

Summary
Background
Clinical and research data are essential for patient care, research and healthcare system planning. REDCapTM is a web-based tool for research data curatorship developed at Vanderbilt University in Nashville, USA. The Faculty of Health Sciences at the University of the Witwatersrand, Johannesburg South Africa identified the need for a cost effective data management instrument. REDCap was installed as per the user agreement with Vanderbilt University in August 2012.
Objectives
In order to assist other institutions that may lack the in-house Information Technology capacity, this paper describes the installation and support of REDCap and incorporates an analysis of user uptake over the first year of use.
Methods
We reviewed the staffing requirements, costs of installation, process of installation and necessary infrastructure and end-user requests following the introduction of REDCap at Wits. The University Legal Office and Human Research Ethics Committee were consulted regarding the REDCap end-user agreement. Bi-monthly user meetings resulted in a training workshop in August 2013. We compared our REDCap software user numbers and records before and after the first training workshop.
Results
Human resources were recruited from existing staff. Installation costs were limited to servers and security certificates. The total costs to provide a functional REDCap platform was less than $9000. Eighty-one (81) users were registered in the first year. After the first training workshop the user numbers increased by 59 in one month and the total number of active users to 140 by the end of August 2013. Custom software applications for REDCap were created by collaboration between clinicians and software developers.
Conclusion
REDCap was installed and maintained at limited cost. A small number of people with defined skills can support multiple REDCap users in two to four hours a week. End user training increased in the number of users, number of projects created and the number of projects moved to production.
Keywords: Database management systems, medical informatics, electronic data capture, clinical research, translational research
1. Background
South Africa is a middle-income country with an escalating quadruple burden of diseases. Namely, poverty related diseases, non-communicable diseases, communicable diseases and violence related diseases [1]. Clinical and research data acquisition, storage and management are essential for patient care, basic and translational research and healthcare strategy and planning. At the University of the Witwatersrand (Wits), Johannesburg Faculty of Health Sciences, clinical practice and research is spread over three geographically separate academic teaching platforms. These academic platforms service approximately 5200 inpatient beds. Each platform has varying policies and practices for data capture and management. In addition, large amounts of data are collected at rural research sites, which are often distant from the institutional complex. The University does not currently have a universal policy regarding data curatorship.
The staff complement in the Faculty of Health Sciences includes well over 2500 academics, comprising both non-clinical and clinical staff. In this group are included over 700 residents in training to be specialists and who are required to carry out research as part of their training [2]. The academic staff is spread throughout the Johannesburg metropolitan area and to rural hospitals in other provinces of South Africa. This geographic distribution of staff and services affects data capture, data access, and ultimately patient care. Consequently the relevant research to guide treatment, inform management and plan strategic policy is limited.
The Faculty of Health Sciences is constrained in providing a data acquisition and curatorship instrument by limited funds and a paucity of specialist information technology skills.
Until recently, researchers in the Faculty of Health Sciences have been responsible for their own data management. This often takes the format of paper-based records and/or spreadsheets. Data storage, privacy and security are variable and dependent on the individual researcher. Advice and support for data management is available from the University Library in the form of a web link [3]. However, there is limited support for electronic database design and maintenance.
Developing the capacity for accurate and reliable data acquisition was thus our first step in strengthening the research endeavor in our Faculty. Inadequate computer facilities and/or computer software are listed as a constraint to research in almost 50% (9/19) of cohort studies in India, Mexico, Nigeria, South Africa, Sweden, Tanzania and Uganda [4]. Moreover 13 of 19 cohort study leaders (72%) listed database management as a constraint to research [4]. In addition, information systems are listed as a limiting capacity for the implementation of the WHO Millennium Development Goals. An obvious strategy for strengthening capacity is to integrate existing knowledge into practice [5]. Clinical and translational research requires a robust and secure manner in which to collect, store, transfer and analyze data [6]. Researchers require environment specific data management tools in order to undertake accurate, safe and secure data curatorship. An independent researcher may not have access to formal informatics and data management resources. Health care researchers often have limited information technology and computer skills. Emergent researchers find this to be another constraint in carrying out research [5]. Data quality is improved by enabling data collection by a diverse team [7].
