

Abstract
A 67-year-old man was referred to our institution for the management of a left-sided intracardiac mass discovered following two cardioembolic events. Imaging studies revealed a highly mobile mass attached to the ventricular side of a calcified mitral annulus. The mass had not been present on echocardiography 1 year earlier. Surgical resection was performed. Microscopic examination confirmed the diagnosis of a calcified amorphous tumour. The postoperative course was unremarkable, and the patient remains asymptomatic and without recurrence of a mass or neurological event after a 12-month follow-up.
Background
A calcified amorphous tumour (CAT) of the heart is a rare non-neoplastic intracavitary cardiac mass, with microscopic features of calcification and amorphous fibrinous material. Since its first description in 1997 as a specific entity by Reynolds et al,1 several case reports have been published. Among them, cases of CAT arising from mitral annular calcification (MAC) seem to constitute a specific subgroup and were thought to be exclusively associated with end-stage renal disease. Ours is the first reported case of MAC-related CAT in a patient with normal renal function, and stresses the high embolic risk and fast growth characteristics associated with this subgroup of CAT.
Case presentation
A 67-year-old man with a medical history of hypertension and hypercholesterolaemia was referred to our institution for the management of a left-sided intracardiac mass discovered after two embolic events. One year before admission, the patient had presented a transient ischaemic attack characterised by diplopia and facial dysesthaesia with disseminated punctate lesions in multiple territories on brain MRI scan. The carotid ultrasound was unremarkable. Transthoracic and transoesophageal echocardiography as well as cardiac MRI scan had revealed mitral annulus calcification, without mass or other definite cardioembolic source. The patient was discharged on aspirin and clopidogrel. One year later, the patient presented a second cerebrovascular embolic accident revealed by a left eye scotoma due to a retinal artery branch occlusion.
Investigations
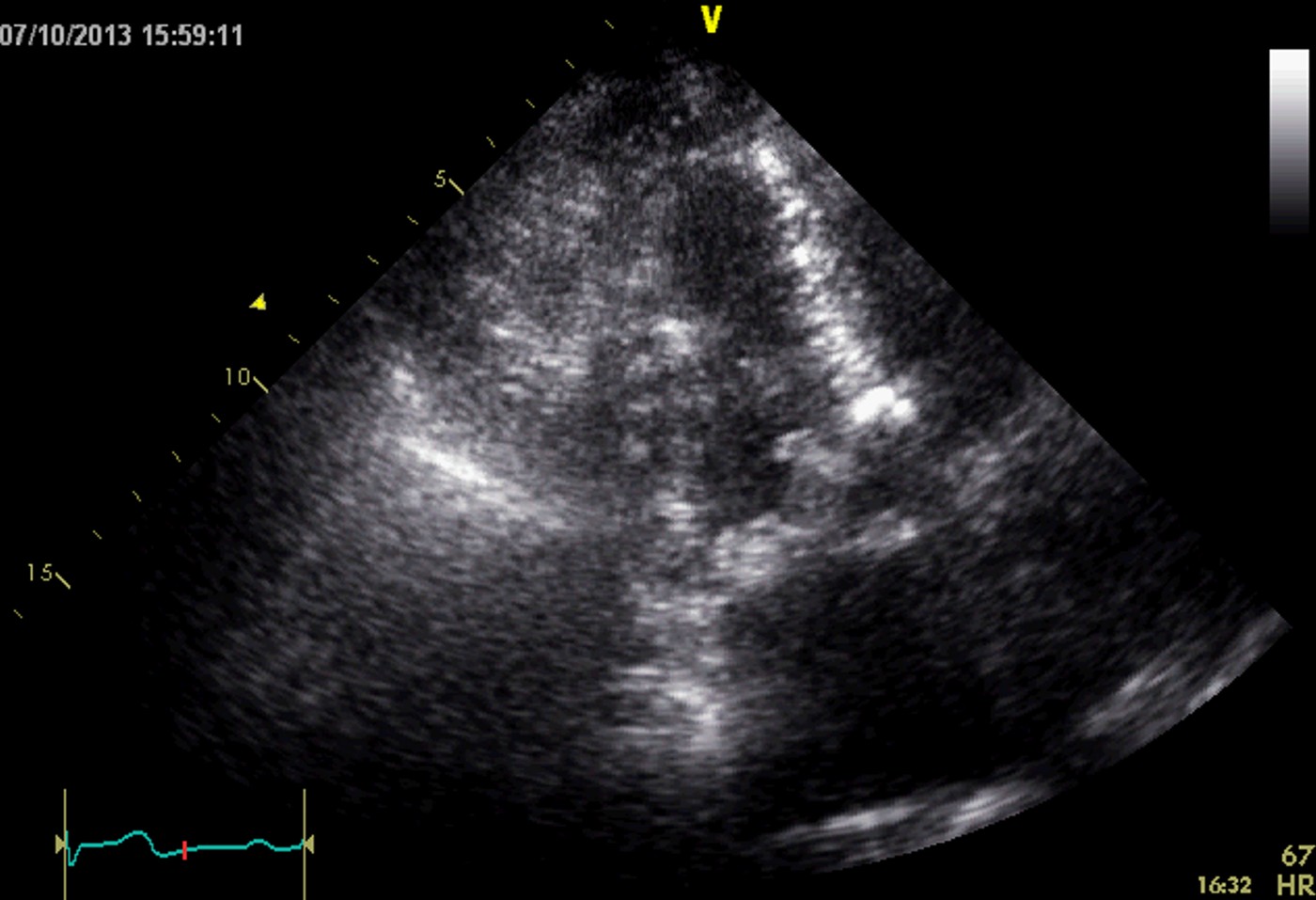
Transthoracic echocardiography showed a highly mobile mass (9×7 mm) attached to the ventricular side of a calcified mitral annulus, close to its posterior commissure (figure 1 and video 1). Platelet and white cell counts, coagulation studies, thrombophilia screening and tests of renal function, as well as serum levels of glucose and inflammatory markers (C reactive protein) were normal.
Figure 1.

