceding the video (see the electronic supplementary material for more details about technical details of physiological recording). To correct for normality, data were log transformed (log(x + 10)) with a constant of 10 to avoid having negative data in the log. A 3 × 2 × 4 (responsibility × pain intensity/unpleasantness ratings × intensity) MANOVA test, and post hoc Tukey's tests were conducted on the transformed data. The EMG response of the two facial muscles involved in the expression of pain increased with participants’ responsibility for the volunteer's pain (for both muscles: F2,17 ≥ 6.49, p ≤ 0.008, partial η2 ≥ 0.22). Cheek raising (orbicularis oculi) was significantly more intense for both ‘execute’, and ‘decide and execute’ conditions compared with the ‘observe’ condition (p ≤ 0.01), whereas frowning (corrugator supercilii) increased in the ‘execute’ condition compared with the ‘observe’ condition (p = 0.01; figure 3a).
Figure 3.
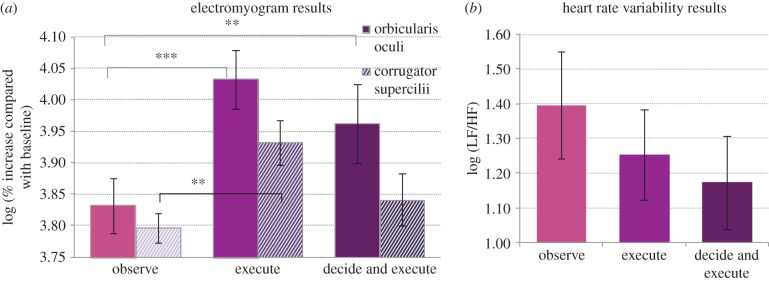
Physiological results of experiment 1. The results have been calculated for both pain and unpleasantness ratings. (a) The orbicularis oculi, the muscle that raises the cheek during facial expression of pain, was more contracted when participants only executed or decided and executed the action than when they passively observed the actor's facial expression of pain. The corrugator supercilii (frowning) was significantly more contracted compared with the ‘observe’ condition only when participants executed the action. (b) The ratio low frequency/high frequency (LF/HF) of the heart rate variability was significantly affected by the main factor responsibility, with a significant difference between the ‘observe’ and the ‘decide and execute’ condition. Reported values are mean ± s.e.m. **0.01 ≤ p > 0.001, ***p ≤ 0.001.
Standard deviation (s.d.) of the interbeat intervals (IBIs) and spectral analysis of HRV were computed throughout each experimental session, thus independently of pain intensity. We then calculated the ratio of low-frequency bands and high-frequency bands (LF/HF; see the electronic supplementary material for more details about technical details of physiological recording). Because the response type (pain intensity/unpleasantness ratings) had no effect on the ratio low frequency/high frequency (LF/HF), the final MANOVA model comprised only the three responsibility conditions for analysing the ratio, along with a rest condition for the s.d. analysis. We observed a significant decrease in the s.d. of the IBI for all conditions compared with rest (F3,15 = 3.83, p = 0.032, partial η2 = 0.24, Tukey's comparison of each condition versus rest: p ≤ 0.021), confirming that participants were cognitively and/or emotionally involved in the task (figure 3b). Analysing the LF/HF ratio, which is considered an index of ‘sympathovagal balance’ [19], we found that this ratio decreased with participants' responsibility (F2,17 = 6.48, p = 0.008, partial η2 = 0.19), with a significant difference between the ‘observe’ condition and the ‘decide and execute’ condition (p = 0.019). This difference can be explained by a concomitant increase in HF and a decrease in LF in the ‘decide and execute’ condition compared with the ‘observe’ condition (F2,17 = 4.71, p = 0.023, partial η2 = 0.18, Tukey comparison p = 0.027), demonstrating a higher engagement of cardiac vagal control when participants had to both select the pain intensity level and trigger the current.
