

Abstract
We report a case of primary gastric malignant melanoma that was diagnosed after curative resection but initially misdiagnosed as adenocarcinoma. A 68-year-old woman was referred to our department for surgery for gastric adenocarcinoma presenting as a polypoid lesion with central ulceration located in the upper body of the stomach. The preoperative diagnosis was confirmed by endoscopic biopsy. We performed laparoscopic total gastrectomy, and the final pathologic evaluation led to the diagnosis of primary gastric malignant melanoma without a primary lesion detected in the body. To the best of our knowledge, primary gastric malignant melanoma is extremely rare, and this is the first case reported in our country. According to the literature, it has aggressive biologic activity compared with adenocarcinoma, and curative resection is the only promising treatment strategy. In our case, the patient received an early diagnosis and underwent curative gastrectomy with radical lymphadenectomy, and no recurrence was noted for about two years.
Keywords: Melanoma, Stomach, Primary malignant
Introduction
Malignant melanoma is a tumor of the melanocytes with high malignant potential. Malignant melanoma arises usually in the skin or less frequently in the eyes. Occasionally, it is found in the gastrointestinal (GI) tract. However, malignant melanomas of the GI tract are mostly metastases from a primary cutaneous tumor. Primary malignant tumors in the GI tract are usually adenocarcinomas, and melanomas are rare. Specifically, a melanoma located primarily in the gastric mucosa is extremely rare. We report an extremely rare case of primary malignant melanoma mimicking adenocarcinoma arising in the upper body of the stomach.
Case Report
A 68-year-old woman was referred to our department after gastroscopy, which showed a mass in the stomach. She had undergone total abdominal hysterectomy with bilateral salpingo-oophorectomy because of an ovarian serous carcinoma (stage IIIa) nine years ago. On routine workup, gastroscopy showed a round mass, approximately 3 cm in diameter, in the upper body on the greater curvature side of the stomach (Fig. 1).
Fig. 1.
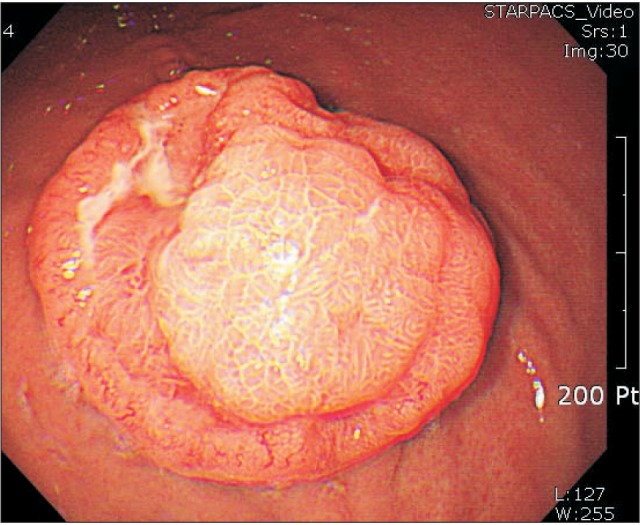
Grossly, the tumor was a round, polypoid lesion with central ulceration on gastroscopy.
A biopsy was performed and histologic examination indicated a poorly differentiated adenocarcinoma. Tumor markers including carcinoembryonic antigen and carbohydrate antigen 19-9 were within the normal ranges. Contrast-enhanced computed tomography showed focal, eccentric, enhancing wall thickening in the greater curvature of the stomach body and no significantly enlarged perigastric lymph nodes (Fig. 2). We diagnosed the patient with gastric adenocarcinoma and performed a laparoscopic-assisted total gastrectomy with D2 lymphadenectomy. No ascites or peritoneal lesion was observed. Reconstruction was performed with a Roux-en-Y anastomosis.
Fig. 2.

Computed tomography showed a focal enhancing wall thickening in the greater curvature of the upper body of the stomach. Enlarged perigastric lymph nodes were not noted.
The resected specimen contained a polypoid tumor with central ulceration 3 cm in diameter (Fig. 3). Tumor cells had spread through the submucosal layer of the stomach with clear resection margins (Fig. 4). None of the 44 resected lymph nodes were positive for metastasis, but lymphatic tumor emboli were detected by immunostaining with CD-31 and D2-40 antibodies (Fig. 5). The tumor cells showed atypical hyperchromatic nuclei (Fig. 6) and accompanying melanin distribution within the tumor nest (Fig. 7). Immunohistochemical examination revealed a positive reaction to HMB-45 antibodies and S-100 proteins and a negative reaction to cytokeratin antibodies (Fig. 8).
Fig. 3.
