

Abstract
The widespread use of echocardiography has contributed to the early recognition of several distinct cardiac diseases in women. During pregnancy, safe monitoring of the disease process, as well as a better understanding of hemodynamics, is possible. During the use of potentially cardiotoxic drugs for breast cancer chemotherapy, echocardiographic patient monitoring is vital. Compared to men, the addition of an imaging modality to routine electrocardiogram monitoring during stress testing is more informative for diagnosing coronary disease in women. This review briefly discusses the role of echocardiography in the management of several women-specific cardiac diseases where echocardiography plays a pivotal role in disease management.
Keywords: Echocardiography, Women, Peripartum cardiomyopathy, Coronary heart disease, Cardiotoxicity
Introduction
Cardiovascular disease, as a cause of mortality in women, is becoming more prevalent than before and will continue to increase, partly because of increasing life expectancies among Koreans.1) In women, the cardiovascular system is exposed to multiple cyclic hormonal changes during the childbearing years, acute hemodynamic burdens during pregnancy, and the sudden deprivation of estrogen at menopause.2),3),4) The cardiovascular problems of women may be divided into two categories. The first involves women-specific cardiac diseases that occur only in women, such as pregnancy-related cardiac problems in previously normal or diseased hearts. The other involves cardiac problems that disproportionately affect women, such as stress-induced cardiomyopathy, or that have different clinical presentations from those occurring in men, such as coronary heart disease and heart failure. For the proper management of heart disease in women, accurate and timely diagnostic procedures are important in the clinic. This review discusses the role of echocardiography in the evaluation of heart disease in women, with a focus on pregnancy-related cardiac disease, chemotherapy-induced cardiotoxicity, and ischemic heart disease.
Pregnancy-Related Cardiac Disease
In pregnant women, the process for diagnosing cardiac disease is challenging. The possible hazards of radiation exposure and intravenous contrast agents limit the use of several diagnostic imaging modalities in pregnant women. Echocardiography is regarded as safe for both the pregnant woman and her fetuses, and it is the most frequently used imaging test for cardiac disease in pregnant women. With echocardiography, several cardiac conditions that might complicate pregnancy can be diagnosed and the cardiac disease severity can also be assessed. The technique also allows safe follow-up monitoring of left and right ventricular function during pregnancy.
During pregnancy, a woman's heart position is displaced antero-superiorly by the enlarged uterus. Other cardiovascular changes that occur during pregnancy include increased total blood volume, increased cardiac output and stroke volume, and decreased peripheral vascular resistance.5),6),7) The size of the right ventricle increases by 20% and the left ventricle and left atrium increase by 10% and 12%, respectively. Systolic and diastolic functional parameters, as well as the longitudinal deformation parameters, are diminished during the last trimester of pregnancy and return to normal within a few weeks or months after delivery.6),8) Normally, flow velocity through each valve orifice may increase and small atrioventricular regurgitations may appear due to the enlarged annulus.
Peripartum Cardiomyopathy
Peripartum cardiomyopathy (PPCM) is defined as an idiopathic cardiomyopathy that develops at the end of pregnancy or during the months following delivery.9),10),11) Its clinical presentation involves systolic heart failure, without an identifiable cause. Viral infection, genetic factors, abnormal immunologic activities, and malnutrition have been suggested to have a role in the etiology of PPCM, but the etiology is not clearly defined. The role of echocardiography is fundamental to the diagnosis of PPCM. Actually, when pregnant women experience symptoms that may have cardiac origins, echocardiography is often the first test considered. However, symptoms of dyspnea during the last trimester of a normal pregnancy are not regarded as pathologic, in general, and may, therefore, result in a diagnostic delay or misdiagnosis of PPCM. The left ventricular systolic function is almost always diminished in the echocardiograms of patients with PPCM. A mural thrombus inside the poorly contracting left ventricle can be visualized. The left ventricular chamber size may be enlarged or may be normal. PPCM prognosis can be evaluated by echocardiography, as well. When the baseline left ventricular ejection fraction is ≥ 30%, the chance of an early recovery early is 6.4-fold higher than in women with an ejection fraction of 10-19%.12) A recently developed echocardiographic technique that uses Doppler tissue imaging or speckle tracking imaging to study left ventricular mechanics has been attempted, but is not widely used, yet.
Pre-Existing Cardiac Disease
As the surgical repair techniques for congenital heart disease progress, the number of pregnant women undergoing congenital heart disease repair is also increasing. Sometimes pregnant women may demonstrate the presence of residua and sequelae from previous cardiac surgery that require cardiological support. As described above, pregnancy is characterized as a high-flow, low-resistance state with increased cardiac output and diminished vascular resistance. The main pathophysiologic mechanisms in pregnant women with congenital heart disease are volume overloads, left-right shunts, pressure overloads and cyanotic right-to-left shunts. Generally, pregnant women with noncyanotic left-to-right shunts are able to tolerate without complications. However, in cases of right-to-left shunts with pulmonary hypertension, the decrease in systemic vascular resistance leads to increased right-to-left shunt flow, causing systemic cyanosis.13),14) The presence of right ventricular dysfunction and high hematocrits were identified as poor prognostic factors in pregnant women with intracardiac right-to-left shunts.