REDCap is a web based software tool developed at the Centre for Clinical and Translational Research at Vanderbilt University in Nashville, Tennessee, USA. REDCap provides researchers with a tool for design and development of electronic data capture tools [6]. The strength and utility of REDCap is supported by web based training materials in the form of prerecorded tutorials, online webinars, and help documentation, most of which are integrated into the software itself [8]. REDCap allows the researcher to choose and define their data elements. Although this may limit interoperability, it is a consequence of the user-defined metadata model. Each individual REDCap user has sole discretion as to who has access to their data. REDCap has a growing international user base with 937 institutional partners in 75 countries at time of writing [9]. The geographic distribution is concentrated in North America and Europe. In the latter part of 2013, Africa had approximately 26 institutional partners of which five were in South Africa [9]. The REDCap consortium provides education and support including two weekly online conferences, one for REDCap users and one for software technical support.
2. Objective
In order to assist other institutions that may lack the necessary in house Information Technology capacity to set up a functional instrument for data support, this paper describes our experience of the installation, infrastructure requirements and user support for REDCap. We include an analysis of end users after the first year.
3. Methods
In July 2012, the Wits Faculty of Health Sciences installed REDCap in terms of the user agreement with Vanderbilt University [9]. The user agreement allows academic and non-profit institutions to download the REDCap software at no cost. After ensuring system stability, REDCap was opened for accredited users in August 2012.
According to the REDCap nomenclature a project is a collection of instruments that allow data curatorship for one study. An instrument may be a survey or a form or a combination of both. Each survey or form has a collection of fields. A project is moved from development to production when the user is comfortable with the design and function of the project. The project was initiated and managed by a group consisting of three academic staff.
A physician with an interest in clinical data management (Faculty of Health Sciences)
A research scientist assigned as the REDCap administrator (Faculty of Health Sciences)
A computer scientist with experience in bioinformatics, for software and server support (School of Electrical and Information Engineering).
The faculty of Health Sciences has recognized the need for information technology support. Dedicated time for the maintenance and support of REDCap was deemed a priority. The three staff each had specific time allocated to the REDCap project away from their core responsibilities from their relevant departments. This brought together the necessary expertise without financial cost to the faculty. The REDCap administrator was allocated 0.2 Full Time Equivalents (FTE), 0.1 FTE for the lead clinician and 0.05 FTE for server and software support. Postgraduate computer science students were employed at University rates to create added functionality (ReportMyWay and a link to the Vermont Oxford Network (Wits2VON)).
3.1. Installation, Hardware and Software Support
The structure and functionality of REDCap is well described elsewhere [6, 9]. The installation of the REDCap software requires specific information technology expertise related to servers, security and access settings, systems backup and maintenance. No clinicians at our institution had the requisite skills. A colleague from the School of Electrical and Information Engineering assisted with the installation and maintenance of the hardware and software. This cross-Faculty collaboration was essential for creating a stable platform for REDCap. The instructions for the installation of REDCap are available on the website [9].
A summary of our experience follows. The installation and maintenance of REDCap can be split into two parts. The installation of the REDCap software, and the infrastructural and environmental considerations.
3.1.1 The Installation of the Redcap Software
The installation of the REDCap Software requires basic system administration skills (in our case Linux). Although possible to use existing machines, it is good practice to install and run REDCap on dedicated machines. The systems administrator must be competent at installing and upgrading software on Linux systems and have knowledge of the basics of MySQL. The installation documentation for REDCap is comprehensive and a good Graphical User Interface is provided through myPHP.
The initial installation of REDCap took one day, although with experience it could be done in less time. REDCap systems upgrades are released regularly and require only 15 minutes to install. Operating systems updates must be done regularly, but are easy to automate or semi-automate.
3.1.2 Infrastructure and Environmental Considerations
This is particularly important, as REDCap is a mission critical system. As user numbers grow, more researchers use the system and system failure or downtime becomes more problematic. Planning for scalability and reliability is crucial. Each organization needs to take this into account. This requires planning and a reasonable level of expertise with virtualization software and file systems.
