

Abstract
Background
Most colonoscopic complications are polypectomy-related and occur more frequently during the removal of numerous small polyps. Therefore, it is important to have the best polypectomy approach of small polyps. The aim of the present animal study was to investigate the effectiveness and safety of cold snare polypectomy (CSP) technique combined with light pull of the snare in order to peel the mucosal and upper submucosal layer, namely pull CSP (PCSP), for the removal of polyps sized up to 12 mm in porcine models.
Methods
We performed a series of polypectomies in the pig colon with a double-channel experimental gastroscope using PCSP technique.
Results
Thirty cases of “polyps” larger than 7 mm and up to 12 mm were treated using PCSP technique. No sign of perforation or bleeding was observed in all cases performed with PCSP.
Conclusions
According to our preliminary results in this animal model, PCSP could be a safe and effective technique for flat colonic polyp removal up to 12 mm in size consistent with the basic polypectomy principles.
Keywords: Keywords Cold snare polypectomy, flat polyp, small polyp, pull technique
Introduction
Colonoscopy has been widely acknowledged as the gold standard medical procedure for colon cancer prevention by performing polypectomy. Most colonoscopic complications are polypectomy-related and occur frequently during the removal of numerous small polyps (<8 mm) [1-3]. Therefore, the best polypectomy approach of small polyps is important. The selection of the appropriate polypectomy technique mainly depends on the endoscopist’s preference and experience, but also on the polyp’s size and shape.
Cold snare polypectomy (CSP) has proven to be safe, effective and quicker than hot snare polypectomy (HSP), and could also be considered as the ideal procedure for small polyp removal without the risk of electrocautery burn and perforation [4]. With CSP the risk of perforation and delayed bleeding is excluded and recent studies have also proven its safety regarding acute intraprocedural bleeding [4-6]. CSP is currently used on pedunculated polyps of up to 5 mm in size and sessile polyps of the same size. Moreover, CSP is also used in flat polyps up to 10 mm by using the piecemeal CSP technique.
During CSP technique, the endoscopist has to ensnare a 1- to 2-mm rim of normal tissue around the edge of the polyp. This is essential for the complete eradication of the polyp without the risk of recurrence. However, cutting through the polyp by fully closing of the snare without the application of current, CSP seems to be impossible in several cases. Therefore, we have to release the polyp, reattach the snare and try to remove the polyp in smaller pieces using piecemeal CSP or alternatively cut through the polyp with the use of electric current (HSP). In cases of flat polyps up to 12 mm in size that cannot be eradicated by conventional CSP, we propose the use of “pull CSP (PCSP)” technique.
The aim of the present preliminary animal study was to investigate the effectiveness and safety of CSP technique combined with light pull of the snare in order to peel mucosal and upper submucosal layer (PCSP) for the removal of “polyps” sized up to 12 mm in porcine models.
Materials and methods
The study took place in the experimental research center of ELPEN Pharmaceuticals (Athens, Greece) at a fully equipped endoscopic unit. Registration number: 2972 (9/5/2012), Athens Central Veterinary Authority. Two landrace porcines were used. We accomplished bowel cleansing of the animals by adding phospho-soda agents in their water. Colonoscopies were conducted under the influence of general anesthesia. According to the anesthesiologic protocol, animals were premedicated with an intramuscular injection of ketamine hydrochloride, midazolam, and atropine sulfate. The marginal auricular vein was catheterized and anesthesia was induced with an intravenous propofol. They were then intubated with an endotracheal tube.
We performed a series of polypectomies in the colon with a double-channel experimental gastroscope (GIF-2T160; Olympus Optical, Tokyo, Japan). Two different types of braided snares were used: the Master® Snare/10mm (Olympus Medical Systems, Tokyo, Japan) and the Exacto® Snare/9mm (US Endoscopy, Mentor, Ohio). The Exacto® Snare is designed exclusively for CSP, is smaller than the Master® Snare and 33% thinner than traditional braided wires. During our experiments, the snare was inserted into the first channel of the endoscope and was consecutively opened and attached in parallel to the mucosa. The “polyps” were created by grasping normal colonic tissue using biopsy forceps, which was inserted by the second channel of the endoscope. When normal mucosa up to 12 mm in size was ensnared, we closed the snare and tried to cut through by using conventional CSP. When the removal of the “polyp” was impossible just by fully closing the snare and consequent cutting through, we tried PCSP technique. This technique consists of a light pull of fully closed snare with an upward direction towards the channel of the scope, in order to peel mucosa and upper submucosal layer, without damaging the entire submucosal layer. Application of mechanical pull of the snare leads to the eradication of the polyp (Fig. 1, 2). Each “polyp” was retrieved separately for histopathological examination. The size of the polyp was measured after the removal by the pathologist.
