

A 65-year-old man underwent computed tomography scan for surveillance of colon cancer and discovered an incidental 2 cm × 2.3 cm × 2.2 cm esophageal mass. The patient was completely asymptomatic, without dysphagia or weight loss. An upper gastrointestinal endoscopy was unremarkable while an endoscopic ultrasound (EUS) revealed an homogenous hypoechoic well-circumscribed subepithelial mass with some calcifications inside, originating from the muscle layer and that completely encircled the upper third of the esophagus (Fig. 1A). EUS-guided fine-needle aspiration (EUS-FNA) (Fig. 1B) showed groups of spindle-shaped cells. The immunohistochemistry was positive for desmin (Fig. 2A) and smooth muscle actin (Fig. 2B) while negative for CD34 and CD117 expression. A diagnosis of circumferential esophageal leiomyoma was made. After explanation of the condition and its long-term implications, the patient refused surgical treatment and is currently asymptomatic, with no change in size of the lesion over the last 2 years.
Figure 1.
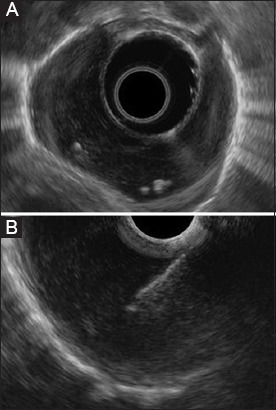
Endoscopic ultrasound findings. (A) A homogenous hypoechoic well-circumscribed tumor with some calcifications inside, originating from muscle layer and that completely encircles the upper third of the esophagus. (B) Endoscopic ultrasound-guided fine-needle aspiration of the tumor
Figure 2.
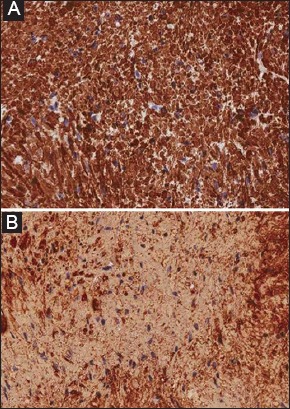
Histologic examinations showed groups of spindle-shaped cells with relatively low cellularity. The immunohistochemistry was positive for (A) desmin and (B) smooth muscle actin (40x total magnification)
Although true leiomyoma is the most common benign lesion of the esophagus, circumferential shape and calcifications are rare findings, especially in the upper esophagus [1,2]. It has become important to distinguish leiomyoma from other subepithelial masses, which have different prognoses and treatment options. EUS-FNA has proven to be a safe and effective technique to diagnose these lesions, especially when immunohistochemical analysis is performed. Asymptomatic leiomyomas may be followed up periodically as they have a slow growth rate, and negligible risk of malignant transformation. Surgical excision is the mainstay of treatment and is recommended for symptomatic leiomyomas and those greater than 5 cm [1].
Biography
A. Murri Hospital, Polytechnic University of Marche, Fermo, Italy
Footnotes
Conflict of Interest: None
References
- 1.Mutrie CJ, Donahue DM, Wain JC, et al. Esophageal leiomyoma: a 40-year experience. AnnThorac Surg. 2005;79:1122–1125. doi: 10.1016/j.athoracsur.2004.08.029. [DOI] [PubMed] [Google Scholar]
- 2.Walters DM, Vaughn NH, Isbell JM, et al. Leiomyoma presenting as a massive calcified circumferential esophageal mass. AnnThorac Surg. 2013;96:1851–1854. doi: 10.1016/j.athoracsur.2013.01.097. [DOI] [PubMed] [Google Scholar]