4. Experiment 2
(a). Material and methods
In the second experiment, we further explored the effect of responsibility on pain intensity and unpleasantness ratings by assessing whether this effect may be partly explained by participants' sense of agency over that pain (i.e. their conscious feeling of causing the pain). The paradigm of experiment 1 was modified in order to modulate the sense of agency while keeping the decision processes (selecting one intensity level) and the action control processes (triggering the current) identical. The sense of agency was made ambiguous by adapting a paradigm in which the outcomes of an action are distorted, resulting in a diminished sense of agency over the outcome [17]. As for experiment 1, participants were asked to rate the pain intensity in half of the sessions and their feeling of unpleasantness in the other half. Three responsibility conditions were examined. The ‘observe’ condition was identical to experiment 1 and allowed participants to implicitly associate the intensity level with the corresponding facial expression of pain. The ‘discrepancy’ condition was similar to the ‘decide and execute’ condition of experiment 1. However, in the ‘discrepancy’ condition, they observed the facial expression corresponding to the intensity level selected in about 50% of the trials (no-discrepancy trials), and they observed a facial expression that did not correspond to the intensity selected in the other half of the trials (discrepancy trials, see the electronic supplementary material for details about discrepancy in the intensity levels). The third condition, ‘sense of agency’, was identical to ‘discrepancy’ except that before the session, participants were told that the current could be applied randomly either by themselves or by the clinician. Participants did not know prior to the video onset whether they or the clinician had actually triggered the current. They became aware of it when seeing the video. Therefore, the main difference with the ‘discrepancy’ condition was that participants could attribute the actress's pain to the clinician. As a consequence, there were trials in which participants did not have a sense of agency over the actress's pain even though they made a decision and executed the action. Participants' sense of agency was measured by requiring them to make a sense of agency judgement about who caused the actress's pain, themselves (‘self’-trials) or the clinician (‘other’-trials; figure 1).
The three conditions were always run in the same order. First, the ‘observe’ condition allowed participants to learn the association between intensity level and the corresponding facial expression of pain. The ‘discrepancy’ condition was then run, followed by the ‘sense of agency’ condition. The ‘sense of agency’ condition was always run after the ‘discrepancy’ condition, to avoid participants attributing the discrepancy trials to the clinician in the ‘discrepancy’ condition. The ‘discrepancy’ condition was used to distinguish the effect of discrepancy on empathy from the effect of the sense of agency.
(b). Analyses and results
(i). Pain intensity and unpleasantness ratings
We first assessed whether the effect of responsibility found in experiment 1 was replicated in this second experiment. To do so, participants' ratings in the ‘observe’ condition were compared with the ratings obtained in the no-discrepancy trials of the ‘discrepancy’ condition as these trials were equivalent to the ‘decide and execute’ conditions of experiment 1. We ran a 2 × 2 × 4 repeated MANOVA test with responsibility×ratings × intensity. Replicating the results of experiment 1, we found a significant interaction between ratings and responsibility (F1,18 = 8.26, p = 0.010, partial η2 = 0.31). As in experiment 1, unpleasantness rating increased when participants were responsible for the actress's pain (p = 0.034) compared with when they passively observed the pain, whereas pain intensity ratings were not modulated by participants’ responsibility (p = 0.72).
Manipulating the degree of discrepancy modulated participants' sense of agency (see the electronic supplementary material for details about the sense of agency judgements). We therefore distinguished the trials in which participants felt that they had triggered the shock and therefore had a sense of agency over the actress's pain (‘self’-trials) from those in which they felt that the clinician had triggered the shock and therefore had no sense of agency (‘other’-trials).
We then examined the effect of the sense of agency on pain and unpleasantness ratings. We first checked whether the degree of discrepancy between the selected pain intensity and the pain intensity expressed by the actress's face affected participants' pain intensity and unpleasantness ratings. In fact, this needed to be discarded from these ratings in order to assess the effect of the sense of agency independently of the degree of discrepancy. A repeated MANOVA test with ratings and degree of discrepancy as factors was run for each pain intensity level. The degree of discrepancy affected both pain intensity and unpleasantness ratings, whatever the intensity of the pain observed (for both ratings: F2/3,17/16 > 7.72, p < 0.004, partial η2 > 0.32). Participants’ ratings decreased when the observed pain intensity was higher than the intensity chosen, and increased when the observed intensity pain was lower. To accurately assess the effect of the sense of agency on pain intensity and unpleasantness ratings, participants' behavioural measurements in the sense of agency condition were therefore corrected with a measurement of the discrepancy effect. We defined the discrepancy effect as the difference in the ratings (separately for pain intensity and unpleasantness ratings) between the no-discrepancy trials and the discrepancy trials. This effect was calculated for each degree of discrepancy and for each subject. These differences were then subtracted from the ratings obtained in the ‘sense of agency’ condition. This resulted in pain intensity and unpleasantness ratings that were not contaminated by the degree of discrepancy. The corrected measures were then analysed using a (2 × 2 × 4; sense of agency × pain/unpleasantness × intensity) MANOVA. We found that participants' ratings increased in the ‘self’-trials compared with the ‘other’-trials (F1,18 = 6.12, p = 0.02, partial η2 = 0.25). Crucially, we found that participants' sense of agency affected pain intensity ratings and unpleasantness ratings differently, as revealed by the interaction between the sense of agency condition and the dependent variable (F1,18 = 5.15, p = 0.04, partial η2 = 0.22). Post hoc analyses further revealed that only unpleasantness ratings increased in the ‘self’-trials compared with the ‘other’-trials. (Tukey's post hoc: pain ‘self’ versus ‘other’ p = 0.98, unpleasantness ‘self’ versus ‘other’ p = 0.046, figure 4).