Figure 1.
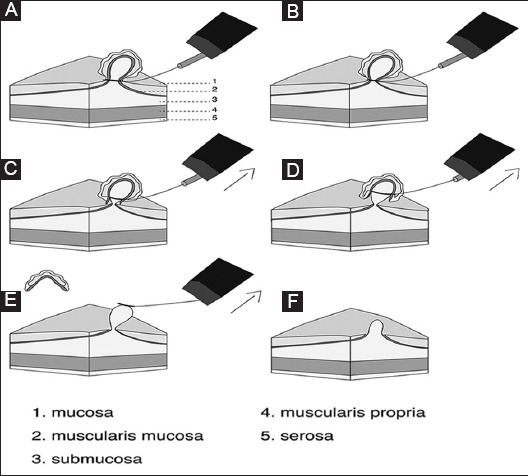
(A) Snaring of the polyp with 1-2 mm rim of normal tissue around it. (B) Fully closing the snare and maintaining this position by the nurse. (C) Starting of an upwards powerfully pulling of the snare and subsequent peeling of the polyp, muscularis mucosa and upper submucosa. (D) Continuing pulling the snare. (E) Complete eradication of the polyp with pull cold snare polypectomy technique. (F) Submucosal chord (“nipple” sign) after polypectomy which disappears with air insufflation
Figure 2.
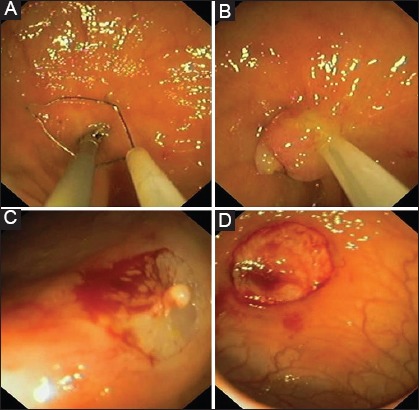
(A) Creation of the polyp using a double channel gastroscope. (B) Polyp grasped by the Exacto® snare. (C) Defect after pull cold snare polypectomy. The “nipple” sign. (D) Levelness of the defect after air insufflation
Results
Fifteen cases of “polyps”, larger than 7 mm and up to 12 mm in size, were effectively treated with each of two snares by using PCSP technique. No sign of perforation or bleeding was observed in all cases performed by PCSP technique with both Master® and Exacto® Snare. There were only 3 cases of intraprocedural bleeding during the removal of the largest parts of the mucosa (10-12 mm), which stopped spontaneously after a few minutes without application of coagulation or clipping. Both snares were equally effective in PCSP technique. All “polyps” were fully eradicated en bloc with PCSP. Following polyp removal, a submucosal chord was observed in the defect (the “nipple” sign) (Fig. 2C). The chord disappeared after air insufflation a few minutes later (Fig. 2D).
Pathological reports of removed polyps were in accordance with our hypothesis, which supports that PCSP excoriates mucosal layer, muscularis mucosa, and upper submucosal layer (Fig. 3). Nevertheless, this technique maintains the deeper submucosal layer and muscularis propria in a stable condition. After the completion of the polypectomy series with both CSP and PCSP, the colon from each pig was retrieved separately and was examined macroscopically. No sign of perforation was observed.
Figure 3.
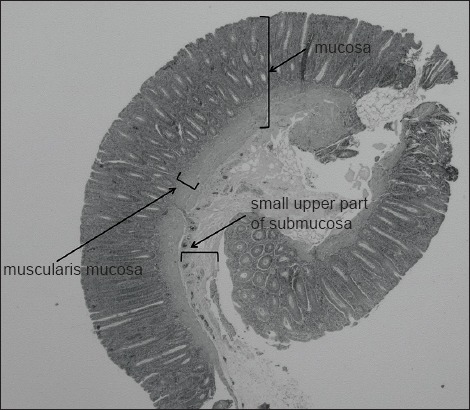
Histological section from the “polyp” of the pig showing the mucosa and a small fragment of the submucosa from large bowel wall (x200, H&E)
Discussion
The preliminary data from this animal study support the hypothesis that PCSP in colon could be an effective and safe technique. The advantages of our suggestion are the following: Firstly, PCSP offers the ability to eradicate larger polyps (up to 12 mm) than conventional CSP (<8 mm). Moreover, this technique is superior to piecemeal CSP, already applied in flat polyps up to 10 mm, since the polyp is removed in one piece en bloc enhancing the accuracy of the pathological examination. Additionally, PCSP technique could offer a time advantage in comparison with HSP. This is due to the needlessness of snare connection with the diathermy or application of the grounding plate.