Two-dimensional echocardiography. Echocardiographic four-chamber view (A) showing a mobile mass 7×9 mm, attached on the ventricular side of the mitral annulus, close to the posterior commissure. Zoom view (B) allows characterisation of the relationship of the mass (small arrows) with the mitral leaflets (large arrows). LV, left ventricle; LA, left atrium; RV, right ventricle.
Two-dimensional echocardiography. Cine-loop, apical five-chamber view showing the swinging mobile mass, attached on the ventricular side of the mitral annulus.
Differential diagnosis
Differential diagnoses of a highly echogenic mobile mass involving the mitral annulus include non-neoplastic causes such as a calcified thrombus, vegetation, caseous calcification of the mitral annulus and tophaceous pseudogout or tumoral calcinosis of the mitral valve, and, more infrequently, neoplastic aetiology such as calcified myxoma. Taking into account the location of the mass, its echocardiographic characteristics and the lack of evidence of infective endocarditis, we suspected the diagnosis of CAT.
Treatment
In order to prevent recurrent neurological events and to further confirm the diagnosis, the patient underwent surgical resection of the mass. Median sternotomy under cardiopulmonary bypass was performed, with mass resection through the aortic valve after a transversal aortotomy. The tumour consisted of a white-greyish 7×3×2 mm friable lump. It was taken out in one piece after resection of its foot in the ventricular muscle. Despite numerous pinkish ventricular trabeculations making it very hard to spot even under direct vision, the precise preoperative echocardiographic description of the mass markedly facilitated its surgical localisation. Microscopic examination confirmed the diagnosis of CAT (figure 2).
Figure 2.

Tumour, microscopic image. Microscopic findings showing heterogeneous calcium deposits with surrounding amorphous eosinophilic and fibrinous material (H&E, original ×400).
Outcome and follow-up
The postoperative course was unremarkable. The patient remains asymptomatic and without any evidence of mass or recurrent neurological event after 12 months.
Discussion
Presentation of CAT may be incidental, but most of the time it presents with symptoms related to embolisation or obstruction depending on the size and the location of the mass. Kubota et al2 proposed the descriptive term of ‘swinging calcified amorphous tumour’ for mobile lesions arising from a MAC. This subgroup of CAT seems to carry a high embolic risk, rapid growth characteristics and is usually associated with end-stage renal disease.2–5 The growth rate of CATs is largely unknown, but may be relatively fast, especially in MAC-related CAT, such as that described in the present report. Indeed, our patient developed a significant mass in less than 1 year; moreover, tumours growing very rapidly in a time span of 6 weeks to 1 year have been reported.2 4 Surgical resection remains the diagnostic and therapeutic standard for CAT, although large series and randomised trials are lacking to assess the natural history and the best management strategy for this rare disease.
Learning points.
A calcified amorphous tumour (CAT) is a rare non-neoplastic intracavitary cardiac mass.
Symptoms are usually related to embolisation or obstruction depending of the size and the location of the mass.
On echocardiography, CAT usually appears as a calcified endocavitarian mass, located in any cardiac chamber, valves or valvular annuli.
Differential diagnosis with other cardiac masses will require surgery for histological confirmation in most cases, as clinical presentation of patients with cardiac masses tends to be similar.
Mitral annular calcification-related CATs seem to carry a high embolic risk and rapid growth characteristics and are usually, but not always, associated with end-stage renal disease.
Footnotes
Twitter: Follow Quentin de Hemptinne at @qdehempt
Contributors: QdH and PU were the treating cardiologists in the reference centre and wrote the report. J-PB is the referring cardiologist of the patient. DdC performed the surgical resection of the tumour. J-PB and DdC critically reviewed the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Reynolds C, Tazelaar HD, Edwards WD. Calcified amorphous tumor of the heart (cardiac CAT). Hum Pathol 1997;28:601–6. 10.1016/S0046-8177(97)90083-6 [DOI] [PubMed] [Google Scholar]
- 2.Kubota H, Fujioka Y, Yoshino H et al. Cardiac swinging calcified amorphous tumors in end-stage renal failure patients. Ann Thorac Surg 2010;90:1692–4. 10.1016/j.athoracsur.2010.04.097 [DOI] [PubMed] [Google Scholar]
- 3.Fujiwara M, Watanabe H, Iino T et al. Two cases of calcified amorphous tumor mimicking mitral valve vegetation. Circulation 2012;125:e432–4. 10.1161/CIRCULATIONAHA.111.072793 [DOI] [PubMed] [Google Scholar]
- 4.Kawata T, Konishi H, Amano A et al. Wavering calcified amorphous tumour of the heart in a haemodialysis patient. Interact Cardiovasc Thorac Surg 2013;16:219–20. 10.1093/icvts/ivs430 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mohamedali B, Tatooles A, Zelinger A. Calcified amorphous tumor of the left ventricular outflow tract. Ann Thorac Surg 2014;97:1053–5. 10.1016/j.athoracsur.2013.06.115 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Two-dimensional echocardiography. Cine-loop, apical five-chamber view showing the swinging mobile mass, attached on the ventricular side of the mitral annulus.