Figure 4.
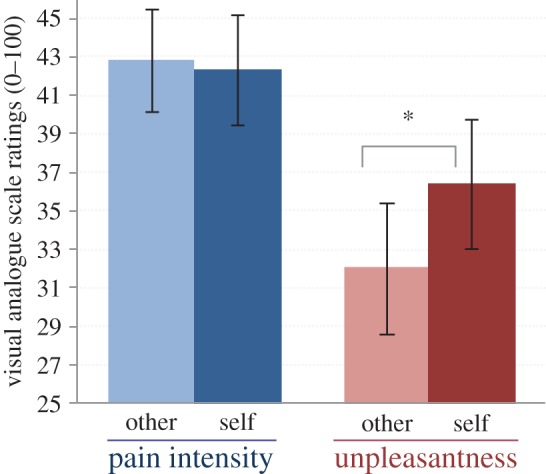
Behavioural results of experiment 2. Unpleasantness rating (red) refers to participants’ evaluation of their own unpleasant feeling induced by observing the actress's pain. Pain intensity rating (blue) refers to the estimation of the intensity of pain experienced by the actress. Participants' unpleasantness ratings were higher when they attributed the trigger of the pain to themselves (‘self’), whereas pain ratings were not modified by participants' sense of agency. Reported values are mean ± s.e.m. *0.05 ≤ p > 0.01. (Online version in colour.)
(ii). Physiological measurement
EMG was recorded as described in experiment 1. As for behavioural data, physiological data were previously corrected for discrepancy effect. However, HRV could not be computed on a trial basis as short as 10 s [22].
The same analytical procedure as for behavioural measurements was used for physiological data. A main effect of responsibility (‘observe’ versus ‘decide and execute’) was found on facial EMGs. Observing a painful expression induced more intense facial EMGs when participants had previously selected the intensity level and triggered the shock (corrugator: F1,18 = 21.55, p < 0.001, partial η2 = 0.55; orbicularis: F1,18 = 13.96, p = 0.001, partial η2 = 0.44). Regarding the comparison between ‘self’ and ‘other’ trials, EMGs were analysed using a 2 × 2 × 4 (sense of agency × pain/unpleasantness × intensity) MANOVA and post hoc Tukey's tests. We did not observe a significant sense of agency effect (corrugator: p = 0.11; orbicularis: p = 0.57).
5. Discussion
Observing the pain reaction of another person is likely to elicit an empathic response towards that person. In this study, we found that being held responsible for that pain by being actively involved in it causes enhanced empathic response. Increasing participants' degree of responsibility over others' pain resulted in increased unpleasantness, which was further corroborated by an increase in facial EMG responses in experiment 1.
The patterns of both electrophysiological and behavioural responses convinced us that participants' affective reaction to the observed pain was correctly characterized as an empathic response, as defined by de Vignemont & Singer [7], and thus could not be confused with other vicarious pain experiences. Indeed, both these patterns show that the affective state elicited by observing painful facial expressions, and modulated by the degree of responsibility, was a negative affect, isomorphic to the feeling that had elicited it (the actress's facial expression of pain). First, the degree of responsibility increased the affective response (i.e. the rating of unpleasantness), but not that of pain intensity. Second, the contraction of two facial muscles involved in pain expression (corrugator supercilii and the pars orbitalis of the orbicularis oculi) also increased with responsibility. The EMG of these two muscles was not modulated by the intensity of the observed facial pain, suggesting that these facial responses did not reflect a mere motor mimicry, in which the contraction of facial muscles are directly and automatically induced by the observation of facial movements [23–25]. Rather, these facial EMGs reflect the expression of negative affect felt by participants, as also observed for the observation of unpleasant scenes in which no facial cues were presented (see [26] for review). Although frowning, controlled by the corrugator supercilii, is a generic facial movement for negative affect, cheek raising and eye narrowing, controlled by the orbicularis occuli, are more specific to painful expression [18,21].