For reliability, we do risks assessment — what faults are we mitigating against, their probability of occurring and the damage caused if there is fault. We consider both the recoverability of the data and availability of the REDCap service. In our case, a single computer or disk failure over the lifetime of the system is a likely occurrence and we must protect against it. A catastrophic failure in our server room that may affect more than one machine (e.g. a fire) is highly unlikely but we feel we need to protect against it. A city-wide catastrophe like an earthquake is not a risk we mitigate against in our environment.
Our risk policy is:
If the machine on which our REDCap services fail, we wish to lose no more than 24 hours of data update, and we want our REDCap service to be up and running within 24 hours.
If there is a more catastrophic failure, which wipes out two independent systems in our secure data center, then we wish to lose no more than a week’s data. In this event, a REDCap system would have to be installed from scratch and the time taken to get running again would depend on the nature of the failure, but in a realistic scenario some sort of service should be available within a further week.
It is recommended that REDCap be run as two machines: a database server, and the REDCap front-end.
A practical and desirable way of running this is to set up these as virtual machines. Virtualization is a technology that allows one physical computer to run one several “virtual” computers, which share the physical hosts’ resources. These virtual machines behave and appear both externally and internally as if they were real computers.
Virtualization has a small performance penalty but has several advantages. It allows resources to be shared making systems more cost effective. And although multiple virtual machines may run on the same physical machine, they each run in their own container thereby promoting security and reliability. Finally, the state or “image” of a virtual machine may be saved, and moved to another physical machine, which allows quicker recovery from physical failure.
There are different virtualization systems available. For our main REDCap system we use a system called KVM [10], but we have also very successfully used Oracle’s VirtualBox system, which runs on a range of computer systems.
Management of file storage is important. The Logical Volume Manager (LVM) [11] is a very flexible way of managing physical storage, allowing several physical disks to managed as one unit, and then partitioning this into logical volumes. These logical volumes can easily be archived, and moved to other physical machines.
For a REDCap system which will support many projects over an extended period, the combination of KVM and LVM makes the management of the underlying physical systems more flexible and robust. To accomplish this level of service, we do the following:
A daily backup is made of the SQL database and REDCap uploads, and kept on a separate machine on a RAID6 disk. For the SQL database, we keep copies of the last 7 days and then weekly snapshots for the previous 7 weeks. This means that three disks would need to fail independently to lose our data.
On a third machine, we make weekly copies of our virtual machine images. This acts as an additional weekly backup of the data, but more importantly means that should our REDCap physical machine fail, we can get the REDCap virtual machines running again on another virtual host, and just restore the database to a more recent state from the daily backup.
Finally, on a weekly basis, a copy of the current database and uploads folder is encrypted and copied to a site at a neighboring university. If there were catastrophic failure in our server room, we would lose no more than a week’s worth of data.
It is difficult to estimate the overall cost of establishing this infrastructure, especially as some of the costs are amortized with other projects. However, a realistic estimate is that the overall cost of installing and running REDCap has been about one-person month of a skilled system administrator over a two-year period.
For our one-project installations on a MacMiniTM, backup is done using Apple’s TimeMachineTM with periodic upload of the SQL database to a central server.
In summary, the cost and expertise in installing REDCap itself is not onerous. It is a stable package that has good documentation and support. However for a system that supports many users and is mission critical, a higher degree of expertise is needed to ensure the system works reliably.
3.2 User Defined Software Development
REDCap is designed as a dynamic instrument. Institutional partners may modify and expand the capacity of the source software. This benefits both the end-user and the REDCap community. A user may tailor the software to their own specific needs and share this added functionality with the greater REDCap community.
Two of our projects are worthy of mention. The first was in response to multiple requests for a user defined printout of completed datasheets we called ReportMyWay. In its native form REDCap generates a PDF document with all fields included. This can result in a bulky redundant paper document especially when branching logic is used. ReportMyWay allows end users to select only chosen fields for a printable report.
The second custom application was a data link between one of our REDCap databases and the Vermont Oxford Network database to allow safe and effective transfer between the two and is termed the Wits2VON plugin.
