

Abstract
Female juvenile offenders report high rates of sexual coercion and substance use, yet the temporal relationship between the two remains unclear. The focus of this study was to conduct a prospective examination of predictors of sexual coercion and substance use for a group of high-risk young women. Two hundred and forty five adolescent females (34% of a sample including males and females), between the ages of 14-17, and from a larger study of juvenile offenders, were recruited from juvenile probation offices to participate in a longitudinal study on substance use and sexual risk. At baseline, participants completed measures associated with increased risk for sexual coercion, including substance use, perceived relationship control, and externalizing behavior. At 6- and 24-month follow-up, participants also completed a measure assessing sexually coercive experiences. Path analysis revealed that less relationship control at baseline predicted sexual coercion at 6-months. Additionally, 6-month sexual coercion predicted alcohol use and sexual coercion at 24-month follow-up. Logistic regression analysis revealed also that alcohol use at 6-months predicted sexual revictimization at 24-months. Sexual coercion appears to be associated with subsequent increases in alcohol use, suggesting that female juvenile offenders may be using alcohol to cope with the psychological and emotional consequences of victimization. Alcohol use is linked to increased risk for repeat sexual coercion, suggesting that exposure to risky environments also may be important in understanding these girls' risk. Difficulties responding assertively in sexual relationships (i.e., low relationship control) also seem to increase female juvenile offenders' risk for sexual coercion. Finally, previous sexual coercion appears to increase risk for future victimization, highlighting the importance of early intervention for this at-risk group.
Keywords: sexual coercion, juvenile offender, alcohol use, revictimization, assertiveness
Introduction
Initiating and maintaining romantic relationships is an important developmental milestone of adolescence. Dating violence, in the form of physical, emotional, or sexual victimization, is a significant risk to adolescents in managing these relationships successfully. Unfortunately, dating violence among adolescents is a common and serious social problem (Wolitzy-Taylor, Ruggiero, Danielson, Resnick, Hanson et al., 2008). An alarming number of adolescents report physical or sexual interpersonal violence, with estimates ranging from 15 to 46% (Halpern, Springs, Martin, & Kupper, 2009; Young & Furman, 2009). Notably, dating violence is linked to a variety of negative psychological and emotional sequelae, including posttraumatic stress disorder, substance use, depression, eating disorders, violence-related behaviors, risky sexual practices, and suicidal behavior (Holms & Sher, 2013; Wolitzky-Taylor et al., 2008). Thus, dating violence has important public health consequences, both for adolescents and for society as a whole.
Because adolescents between the ages of 12-17 account for 33% of sexual assault victims (Snyder, 2000) and report twice the rate of sexual assault than that of adults (Synder & Sickmund, 1999), sexual aggression among adolescents has become the focus of numerous empirical investigations. While adolescent boys experience more physical violence at the hands of peers, adolescent girls are at greater risk of experiencing sexual aggression (Esbensen & Carson, 2009; Finkelhor, Turner, Omrod, & Hamby, 2009), including incidents of sexual assault, flashing, and sexual harassment. National surveys have demonstrated that nearly half of women reporting rape indicated that they were raped in adolescence, with approximately 33% of these rapes occurring when women were between the ages of 12-17 (Bureau of Justice Statistics, 2000). Other studies also have reported sexual victimization rates of nearly 50% among adolescent girls (Young, Grey, & Boyd, 2009) and, alarmingly, a rate of repeat sexual coercion that exceeds 60% (Young & Furman 2009), suggesting that once victimized, adolescent girls are at increased risk for being revictimized.
While research examining sexual victimization among adolescents has grown considerably in recent years, less work has focused on adolescent girls who might be considered to be especially vulnerable or at-risk. One such population is female juvenile offenders. Research has shown that the number of adolescent females entering the juvenile justice system has risen sharply over the years (Snyder, 2003). Twenty percent of juvenile arrests in 1980 were females; by 2003, nearly 30% of juvenile offenses were committed by girls (Snyder & Sickmund, 2006). Highlighting the seriousness of this problem, research with adult offenders indicates that women are the fastest growing incarcerated group in the United States (Guerino, Harrison, & Sabol, 2011). Given evidence that female juvenile offenders are likely to reoffend in adulthood and migrate into the adult criminal justice system (e.g., Colman, Kim, Mitchell-Herzfeld, & Shady, 2009), understanding the characteristics and life experiences of these young girls is of great importance, as such information could inform the development of interventions aimed at reducing problematic behaviors and changing the trajectory of these young girls' lives.
Because the juvenile justice system was designed with boys' needs in mind, there currently is a paucity of effective prevention, diversion, and treatment approaches for girls. This is especially relevant, as extant research shows that adolescent boys and girls enter this system through disparate pathways (Zahn, 2007). For instance, boys are more likely to commit serious offenses (e.g., assault, arson, murder), while girls are more likely to be convicted of status offenses (e.g., truancy, running away from home, underage drinking) (Boesky, 2002). To better understand these gender-specific pathways, a burgeoning body of work has begun to examine the potential underlying reasons for girls' involvement with the juvenile justice system. Cross-sectional studies have shown, for example, that girls in this system often are victims of physical, psychological, and sexual abuse (Dembo, Schmeidler, & Childs, 2007), and also experience serious mental health disorders and substance use problems (Teplin, Abram, McClelland, Dulcan, & Mericle, 2002). Importantly, longitudinal research with adolescents both within the general population (Jackson, Hanson, Amstadter, Saunders, & Kilpatrick, 2013) and juvenile justice system (Dembo, Williams, Wothke, Schmeidler, & Brown, 1992) has demonstrated a temporal relationship between violent victimization, including sexual assault, and subsequent delinquent behavior and substance use.
Despite these findings, more work is needed to explore the temporal order of the relationship between sexual victimization and substance use among female juvenile offenders. In the broader adolescent literature, two theoretical frameworks have been used to explain the link between these constructs – coping theory, which, when applied to these behaviors, posits that adolescents engage in high risk behavior to manage the negative affect that is a consequence of victimization experiences (Lazarus, 1993), and is analogous to the self-medication hypothesis (Khantzian & Albanese, 2008); and lifestyle/routine activities theory, which posits that victimization is the result of exposure to environmental contexts through participation in delinquent activities (e.g., substance use) that increase risk due to a paucity of societal protections and increased contact with possible perpetrators (Lauritsen, Laub, &Sampson, 1992). Notably, recent prospective work with adolescent girls found that a history of sexual abuse predicted involvement in high risk behavior (i.e., substance use and delinquent behavior) at follow-up (Begle et al., 2011). This work found also that high risk behavior at baseline did not predict sexual abuse at follow-up, supporting coping theory as an explanation for the temporal association between sexual victimization and high risk behavior in adolescent girls (Begle et al., 2011). Interestingly, related work with adolescents also has found that alcohol use was associated with victimization prospectively, with those reporting more frequent alcohol use also being more likely to report sexual assault (Buzy, McDonald, Jouriles, Swank, Rosenfield, et al., 2004).