We created the hypothesis of PCSP technique in order to minimize the use of electric current application during colonic polyp removal avoiding the risk of electrocautery burn and perforation. Small polyp removal in everyday practice of busy endoscopy suites should be performed with a quick, safe, and easy-to-apply method. The diathermic removal of small polyps through HSP is not always riskless. There is a low but significant risk of perforation and serious delayed bleeding. This risk can be overpassed with PCSP, which should be applied when the endoscopist faces difficulties in cutting through the polyp just by fully closing of the snare. The choice of re-opening the snare in such cases may damage the surface of the polyp and cause superficial hemorrhage that leads to lack of endoscopic view, inadequate eradication, and waste of time. At this point, we suggest light pulling of the fully closed snare and eradication of the polyp en bloc, additionally to the conventional CSP technique.
PCSP might be a useful tool for quick, complete, and safe eradication of flat colonic polyps of up to 12 mm. In this study both braided snares used were equally effective in PCSP technique.
Another fact we consider that strengthens our study is that the pig colon wall is not identical to the human one. Specifically, pig colon is longer but thinner than the human one [7]. This reinforces the safety of our technique, since PCSP did not lead to perforation in the thinner colonic wall of the pig, hence we assume that the performance of this technique in humans is appropriate to test.
The major weakness of this study is the absence of real polyps. The removed polyps were artificial and not real, created by normal pig colonic tissue as mentioned above. The vasculature in artificial polyps and submucosal layer of pigs are different than in human polyps, thus a study to confirm the risk of post-PCSP bleeding in humans is necessary. Secondly, our study was not randomized with diathermy technique, thus it is referred only as a first attempt to investigate PCSP technique at an animal model. We believe that, according to our results, PCSP could be suggested as an additional technique to CSP for flat polyp removal. Further studies conducted in humans are necessary to evaluate our hypothesis.
In conclusion, according to our preliminary results in this animal model, PCSP is consistent with the basic polypectomy principles and could be considered as a safe and effective method for the removal of flat colonic polyps sized of up to 12 mm.
Biography
Venizeleion General Hospital, Heraklion, Crete; Experimental-Research Center, ELPEN, Athens, Greece
Footnotes
Conflict of Interest: None
References
- 1.Levin TR, Zhao W, Conell C, et al. Complications of colonoscopy in an integrated health care delivery system. Ann Intern Med. 2006;145:880–886. doi: 10.7326/0003-4819-145-12-200612190-00004. [DOI] [PubMed] [Google Scholar]
- 2.Paspatis GA, Vardas E, Theodoropoulou A, et al. Complications of colonoscopy in a large public county hospital in Greece. A 10-year study. Dig Liver Dis. 2008;40:951–957. doi: 10.1016/j.dld.2008.02.041. [DOI] [PubMed] [Google Scholar]
- 3.Tolliver KA, Rex DK. Colonoscopic polypectomy. Gastroenterol Clin North Am. 2008;37:229–251. doi: 10.1016/j.gtc.2007.12.009. [DOI] [PubMed] [Google Scholar]
- 4.Paspatis GA, Tribonias G, Konstantinidis K, et al. A prospective randomized comparison of cold vs hot snare polypectomy in the occurrence of postpolypectomy bleeding in small colonic polyps. Colorectal Dis. 2011;13:e345–e348. doi: 10.1111/j.1463-1318.2011.02696.x. [DOI] [PubMed] [Google Scholar]
- 5.Repici A, Hassan C, Vitetta E, et al. Safety of cold polypectomy for <10 mm polyps at colonoscopy: a prospective multicenter study. Endoscopy. 2012;44:27–31. doi: 10.1055/s-0031-1291387. [DOI] [PubMed] [Google Scholar]
- 6.Ichise Y, Horiuchi A, Nakayama Y, et al. Prospective randomized comparison of cold snare polypectomy and conventional polypectomy for small colorectal polyps. Digestion. 2011;84:78–81. doi: 10.1159/000323959. [DOI] [PubMed] [Google Scholar]
- 7.Yen JT. The large intestine. In: Pond WG, Mersmann HJ, editors. Biology of the domestic pig. Ithaca and London: Comstock Publishing Associates, a division of Cornell University Press; 2001. p. 429. [Google Scholar]