The Wits2VON plugin makes use of a PHP plugin to the REDCap system. eNICQ software is made available to all Vermont Oxford Members as a benefit of membership. The eNICQ application supports the importing of data via tables in its own database. This database is run on the Microsoft SQL Server architecture (MSSQL). Since the PHP programming language supports the querying of an MSSQL database, the plugin accomplished data transfer to eNICQ via this querying.
In summary the Wits2VON plugin retrieves data from a REDCap database via standard PHP querying of a MySQL database. The plugin processes this data, sorting into the exact format which the eNICQ application requires, as described in a document which the Vermont Oxford Network provides to developers [12].
The Wits2VON plugin connects to the remote server running the eNICQ application and places all the formatted data into the eNICQ database. The eNICQ application now has access to this data.
3.3 Legal and Ethical Considerations
Technology tends to evolve faster than legislation and the Internet has created new legal and ethical questions. The University Legal Office and the Human Research Ethics Committee (HREC) were consulted regarding the REDCap non-profit end-user agreement. Two common areas of concern were; the site of data storage, and who may have access to the data captured using REDCap.
Following discussion an institutional user agreement was created with input from the Wits REDCap team and the University Legal Office to inform our users. The process of liaison with the Legal Office and the Human Research Ethics Committee within the institution was a bidirectional learning process.
The installation of REDCap was completed in July 2012. For the first month the group created test projects and validated the functioning of REDCap on our servers. Data security and backup were verified and the stability of the REDCap software on the University system was tested. Only when we were satisfied with the integrity of the installation did we open it to our end users. The fully functional software was made available to users on 7 August 2012.
3.4 Hands on Training
Bi-monthly Wits-REDCap user-group meetings were hosted by the REDCap administrator for feedback from users. A consistent request for hands-on training resulted in a formal workshop in August 2013.
3.5. Data Collection
We reviewed our user numbers graphs and correlated them with the hands-on REDCap workshop. The REDCap software keeps a record of concurrent users, daily user logins, projects created, projects moved to production, active users, first-time visitors, logged events and page hits. News of the REDCap installation was spread by word of mouth, presentation at Faculty research fora and via the Faculty research communication infrastructure.
We assessed user numbers, number of projects created and number of projects moved from development to production before and after a hands-on REDCap training workshop. The workshop was conducted by the REDCap administrator in a computer laboratory. Each user had access to an internet-connected computer terminal. The first REDCap computer workshop with hands-on training was conducted in August 2013. The number of attendees at the workshop was limited to 40. The aim of the workshop was to guide new users through the steps of creating a REDCap project of their own.
4. Results
4.1. Budget
In order to set up the support system, a number of costs were incurred. Two servers were purchased at a cost of R80000.00 (US$ 8000) through the Institution’s Strategic Planning and Allocation of Resources Committee (SPARC) fund. Each server has dual Xeon E5-2620 processors, 6TB of disk and 32GB of RAM. The REDCap and database servers run as virtual machines on the one while the other acts as a backup device. The databases are backed up daily and several copies are kept on site. Once a week a copy is encrypted and stored off-site. Security certificates totaled US$570 for three years. The estimated annual costs of the three core staff at 0.2 FTE for the REDCap administrator, 0.1 FTE for the lead clinician and 0.05 FTE for the Information technology support are US$ 50000, US$ 8000 and US$ 4500 respectively. (Currency conversion at 10ZAR to 1 US$). Specific software developments (ReportMyWay and Wits2VON) were funded by the Health Sciences Research Office (approximately $7800).
4.2 User Accrual
Following installation in August 2012, the numbers of registered users increased until the end of the year to a total of 81. The cumulative uptake was approximately seven new users per month in the first year. However, following the hands-on workshop in August 2013, the user base increased by 59 in one month and brought the total number of active users to 140 by the end of August 2013 (▶Figure 1).
Fig. 1.