Overall, then, there is some empirical support for the theory that victimization experiences among adolescent girls may result in delinquent behavior, including substance use. There is also evidence that substance use, specifically alcohol use, increases risk for victimization. Further work is needed, however, to assess the extent to which these findings generalize to other populations, as well as to examine whether victimization reoccurs over time. Exploring the timing of life events and their longitudinal nature is relevant in understanding adolescent health (Elder & Shanahan, 2006), and can illuminate possible explanations for the mechanisms underlying victimization (Shanahan, Erickson, & Bauer, 2005). Importantly, such work also has direct implications for the development of interventions aimed at reducing risk for victimization among youth in general, and in particular, for at-risk, adolescent girls, such as female juvenile offenders.
Current Study
The focus of the current study, then, was to conduct a prospective examination of predictors of sexual victimization and substance use among female juvenile offenders. The longitudinal nature of the study is important, as it allowed us to examine the temporal relationship between these two constructs, and to evaluate whether victimization experiences place these adolescents at risk for substance use (supporting coping theory), or whether substance use increases their risk for victimization (supporting life style/routine activities theory). Thus, the study design allowed for a unique examination of the trajectories of these girls' experiences. In addition to substance use, we examined other putative risk factors for victimization, including perceived control in relationships and behavioral disinhibition. We included these, as opposed to other risk factors, given work with female adolescents demonstrating relationships between attention-deficit hyperactivity disorder (an externalizing disorder problem) and sexual victimization (White & Buchler, 2012), and high levels of rejection sensitivity and sexual aggression (Young & Furman, 2008). Related work with college and community samples of women supporting links between risk for sexual victimization and difficulties responding assertively to sexual situations (Livingston, Testa, & VanZile-Tamsen, 2007; Testa, VanZile-Tamsen, & Livingston, 2007), and sexual victimization and trait disinhibition (Yeater & Viken, 2010) also supported their inclusion in the present study. Thus, we included measures appropriate for use with adolescents that most closely tapped these constructs, specifically, measures of perceived relationship control and externalizing behavior.
Prior to describing our study in detail, we provide definitions for key terms. By adolescent, we mean a young person between the ages of 12 and 18, a definition supported by the Society of Adolescent Health and Medicine (SAHM). By juvenile offender, we mean an adolescent who is known to the juvenile justice system due to arrest, diversion, probation, detention, or incarceration. Finally, as there are often disparate definitions of sexual victimization in the literature, we use a measure that relies on behaviorally-specific definitions of such experiences, a strategy supported by and adhered to by experts in the field (described below) (e.g., Koss, Gidycz, & Wisniewski, 1987). Because this measure assessed a broad array of experiences, we labeled this variable sexual coercion.
Participants in this study were adolescent females involved with the juvenile justice system who volunteered to participate in a longitudinal study of substance use and sexual risk. We examined the self-reported behavior of these girls across three waves: baseline (Time 1), 6-months (Time 2), and 24-months (Time 3). Based on the extant literature, we examined whether baseline measures of substance use (i.e., alcohol and drug use), perceived control in relationships, and behavioral disinhibition (i.e., externalizing behavior) predicted sexual coercion at 6-months. We examined also whether these variables, in concert with sexual coercion at 6-months, predicted sexual coercion and substance use at 24-months. Finally, we examined which variables, when considered together, predicted the experience of different types of sexual coercion at the 6- and 24-month follow-up (sexual harassment, unwanted contact, forced sex) and repeat incidents of sexual coercion at 24-months among those who reported experiencing victimization at 6-months.
Method
Participants
Females (n = 245) from a larger study also involving male juvenile offenders were included in the following analyses (Yeater, Lenberg, & Bryan, 2012). Participants were recruited from juvenile probation offices in the Denver metropolitan area. The length of time on probation varied from newly on probation to over a year or more. From baseline to 6-month follow-up, 19.8% (n = 43) reported being in juvenile justice facility. Detainment was not assessed at the 24-month follow-up. The retention rate at 6-months was 94.9%; at 24-months it was 77.1%. Participants who dropped out of the study did not differ significantly on key variables from participants who were retained throughout the follow-ups.
Mean age of participants at baseline was 15.70 years (SD = 1.05, range 14-18). The sample was ethnically diverse, including Caucasian (13.2%), African American (23.4%), Hispanic (45.1%), American Indian/Alaska Native (3.4%), Asian/Pacific Islander (.4%), Multi-Racial (13.2%), and “Other” (1.3%). Mean grade level of participants was 9.98 (SD = 1.16, range 7-12). The largest group of participants reported living in a single family home with their mothers (48.9%); only 20.2% of participants reported living with their mother and father.
Measures
Demographic Information
These items assessed participants' ethnicity, age, year in school, and living situation.
Sexual Coercion
Participants completed a 7-item measure developed by Abbey and colleagues (Abbey & McAuslan, 2004; Abbey, Zawacki & Buck, 2005) designed to assess both the frequency and severity of adolescents' experience with sexually coercive behavior. This measure is a modified version of the Sexual Experiences Survey, which has been used extensively in past work and has good internal consistency and test-retest reliability (Koss, Gidycz, & Wisnieski, 1987). Abbey et al. (2005) reported the internal consistency of this measure to be .84.
For adolescent girls, this measure assessed how many times in the last 6 months they experienced different types of sexual coercion. As with related instruments (Koss et al., 1987), this measure uses behaviorally-specific definitions of these behaviors and presents items from the least to the most severe. Three types of sexually unwanted behavior are assessed: (a) four items assessed sexual harassment (e.g., being stared at in a sexual way even though you made it clear you did not want it), (b) one item assessed unwanted contact (i.e., being kissed, hugged, or touched by someone even though you made it clear you did not want it), and (c) two items assessed forced oral sex or sexual intercourse (i.e., being forced to have oral sex or sexual intercourse even though you made it clear you did not want it). Response options for each of the seven questions ranged from 0 = never to 3 = three or more times. In the current study, the internal consistency for the sexual harassment subscale was .71 and for the forced sex subscale, it was .66 (no alpha was computed for the unwanted contact subscale, as it had only one item). The internal consistency for all items was .73.
Participants' responses to this measure were scored in two ways. First, because of the relatively low frequency of endorsement of each item, participants' experience with each type of sexual coercion (i.e., sexual harassment, unwanted contact, and forced oral sex or sexual intercourse) was dichotomized to indicate whether they did (coded 1) or did not (coded 0) report any experience with this type of coercion. Second, participants were assigned to a category that reflected the severity of their sexually coercive experiences at both the 6- and 24-month follow-up. That is, if a participant reported that she experienced sexual harassment only, her experience was labeled as sexual harassment; however, if she indicated that she experienced both sexual harassment and forced sexual intercourse, then her experience was labeled as forced sex. This resulted in a single item coded as follows: 0=no experience of coercion, 1=sexual harassment, 2=unwanted contact, and 3=forced sex.
Sexual Relationship Power
The Sexual Relationship Power Scale (SRPS)—Relationship Control subscale (SRPS; Pulerwitz et al., 2000) examines interpersonal power within a sexual relationship. This is a 15-item questionnaire with items such as “My partner does what he wants, even if I do not want him to” with response options ranging from 1=strongly disagree to 4=strongly agree. Items were reverse coded and averaged such that higher scores indicate more control in the sexual relationship. In the current study, the internal consistency of this scale was .80.