Other authors do not limit their definition of empathy to the affective aspect and argue instead for two components of empathy: the affective and the cognitive [27,28]. In this study, the affective component referred to the evaluation of unpleasantness for the observer, whereas the cognitive component referred to the evaluation of the intensity of another's pain. This cognitive component was modulated neither by the degree of responsibility (experiment 1) nor by the sense of agency (experiment 2). This means that the increased unpleasantness (or emotional empathy) when the participants' degree of responsibility for the actress's pain increased cannot be explained by an overestimation of the observed pain. This is in line with Shamay-Tsoory's arguments [9], which view the cognitive and emotional components of empathy as partially separate and involving independent processes, as well as Morrison et al.'s [29] proposal to distinguish between pain empathy and pain recognition.
Responsibility also affected participants’ emotional regulation as revealed by variations in the HRV across conditions. In experiment 1, changes in HRV were observed in the ‘decide and execute’ condition, with a decrease in the LF/HF ratio reflecting a higher involvement of vagal control over HRV. High vagal activity has been linked to successfully coping with stressful or unpleasant situations [19,30–32] and results in successful emotional and cognitive regulation [33]. These results show that there was more emotional regulation when participants had to decide on the intensity level and to execute the action.
Responsibility for an action strongly depends on whether the action is intentional. We found that the decision component of intentional action had the most pronounced effect on participants' empathy, on both their behavioural and physiological responses. The feeling of unpleasantness significantly increased when participants had to select an action (i.e. select the intensity level) and execute the action (i.e. trigger the shock) compared with when they passively observed another's facial pain expression. Likewise, facial EMG over the orbicularis occuli significantly increased when participants had to take a decision and execute the action. One significant difference was found, however, in that the orbicularis occuli and the corrugator supercilii activity also increased when participants solely executed the action previously selected by the clinician. Therefore, these findings show that the effect of participants' responsibility on their empathic response can be accounted for by decision processes and more specifically by the decision about which action to select. Action control processes might also be involved, because facial EMG increased in the ‘execute’ condition compared with the ‘observe’ condition. However, this effect was not observed on participants' unpleasantness ratings suggesting that action control might be involved to a lower extent in the modulation of empathy. This difference might be explained by the fact that the judgement of unpleasantness does not solely rely on participants' negative affect, which is reflected by facial EMG. Therefore, participants' degree of responsibility in the ‘execute’ condition might be sufficient to affect their negative affect but not the explicit judgement about their affect.
In the second experiment, we found that participants’ sense of agency over the pain also affected their empathic response. Participants' feeling of unpleasantness increased when they became consciously aware that their action (and not the clinician's) caused the observed pain. The effect of participants' sense of agency on their empathic response cannot be explained in terms of anticipation nor in terms of difference in the decision and the control of action, as these processes were carefully controlled: (i) participants always had to take a decision and execute the action and (ii) the judgements of agency could not be anticipated as participants did not know at the beginning of the trial whether they or the clinician would trigger the current, and only became aware of it when watching the video. Furthermore, the sense of agency's effect on empathy occurred irrespective of the magnitude of the error, as unpleasantness and pain ratings were carefully corrected for the discrepancy effect. Recently, Koban et al. [12] manipulated participants' responsibility for another's pain by creating situations in which their actions accidentally caused another's pain. This error agency modulated the participants' perception of the pain and yielded enhanced activity in the anterior insula. Our present findings differ from those of Koban et al. [12] because they showed that the conscious feeling of controlling an action per se affected the empathic response independently of any error effects.
