

Abstract
The development of protease inhibitors (PIs) such as telaprevir and boceprevir constitutes a milestone in chronic hepatitis C antiviral treatment since it has achieved sustained virological response (SVR) rates of up to 75% in naïve and 29-88% in treatment-experienced patients with genotype 1 infection. Both require combination treatment with pegylated interferon (PEG-IFN) plus ribavirin (RBV) as PI monotherapy results in resistant mutations. New direct acting antiviral agents (DAAs) have recently been approved or their approval is imminent. Simeprevir administered orally as one pill per day in combination with PEG-IFN/RBV will be the next PI to be approved. The SVR rates at about 72-80% for treatment-naïve patients are not a major improvement over telaprevir or boceprevir. However, this treble combination has fewer side effects and drug-drug interactions and most patients undergo shorter treatment duration (24 months) due to earlier treatment responses. Sofosbuvir is the first available once-daily NS5B polymerase inhibitor which has been approved in combination with PEG-IFN/RBV for just 12 weeks with 89% SVR in treatment-naïve patients with genotype 1 infection and 83-100% in treatment-experienced patients with genotypes 2/3. The current review focuses on the recent rapid and continuous developments in the management of chronic HCV infection with DAAs in combination with PEG-IFN/RBV.
Keywords: Keywords Protease inhibitors, NS5B polymerase inhibitors, NS5A inhibitors, cyclophilin inhibitors, pegylated interferon plus ribavirin
Introduction
Chronic hepatitis C virus (HCV) infection affects approximately 170 million people worldwide [1] and long-term carriage may lead to the development of cirrhosis, liver decompensation and hepatocellular carcinoma, a major indication for liver transplantation, particularly in Western countries [2]. HCV is classified into 6 major genotypes. Some genotypes have a restricted geographical distribution (genotypes 4-6), while others (genotypes 1-3) are more broadly disseminated. Genotype 1 (subtypes 1a and 1b) is the most prevalent genotype in the world. Genotype 2 is found in clusters in the Mediterranean region, genotype 3 is most prevalent among intravenous drug users and genotype 4 is found mostly in Egypt, while genotypes 5 and 6 are less frequent [3]. The HCV genotypes strongly affect the likelihood of response to antiviral treatment.
During the last decade, the standard of care (SOC) for patients with HCV genotypes 2 or 3 consisted of pegylated interferon (PEG-IFN) alfa-2a or alfa-2b combined with ribavirin (RBV), usually for 24 weeks, achieving rates of sustained virological response (SVR), i.e. absence of HCV RNA at 6 months or more after cessation of therapy, of about 75-85%. The SOC for patients with genotypes 1 and 4 also consisted of PEG-IFN and RBV, but usually for 48 weeks, resulting in SVR rates of 40-50% for genotype 1 and 55-65% for genotype 4 patients [4,5]. The SVR rates are substantially lower in previous non-responders to PEG-IFN and RBV, in whom the proportion of genotype 1 patients is higher due to the lower initial SVR rates. Justifiably therefore, new treatment approaches with improved efficacy have focused on patients with genotype 1 infection. In addition and regardless of HCV genotype, there are chronic HCV patients who cannot be treated with PEG-IFN and RBV for several reasons. First and of most clinical relevance, PEG-IFN therapy is contraindicated in patients with decompensated liver disease. Second, patients may not tolerate and/or may have other contraindication(s) to treatment with PEG-IFN or RBV. So, there is a definite need for new antiviral drugs with better efficacy, improved tolerance and good safety profiles for the treatment of chronic HCV infection.
Our better understanding of the HCV genomic structure, life cycle and the key viral enzymes has led to the development of DAAs which hold promise for the future. In 2011, the NS3/4A protease inhibitors telaprevir and boceprevir were approved for the treatment of chronic HCV genotype 1 infection by the FDA, EMA and other agencies. Monotherapy with these agents resulted in the selection of drug resistant variants. However, the addition of these agents to the SOC consisting of the combination of PEG-IFN and RBV led to reduced frequencies of resistant mutants and viral breakthrough, and to significantly higher SVR rates in both treatment-naïve and treatment-experienced patients. The current review focuses on the recent rapid and continuous developments in the management of chronic HCV infection with DAAs in combination with PEG-IFN/RBV.