Sexual History
Number of lifetime sexual partners and age of first sexual intercourse were used to measure sexual history.
Alcohol and Marijuana Use
A single item asking about frequency of alcohol use for each time point (baseline, 6-months, and 24-months) was used to measure general alcohol consumption. Participants were asked how often they consumed at least one alcoholic drink with response options ranging from 1 = never to 9 = every day. Similarly, a single item also was used to assess marijuana use for the same time points. Participants who reported smoking marijuana in the past six months were asked how often they smoked marijuana with response options ranging from 1= occasionally to 8 = every day.
Hard Drug Use
As used in previous work (Yeater et al., 2011), a composite measure was created for hard drug use. Any use of each drug was coded as “1” and nonuse was coded as “0,” and then answers were summed across the hard drugs assessed (crack, LSD, mushroom, ecstasy, GHB, ketamine, methamphetamine, and heroin). Scores ranged from 0 = none used to 8 = all hard drugs used. In the current study, the internal consistency of this measure was .70.
Externalizing Behavior
The Child Behavior Checklist (CBCL) Youth Self-Report was used to measure participants' externalizing behavior (Achenbach, 1999). This is a 31-item questionnaire with items such as “I steal from home.” Response options were 0=not true, 1=somewhat/sometimes true, and 2=very true/often true. Higher scores on this measure indicate higher levels of externalizing behavior. In the current study, the internal consistency of the CBCL was .88.
Procedure
The study was conducted in compliance with the university's Internal Review Board. A federal Certificate of Confidentiality was obtained from the National Institute on Drug Abuse due to the age of the participants and the sensitivity of the data.
Research assistants recruited participants from the waiting rooms of juvenile probation offices. Interested participants were evaluated to ensure that they met inclusion criteria for the study (i.e., 14-17 years old, on probation, able to speak and read English and comprehend the assent form). Their parent/guardian then was contacted by telephone, read the informed consent form, and provided audiotaped verbal consent.
Participants were compensated $20 for the baseline and $50 for the 6- and 24-month assessments. Baseline assessments included all measures except for the sexual harassment and victimization questionnaire and were conducted in a private room at the probation office. Only a research assistant was present to answer questions from participants about the self-report measures. The 6- and 24-month assessments included the previous questionnaires in addition to the sexual coercion measure. These assessments occurred in a place that was convenient for the participant (e.g., their home, a fast food restaurant, the private room at the probation office). All questionnaires were completed by participants on laptop computers using audio-computer assisted interview (ACASI) technology. ACASI encourages reporting of high risk behaviors (Wight et al., 2000), and is especially useful with juvenile offender populations, who often have problems with literacy and negotiating simple skip patterns (Schmiege, Broaddus, Levin, & Bryan, 2009), as it facilitates comprehension of the questionnaires and eliminates mistakes based on contingent questioning by initiating skip patterns for participants.
Data Analytic Strategy
All continuously scaled variables first were checked for distributional properties to ensure that none departed substantially from normality. Bivariate correlations then were examined among the variables (see Table 1). Those with significant relationships were included in a mediational model using path analysis to examine which variables accounted for unique variance in sexual coercion at the 6-month and 24-month follow-up. Logistic regression analysis (Hosmer & Lemeshow, 2000) also was used to evaluate which variables, when considered together, predicted the experience of different types of sexual coercion at the 6- and 24-month follow-up (sexual harassment, unwanted contact, forced sex) and repeat incidents of sexual coercion at 24-months. Demographic variables were not significantly correlated with any of the outcome variables (all ps > .05); thus, we did not control for these in the path analytic or logistic regression models.
Table 1. Intercorrelations Between Predictors and Sexual Coercion.
| Variables | M | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | 12. | 13. | 14. | 15. | 16. | 17. | 18. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. CBCL | 1.73 | .30 | — | |||||||||||||||||
| 2. Relationship Control | 5.83 | .61 | .19** | — | ||||||||||||||||
| 3. Drug Use (Baseline) | .79 | 1.49 | .27*** | -.15* | — | |||||||||||||||
| 4. MJ Use (Baseline) | 5.47 | 2.93 | .17 | -.01 | .26** | — | ||||||||||||||
| 5. Etoh Use (Baseline) | 3.13 | 2.23 | .41*** | -.17* | .43*** | .33*** | — | |||||||||||||
| 6. MJ Use (6 Months) | 5.02 | 2.60 | .13 | -.11 | .05 | .20 | .20* | — | ||||||||||||
| 7. Etoh Use (6 Months) | 3.17 | 2.20 | .25*** | -.07 | .32*** | .14 | .50*** | .06 | — | |||||||||||
| 8. Harassment (6 Months) | .77 | .42 | .14* | -.02 | .06 | -.14 | .13 | -.13 | .17* | — | ||||||||||
| 9. Contact (6 Months) | .40 | .49 | .08 | -.17* | .07 | -.14 | .10 | .01 | .16* | .41*** | — | |||||||||
| 10. Forced (6 Months) | .22 | .42 | .20** | -.27*** | .13 | .04 | .20** | .14 | .21** | .19** | .35*** | — | ||||||||
| 11. Coercion (6 months) | 1.46 | 1.05 | .19** | -.22** | .09 | -.12 | .19** | .07 | .25*** | .60*** | .71*** | .76*** | — | |||||||
| 12. Drug Use (24 Months) | .57 | 1.20 | .23* | -.18* | .58*** | .10 | .31*** | .03 | .34*** | .09 | .06 | .10 | .13 | — | ||||||
| 13. MJ Use (24 Months) | 5.12 | 3.02 | .07 | -.13 | .06 | .41** | .09 | .20 | -.02 | -.11 | -.05 | -.07 | -.12 | .04 | — | |||||
| 14. Etoh Use (24 Months) | 2.95 | 2.15 | .19 | -.16 | .22** | -.03 | .34*** | -.08 | .40*** | .23** | .19* | .22** | .24** | .41*** | .05 | — | ||||
| 15. Harassment (24 Months) | .60 | .49 | .33** | .-12 | .10 | .05 | .22* | .18 | .24* | .19 | .22* | .16 | .24* | .32** | -.10 | .36*** | — | |||
| 16. Contact (24 Months) | .35 | .48 | .32** | -.20 | .24* | .17 | .31** | .03 | .11 | .23* | .21* | .23* | .22* | .34** | -.06 | .24* | .55*** | — | ||
| 17. Forced (24 Months) | .20 | .40 | -.04 | -.26* | -.11 | .18 | .16 | .00 | .14 | .10 | .31** | .16 | .22* | .12 | .05 | .15 | .31** | .43*** | — | |
| 18. Coercion (24 months) | 1.21 | 1.16 | .22* | -.24* | .07 | .16 | .30** | .08 | .21* | .20 | .36*** | .24* | .33** | .31** | -.04 | .31** | .75*** | .77*** | .78*** | — |
Note. R values of .10, .30, and .50 are considered to be, respectively, small, medium, and large effect sizes [37]. Hard drug use at 6-months was not measured; thus, it is not included within. CBCL = Child Behavior Checklist; Relationship Control = Perceived control in current relationship; Drug Use = Hard drug use; MJ = Marijuana use; Etoh Use = Frequency of alcohol use; Harassment = sexual harassment; Contact = unwanted sexual contact; Forced = forced oral sex or sexual intercourse; Coercion = Sexual coercion; Sexual harassment, unwanted contact, and forced oral sex or sexual intercourse coded as 0 = experienced the behavior or 1 = did not experience the behavior. Sexual coercion coded as 0 = no sexual coercion, 1 = sexual harassment, 2 = unwanted sexual contact, 3 = forced oral sex or sexual intercourse.
p < .05.
p < .01.
p < .001.