This reveals an important and yet unexplored aspect of the sense of agency: its role in social cognition. This role could well not be limited to empathy and encompass other aspects of social cognition. Indeed, the consciousness of our actions and their effects on others could affect the way we perceive others' reactions, in terms of their emotions, their actions and even their intentions; this, in turn, might have some implications in the regulation of our social behaviours. There is, indeed, previous evidence that the effects of our actions on others generate emotional and affective reactions that might help regulate social behaviour. When our actions have positive consequences (acts of kindness or sympathy), they are accompanied by a positive feeling that helps reinforce these actions [34]. The present findings show that when an action has negative or unpleasant consequences for others, there is a stronger negative emotional reaction. This amplified response may have an impact on the regulation of that behaviour. Indeed, we found that responsibility led to more emotional regulation, suggesting that participants were reluctant to carry out the action. These findings confirm previous research in social psychology showing that, when people witness the pain they have inflicted on others, this can generate vicarious negative affect that may help to restrain harmful conduct [35]. We therefore argue that enhanced empathy associated with responsibility may play a role in regulating our social behaviour by preventing us from harmful actions, thereby reinforcing our moral conduct. Note, however, that this regulation effect cannot be considered as systematic, but is highly dependent on the social context (e.g. a physician will not interrupt a medical painful act because he/she is responsible for it). In other contexts, the enhanced empathic response might lead to prosocial behaviour (e.g. a parent will comfort her/his child after having applied a painful medical treatment to her/him). Indeed, it is known that empathic response can trigger prosocial behaviour [31,36–39], which can even be species-specific [40]. Therefore, depending on the social context, responsibility and sense of agency can have different impacts on social cognition, and these effects might, in turn, lead to distinct social behaviours. Future research will need to further characterize these effects and the resulting social behaviours.
6. Conclusion
This study has shown that when we have a responsibility for others' suffering, our empathic response to that suffering is increased. We have also demonstrated that both decision processes and the conscious feeling of controlling our action, the sense of agency, explain this effect. This enhanced empathy elicited by intentional voluntary action may play a role in the regulation of moral conduct. These findings therefore open up avenues for future research on the ways in which responsibility and sense of agency effects on other perception may influence moral behaviour.
Supplementary Material
Acknowledgements
We gratefully acknowledge Chris Frith for his insightful comments on an earlier version of the article, Nicolas Danziger for providing us with the French translation of the SPQ, Hélène Marcombe for her help in recruiting and testing participants, and Cynthia Johnson for her help in proofreading the final draft of the article.
Data accessibility
Data are available at http://cerco.ups-tlse.fr/Chloe-FARRER-PUJOL.
Funding statement
This study was supported by grants from the CNRS and the region of Midi-Pyrénées.
References
- 1.Cushman F. 2008. Crime and punishment: distinguishing the roles of causal and intentional analyses in moral judgment. Cognition 108, 353–380. ( 10.1016/j.cognition.2008.03.006) [DOI] [PubMed] [Google Scholar]