HCV genome organization and new antivirals
HCV has a positive-sense, single-stranded RNA genome of about 9.6 kilobases in length that encodes a polyprotein of approximately 3000 amino acids long [6,7]. The open reading frame for the polyprotein is flanked by 5’ and 3’ untranslated regions (UTRs), which contain elements that regulate translation and replication respectively. The polyprotein is generated by the host cell translation machinery and cleaved co- and post-translationally by host and viral proteases to yield the mature viral proteins. The N-terminal segment of the polyprotein encodes the structural components of the virus (Core, E1, E2 and p7). The core protein forms the capsid into which the virus genome is packaged, while the glycoproteins E1 and E2 are located in the lipid bilayer constituting the viral envelope surrounding the capsid, derived from the endoplasmic reticulum membrane. Strictly speaking, P7 is not a structural component of the virion but is thought to be a viroporin required for virus assembly [8,9].
The C-terminal component of the polyprotein contains the non-structural proteins (NS2, NS3, NS4A, NS4B, NS5A and NS5B). NS2 and NS3 are viral proteases required for the processing of the HCV non-structural portion of the polyprotein [10]. NS3 is a multifunctional enzyme, with serine protease, helicase and nucleotide triphosphatase activities, that forms a stable heterodimeric complex with its NS4A cofactor, essential for protein folding and stabilization. The NS3A/NS4A complex cleaves the junctions between NS3/4A, NS4A/NS4B, NS4B/NS5A and NS5A/NS5B. NS3 has also helicase activity necessary for the unwinding of the HCV genome during replication of the RNA [11]. NS4B, a hydrophobic transmembrane protein, is the presumed central organizer of the HCV replicase complex and a main inducer of intracellular membrane rearrangements that constitute the membraneous web [12]. NS5A is an RNA-binding phosphoprotein required for RNA replication and assembly of infectious virus particles [13], whilst NS5B is the RNA-dependent RNA-polymerase required for viral replication.
The nonstructural proteins mentioned above have been the target for DAAs or Specifically Targeted Antiviral Therapy for hepatitis C (STAT-C). In particular, DAAs under development include NS3/4A PIs, and NS5B polymerase as well as NS5A inhibitors. In addition, inhibitors which target host factors such as cyclophilin, which has an important role in HCV RNA replication, are also under development (Fig. 1).
Figure 1.
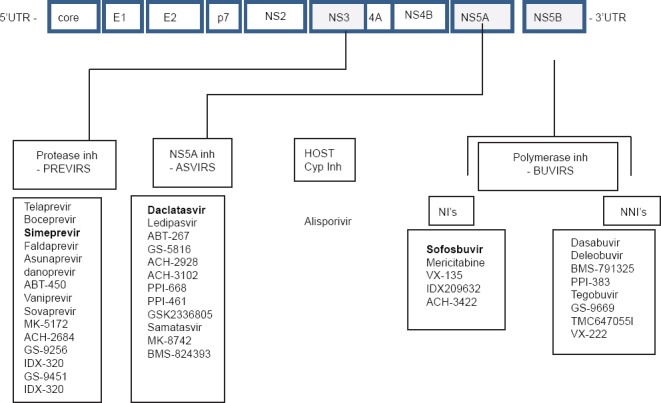
Different families of Direct Acting Antiviral drugs. First-generation protease inhibitors in italics. Available drugs approved by EMA and recommended by EASL in bold. Faldaprevir and Deleobuvir development has stopped
Inh, inhibitors; Cyp, cyclophilin; NIs, nucleos(t)ide inhibitors; NNIs, non- nucleos(t)ide inhibitors
NS3/4A protease inhibitors
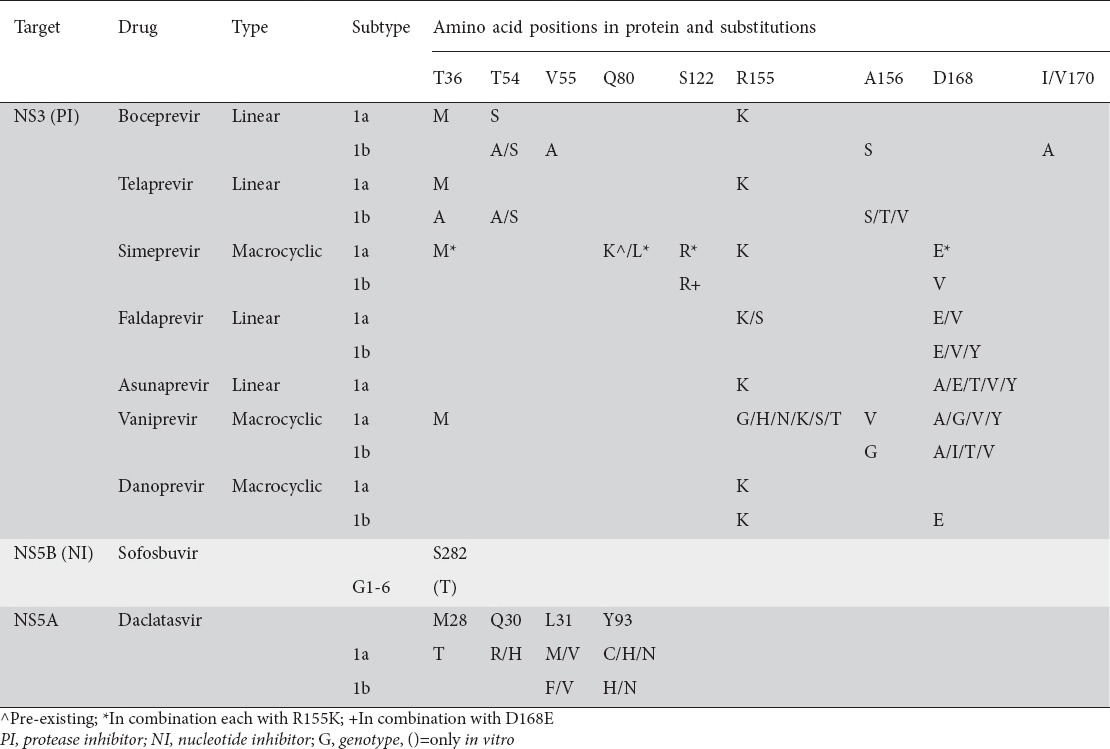