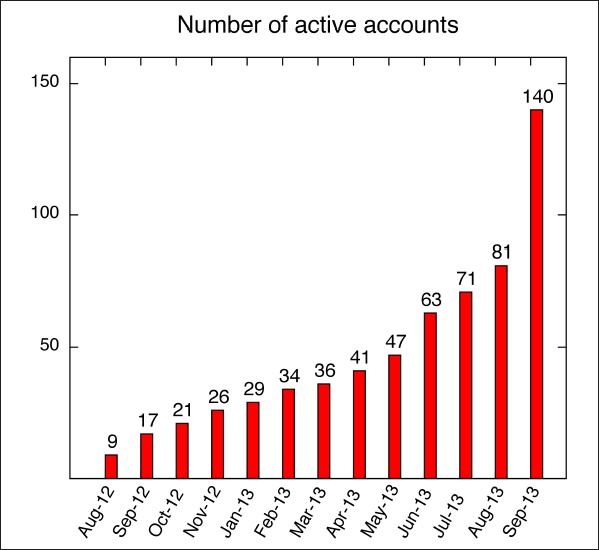
The cumulative rate of user uptake of REDCap
An increase in the number of projects created and moved to production was noted over the same time period (▶Figure 2 and ▶Figure 3). In the first year, approximately ten projects per month were created with only two per month being moved to production status. After the workshop, 45 new projects were created and 18 were moved to production.
Fig. 2.
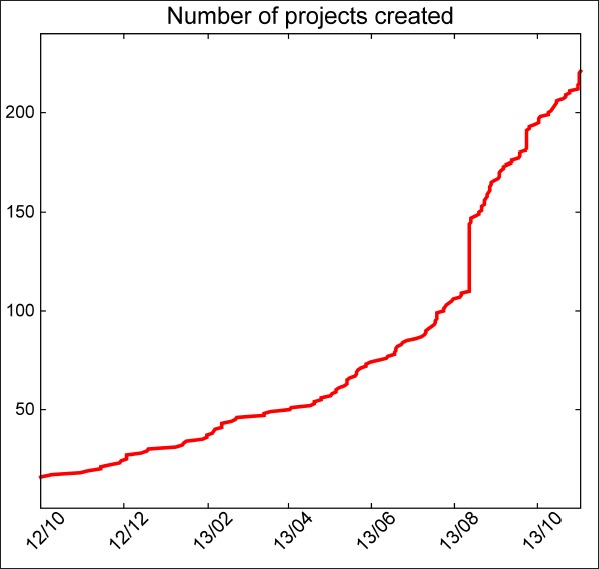
Number of projects created vs. time. The sudden increase in gradient correlates with the user workshop.
Fig. 3.
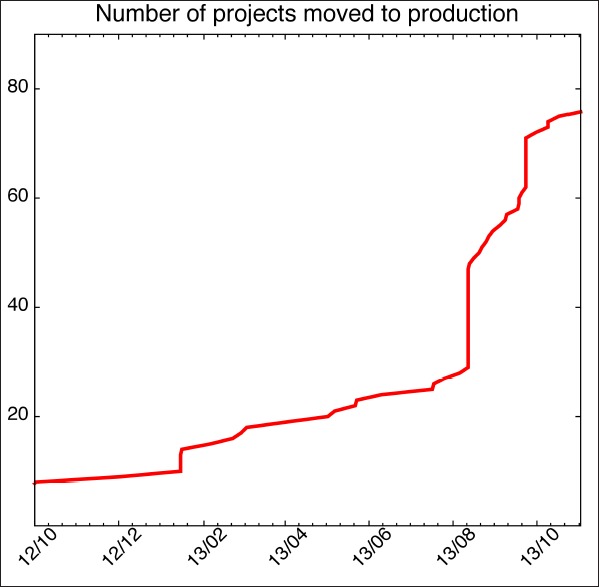
Number of projects moved to production vs. time.
As of August 2013, there were 133 projects on the Wits REDCap system. 35 projects in production and 78 projects still in development. 20 projects were archived, and no longer active. This number does not take into account projects that were deleted before the date of this report; neither does it include practice databases. The mean lifetime of the production projects by the end of November 2013 was 4.95 months (Median 3, SD 3.67). 22 Users had created production projects, the average production projects per user was 1.64 (Median 1; SD 1.46).
The projects could be broadly divided into four functional groups. The largest group was research (81), followed by quality improvement (28), and operational support (16). Eight were not classified.
A Breakdown of Project by Research Types is provided in ▶Table 1.
Table 1.