In left-heart stenotic valvular disease, the increased blood volume during pregnancy may cause worsened relative valvular obstructions. The degree of valvular stenosis determines the pregnancy outcomes. In pregnant women with mitral or aortic stenosis, a < 2.0 cm2 mitral valve area, < 1.5 cm2 aortic valve area, and a > 30 mm Hg peak pressure gradient in the left ventricular outflow tract, determined using echocardiography, are predictors of maternal cardiac morbidity and neonatal events. Left ventricular ejection fraction, diminished by 40%, is also considered a risk predictor during pregnancy.14),15),16) Specifically, pregnancy is contraindicated in patients with pulmonary arterial hypertension, severe left ventricular dysfunction (< 30% ejection fraction), previous PPCM with residual left ventricular dysfunction, symptomatic severe aortic and mitral stenosis, dilated aorta (> 45 mm in patients with Marfan syndrome, > 50 mm in patients with bicuspid aortic valve), or severe coarctation (Table 1).16) With echocardiography, prenatal risk quantification can be safely performed and can assist in genetic counseling. Monitoring cardiac and valvular function during pregnancy is also important for selecting patients who need cesarean delivery because of their hemodynamic instability or risk of aortic dissection.17),18)
Table 1.
World Health Organization (WHO) classification of maternal cardiovascular risk
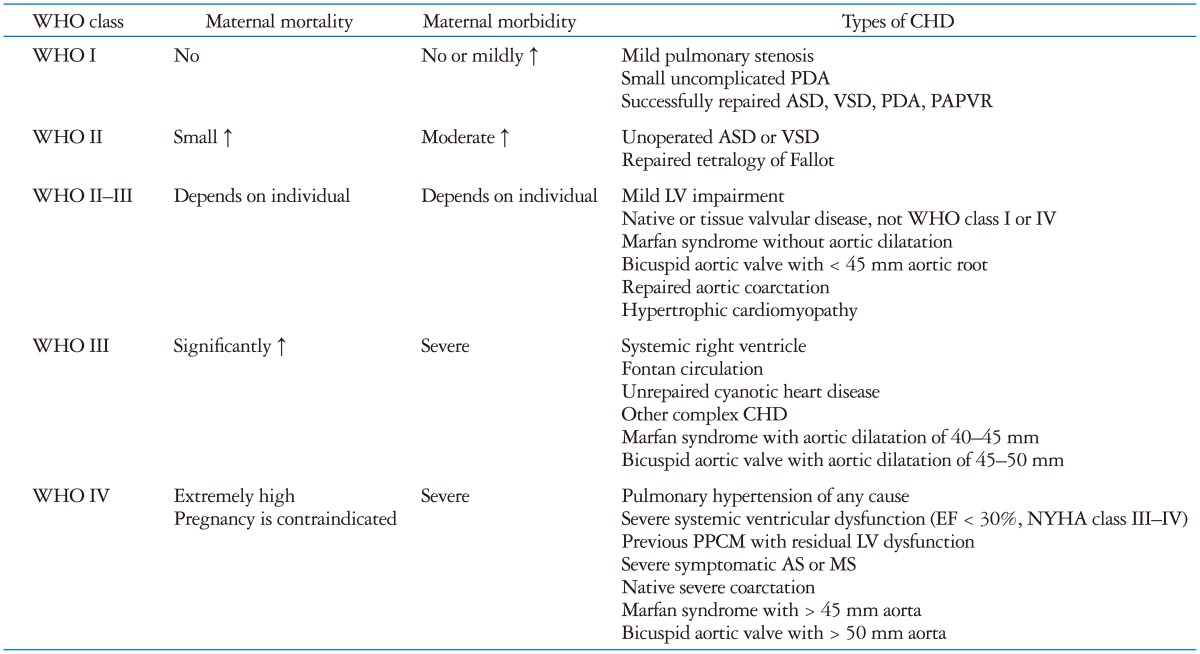
AS: aortic stenosis, ASD: atrial septal defect, CHD: congenital heart disease, EF: ejection fraction, LV: left ventricle, MS: mitral stenosis, NYHA: New York Heart Association, PAPVR: partial anomalous pulmonary venous return, PDA: patent ductus arteriosus, VSD: ventricular septal defect
Chemotherapy Associated Cardiotoxicity
Cardiovascular complications can arise in significant numbers of patients following cancer therapy.19),20),21) In Korea, the incidence of breast cancer has increased steeply among women. The drugs used to treat breast cancer, including anthracycline, trastuzumab, and tyrosine kinase inhibitors, also have cardiotoxic potential. As the survival rate, after cancer therapy, has improved, the numbers of survivors with treatment-related cardiac morbidity have also increased. Left ventricular dysfunction, with or without heart failure, is the most common type of breast cancer chemotherapy-related cardiotoxicity. Chemotherapy-induced left ventricular dysfunction is defined as a ≥ 5% decline in left ventricular ejection fraction to < 55%, with accompanying symptoms, or a decline in ejection fraction of at least 10% to below 55%, without symptoms, and signs of heart failure (Fig. 1).22)
Fig. 1.

Spherically shaped end-systolic left ventricle in a 50-year-old woman, with diminished left ventricular systolic function, after treatment with 360 mg of doxorubicin (A: before treatment, B: after treatment).