Results
Sexual Behavior and Sexual Coercion Experiences
Approximately 84% of participants reported ever having had sexual intercourse, with a mean age at first intercourse of 13.59 years (SD = 1.36; range 9-18). Participants had an average of 5.68 (SD = 6.91, range 1-45) lifetime sexual partners. Approximately 67% (n = 144) of participants reported being sexually attracted to people of the opposite sex, while 6% (n = 13) reported being sexually attracted to people of the same sex, and 27.6% (n = 60) reported being sexually attracted to people of both sexes.
The majority of participants reported having experienced some sexual coercion in the past 6 months as assessed by the 6-month follow-up. Specifically, 76.7% (n = 171) had experienced sexual harassment, 40.03% (n = 89) had experienced unwanted contact, and 22.0% (n = 49) had experienced forced oral sex or sexual intercourse. At the 24-month follow-up, the majority of participants again had experienced sexual coercion at least once in the past 6 months. Specifically, 60.2% (n = 59) had experienced sexual harassment, 35.1% (n = 34) had unwanted contact, and 20.2% (n = 20) had experienced forced oral sex or sexual intercourse. Regarding experiences of repeat sexual coercion at both the 6- and 24-month follow-ups (i.e., typically referred to as sexual revictimization in the literature), 66.7% of participants reported some type of repeat sexual coercion experiences (i.e., at least one incident of some type of sexually coercive experience at each time point).
Factors Associated with Sexual Coercion at the 6- and 24-Month Follow-Up
We first examined the bivariate relationships among the hypothesized risk factors at baseline and 6-months and the severity of sexual coercion at the 6- and 24-month follow-up, and then separately for the specific categories of sexual harassment, unwanted contact, and forced sex (see Table 1). Externalizing behavior and frequency of alcohol use at baseline were significantly positively correlated with severity of sexual coercion at 6-months, while perceived relationship control was negatively associated with sexual coercion severity. Sexual coercion at 6-months was in turn correlated positively with frequency of alcohol use at 24-months and severity of sexual coercion at 24-months. Similar to the 6-month follow-up, externalizing behavior, hard drug use, and frequency of alcohol use at 24-months were associated positively with more severe sexual coercion at 24-months, while perceived relationship control was negatively associated with 24-month severity of sexual coercion.
In terms of type of sexual coercion at the 6-month follow-up, externalizing behavior at baseline was positively associated with both sexual harassment and forced sex at 6-months, while frequency of alcohol use at baseline was positively associated with forced sex, but not harassment or coercion at 6-months. Perceived relationship control at baseline was associated with the experience of unwanted contact and forced sex, but not harassment at 6-months. Finally, externalizing behavior at baseline was positively associated with sexual harassment, unwanted contact, and forced sex at 24-months, while perceived relationship control at baseline was negatively associated with forced sex at 24-months.
Path Analytic Model Findings
We then estimated a mediational model via path analysis (c.f, Bryan et al, 2007) using EQS 6.1 (See Figure 1). Variables related to 6- and 24-month sexual coercion at the bivariate level were used as predictors in the mediational model. To account for the missing data at follow-up, we utilized maximum likelihood estimation of missing data (c.f., Schafer & Graham, 2002); thus, robust estimation of standard errors was used for tests of fit and significance of the paths. The fit of the model was adequate, Santorra- Bentler χ2(10, N = 245) = 13.16, p = .21, CFI=927, RMSEA=. 114 (90% CI .079-. 150). As would be expected, alcohol use at baseline predicted alcohol use at the 24-month follow-up, and along with sexual coercion at 6-months, accounted for 11.9% of the variability in alcohol use at 24-months. Hard drug use at baseline predicted hard drug use at 24-months. Additionally, hard drug use at baseline and sexual coercion at 6-months accounted for 26.1% of the variability in hard drug use at 24-months. Relationship control at baseline predicted 6-month sexual coercion, such that those who reported less relationship control at baseline also were more likely to report experiencing sexual coercion at 6-months. Baseline alcohol use, hard drug use, externalizing behavior, and relationship control accounted for 8.2% of the variance in sexual coercion at 6-months. Controlling for alcohol use, hard drug use, externalizing behavior, and relationship control at baseline, 6-month sexual coercion significantly predicted alcohol use at the 24-month follow-up and 24-month sexual coercion. Finally, sexual coercion at 6-months accounted for 11.1% of the variance in 24- month sexual coercion. None of the other variables were related to 6-month or 24-month sexual coercion.
Figure 1.
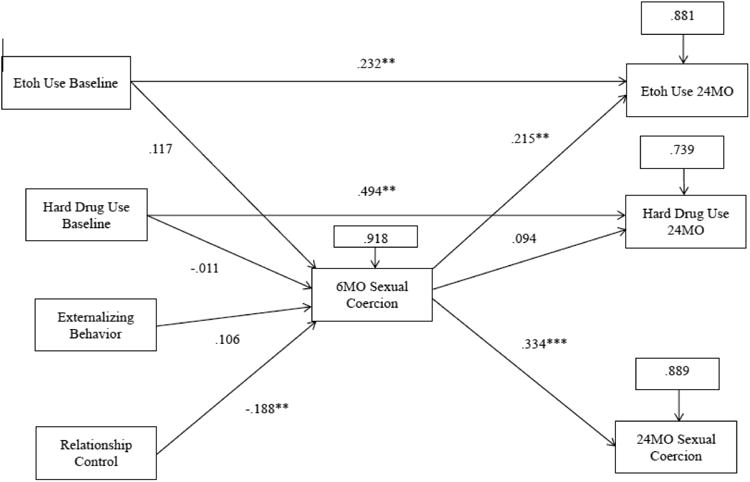
Mediational model of sexual coercion. Coefficients are standardized path coefficients.
*p< .05, two-tailed. **p<.01, two-tailed. ***p<001, two-tailed.
Note: Etoh Use = Frequency of alcohol use; Sexual coercion coded as 0 = no sexual coercion, 1 = sexual harassment, 2 = unwanted sexual contact. 3 = forced oral sex or sexual intercourse.
Factors Predicting Different Types of Sexual Coercion at the 6- and 24-Month Follow-Up
We also used logistic regression analysis (Hosmer and Lemeshow, 2000) to evaluate which variables predicted different types of sexual coercion (sexual harassment, unwanted contact, forced sex) at the 6- and 24-month follow-up. Only those analyses resulting in significant findings will be presented here (see Table 2 for the entire set of analyses).