A Breakdown of Project by Research Type
| Research type | Number of Projects |
|---|---|
| Clinical trial/study | 36 |
| Repository | 26 |
| Basic/bench research | 18 |
| Epidemiological | 17 |
| Translational research | 5 |
| Behavioural or psychosocial | 3 |
| Other | 5 |
| Total | 81 |
5. Discussion
A major barrier to the use of electronic data tools in the Faculty of Health Sciences has been the lack of information technology support necessary for the installation and maintenance of such tools. In our institution three people with the necessary knowledge of servers, clinical process and user support manage the Wits REDCap project as an adjunct to their other responsibilities. This is one component of an ongoing effort to develop a robust informatics infrastructure within the faculty.
The widespread adoption of REDCap as a data capture and management instrument is attributed to its ease of use for researchers with limited Information Technology (IT) training. Extensive web-based training modalities are central to REDCap’s adoption [8]. Moreover there is no cost to an academic institution for the software and limited cost for installation, maintenance and security. Support is provided for both technical staff and users at a weekly online consortium meeting hosted by the REDCap developers at the Vanderbilt University Centre for Clinical and Translational Research in Nashville Tennessee, USA.
There is a paucity of information on the provision and use of electronic data resources for audit and research within the greater healthcare enterprise in the developing world. The global disparity in research can only be resolved if teaching and training initiatives are developed in parallel to scientific expertise [13].
Technology implementation in healthcare is an established field. The limited success of many health informatics projects reflects the complexity of health systems and can broadly be ascribed to three categories; technical shortcomings, project management shortcomings and organizational shortcomings [14].
REDCap as a database instrument can be implemented and managed by a small team.
Setting up a practical and user-friendly database instrument, which can be modified according to the needs of the clinicians and researchers, serves a valuable and extremely important role in enabling research. Researchers do not want to spend their time on finding data management solutions or solving technology problems. They would rather spend their time on research [8]. The quality of data determines the quality of information. It is crucial that clinical databases are well designed and curated if they are to perform their function to inform researchers, providers and improve clinical care [15, 16, 17].
After one year of Recap being introduced at the University of the Witwatersrand Faculty of Health Sciences there were 133 active projects of which 81 were research projects. User defined software development was created to facilitate report printing (ReportMyWay) and a data transfer interface with the Vermont Oxford Network (Wits2VON). Repeated user requests resulted in scheduling hand on user training workshops. The introduction of REDCap has created a platform of trust in information technology tools and users have a positive attitude towards future IT projects within the Faculty of Health Science.
6. Conclusion
The Faculty of Health Science at the University of the Witwatersrand has introduced REDCap as a component of an ongoing effort to create a robust informatics infrastructure. REDCap is a valuable data management instrument that we believe fulfills a need within our Institution. The installation and maintenance of software such as REDCap requires skills that few clinicians have, but are easily accessed by collaborating with by IT professionals.
The major difficulties experienced were an initial distrust and suspicion of an electronic data management system. In part this may have been due to negative previous experiences with electronic databases, doubts around data security, privacy and the legal implications surrounding electronic data. However, the ease of use, stability and rapid adoption of REDCap had a number of secondary benefits.
Consultations with the Legal and Ethics Offices of our institution created support for REDCap and an appreciation for data security and privacy. A functional implementation of REDCap was possible due to appropriate hardware, software and staff. A large number of REDCap users can be supported successfully at low cost by few staff. Collaborative meetings between software developers and clinicians enabled the creation of custom applications for data transfer between collaborating networks. Following requests for user support we created the capacity for hands-on training which increased the uptake and use of REDCap. Ensuring system stability before allowing access to end users ensured a positive first experience and was central to creating confidence amongst users of the platform. We believe REDCap, as well as fulfilling a need for data management, has created an awareness and support for functional information technology instruments that has paved the way for implementation of further informatics tools within the Faculty of Health Sciences at Wits.
Acknowledgments
The authors would like to thank the University of the Witwatersrand Strategic Planning and Resource Allocation (SPARC) fund for funding servers and software development.
Footnotes
Clinical Relevance Statement
Clinicians may not have the requisite skills to install and maintain data curatorship instruments with the security and privacy necessary for clinical use. Collaboration by computer scientists, software engineers and clinicians resulted in the effective installation and use of REDCap within our institution. User defined applications may be created by collaboration between clinicians and software engineers.