Chemotherapy-induced left ventricular dysfunction is classified into two types. Type I refers to cardiotoxicity due to direct myocardial injury, causing myocyte loss and irreversible myocardial dysfunction, such as in anthracycline toxicity. The incidence of cardiotoxicity may reach 25% (18% subclinical and 6% overt) over a 9-year follow-up period, dependent upon the dose of anthracycline.19) When this type of cardiotoxicity is induced, further drug use is contraindicated. In contrast, myocardial dysfunction is usually reversible in type II cardiac toxicity (mitochondrial and protein alterations), such as in trastuzumab toxicity.20) However, the distinction between the 2 types does have limitations, and there are overlaps in the patterns of cardiac complications, based on the type of chemotherapeutic agent.23) In addition to these two types of drugs that directly target the cardiomyocyte, bevacizumab and sunitinib may induce heart failure or hypertension through the targeting of vascular endothelial growth factor.24)
Because of the potential cardiotoxic hazard of chemotherapeutic agents, monitoring of cardiac function is recommended pre- and post-treatment when these agents are used. Early detection of cardiotoxicity is critical because asymptomatic cardiotoxicity may persist for long periods before clinical manifestations occur, and the therapeutic benefits of drugs that treat the cardiotoxicity are greatest during the early period of cardiac dysfunction.25) For this purpose, echocardiographic measurements of the left ventricular ejection fraction remain the most widely used clinical tool. According to the European Society for Medical Oncology practice guidelines,22) echocardiographic screening before, during, and after cardiotoxic chemotherapy (every 3-6 months for the first year and every year, thereafter) is recommended in conjunction with anthracycline or trastuzumab treatment. But the detection of early, subtle, cardiotoxicity using two-dimensional echocardiography measurements of left ventricular ejection fraction is not sufficiently sensitive and has high inter-observer variability.26),27),28),29) Left ventricular functional evaluations using three-dimensional echocardiography are more accurate and may overcome this shortcoming.30) Recent studies suggest that post-chemotherapy left ventricular deformation imaging, especially for the detection of reduced global longitudinal left ventricle strain, with or without biochemical analysis, may be promising for diagnosing early-stage, chemotherapy-induced cardiotoxicity. A longitudinal strain reduction of > 10% from baseline may predict future cardiotoxicity with 78-79% sensitivity and 79-82% specificity.20) However, the clinical implications of deformation imaging for detecting chemotherapy-related cardiotoxicity need to be explored in a large number of patients before it can be clinically applied.31),32)
Ischemic Heart Disease
The morbidity and mortality associated with ischemic heart disease in women is lower than in men. But, unlike the situation in Western countries, the prevalence and mortality of ischemic heart disease in women has steadily increased over the previous two decades in Korea.1),33),34) Early identification of women at risk of ischemic heart disease is of the utmost importance because there is a concern about the excessive mortality among women, especially young women, who have had acute myocardial infarctions, even after successful revascularization therapy.35),36) Moreover, because of the longevity of female patients, the burden of cardiovascular disease is higher than for male patients. The clinical impact and role of prognostic stratification research, focused on the sex-specific diagnostic accuracy of several noninvasive tests designed to detect coronary disease, has been insufficient because women have constituted only about 30% of the clinical trial patients.37),38)
The presentation of ischemic heart disease symptoms in women is frequently atypical, and its pathophysiology appears different from that seen in men. A substantial proportion of women patients with chest pain may not have critical coronary stenosis. However, even without angiographic confirmation of the extent of coronary stenosis, women patients with chest pain have a worse prognosis than age-matched men when they have coronary microvascular dysfunction.39),40)
In the clinic, recognition of coronary heart disease starts with exercise electrocardiogram (ECG) testing in symptomatic patients. Partly because of the lower rate of obstructive coronary disease in women, the sensitivity and specificity of this testing is approximately 65%, which is lower than that reported for men.33),41) The Duke Treadmill Score, a calculated index that combines exercise duration, exercise-induced angina, and ST segment deviations may increase the test's accuracy in symptomatic women.42),43) But ischemic ECG changes may be obscured when the baseline ECG is abnormal, and many women cannot perform sufficient treadmill exercise to achieve an optimal stress burden because of their not being physically conditioned. Together, these factors may limit the use of exercise ECGs for diagnosing ischemic heart disease in women, indicating the need for imaging studies in a large portion of symptomatic women.
Stress echocardiography, using exercise or dobutamine- or adenosine-mediated vasodilation, has been established as an accurate, noninvasive test for diagnosing coronary heart disease in women.44),45),46),47) The development of new, abnormal, regional wall motion during or after stress is considered an indication of myocardial ischemia. The reported sensitivity and specificity of stress echocardiography for diagnosing coronary disease ranges from 80-85%. Besides diagnosing coronary artery disease, the prognostic role of stress echocardiography has been well documented by several researchers.47),48),49) The positive and negative results of stress echocardiography can efficiently discriminate future events. The prognostic value of echocardiography is especially comparable in women and men.49) When abnormal regional wall motion is not induced after exercise or dobutamine stress, the annual event rate of coronary artery disease is < 1% or 2-4%, respectively. The event rate is lower if the patient can exercise, but if the regional wall motion abnormality develops in multiple vascular territories after dobutamine stress, the event rate increases up to 10%.44),50),51) In addition to providing a myocardial ischemia diagnosis, additional anatomical and functional information can be obtained using imaging, without radiation exposure, during echocardiography. Another interesting finding is the induction of dynamic left ventricular outflow tract obstruction during dobutamine infusion (Fig. 2). The clinical significance of dynamic left ventricular outflow obstruction is not well elucidated,52),53),54) but it may be related to the degree of left ventricular remodeling and the presenting symptoms of the patient (presented at the 57th annual scientific meeting of The Korean Society of Cardiology).