- 2.Young L, Bechara A, Tranel D, Damasio H, Hauser M, Damasio A. 2010. Damage to ventromedial prefrontal cortex impairs judgment of harmful intent. Neuron 65, 845–851. ( 10.1016/j.neuron.2010.03.003) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Young L, Cushman F, Hauser M, Saxe R. 2007. The neural basis of the interaction between theory of mind and moral judgment. Proc. Natl Acad. Sci. USA 104, 8235–8240. ( 10.1073/pnas.0701408104) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hauser M, Cushman F, Young L, Jin RK-X, Mikhail J. 2007. A dissociation between moral judgments and justifications. Mind Lang. 22, 1–21. ( 10.1111/j.1468-0017.2006.00297.x) [DOI] [Google Scholar]
- 5.Cushman F, Young L, Hauser M. 2006. The role of conscious reasoning and intuition in moral judgment testing three principles of harm. Psychol. Sci. 17, 1082–1089. ( 10.1111/j.1467-9280.2006.01834.x) [DOI] [PubMed] [Google Scholar]
- 6.Singer T, Lamm C. 2009. The social neuroscience of empathy. Ann. Nat. Acad. Sci. 1156, 81–96. ( 10.1111/j.1749-6632.2009.04418.x) [DOI] [PubMed] [Google Scholar]
- 7.de Vignemont F, Singer T. 2006. The empathic brain: how, when and why? Trends Cogn. Sci. 10, 435–441. ( 10.1016/j.tics.2006.08.008) [DOI] [PubMed] [Google Scholar]
- 8.Decety J, Lamm C. 2006. Human empathy through the lens of social neuroscience. Sci. World J. 6, 1146–1163. ( 10.1100/tsw.2006.221) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shamay-Tsoory SG. 2011. The neural bases for empathy. Neuroscientist 17, 18–24. ( 10.1177/1073858410379268) [DOI] [PubMed] [Google Scholar]
- 10.Akitsuki Y, Decety J. 2009. Social context and perceived agency affects empathy for pain: an event-related fMRI investigation. Neuroimage 47, 722–734. ( 10.1016/j.neuroimage.2009.04.091) [DOI] [PubMed] [Google Scholar]
- 11.Decety J, Porges EC. 2011. Imagining being the agent of actions that carry different moral consequences: an fMRI study. Neuropsychologia 49, 2994–3001. ( 10.1016/j.neuropsychologia.2011.06.024) [DOI] [PubMed] [Google Scholar]
- 12.Koban L, Corradi-Dell'Acqua C, Vuilleumier P. 2013. Integration of error agency and representation of others’ pain in the anterior insula. J. Cogn. Neurosci. 25, 258–272. ( 10.1162/jocn_a_00324) [DOI] [PubMed] [Google Scholar]
- 13.Fulbright RK, Troche CJ, Skudlarski P, Gore JC, Wexler BE. 2001. Functional MR imaging of regional brain activation associated with the affective experience of pain. Am. J. Roentgenol. 177, 1205–1210. ( 10.2214/ajr.177.5.1771205) [DOI] [PubMed] [Google Scholar]
- 14.Brass M, Haggard P. 2008. The what, when, whether model of intentional action. Neuroscientist 14, 319–325. ( 10.1177/1073858408317417) [DOI] [PubMed] [Google Scholar]
- 15.Frith C. 2013. The psychology of volition. Exp. Brain Res. Exp. Hirnforsch. Exp. Cerebrale 229, 289–299. ( 10.1007/s00221-013-3407-6) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moretto G, Walsh E, Haggard P. 2011. Experience of agency and sense of responsibility. Conscious. Cogn. 20, 1847–1854. ( 10.1016/j.concog.2011.08.014) [DOI] [PubMed] [Google Scholar]
- 17.Farrer C, Bouchereau M, Jeannerod M, Franck N. 2008. Effect of distorted visual feedback on the sense of agency. Behav. Neurol. 19, 53–57. ( 10.1155/2008/425267) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lamm C, Porges EC, Cacioppo JT, Decety J. 2008. Perspective taking is associated with specific facial responses during empathy for pain. Brain Res. 1227, 153–161. ( 10.1016/j.brainres.2008.06.066) [DOI] [PubMed] [Google Scholar]
- 19.Appelhans BM, Luecken LJ. 2006. Heart rate variability as an index of regulated emotional responding. Rev. Gen. Psychol. 10, 229 ( 10.1037/1089-2680.10.3.229) [DOI] [Google Scholar]
- 20.Thayer JF, Lane RD. 2000. A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 61, 201–216. ( 10.1016/S0165-0327(00)00338-4) [DOI] [PubMed] [Google Scholar]
- 21.Ekman P, Rosenberg EL. 1997. What the face reveals: basic and applied studies of spontaneous expression using the facial action coding system (FACS). Oxford, UK: Oxford University Press. [Google Scholar]
- 22.Berntson GG, Quigley KS, Lozano D. 2007. Cardiovascular psychophysiology. In Handbook of psychophysiology (eds Cacioppo JT, Tassinary LG, Berntson GG.), 3rd edn, pp. 182–210. New York, NY: Cambridge University Press. [Google Scholar]