Conflict of interest
The authors declare that they have no conflicts of interest in the research
Human Subjects Protections
No human subject data was used in this paper.
References
- 1.Coovadia H, Jewkesn R, Barron P, Sanders D, McIntyre D.The health and health system of South Africa: historical roots of current public health challenges. Lancet 2009; 374(9692): 817-834. [DOI] [PubMed] [Google Scholar]
- 2.University of the Witwatersrand. Faculty of health Sciences, Faculty. http://www.wits.ac.za/academic/health/faculty/ (Last accessed 4/21/2014) [Google Scholar]
- 3.University of the Witwatersrand. Library. Database management guidelines. http://libguides.wits.ac.za/DataManagement/ (Last accessed 4/21/2014) [Google Scholar]
- 4.Paulus JK, Santoyo-Vistrain R, Havelick D, Cohen A, Kalyesubula R, Ajayi IO, Mattsson JG, Adami H, Dalal H.Global teaching and training initiatives for emerging cohort studies. Journal of Epidemiology and Global Health 2012; 2: 125–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Travis P, Bennett S, Haines A, Pang T, Bhutta Z, Hyder AA, Pielemeier NR, Mills A, Evans T.Overcoming health-systems constraints to achieve the Millennium Development Goals. Lancet 2004; 364(9437): 900-906. [DOI] [PubMed] [Google Scholar]
- 6.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG.Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42(2): 377-381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gallagher SA, Smith AB, Mathews JE, Potter CW, Woods ME, Raynor M, Wallen EM, Rathmell WK, Whang YE, Kim WY, Godley PA, Chen RC, Wang A, You C, Barocas DA, Pruthi RS, Nielson ME, Milowsky MI.Roadmap for the development of the University of North Carolina at Chapel Hill Genitourinary Oncology Database – UNC GOLD. Urologic Oncology: Seminars and Original Investigations 2014; 32(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Franklin JD, Guidrya A, Brinkleya JF.A partnership approach for electronic data capture in small-scale clinical trials. J Biomed Inform 2011; 44 (Suppl. 1): S103–S108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.REDCap. http://project-REDCap.org/ (Last accessed 4/21/2014) [Google Scholar]
- 10.Habib I.Virtualization with KVM. Linux Journal 2008; 166: 8. [Google Scholar]
- 11.Powers S.LVM Demystified. Linux Journal 2013; 236: 7. [Google Scholar]
- 12.http://www.vtoxford.org/enicq/enicq5/documents/eNICQ5ExternalDataInterfaceGuide.pdf). (Last accessed 4/21/2014)
- 13.Paulus JK, Santoyo-Vistrain R, Havelick D, Cohen A, Kalyesubula R, Ajayi IO, Mattsson JG, Adami H, Dalal H.Global teaching and training initiatives for emerging cohort studies. Journal of Epidemiology and Global Health 2102; 2: 125–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lorenzi NM, Riley RT.Managing Technological Change: Organizational Aspects of Health Informatics. 2nd Ed. New York: Springer Verlag; 2004. [Google Scholar]
- 15.Lyratzopoulos G, Patrick H, Campbell B.Registers needed for new interventional procedures. Lancet 2008; 371(9626):1734–1736. [DOI] [PubMed] [Google Scholar]
- 16.Dreyer NA., Garner S.Registries for robust evidence. JAMA 2009; 302(7):790–791. [DOI] [PubMed] [Google Scholar]
- 17.Jacobs JP, Edwards FH, Shahian DM, Haan CK, Puskas JD, Morales LS, Gammie JS, Sanches JA, Brennan MJ, O’Brien SM, Dokholyan SD, Hammill BG, Curtis LH, Peterson ED, Badhwar V, George KM, Mayer JE, Chitwood WR, Murray GF, Grover FL.Successful linking of the Society of Thoracic Surgeons adult cardiac surgery database to Centers for Medicare and Medicaid Services Medicare data. Ann Thoracic Surg 2010; 90(1):1150–1156. [DOI] [PubMed] [Google Scholar]