Fig. 2.
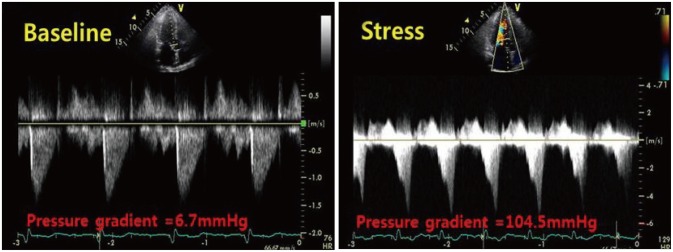
Example of inducible left ventricular outflow obstruction after dobutamine infusion.
Specifically, exercise echocardiography is recommended for women with chest pain and an intermediate to high pretest probability of coronary disease. Dobutamine stress echocardiography may also be used for women who cannot perform the exercise test (Fig. 3).47)
Fig. 3.

American Heart Association proposed algorithm for evaluating symptomatic women using noninvasive tests.47) CVA: cerebrovascular accident, ECG: electrocardiogram, EF: ejection fraction, ETT: exercise treadmill test, LBBB: left branch bundle block, LV: left ventricular, Rx: prescription, TM: treadmill.
As discussed above, more than 50% of women who present for coronary angiography due to chest pain do not have significant coronary stenosis, but they still have increased risks of future cardiovascular events.55),56) Coronary microvascular dysfunction has been advocated as a primary pathophysiologic explanation for this specific type of angina,57) and it is closely related with the risk of atherosclerosis.58) For this specific type of angina, the clinical utility of stress echocardiography, for which the positive criteria is inducible abnormal regional wall motion, is limited.59),60) A clinical investigation of microvascular angina, involving the measurement of transthoracic Doppler coronary flow velocities, before and after adenosine infusion, is now ongoing in a large population, and will clarify the significance of coronary microvascular dysfunction.61) A recent study used speckle tracking echocardiography, layer-specific global longitudinal strain, and strain rate measurements in microvascular angina patients. The study showed that lower increases in the endocardial global longitudinal strain and strain rate by exercise in the patient group compared to the controls.62) However, diagnosing microvascular angina is still difficult and needs further clarification.
Conclusion
In summary, echocardiography is considered to be an essential test for the evaluation of cardiac structures and hemodynamics in many cardiac disorders. The unique characteristics of the test are specifically suitable for repeated patient screening and monitoring during pregnancy and cardiotoxic chemotherapy. Unlike exercise ECGs, the diagnostic accuracy and ability to assess the prognosis of female coronary artery disease patients using stress echocardiography is comparable with that for men. However, in patients with chest pain, but without significant coronary stenosis, additional imaging information regarding the patient's myocardial perfusion status may be necessary. This information may include coronary flow velocity measurements using Doppler imaging, evaluation of myocardial perfusion using myocardial contrast echocardiography, or deformation imaging of the layered left ventricular wall motion.
References
- 1.Statistics Korea. 2013 Death statistics. Deajeon: Statistics Korea; 2014. [Google Scholar]
- 2.Bilhartz TD, Bilhartz PA, Bilhartz TN, Bilhartz RD. Making use of a natural stress test: pregnancy and cardiovascular risk. J Womens Health (Larchmt) 2011;20:695–701. doi: 10.1089/jwh.2010.2291. [DOI] [PubMed] [Google Scholar]
- 3.Miller VM, Garovic VD, Kantarci K, Barnes JN, Jayachandran M, Mielke MM, Joyner MJ, Shuster LT, Rocca WA. Sex-specific risk of cardiovascular disease and cognitive decline: pregnancy and menopause. Biol Sex Differ. 2013;4:6. doi: 10.1186/2042-6410-4-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wenger NK. Gender disparity in cardiovascular disease: bias or biology? Expert Rev Cardiovasc Ther. 2012;10:1401–1411. doi: 10.1586/erc.12.133. [DOI] [PubMed] [Google Scholar]
- 5.Ain DL, Narula J, Sengupta PP. Cardiovascular imaging and diagnostic procedures in pregnancy. Cardiol Clin. 2012;30:331–341. doi: 10.1016/j.ccl.2012.05.002. [DOI] [PubMed] [Google Scholar]
- 6.Savu O, Jurcuţ R, Giuşcă S, van Mieghem T, Gussi I, Popescu BA, Ginghină C, Rademakers F, Deprest J, Voigt JU. Morphological and functional adaptation of the maternal heart during pregnancy. Circ Cardiovasc Imaging. 2012;5:289–297. doi: 10.1161/CIRCIMAGING.111.970012. [DOI] [PubMed] [Google Scholar]