- 23.Cacioppo JT, Petty RE, Losch ME, Kim HS. 1986. Electromyographic activity over facial muscle regions can differentiate the valence and intensity of affective reactions. J. Pers. Soc. Psychol. 50, 260–268. ( 10.1037/0022-3514.50.2.260) [DOI] [PubMed] [Google Scholar]
- 24.Magnée MJCM, Stekelenburg JJ, Kemner C, Gelder B. 2007. Similar facial EMG responses to faces, voices, and body expressions. Neuroreport 18, 369–372. ( 10.1097/WNR.0b013e32801776e6) [DOI] [PubMed] [Google Scholar]
- 25.Moody EJ, McIntosh DN, Mann LJ, Weisser KR. 2007. More than mere mimicry? The influence of emotion on rapid facial reactions to faces. Emotion 7, 447–457. ( 10.1037/1528-3542.7.2.447) [DOI] [PubMed] [Google Scholar]
- 26.Cacioppo JT, Berntson GG, Sheridan JF, McClintock MK. 2000. Multilevel integrative analyses of human behaviour: social neuroscience and the complementing nature of social and biological approaches. Psychol. Bull. 126, 829–843. ( 10.1037/0033-2909.126.6.829) [DOI] [PubMed] [Google Scholar]
- 27.Schulte-Ruther M, Markowitsch HJ, Fink GR, Piefke M. 2007. Mirror neuron and theory of mind mechanisms involved in face-to-face interactions: a functional magnetic resonance imaging approach to empathy. J. Cogn. Neurosci. 19, 1354–1372. ( 10.1162/jocn.2007.19.8.1354) [DOI] [PubMed] [Google Scholar]
- 28.Shamay-Tsoory SG, Aharon-Peretz J, Perry D. 2009. Two systems for empathy: a double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 132, 617–627. ( 10.1093/brain/awn279) [DOI] [PubMed] [Google Scholar]
- 29.Morrison I, Poliakoff E, Gordon L, Downing P. 2007. Response-specific effects of pain observation on motor behaviour. Cognition 104, 407–416. ( 10.1016/j.cognition.2006.07.006) [DOI] [PubMed] [Google Scholar]
- 30.Butler EA, Wilhelm FH, Gross JJ. 2006. Respiratory sinus arrhythmia, emotion, and emotion regulation during social interaction. Psychophysiology 43, 612–622. ( 10.1111/j.1469-8986.2006.00467.x) [DOI] [PubMed] [Google Scholar]
- 31.Geisler FC, Kubiak T, Siewert K, Weber H. 2013. Cardiac vagal tone is associated with social engagement and self-regulation. Biol. Psychol. 93, 279–286. ( 10.1016/j.biopsycho.2013.02.013) [DOI] [PubMed] [Google Scholar]
- 32.Pu J, Schmeichel BJ, Demaree HA. 2010. Cardiac vagal control predicts spontaneous regulation of negative emotional expression and subsequent cognitive performance. Biol. Psychol. 84, 531–540. ( 10.1016/j.biopsycho.2009.07.006) [DOI] [Google Scholar]
- 33.Thayer JF, Hansen AL, Saus-Rose E, Johnsen BH. 2009. Heart rate variability, prefrontal neural function, and cognitive performance: the neurovisceral integration perspective on self-regulation, adaptation, and health. Ann. Behav. Med. 37, 141–153. ( 10.1007/s12160-009-9101-z) [DOI] [PubMed] [Google Scholar]
- 34.Fredrickson BL, Cohn MA, Coffey KA, Pek J, Finkel SM. 2008. Open hearts build lives: positive emotions, induced through loving-kindness meditation, build consequential personal resources. J. Pers. Soc. Psychol. 95, 1045–1062. ( 10.1037/a0013262) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bandura A. 1991. Social cognitive theory of self-regulation. Organ. Behav. Hum. Decis. Process. 50, 248–287. ( 10.1016/0749-5978(91)90022-L) [DOI] [Google Scholar]
- 36.Vélez García AE, Ostrosky-Solís F. 2006. From morality to moral emotions. Int. J. Psychol. 41, 348–354. ( 10.1080/00207590500345898) [DOI] [Google Scholar]
- 37.Hess U, Fischer A. 2013. Emotional mimicry as social regulation. Pers. Soc. Psychol. Rev. 17, 142–157. ( 10.1177/1088868312472607) [DOI] [PubMed] [Google Scholar]
- 38.Chartrand TL, Bargh JA. 1999. The chameleon effect: The perception–behaviour link and social interaction. J. Pers. Soc. Psychol. 76, 893–910. ( 10.1037/0022-3514.76.6.893) [DOI] [PubMed] [Google Scholar]
- 39.Porges SW. 2007. The polyvagal perspective. Biol. Psychol. 74, 116–143. ( 10.1016/j.biopsycho.2006.06.009) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Anelli F, Borghi AM, Nicoletti R. 2012. Grasping the pain: motor resonance with dangerous affordances. Conscious. Cogn. 21, 1627–1639. ( 10.1016/j.concog.2012.09.001) [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are available at http://cerco.ups-tlse.fr/Chloe-FARRER-PUJOL.