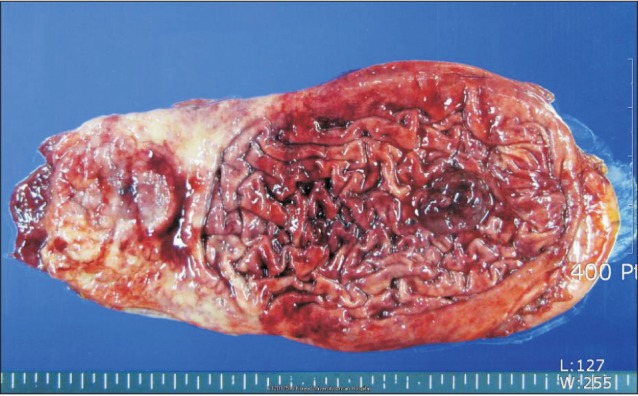
Photograph of the gross specimen that contained a polypoid tumor with central ulceration 3 cm in diameter located in the greater curvature of the upper body of the stomach.
Fig. 4.
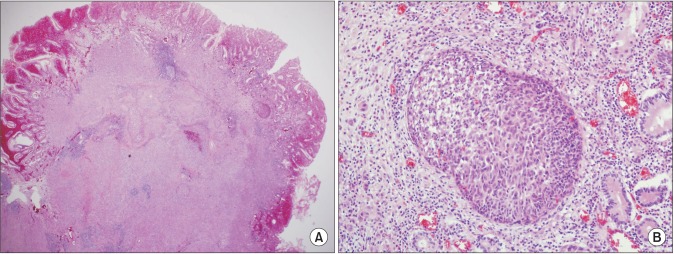
Microscopic findings showed that tumor cells were spreading through the submucosal layer of the stomach with a clear resection margin (A: H&E, ×20; B: H&E, ×200).
Fig. 5.
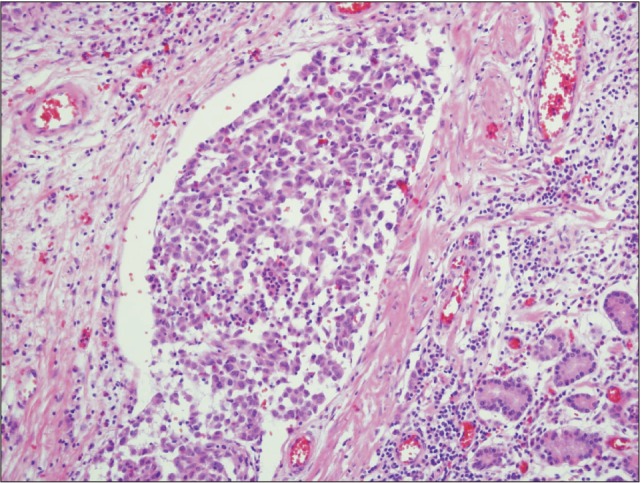
Findings of immunohistochemical staining: lymphatic tumor emboli were noted by immunostaining with CD-31 and D2-40 antibody (×200).
Fig. 6.
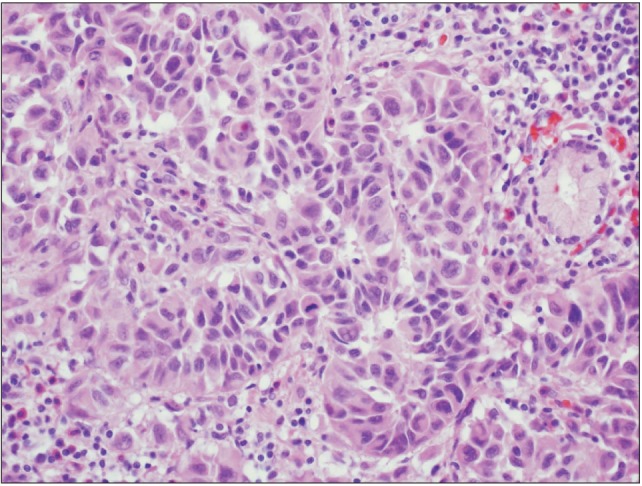
The tumor cells contained atypical hyperchromatic nuclei on H&E staining (×400).
Fig. 7.
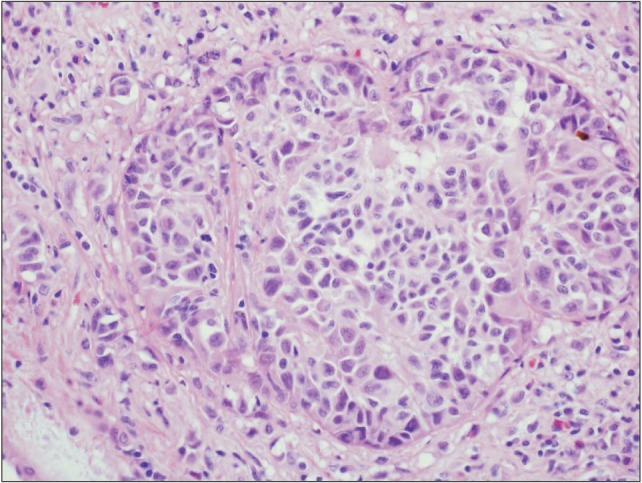
The tumor nest was accompanied by melanin on H&E staining (×400).