- 7.Cornette J, Ruys TP, Rossi A, Rizopoulos D, Takkenberg JJ, Karamermer Y, Opić P, Van den Bosch AE, Geleijnse ML, Duvekot JJ, Steegers EA, Roos-Hesselink JW. Hemodynamic adaptation to pregnancy in women with structural heart disease. Int J Cardiol. 2013;168:825–831. doi: 10.1016/j.ijcard.2012.10.005. [DOI] [PubMed] [Google Scholar]
- 8.Bamfo JE, Kametas NA, Nicolaides KH, Chambers JB. Maternal left ventricular diastolic and systolic long-axis function during normal pregnancy. Eur J Echocardiogr. 2007;8:360–368. doi: 10.1016/j.euje.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 9.Sliwa K, Hilfiker-Kleiner D, Petrie MC, Mebazaa A, Pieske B, Buchmann E, Regitz-Zagrosek V, Schaufelberger M, Tavazzi L, van Veldhuisen DJ, Watkins H, Shah AJ, Seferovic PM, Elkayam U, Pankuweit S, Papp Z, Mouquet F, McMurray JJ Heart Failure Association of the European Society of Cardiology Working Group on Peripartum Cardiomyopathy. Current state of knowledge on aetiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. Eur J Heart Fail. 2010;12:767–778. doi: 10.1093/eurjhf/hfq120. [DOI] [PubMed] [Google Scholar]
- 10.Karaye KM, Henein MY. Peripartum cardiomyopathy: a review article. Int J Cardiol. 2013;164:33–38. doi: 10.1016/j.ijcard.2011.11.069. [DOI] [PubMed] [Google Scholar]
- 11.Elkayam U. Clinical characteristics of peripartum cardiomyopathy in the United States: diagnosis, prognosis, and management. J Am Coll Cardiol. 2011;58:659–670. doi: 10.1016/j.jacc.2011.03.047. [DOI] [PubMed] [Google Scholar]
- 12.Goland S, Bitar F, Modi K, Safirstein J, Ro A, Mirocha J, Khatri N, Elkayam U. Evaluation of the clinical relevance of baseline left ventricular ejection fraction as a predictor of recovery or persistence of severe dysfunction in women in the United States with peripartum cardiomyopathy. J Card Fail. 2011;17:426–430. doi: 10.1016/j.cardfail.2011.01.007. [DOI] [PubMed] [Google Scholar]
- 13.Vitarelli A, Capotosto L. Role of echocardiography in the assessment and management of adult congenital heart disease in pregnancy. Int J Cardiovasc Imaging. 2011;27:843–857. doi: 10.1007/s10554-010-9750-9. [DOI] [PubMed] [Google Scholar]
- 14.Siu SC, Sermer M, Colman JM, Alvarez AN, Mercier LA, Morton BC, Kells CM, Bergin ML, Kiess MC, Marcotte F, Taylor DA, Gordon EP, Spears JC, Tam JW, Amankwah KS, Smallhorn JF, Farine D, Sorensen S Cardiac Disease in Pregnancy (CARPREG) Investigators. Prospective multicenter study of pregnancy outcomes in women with heart disease. Circulation. 2001;104:515–521. doi: 10.1161/hc3001.093437. [DOI] [PubMed] [Google Scholar]
- 15.Brickner ME. Cardiovascular management in pregnancy: congenital heart disease. Circulation. 2014;130:273–282. doi: 10.1161/CIRCULATIONAHA.113.002105. [DOI] [PubMed] [Google Scholar]
- 16.European Society of Gynecology (ESG); Association for European Paediatric Cardiology (AEPC); German Society for Gender Medicine (DGesGM); Regitz-Zagrosek V, Blomstrom Lundqvist C, Borghi C, Cifkova R, Ferreira R, Foidart JM, Gibbs JS, Gohlke-Baerwolf C, Gorenek B, Iung B, Kirby M, Maas AH, Morais J, Nihoyannopoulos P, Pieper PG, Presbitero P, Roos-Hesselink JW, Schaufelberger M, Seeland U, Torracca L ESC Committee for Practice Guidelines. ESC Guidelines on the management of cardiovascular diseases during pregnancy: the Task Force on the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC) Eur Heart J. 2011;32:3147–3197. doi: 10.1093/eurheartj/ehr218. [DOI] [PubMed] [Google Scholar]
- 17.Asfour V, Murphy MO, Attia R. Is vaginal delivery or caesarean section the safer mode of delivery in patients with adult congenital heart disease? Interact Cardiovasc Thorac Surg. 2013;17:144–150. doi: 10.1093/icvts/ivt110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Omnes S, Jondeau G, Detaint D, Dumont A, Yazbeck C, Guglielminotti J, Luton D, Azria E. Pregnancy outcomes among women with Marfan syndrome. Int J Gynaecol Obstet. 2013;122:219–223. doi: 10.1016/j.ijgo.2013.04.013. [DOI] [PubMed] [Google Scholar]
- 19.Lotrionte M, Biondi-Zoccai G, Abbate A, Lanzetta G, D'Ascenzo F, Malavasi V, Peruzzi M, Frati G, Palazzoni G. Review and meta-analysis of incidence and clinical predictors of anthracycline cardiotoxicity. Am J Cardiol. 2013;112:1980–1984. doi: 10.1016/j.amjcard.2013.08.026. [DOI] [PubMed] [Google Scholar]