Table 2. Summary of the Logistic Regression Analyses Predicting Different Types of Sexual Coercion at the 6- and 24-Month Follow-ups.
| β | SE | Wald's χ2 | df | p-value | Odd Ratio | Omnibus χ 2 | |
|---|---|---|---|---|---|---|---|
| Sexual Harassment 6 Months | 5.80, ns | ||||||
| Externalizing Behavior | .93 | .65 | 2.06 | 1 | .15 | 2.54 | |
| Perceived Relationship Control | -.13 | .29 | .21 | 1 | .65 | .88 | |
| Baseline Hard Drug Use | -.05 | .13 | .11 | 1 | .74 | .96 | |
| Baseline Alcohol Use | .10 | .10 | 1.19 | 1 | .28 | 1.11 | |
|
| |||||||
| Unwanted Contact 6 Months | 8.97, ns | ||||||
| Externalizing Behavior | .09 | .55 | .03 | 1 | .87 | 1.09 | |
| Perceived Relationship Control | -.66 | .26 | 6.44 | 1 | .01 | .52 | |
| Baseline Hard Drug Use | -.01 | .11 | .01 | 1 | .92 | .99 | |
| Baseline Alcohol Use | .07 | .08 | .73 | 1 | .39 | 1.07 | |
|
| |||||||
| Forced Sex 6 Months | 24.08*** | ||||||
| Externalizing Behavior | 1.23 | .67 | 3.36 | 1 | .07 | 3.41 | |
| Perceived Relationship Control | -1.09 | .33 | 10.97 | 1 | .001 | .34 | |
| Baseline Hard Drug Use | .02 | .12 | .02 | 1 | .89 | 1.02 | |
| Baseline Alcohol Use | .11 | .09 | 1.63 | 1 | .20 | 1.12 | |
|
| |||||||
| Sexual Harassment 24 Months | 11.32* | ||||||
| Externalizing Behavior | 1.80 | .95 | 3.63 | 1 | .06 | 6.06 | |
| Perceived Relationship Control | -.36 | .43 | .68 | 1 | .41 | .70 | |
| Baseline Hard Drug Use | -.09 | .17 | .28 | 1 | .60 | .92 | |
| 6 Month Alcohol Use | .26 | .13 | 4.32 | 1 | .04 | 1.30 | |
|
| |||||||
| Unwanted Contact 24 Months | 9.79* | ||||||
| Externalizing Behavior | 2.04 | 1.00 | 4.15 | 1 | .04 | 7.70 | |
| Perceived Relationship Control | -.40 | .45 | .78 | 1 | .38 | .67 | |
| Baseline Hard Drug Use | .13 | .17 | .59 | 1 | .44 | 1.14 | |
| 6 Month Alcohol Use | .09 | .12 | .56 | 1 | .45 | 1.09 | |
|
| |||||||
| Forced Sex 24 Months | 8.91, ns | ||||||
| Externalizing Behavior | -.50 | 1.27 | .15 | 1 | .70 | .61 | |
| Perceived Relationship Control | -1.32 | .56 | 5.50 | 1 | .02 | .27 | |
| Baseline Hard Drug Use | -.49 | .30 | 2.72 | 1 | .10 | .61 | |
| 6 Month Alcohol Use | .23 | .144 | 2.57 | 1 | .11 | 1.26 | |
p < .05.
p < .001.
The logistic regression analysis including forced sex at 6-months as the outcome variable and externalizing behavior, perceived relationship control, baseline alcohol use, and baseline hard drug use as predictors revealed that the model distinguished reliably between those who experienced forced sex at the 6 month follow-up and those who did not, χ2(4) = 24.08, p < .001, Nagelkerke R2 =.17. Externalizing behavior and baseline alcohol and hard drug use were not significant unique predictors of forced sex. However, for every unit of increase in perceived relationship control, participants were roughly 3 times less likely to experience forced sex at the 6 month follow-up, Exp (β) = 2.96.
The logistic regression analysis including sexual harassment at 24-months as the outcome variable and externalizing behavior, perceived relationship control, baseline hard drug use, and 6-month alcohol use as predictors revealed that the model distinguished reliably between those who experienced sexual harassment at 24-month follow-up and those who did not, χ2(4) = 11.32, p < .05, Nagelkerke R2 =. 18. Externalizing behavior, perceived relationship control, and baseline hard drug use were again not significant unique predictors of sexual harassment. However, with every unit of increase in alcohol use at 6-months, participants were 1.3 times more likely to experience sexual harassment at the 24 month follow-up, Exp (β) = 1.30.
Finally, the logistic regression analysis including unwanted contact at 24-months as the outcome variable and externalizing behavior, perceived relationship control, baseline hard drug use, and 6-month alcohol use as predictors revealed that the model distinguished reliably between those who experienced unwanted contact at the 24-month follow-up and those who did not, χ2(4) = 9.79, p < .05, Nagelkerke R2 =.16. Perceived relationship control, baseline hard drug use, and 6-month alcohol use were not significant unique predictors of unwanted contact at the 24 month follow-up. However, with every unit of increase in externalizing behavior, participants were 7 times more likely to experience unwanted contact at the 24 month follow-up, Exp (β) = 7.70.
Factors Predicting Sexual Revictimization at the 24-Month Follow-Up
A logistic regression analysis including sexual coercion revictimization (i.e. those who experienced sexual coercion at both 6 and 24-months) at 24-months as the outcome variable and externalizing behavior, perceived relationship control, baseline hard drug use, and 6-month alcohol use as predictors revealed that the model distinguished reliably between those who experienced revictimization at the 24 month follow-up and those who did not, χ2(4) = 10.43, p < .05, Nagelkerke R2 =. 16. Externalizing behavior, perceived relationship control, and baseline hard drug use were not significant unique predictors of revictimization at the 24 month follow-up. However, with every unit of increase in 6-month alcohol use, participants who had been victimized at 6 months were 1.27 times more likely to experience revictimization at the 24 month follow-up, Exp (β) = 1.27 (see Table 3 for a complete set of results).
Table 3. Summary of the Logistic Regression Analyses Predicting Sexual Revictimization at the 24-Month Follow-up.
| β | SE | Wald's χ2 | df | p-value | Odd Ratio | Omnibus χ2 | |
|---|---|---|---|---|---|---|---|
| Revictimization 24 Months | 10.43* | ||||||
| Externalizing Behavior | 1.47 | .91 | 2.63 | 1 | .11 | 4.32 | |
| Perceived Relationship Control | -.43 | .42 | 1.02 | 1 | .31 | .65 | |
| Baseline Hard Drug Use | -.02 | .17 | .02 | 1 | .90 | .98 | |
| 6 Month Alcohol Use | .24 | .12 | 4.15 | 1 | .04 | 1.27 |
p < .05.