Fig. 8.
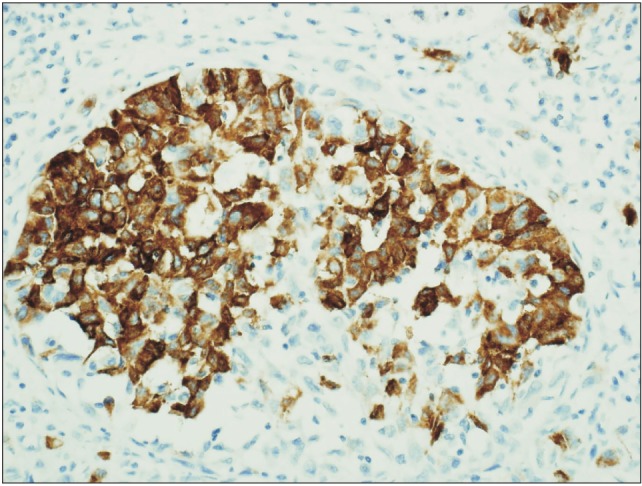
Immunohistochemical examination revealed a positive reaction with HMB-45 antibodies and S-100 proteins and a negative reaction with cytokeratin antibodies (immunostaining, ×200).
Based on these findings, we diagnosed the patient with malignant melanoma. In the pathologic examination, the depth of tumor involvement was to the submucosal level and no metastasis showed in 44 lymph nodes. Therefore, the final pathologic tumor's TNM stage was pT1bN0M0. Postoperatively, further examinations were performed to identify the primary tumor or other metastatic foci. Ophthalmologic, dermatologic, and oral examinations showed negative findings. Positron emission tomography/computed tomography was performed, but no hot spots were detected (Fig. 9). These results indicated a final diagnosis of primary malignant melanoma of the stomach. After total gastrectomy, a follow-up study was performed with abdominal computed tomography scans at 3, 6, 12, 18, and 24 months (5 times) over the course of 2 years and there was no recurrence. The TNM tumor stage was early (pT1bN0M0); therefore, we did not perform any adjuvant chemotherapy, but the patient has taken oral immunotherapeutic medication for 4 months.
Fig. 9.

Positron emission tomography/computed tomography scan showed no other hot spots except the stomach cancer portion.
Discussion
Malignant melanomas of the GI tract are rare. Most of them are metastases from cutaneous lesions and are reported in up to 4% of patients who are alive and in up to 60% of patients at autopsy.1,2,3,4 Primary GI melanomas are very rare and have been reported to arise in the esophagus, anorectum, and small intestine.5 Primary gastric melanoma has also been reported sporadically.6,7,8,9,10 An autopsy series of patients with melanoma revealed gastric metastasis rates of more than 22%.4 The median overall survival associated with primary malignant melanoma of the GI tract is reportedly 17 months, whereas that associated with primary malignant melanoma of the stomach is only 5 months.11 Criteria for the diagnosis of primary malignant melanoma of the GI tract include the absence of other primary site melanomas and no history of melanoma or atypical melanocytic lesion removal from the skin or other organs.6 On diagnosis, the computed tomography scan is commonly used to detect intra-abdominal lesions. Also, the positron emission tomography/computed tomography scan has been shown to have higher sensitivity and accuracy in the detection of visceral metastases, including extra-intestinal metastatic disease.12 Since there are no melanocytes in the stomach, gastric melanoma may originate from ectopic melanocytes that migrate to the GI tract during embryogenesis or differentiation of amine precursor uptake and decarboxylation cells to melanocytes.13 Surgical resection is the only identifiable treatment modality for which independent predictive prognostic values have been demonstrated.11 Systemic chemotherapy regimens show no benefit in overall survival and are not recommended for the treatment of malignant GI melanomas.14 In this case, we initially misdiagnosed the mass as adenocarcinoma of the stomach in the biopsied tumor cell specimens obtained during endoscopic examination. We supposed that the initial biopsied tumor cells might have been so scanty that they resembled poorly differentiated adenocarcinoma in the pathologic view. The patient had a history of tubular adenoma with high-grade dysplasia in the angular portion of the stomach three years ago and had undergone endoscopic mucosal resection. Therefore, we mistook the mass as adenocarcinoma from the intestinal metaplastic precancerous lesion, and the grossly protruding tumor resembled Borrmann type I or early gastric cancer type I. However, this lesion was located away from the previous site of dysplasia and was not associated with it.