- 20.Nolan MT, Lowenthal RM, Venn A, Marwick TH. Chemotherapy-related cardiomyopathy: a neglected aspect of cancer survivorship. Intern Med J. 2014;44:939–950. doi: 10.1111/imj.12532. [DOI] [PubMed] [Google Scholar]
- 21.Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, Hudson MM, Kremer LC, Landy DC, Miller TL, Oeffinger KC, Rosenthal DN, Sable CA, Sallan SE, Singh GK, Steinberger J, Cochran TR, Wilkinson JD American Heart Association Congenital Heart Defects Committee of the Council on Cardiovascular Disease in the Young, Council on Basic Cardiovascular Sciences, Council on Cardiovascular and Stroke Nursing, Council on Cardiovascular Radiolo. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation. 2013;128:1927–1995. doi: 10.1161/CIR.0b013e3182a88099. [DOI] [PubMed] [Google Scholar]
- 22.Curigliano G, Cardinale D, Suter T, Plataniotis G, de Azambuja E, Sandri MT, Criscitiello C, Goldhirsch A, Cipolla C, Roila F ESMO Guidelines Working Group. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO Clinical Practice Guidelines. Ann Oncol. 2012;23(Suppl 7):vii155–vii166. doi: 10.1093/annonc/mds293. [DOI] [PubMed] [Google Scholar]
- 23.Telli ML, Hunt SA, Carlson RW, Guardino AE. Trastuzumab-related cardiotoxicity: calling into question the concept of reversibility. J Clin Oncol. 2007;25:3525–3533. doi: 10.1200/JCO.2007.11.0106. [DOI] [PubMed] [Google Scholar]
- 24.Choueiri TK, Mayer EL, Je Y, Rosenberg JE, Nguyen PL, Azzi GR, Bellmunt J, Burstein HJ, Schutz FA. Congestive heart failure risk in patients with breast cancer treated with bevacizumab. J Clin Oncol. 2011;29:632–638. doi: 10.1200/JCO.2010.31.9129. [DOI] [PubMed] [Google Scholar]
- 25.Kalam K, Marwick TH. Role of cardioprotective therapy for prevention of cardiotoxicity with chemotherapy: a systematic review and meta-analysis. Eur J Cancer. 2013;49:2900–2909. doi: 10.1016/j.ejca.2013.04.030. [DOI] [PubMed] [Google Scholar]
- 26.Sawaya H, Sebag IA, Plana JC, Januzzi JL, Ky B, Tan TC, Cohen V, Banchs J, Carver JR, Wiegers SE, Martin RP, Picard MH, Gerszten RE, Halpern EF, Passeri J, Kuter I, Scherrer-Crosbie M. Assessment of echocardiography and biomarkers for the extended prediction of cardiotoxicity in patients treated with anthracyclines, taxanes, and trastuzumab. Circ Cardiovasc Imaging. 2012;5:596–603. doi: 10.1161/CIRCIMAGING.112.973321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Truong J, Yan AT, Cramarossa G, Chan KK. Chemotherapy-induced cardiotoxicity: detection, prevention, and management. Can J Cardiol. 2014;30:869–878. doi: 10.1016/j.cjca.2014.04.029. [DOI] [PubMed] [Google Scholar]
- 28.Altena R, Perik PJ, van Veldhuisen DJ, de Vries EG, Gietema JA. Cardiovascular toxicity caused by cancer treatment: strategies for early detection. Lancet Oncol. 2009;10:391–399. doi: 10.1016/S1470-2045(09)70042-7. [DOI] [PubMed] [Google Scholar]
- 29.Thavendiranathan P, Grant AD, Negishi T, Plana JC, Popović ZB, Marwick TH. Reproducibility of echocardiographic techniques for sequential assessment of left ventricular ejection fraction and volumes: application to patients undergoing cancer chemotherapy. J Am Coll Cardiol. 2013;61:77–84. doi: 10.1016/j.jacc.2012.09.035. [DOI] [PubMed] [Google Scholar]
- 30.Villarraga HR, Herrmann J, Nkomo VT. Cardio-oncology: role of echocardiography. Prog Cardiovasc Dis. 2014;57:10–18. doi: 10.1016/j.pcad.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 31.Thavendiranathan P, Poulin F, Lim KD, Plana JC, Woo A, Marwick TH. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: a systematic review. J Am Coll Cardiol. 2014;63(25 Pt A):2751–2768. doi: 10.1016/j.jacc.2014.01.073. [DOI] [PubMed] [Google Scholar]
- 32.Lotrionte M, Cavarretta E, Abbate A, Mezzaroma E, De Marco E, Di Persio S, Loperfido F, Biondi-Zoccai G, Frati G, Palazzoni G. Temporal changes in standard and tissue Doppler imaging echocardiographic parameters after anthracycline chemotherapy in women with breast cancer. Am J Cardiol. 2013;112:1005–1012. doi: 10.1016/j.amjcard.2013.05.038. [DOI] [PubMed] [Google Scholar]
- 33.National Heart, Lung, and Blood Institute. Morbidity and mortality: 2012 chart book on cardiovascular, lung, and blood diseases. pp. 28–33. Available at: https://www.nhlbi.nih.gov/files/docs/research/2012_ChartBook_508.pdf.