Discussion
Adolescent girls are at particular risk for sexual coercion, an event that is linked to numerous negative psychological, emotional, and behavioral outcomes, including increased risk for sexual revictimization (Young & Furman, 2009; Young et al., 2009). Although substantial progress has been made in this research area, fewer studies have focused on adolescent girls who might be at particular risk for sexual victimization, such as female juvenile offenders. Thus, we focused on female juvenile offenders, a highly vulnerable group of young women about whom more research is needed, both to pinpoint the potential underlying reasons for their involvement in the juvenile justice system and to identify their unique mental health, preventative, and intervention needs.
Prospective studies with adolescents both within the general community and the juvenile justice system have found a relationship between sexual assault and consequent delinquent behavior and substance use (Dembo et al., 1992; Jackson et al., 2013). Of particular importance has been unpacking the relationship between sexual victimization and substance use – that is, whether substance use, with its concomitant exposure to high-risk environments, results in increased risk for victimization, or whether victimization leads to substance use as a means to cope with the adverse consequences of the victimization experience. Thus, two theoretical frameworks, lifestyle/routine activities theory and coping theory, have been used to explain the temporal relationship between the two, with research to date providing support for both explanations (Begle et al., 2011; Buzy et al., 2004).
In our study, we recruited adolescent females from juvenile probation offices to participate in a longitudinal study on substance use and sexual risk. At baseline, participants completed measures associated with increased risk for sexual coercion, including substance use, perceived relationship control, and externalizing behavior. At 6- and 24-month follow-up, participants also completed a measure assessing sexually coercive experiences. Thus, our study allowed for a prospective examination of predictors of sexual coercion over time. Using related work as a guide, we explored whether substance use, perceived control in relationships, and behavioral disinhibition predicted sexual coercion among female juvenile offenders at 6- and 24-months. Notably, we were able to examine the temporal relationship between sexual coercion and substance use, allowing us to determine whether sexual coercion places these young women at risk for substance use (supporting coping theory), or whether substance use increases their risk for experiencing sexual coercion (supporting lifestyle/routine activities theory).
The results of our path analytic model revealed several notable findings. First, controlling for multiple other correlates, sexual coercion at 6-months predicted alcohol use at 24-month follow-up. As was found by Begle et al. (2011), previous sexual coercion appears to be linked to subsequent alcohol use, suggesting that these young girls may be coping with the negative psychological sequelae of coercion by using alcohol. This finding offers tentative support then for coping theory as a way of explaining the association between sexual coercion and substance use in this population.
Second, sexual coercion at 6-months predicted sexual coercion at 24-months. Related work both with adolescents (Begle et al., 2011) and college women (Gidycz, Rich, Orchowski, King, & Miller, 2006) has reported similar findings, highlighting the invariance of this construct. This finding also suggests that sexual coercion is non-random among these vulnerable young women and emphasizes the need for early intervention to reduce their risk of revictimization. Of course, there are likely other individual difference variables that increase these girls' risk, and future work should endeavor to explore these as well. Similarly, alcohol and hard drug use at baseline predicted alcohol and hard drug use at 24-months, suggesting that use of these substances among female juvenile offenders is relatively stable over time. Given the elevated rates of substance use in this population, and the robust relationship between alcohol use and sexual assault, interventions should probably focus also on ways to reduce these young girls' alcohol use.
It is important to note that rates of sexual coercion among these young girls were not negligible. In fact, incident rates for both 6- and the 24-month follow-ups were high, and, notably, approximately 67% reported repeat incidents of sexual coercion during the course of the study. Interestingly, the results of our logistic regression analysis regarding repeat sexual coercion revealed that alcohol use alone uniquely predicted these experiences over and above other risk factors. This finding suggests that exposure to high risk environments (as conceptualized by life style/routine activities theory) increases risk for revictimization. Future work with female juvenile offenders should investigate further what it is about the experience of sexual coercion that precipitates additional coercive experiences. Clearly, substance use appears relevant, but the substantial mental health needs of these young girls point to another avenue to explore –specifically, symptoms of depression, anxiety, and posttraumatic stress could interfere with their ability to both identify and respond effectively to high risk situations. Indeed, related work with college women has found a link longitudinally between psychopathology and sexual victimization (e.g., Messman-Moore et al., 2008).
Third, less perceived relationship control at baseline predicted sexual coercion at 6-months. This finding dovetails nicely with related work with adolescents demonstrating a relationship between rejection sensitivity and sexual aggression (Young & Furman, 2008), and research with both college (Yeater & Viken, 2010) and community samples (Testa, et al., 2007) of women showing that difficulty responding assertively to risky situations is linked to increased risk for sexual victimization. This finding suggests that female juvenile offenders might benefit from interventions that focus on teaching skills for responding to situations that have a high risk for sexual victimization. Interventions to decrease high risk sexual behavior with this group (e.g., having sex without a condom) have proved effective (e.g., Schmiege, Hendershot, Feldstein-Ewing, & Bryan, 2011). Thus, it might be possible to incorporate into existing interventions a component that teaches skills for decreasing risk for sexual coercion. Such interventions might involve having participants identify situations that are relevant to them and which presumably are high risk, followed by a discussion and rehearsal of possible responses to such situations. Similar interventions with college women with a history of sexual revictimization have been shown to be somewhat effective in decreasing revictimization rates (Marx, Calhoun, Wilson, & Meyerson, 2001). It also might be possible to involve juvenile justice staff, such as probation officers, or peer mentors in these interventions, who then could provide additional opportunities to rehearse these skills, thereby increasing these girls' sense of self-efficacy about executing them in real life situations.
With respect to explaining different types of sexual coercion, the results of our logistic regression analyses revealed variability in the predictors of these events. Specifically, greater perceived relationship control was related to decreased likelihood of experiencing forced sex at 6-months, greater alcohol use was related to increased likelihood of experiencing sexual harassment at 6-months, and greater externalizing behavior was related to increased likelihood of experiencing unwanted contact at 24 months. Overall then, lack of control in relationships, alcohol use, and difficulties with behavioral disinhibition all appear relevant in understanding female juvenile offenders' risk for different types of sexual coercion. Future work should continue to examine what factors predict the severity of sexual coercion, as such information may have important preventive intervention implications.
While our study has several strengths, it also has limitations. First, although we found statistically significant associations between some of our predictor variables and sexual coercion, the effect sizes for these findings were small-to-moderate in size. Thus, further research is needed to identify additional and/or more powerful predictors of sexual coercion among female juvenile offenders. Second, we did not measure child sexual abuse or adolescent sexual coercion at baseline. As a consequence, we were unable to examine whether earlier victimization experiences preceded some of the baseline behaviors. Given the high rates of child maltreatment in this population (including child sexual abuse), future research should endeavor to assess these experiences at multiple time points, as such information would allow us to better understand the trajectory of the sexual coercion-high risk behavior relationship over time. Third, we assessed only one type of victimization in our study. Recent research suggests that over 65% of adolescents experience polyvictimization, or multiple forms of victimization, either at the hands of peers and/or family members (Turner, Finkelhor, & Ormrod, 2010). Thus, future work with this population might assess polyvictimization in order to examine whether particular outcomes are linked to specific abuse experiences. Finally, our results may not be applicable to female adolescents who engage in high risk behaviors but who are not part of the juvenile justice system.