Two first-generation, linear NS3/4A PIs, boceprevir and telaprevir, were approved in the USA and Europe in 2011 for clinical use in patients with genotype 1, while numerous new NS3/4 PIs are currently under evaluation in clinical trials (Fig. 1). Boceprevir and telaprevir have high antiviral potency only against genotypes 1 and 2 [14], but a low barrier to resistance. In particular, resistant HCV strains develop within a few days of monotherapy with both of these agents [15,16], while most mutations confer cross resistance to both drugs (V36A/M, T54S/A, V55A, R155K/T/Q, A156S, A156T/V) (Table 1) [17]. HCV subtype 1a develops resistance more frequently and more rapidly than subtype 1b [18], as just one (instead of two in subtype 1b) nucleotide change (R155K) is enough for an amino acid substitution to lead to the emergence of a resistant strain. Codon 155 is the main cause of resistance when different nucleotide substitutions at this site confer cross resistance to nearly all PIs (only MK-5172 exhibits activity against R155 variants) [19]. Because of the low barrier to resistance, boceprevir and telaprevir should always be used in triple combinations together with PEG-IFN and RBV. Since viral resistance may develop even in triple combinations with PEG-IFN and RBV, strict stopping rules are applied in triple therapy-based regimens. Newer, first-generation NS3/4A inhibitors under development are mainly macrocyclic compounds (simeprevir-TMC-435, danoprevir-R7227, vaniprevir-MK-7009) and the linear asunaprevir (BMS-650032). Newer first generation as well as second- and third-generation NS3/4A inhibitors (i.e. faldaprevir-BI 201335, GS-9256, ABT-450, MK-5172 etc.) are expected to have better pharmacokinetics for once daily dosage, less complicated treatment algorithms and less side effects compared to boceprevir and telaprevir. However, as shown in Table 1, use of these PIs in monotherapy regimens leads to amino acid substitutions that confer cross-resistance, precluding switch from one PI to another.
Table 1.
Resistance mutations induced by DAAs when used as monotherapy (modified from De Luca et al, Fridell et al [59,60])
NS5B polymerase inhibitors
There are two categories of NS5B polymerase inhibitors: nucleos(t)ide (NIs) and non-nucleoside inhibitors (NNIs) (Fig. 1). NIs mimic the naturally occurring nucleos(t)ides and thus are incorporated into the nascent RNA chain causing premature chain termination [20]. NIs are considered to have a high genetic barrier to resistance, although single amino acid substitutions are able to confer drug resistance in vitro. Nevertheless, because the active site of NS5B is highly conserved and amino acid substitutions in any position of the active site can result in loss of function, such resistant variants are less fit requiring weeks or months to reach detectable levels in the presence of the drug. NIs have antiviral activity against all HCV genotypes (pan-genotype activity) as the active site of NS5B is well conserved across genotypes [21]. An S282T substitution detected in vitro in the presence of sofosbuvir has not been of particular concern in vivo. However, this substitution has been detected following combination treatment with mericitabine (nucleoside inhibitor, PSI-6130). Dual resistance (NS3 R155K, NS5B S282T) has been detected in two patients with breakthrough infection treated with mericitabine and ritonavir-boosted danoprevir +/- ribavirin [22].