- 34.Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–2398. doi: 10.1056/NEJMsa053935. [DOI] [PubMed] [Google Scholar]
- 35.de Boer SP, Roos-Hesselink JW, van Leeuwen MA, Lenzen MJ, van Geuns RJ, Regar E, van Mieghem NM, van Domburg R, Zijlstra F, Serruys PW, Boersma E. Excess mortality in women compared to men after PCI in STEMI: an analysis of 11,931 patients during 2000-2009. Int J Cardiol. 2014;176:456–463. doi: 10.1016/j.ijcard.2014.07.091. [DOI] [PubMed] [Google Scholar]
- 36.Vaccarino V, Parsons L, Peterson ED, Rogers WJ, Kiefe CI, Canto J. Sex differences in mortality after acute myocardial infarction: changes from 1994 to 2006. Arch Intern Med. 2009;169:1767–1774. doi: 10.1001/archinternmed.2009.332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sanders GD, Patel MR, Chatterjee R, Ross AK, Bastian LA, Coeytaux RR, Heidenfelder BL, Musty MD, Dolor RJ. Noninvasive technologies for the diagnosis of coronary artery disease in women: future research needs: identification of future research needs from comparative effectiveness review No. 58. Rockville: Agency for Healthcare Research and Quality (US); 2013. Report No.: 13-EHC072-EF. [PubMed] [Google Scholar]
- 38.Wenger NK. Women and coronary heart disease: a century after Herrick: understudied, underdiagnosed, and undertreated. Circulation. 2012;126:604–611. doi: 10.1161/CIRCULATIONAHA.111.086892. [DOI] [PubMed] [Google Scholar]
- 39.Shaw LJ, Bairey Merz CN, Pepine CJ, Reis SE, Bittner V, Kelsey SF, Olson M, Johnson BD, Mankad S, Sharaf BL, Rogers WJ, Wessel TR, Arant CB, Pohost GM, Lerman A, Quyyumi AA, Sopko G WISE Investigators. Insights from the NHLBI-Sponsored Women's Ischemia Syndrome Evaluation (WISE) Study: Part I: gender differences in traditional and novel risk factors, symptom evaluation, and gender-optimized diagnostic strategies. J Am Coll Cardiol. 2006;47(3 Suppl):S4–S20. doi: 10.1016/j.jacc.2005.01.072. [DOI] [PubMed] [Google Scholar]
- 40.Gulati M, Cooper-DeHoff RM, McClure C, Johnson BD, Shaw LJ, Handberg EM, Zineh I, Kelsey SF, Arnsdorf MF, Black HR, Pepine CJ, Merz CN. Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: a report from the Women's Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Arch Intern Med. 2009;169:843–850. doi: 10.1001/archinternmed.2009.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kwok Y, Kim C, Grady D, Segal M, Redberg R. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol. 1999;83:660–666. doi: 10.1016/s0002-9149(98)00963-1. [DOI] [PubMed] [Google Scholar]
- 42.Gulati M, Arnsdorf MF, Shaw LJ, Pandey DK, Thisted RA, Lauderdale DS, Wicklund RH, Al-Hani AJ, Black HR. Prognostic value of the duke treadmill score in asymptomatic women. Am J Cardiol. 2005;96:369–375. doi: 10.1016/j.amjcard.2005.03.078. [DOI] [PubMed] [Google Scholar]
- 43.Alexander KP, Shaw LJ, Shaw LK, Delong ER, Mark DB, Peterson ED. Value of exercise treadmill testing in women. J Am Coll Cardiol. 1998;32:1657–1664. doi: 10.1016/s0735-1097(98)00451-3. [DOI] [PubMed] [Google Scholar]
- 44.Shaw LJ, Vasey C, Sawada S, Rimmerman C, Marwick TH. Impact of gender on risk stratification by exercise and dobutamine stress echocardiography: long-term mortality in 4234 women and 6898 men. Eur Heart J. 2005;26:447–456. doi: 10.1093/eurheartj/ehi102. [DOI] [PubMed] [Google Scholar]
- 45.Marwick TH, Anderson T, Williams MJ, Haluska B, Melin JA, Pashkow F, Thomas JD. Exercise echocardiography is an accurate and cost-efficient technique for detection of coronary artery disease in women. J Am Coll Cardiol. 1995;26:335–341. doi: 10.1016/0735-1097(95)80004-z. [DOI] [PubMed] [Google Scholar]
- 46.Vavas E, Hong SN, Rosen SE, Mieres JH. Noninvasive diagnostic techniques for coronary disease in women. Clin Cardiol. 2012;35:149–155. doi: 10.1002/clc.21953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mieres JH, Shaw LJ, Arai A, Budoff MJ, Flamm SD, Hundley WG, Marwick TH, Mosca L, Patel AR, Quinones MA, Redberg RF, Taubert KA, Taylor AJ, Thomas GS, Wenger NK Cardiac Imaging Committee, Council on Clinical Cardiology, and the Cardiovascular Imaging and Intervention Committee, Council on Cardiovascular Radiology and Intervention, American Heart Association. Role of noninvasive testing in the clinical evaluation of women with suspected coronary artery disease: Consensus statement from the Cardiac Imaging Committee, Council on Clinical Cardiology, and the Cardiovascular Imaging and Intervention Committee, Council on Cardiovascular Radiology and Intervention, American Heart Association. Circulation. 2005;111:682–696. doi: 10.1161/01.CIR.0000155233.67287.60. [DOI] [PubMed] [Google Scholar]