Conclusion
Victimization among adolescents has become increasingly common and has clear negative consequences for adolescent development (Finkelhor, Ormrod, & Turner, 2007). Female juvenile offenders are a high risk, vulnerable, and understudied population who report particularly high rates of sexual victimization and substance use, as well as other mental health issues. Given the increasing number of girls becoming involved in the juvenile justice system, more work is needed in this area to meet the needs of this population. In this study, we found that incidents of sexual coercion predicted alcohol use at follow-up, suggesting that these girls may be using alcohol to cope with the negative effects of victimization. We also found that alcohol use predicted repeat incidents of sexual coercion, suggesting a vicious cycle whereby girls who are victimized subsequently increase their exposure to high risk environments as compared to those who do not have a previous history of victimization. Clearly, interventions are needed for these young girls to help them both avoid and cope effectively with the consequences of victimization. It is our hope that additional research with female juvenile offenders will help inform the development of interventions to reduce the causes and consequences of sexual coercion for this group of at-risk, young women.
Acknowledgments
This research was supported by a grant from the National Institute on Drug Abuse (R01DA019139) to the last author. The authors wish to thank the probation offices (Denver Metro and Adams County), the young people who participated in our study, and the Colorado Department of Youth Corrections (DYC) for their cooperation and support. Additionally, we wish to thank Dr. Sarah Schmiege who was a postdoc on the project, and our research assistants, Katy Seals, Renea Nilsson, Miranda Dettmann, Kerry Trachsel, Teni Davoudian, Angela Hendricks, Roger Pressman, Jake Lee, Nettie Smith, Sarah Taylor, and Ben Veralrud.
Biographies
Elizabeth A. Yeater, Ph.D. Department of Psychology, University of New Mexico
Dr. Yeater is an Associate Professor in the Department of Psychology at the University of New Mexico. She received her doctorate in clinical psychology from the University of Nevada, Reno. Dr. Yeater's research program attempts to understand the processes involved in the sexual victimization and revictimization of women by using a social information processing model (SIP) as a general framework and methods borrowed from cognitive science.
Erika A. Montanaro, M.S. Department of Psychology and Neuroscience, University of Colorado Boulder
Ms. Montanaro is a graduate student in the Department of Psychology and Neuroscience at the University of Colorado, Boulder. Her research interests involve preventative interventions for reducing high risk sexual behavior among adolescents.
Angela D. Bryan, Ph.D. Department of Psychology and Neuroscience, University of Colorado Boulder
Dr. Bryan is a Full Professor in the Department of Psychology and Neuroscience at the University of Colorado, Boulder. She received her doctorate in social psychology from Arizona State University. Dr. Bryan's research program focuses on biopsychosocial models of health behavior to design, implement, and evaluate theory-based behavior change interventions to improve preventative health behavior.
Footnotes
Ethical Standards: This study has been approved by the appropriate ethics committee and has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants in the study gave their informed consent prior to their inclusion in the study.
The authors declare they have no conflict of interest.
Author Contributions: With respect to specific author contributions, EY wrote all sections of the paper except for the results section, suggested the statistical analyses to be used in the study, and provided the conceptual and theoretical background for the paper. AB conceived of and designed the study, obtained grant funding from NIDA for the project (R01DA019130), and assisted with the analyses and editing of the manuscript. EM performed the analyses and wrote the results section. All authors have read and approved the final manuscript.
Contributor Information
Elizabeth A. Yeater, Department of Psychology, University of New Mexico
Erika A. Montanaro, Department of Psychology and Neuroscience, University of Colorado Boulder
Angela D. Bryan, Department of Psychology and Neuroscience, University of Colorado Boulder
References
- Abbey A, McAuslan PA. Longitudinal examination of male college students' perpetration of sexual assault. Journal of Consulting and Clinical Psychology. 2004;72:747–756. doi: 10.1037/0022-006X.72.5.747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abbey A, Zawacki T, Buck PO. The effects of past sexual assault perpetration and alcohol consumption on men's reactions to women's mixed signals. Journal of Social and Clinical Psychology. 2005;24:129–155. doi: 10.1521/jscp.24.2.129.62273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Achenbach TM. The Child Behavior Checklist and related instruments. In: Maruish ME, editor. The use of psychological testing and treatment planning and outcomes assessment. 2nd. Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 1999. pp. 429–466. [Google Scholar]
- Begle AM, Hanson RF, Danielson CK, McCart MR, Ruggiero KJ, et al. Longitudinal pathways of victimization, substance use, and delinquency: Findings from the National Survey on Adolescents. Addictive Behaviors. 2011;36:682–689. doi: 10.1016/j.addbeh.2010.12.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boesky LM. Juvenile offenders with mental health disorders: Who are they and what do we do with them? Lanham, MD: American Correctional Association; 2002. [Google Scholar]
- Bryan A, Schmiege SJ, Broaddus MR. Mediational analysis in HIV/AIDS research: estimating multivariate path analytic models in a structural equation modeling framework. AIDS and Behavior. 2007;11(3):365–383. doi: 10.1007/s10461-006-9150-2. [DOI] [PubMed] [Google Scholar]
- Buzy WM, McDonald R, Jouriles EN, Swank PR, Rosenfield D, et al. Adolescent girls' alcohol use as a risk factor for relationship violence. Journal of Research on Adolescents. 2004;14:449–470. [Google Scholar]
- Bureau of Justice Statistics. Sexual assault of young children as reported to law enforcement: Victim, incident, and offender characteristics. Rockville, MD: U.S. Department of Justice; 2000. Rep No NCJ - 182990. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Colman RA, Kim DH, Mitchell-Herezfeld S, Shady TA. Delinquent girls grown up: Young adult offending patterns and their relation to early legal, individual, and family risk. Journal of Youth and Adolescence. 2009;38:355–366. doi: 10.1007/s10964-008-9341-4. [DOI] [PubMed] [Google Scholar]
- Danielson CK, de Arellano MA, Ehrenreich JT, Suarez LM, Bennett SM, et al. Identification of high-risk behaviors among victimized adolescents and implications for empirically-supported psychosocial treatment. Journal of Psychiatric Practice. 2006;12:364–383. doi: 10.1097/00131746-200611000-00004. [DOI] [PubMed] [Google Scholar]
- Dembo R, Schmeidler J, Childs K. Correlates of male and female juvenile offender abuse experiences. Journal of Child Sexual Abuse. 2007;16:75–94. doi: 10.1300/J070v16n03_05. [DOI] [PubMed] [Google Scholar]
- Elder J, Shanahan M. The life course and human development. In: Damon W, Lemer R, editors. Handbook of Child Psychology, Vol 1: Theoretical models of human development. 6th. New York: Wiley and Stone; 2006. pp. 665–175. [Google Scholar]
- Esbensen FA, Carson DC. Consequences of being bullied: Results from a longitudinal assessment of bullying victimization in a multisite sample of American students. Youth & Society. 2009;41(2):209–233. [Google Scholar]
- Finkelhor D, Ormrod RK, Turner HA. Polyvictimization and trauma in a national longitudinal cohort. Development and Psychopathology. 2007;19:149–166. doi: 10.1017/S0954579407070083. [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Turner HA, Ormrod R, Hamby SL. Violence, abuse, and crime exposure in a national sample of children and youth. Pediatrics. 2009;124(5):1–13. doi: 10.1542/peds.2009-0467. [DOI] [PubMed] [Google Scholar]
- Guerino P, Harrison PM, Sabol WJ. Prisoners in 2010. 2010 Retrived from Bureau of Justice Statistics website: http://bjs.ojp.usdoj.gov/content/pub/pdf/p10.pdf.