During the pathologic examination of the resected specimen, the tumor appearance differed from ordinary adenocarcinoma. Therefore, we performed immunohistochemical staining with several markers, and the results were positive for HMB45, S-100, and vimentin and negative for cytokeratin, CAM5.2, chromogranin, and synaptophysin. This patient was finally diagnosed with primary malignant melanoma based on the immunohistochemical staining results. After curative laparoscopic total gastrectomy, the patient received routine follow-up, and there was no recurrence for two years.
References
- 1.Elsayed AM, Albahra M, Nzeako UC, Sobin LH. Malignant melanomas in the small intestine: a study of 103 patients. Am J Gastroenterol. 1996;91:1001–1006. [PubMed] [Google Scholar]
- 2.Woollons A, Derrick EK, Price ML, Darley CR. Gastrointestinal malignant melanoma. Int J Dermatol. 1997;36:129–131. doi: 10.1111/j.1365-4362.1997.tb03072.x. [DOI] [PubMed] [Google Scholar]
- 3.Liang KV, Sanderson SO, Nowakowski GS, Arora AS. Metastatic malignant melanoma of the gastrointestinal tract. Mayo Clin Proc. 2006;81:511–516. doi: 10.4065/81.4.511. [DOI] [PubMed] [Google Scholar]
- 4.Patel JK, Didolkar MS, Pickren JW, Moore RH. Metastatic pattern of malignant melanoma. A study of 216 autopsy cases. Am J Surg. 1978;135:807–810. doi: 10.1016/0002-9610(78)90171-x. [DOI] [PubMed] [Google Scholar]
- 5.Lagoudianakis EE, Genetzakis M, Tsekouras DK, Papadima A, Kafiri G, Toutouzas K, et al. Primary gastric melanoma: a case report. World J Gastroenterol. 2006;12:4425–4427. doi: 10.3748/wjg.v12.i27.4425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yamamura K, Kondo K, Moritani S. Primary malignant melanoma of the stomach: report of a case. Surg Today. 2012;42:195–199. doi: 10.1007/s00595-011-0077-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Goral V, Ucmak F, Yildirim S, Barutcu S, Ileri S, Aslan I, et al. Malignant melanoma of the stomach presenting in a woman: a case report. J Med Case Rep. 2011;5:94. doi: 10.1186/1752-1947-5-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alazmi WM, Nehme OS, Regalado JJ, Rogers AI. Primary gastric melanoma presenting as a nonhealing ulcer. Gastrointest Endosc. 2003;57:431–433. doi: 10.1067/mge.2003.120. [DOI] [PubMed] [Google Scholar]
- 9.Germano D, Rosati G, Romano R, Vita G, Lepore G, De Sanctis D, et al. Primary gastric melanoma presenting as a double ulcer. J Clin Gastroenterol. 2004;38:828. doi: 10.1097/01.mcg.0000139030.08074.da. [DOI] [PubMed] [Google Scholar]
- 10.Jelincic Z, Jakic-Razumovic J, Petrovic I, Cavcic AM, Unusic J, Trotic R. Primary malignant melanoma of the stomach. Tumori. 2005;91:201–203. doi: 10.1177/030089160509100219. [DOI] [PubMed] [Google Scholar]
- 11.Cheung MC, Perez EA, Molina MA, Jin X, Gutierrez JC, Franceschi D, et al. Defining the role of surgery for primary gastrointestinal tract melanoma. J Gastrointest Surg. 2008;12:731–738. doi: 10.1007/s11605-007-0417-3. [DOI] [PubMed] [Google Scholar]
- 12.Marsden JR, Newton-Bishop JA, Burrows L, Cook M, Corrie PG, Cox NH, et al. British Association of Dermatologists Clinical Standards Unit. Revised UK guidelines for the management of cutaneous melanoma 2010. Br J Dermatol. 2010;163:238–256. doi: 10.1111/j.1365-2133.2010.09883.x. [DOI] [PubMed] [Google Scholar]
- 13.Krausz MM, Ariel I, Behar AJ. Primary malignant melanoma of the small intestine and the APUD cell concept. J Surg Oncol. 1978;10:283–288. doi: 10.1002/jso.2930100402. [DOI] [PubMed] [Google Scholar]
- 14.Verma S, Petrella T, Hamm C, Bak K, Charette M Melanoma Disease Site Group of Cancer Care Ontario's Program in Evidence-based Care. Biochemotherapy for the treatment of metastatic malignant melanoma: a clinical practice guideline. Curr Oncol. 2008;15:85–89. [PMC free article] [PubMed] [Google Scholar]