- 48.Dodi C, Cortigiani L, Masini M, Olivotto I, Azzarelli A, Nannini E. The incremental prognostic value of pharmacological stress echo over exercise electrocardiography in women with chest pain of unknown origin. Eur Heart J. 2001;22:145–152. doi: 10.1053/euhj.2000.2321. [DOI] [PubMed] [Google Scholar]
- 49.Arruda-Olson AM, Juracan EM, Mahoney DW, McCully RB, Roger VL, Pellikka PA. Prognostic value of exercise echocardiography in 5,798 patients: is there a gender difference? J Am Coll Cardiol. 2002;39:625–631. doi: 10.1016/s0735-1097(01)01801-0. [DOI] [PubMed] [Google Scholar]
- 50.Metz LD, Beattie M, Hom R, Redberg RF, Grady D, Fleischmann KE. The prognostic value of normal exercise myocardial perfusion imaging and exercise echocardiography: a meta-analysis. J Am Coll Cardiol. 2007;49:227–237. doi: 10.1016/j.jacc.2006.08.048. [DOI] [PubMed] [Google Scholar]
- 51.Shaw LJ, Tandon S, Rosen S, Mieres JH. Evaluation of suspected ischemic heart disease in symptomatic women. Can J Cardiol. 2014;30:729–737. doi: 10.1016/j.cjca.2013.09.019. [DOI] [PubMed] [Google Scholar]
- 52.Câmara EJ, Oliveira MM, Ribeiro FM. Baseline echocardiographic predictors of dynamic intraventricular obstruction of the left ventricle during dobutamine stress echocardiogram. Echocardiography. 2009;26:1195–1203. doi: 10.1111/j.1540-8175.2009.00953.x. [DOI] [PubMed] [Google Scholar]
- 53.Dawn B, Paliwal VS, Raza ST, Mastali K, Longaker RA, Stoddard MF. Left ventricular outflow tract obstruction provoked during dobutamine stress echocardiography predicts future chest pain, syncope, and near syncope. Am Heart J. 2005;149:908–916. doi: 10.1016/j.ahj.2004.07.029. [DOI] [PubMed] [Google Scholar]
- 54.Pellikka PA, Oh JK, Bailey KR, Nichols BA, Monahan KH, Tajik AJ. Dynamic intraventricular obstruction during dobutamine stress echocardiography. A new observation. Circulation. 1992;86:1429–1432. doi: 10.1161/01.cir.86.5.1429. [DOI] [PubMed] [Google Scholar]
- 55.Bairey Merz CN, Shaw LJ, Reis SE, Bittner V, Kelsey SF, Olson M, Johnson BD, Pepine CJ, Mankad S, Sharaf BL, Rogers WJ, Pohost GM, Lerman A, Quyyumi AA, Sopko G WISE Investigators. Insights from the NHLBI-Sponsored Women's Ischemia Syndrome Evaluation (WISE) Study: Part II: gender differences in presentation, diagnosis, and outcome with regard to gender-based pathophysiology of atherosclerosis and macrovascular and microvascular coronary disease. J Am Coll Cardiol. 2006;47(3 Suppl):S21–S29. doi: 10.1016/j.jacc.2004.12.084. [DOI] [PubMed] [Google Scholar]
- 56.Shaw LJ, Shaw RE, Merz CN, Brindis RG, Klein LW, Nallamothu B, Douglas PS, Krone RJ, McKay CR, Block PC, Hewitt K, Weintraub WS, Peterson ED American College of Cardiology-National Cardiovascular Data Registry Investigators. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry. Circulation. 2008;117:1787–1801. doi: 10.1161/CIRCULATIONAHA.107.726562. [DOI] [PubMed] [Google Scholar]
- 57.Pepine CJ, Anderson RD, Sharaf BL, Reis SE, Smith KM, Handberg EM, Johnson BD, Sopko G, Bairey Merz CN. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women's Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55:2825–2832. doi: 10.1016/j.jacc.2010.01.054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Dhawan SS, Corban MT, Nanjundappa RA, Eshtehardi P, McDaniel MC, Kwarteng CA, Samady H. Coronary microvascular dysfunction is associated with higher frequency of thin-cap fibroatheroma. Atherosclerosis. 2012;223:384–388. doi: 10.1016/j.atherosclerosis.2012.05.034. [DOI] [PubMed] [Google Scholar]
- 59.Nihoyannopoulos P, Kaski JC, Crake T, Maseri A. Absence of myocardial dysfunction during stress in patients with syndrome X. J Am Coll Cardiol. 1991;18:1463–1470. doi: 10.1016/0735-1097(91)90676-z. [DOI] [PubMed] [Google Scholar]
- 60.Picano E, Lattanzi F, Masini M, Distante A, L'Abbate A. Usefulness of a high-dose dipyridamole-echocardiography test for diagnosis of syndrome X. Am J Cardiol. 1987;60:508–512. doi: 10.1016/0002-9149(87)90295-5. [DOI] [PubMed] [Google Scholar]
- 61.Prescott E, Abildstrøm SZ, Aziz A, Merz NB, Gustafsson I, Halcox J, Hansen HS, Hansen PR, Kastrup J, Michelsen M, Mygind ND, Ong P, Pena A, Rosengren A, Sechtem U, Søgaard P. Improving diagnosis and treatment of women with angina pectoris and microvascular disease: the iPOWER study design and rationale. Am Heart J. 2014;167:452–458. doi: 10.1016/j.ahj.2014.01.003. [DOI] [PubMed] [Google Scholar]
- 62.Cadeddu C, Nocco S, Deidda M, Pau F, Colonna P, Mercuro G. Altered transmural contractility in postmenopausal women affected by cardiac syndrome X. J Am Soc Echocardiogr. 2014;27:208–214. doi: 10.1016/j.echo.2013.09.014. [DOI] [PubMed] [Google Scholar]