- Halpern CT, Spriggs AL, Martin SL, Kupper LL. Patterns of intimate partner violence victimization from adolescence to young adulthood in a nationally representative sample. Journal of Adolescent Health. 2009;45:508–516. doi: 10.1016/j.jadohealth.2009.03.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holms K, Sher L. Dating violence and suicidal behavior in adolescents. International Journal of Adolescent Medicine and Health. 2013;25(3):257–261. doi: 10.1515/ijamh-2013-0059. [DOI] [PubMed] [Google Scholar]
- Hosmer DW, Lemeshow L. Applied logistic regression. 2nd. New York: Wiley; 2000. [Google Scholar]
- Jackson CL, Hanson RF, Amstadter AB, Saunders BE, Kilpatrick DG. The longitudinal relation between peer violent victimization and delinquency: Results from a national representative sample of U. S. adolescents. Journal of Interpersonal Violence. 2013;28:1596–1616. doi: 10.1177/0886260512468328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khantzian EJ, Albanese MJ. Understanding addiction as self-medication: Finding hope behind the pain. Lanham, MD: Rowman & Littlefield; 2008. [Google Scholar]
- Lauritsen JL, Laub JH, Sampson RJ. Conventional and delinquent activities: Implications for the prevention of violent victimization among adolescents. Violence & Victims. 1992;7:91–108. [PubMed] [Google Scholar]
- Lazarus RS. Coping theory and research: Past, present, and future. Psychosomatic Medicine. 1993;55:234–247. doi: 10.1097/00006842-199305000-00002. [DOI] [PubMed] [Google Scholar]
- Livingston JA, Testa M, VanZile-Tamsen C. The reciprocal relationship between sexual victimization and sexual assertiveness. Violence Against Women. 2007;13:298–313. doi: 10.1177/1077801206297339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marx BP, Calhoun KS, Wilson AE, Meyerson LA. Sexual revictimization prevention: An outcome study. Journal of Consulting and Clinical Psychology. 2001;69:25–32. doi: 10.1037//0022-006x.69.1.25. [DOI] [PubMed] [Google Scholar]
- Messman-Moore TL, Coates AA, Gaffey KJ, Johnson CF. Sexuality, substance use, and susceptibility to victimization: Risk for rape and sexual coercion in a prospective study of college women. Journal of Interpersonal Violence. 2008;23:1730–1746. doi: 10.1177/0886260508314336. [DOI] [PubMed] [Google Scholar]
- Riley D. Time and crime: The link between teenager lifestyle and delinquency. Journal of Quantitative Criminology. 1987;3:339–354. [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7(2):147–177. [PubMed] [Google Scholar]
- Schmiege SJ, Broaddus MR, Levin M, Bryan AD. Randomized trial of group interventions to reduce HIV/STD risk and change theoretical mediators among detained adolescents. Journal of Consulting and Clinical Psychology. 2009;77:38–50. doi: 10.1037/a0014513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmiege SJ, Hendershot C, Feldstein-Ewing SW, Bryan AD. Positive outlook as a moderator of the effectiveness of an HIV/STD intervention with adolescents in detection. Health Education Research. 2011;26:432–442. doi: 10.1093/her/cyq060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shanahan M, Erickson L, Bauer D. One hundred years of knowing: The changing science of adolescence, 1904 and 2004. Journal of Research on Adolescence. 2005;15:383–394. [Google Scholar]
- Snyder HN. Juvenile arrests 2001. Washington DC: Office of Juvenile Justice and Delinquency Prevention, U. S. Department of Justice; 2003. [Google Scholar]
- Snyder HN, Sickmund M. Juvenile offenders and victims: 1999 national report. Washington DC: Office of Juvenile Justice and Delinquency Prevention, U. S. Department of Justice; 1999. [Google Scholar]
- Snyder HN, Sickmund M. Juvenile offenders and victims: 2006 national report. Washington, DC: U. S. Department of Justice, Office of Juvenile Justice and Delinquency Prevention; 2006. [Google Scholar]
- Teplin LA, Abram KM, McClelland GM, Dulcan MK, Mericle AA. Psychiatric disorders in youth in juvenile detection. Archives of General Psychiatry. 2002;59:1133–1143. doi: 10.1001/archpsyc.59.12.1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, VanZile-Tamsen C, Livingston JA. Prospective prediction of women's sexual victimization by intimate and nonintimate male perpetrators. Journal of Consulting and Clinical Psychology. 2007;75:52–60. doi: 10.1037/0022-006X.75.1.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner HA, Finkelhor D, Ormrod R. Poly-victimization in a national sample of children and youth. American Journal of Preventive Medicine. 38:323–330. doi: 10.1016/j.amepre.2009.11.012. [DOI] [PubMed] [Google Scholar]
- Wight RG, Rotheram-Borus MJ, Klosinski L, Ramos B, Calabro M, Smith R. Screening for transmission behaviors among HIV-infected adults. AIDS Education & Prevention. 2000;12:431–441. [PubMed] [Google Scholar]
- Wolitzky-Taylor KB, Ruggiero KJ, Danielson CK, Resnick HS, Hanson RF, Smith DW, et al. Prevalence and correlates of dating violence in a national sample of adolescents. Journal of American Academy of Child and Adolescent Psychiatry. 2008;47(7):755–762. doi: 10.1097/CHI.0b013e318172ef5f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeater EA, Viken RJ. Factors affecting women's response choices to dating and social situations. Journal of Interpersonal Violence. 2010;25:1411–1428. doi: 10.1177/0886260509354588. [DOI] [PubMed] [Google Scholar]
- Yeater EA, Lenberg KL, Bryan A. Predictors of sexual aggression among male juvenile offenders. Journal of Interpersonal Violence. 2012;27:1242–1258. doi: 10.1177/0886260511425243. [DOI] [PubMed] [Google Scholar]
- Young BJ, Furman W. Interpersonal factors in the risk for sexual victimization and its recurrence during adolescence. Journal of Youth Adolescence. 2008;37(3):297–309. [Google Scholar]
- Young AM, Grey M, Boyd CJ. Adolescents' experiences of sexual assault by peers: Prevalence and nature of victimization occurring within and outside of school. Journal of Youth Adolescence. 2009;38:1072–1083. doi: 10.1007/s10964-008-9363-y. [DOI] [PubMed] [Google Scholar]
- Zahn MA. The causes of girls' delinquency and their program implications. Family Court Review. 2007;45:456–465. [Google Scholar]