NNIs bind to a distant site of the NS5B and cause a conformational change rendering the enzyme ineffective. In particular, NNIs bind to one of four allosteric sites on the surface of NS5B (“thumb” domain I, “thumb” domain II, “palm” domain I, “palm” domain II). NNIs have a more limited spectrum of activity being specifically targeted against genotype 1. Because NNIs bind more distantly from the active site, resistant variants are fit in the presence of the drug and therefore NNIs have a low barrier to resistance.
NS5A inhibitors
The NS5A protein is a regulator of replication. NS5A inhibitors have high antiviral activity against different genotypes, but a low genetic barrier to resistance. Daclatasvir (BMS-790052), a representative of this group of inhibitors (Fig. 1), is under evaluation in a number of drug combinations with promising results [23]. Resistance variants to NS5A inhibitors are not associated with impaired viral replication fitness and they do not disappear after the end of treatment. Persistence of NS5A resistance mutations was detected up to one year after stopping treatment [24]. Other NS5A inhibitors like BMS-824393, PPI-461, ledipasvir (GS-5885) and ABT-267 (Fig. 1) are still under clinical development.
Daclatasvir resistance is associated with a number of substitutions as shown in Table 1. Similar inhibitors such as ledipasvir and ABT-267, which are now in phase III clinical trials, could result in resistance mutations also. Newer NS5A inhibitors such as GS-5816, ACH-3102, and MK-8742, appear to have improved genetic barrier while maintaining potency [25]. Dual resistance however, has been reported following combination therapy with asunaprevir and daclatasvir (NS3 D168A/V, NS5A L31N+Y93Y) [26].
Factors influencing resistance
As discussed earlier, resistance mutations do occur when DAAs are used in monotherapy protocols. Moreover, resistance varies depending on the drug. As it is widely known, viral load in any individual is not homogeneous but consists of numerous variants which arise as a result of the poor fidelity and high error rate of the NS5B RNA polymerase. Unexpectedly, such variants carry resistance mutations to some of the existing DAAs. These naturally occurring resistance associated variants (RAVs) as they are known, vary in frequency ranging from 0.1-7.5% depending on the substitution, and according to subtype being higher in subtype 1a isolates than 1b [27]. The exception is the simeprevir resistant Q80K pre-existing 1a variant which has much higher frequencies compromising response to treatment as discussed later. Recorded frequencies are 48.1% in North America, 19.4% in Europe and 9.1% in South America, whilst this variant is rarely detected in 1b isolates (<1%). Other but less common RAVs include V36M/L, T54S, R155K and D168E.
Cyclophilin A inhibitors
Cyclophilins are host proteins involved in protein folding. They play an important role in the HCV lifecycle as regulators of replication. The cyclophilin inhibitor alisporivir (DEB-025) is a cyclosporine analog without its immunosuppressive properties that has shown pan-genotypic antiviral activity and has been used both alone and in combination with PEG-IFN and RBV with promising results [28-30]. Phase III trials with alisporivir are ongoing, but very recently the development of this drug was put on hold by the FDA due to safety concerns (a few cases of pancreatitis occurred, one of which was fatal).
Clinical trials
First-generation PIs
Telaprevir and boceprevir are first-generation NS3/4 PIs firstly approved in 2011. They are characterized by high antiviral activity against genotype 1. Phase III clinical trials evaluated telaprevir and boceprevir in combination with PEG-IFN/RBV (PR). ADVANCE [31], ILLUMINATE [32] and SPRINT-2 [33] enrolled treatment-naïve patients. REALIZE [34] and RESPOND-2 [35] enrolled treatment experienced patients. Telaprevir was administered for 8-12 weeks in combination with PR followed by 12-40 weeks of PR alone. Boceprevir was administered over the whole treatment period of 28-48 weeks in combination with PR except for the first 4 weeks lead-IN therapy with PR. Telaprevir with PR led to remarkably higher SVR rates compared to treatment with PR alone: 72-75% vs. 44% in treatment-naïve patients (ADVANCE and ILLUMINATE) and 31%, 57% and 86% in prior null, partial and relapse responders, respectively (REALIZE). Boceprevir with PR led to significantly higher SVR rates compared to treatment with PR alone: 63-69% vs. 38% in treatment-naïve patients (SPRINT-2) and 59-66% vs. 21% in previously treated patients (RESPOND-2). The last study did not include null responders. The PROVIDE study in which boceprevir with PR were given in treatment-experienced patients led to SVR rates of 38%, 67% and 93% in prior null, partial and relapse responders, respectively [36]. In a recent phase III study (OPTIMIZE), it was shown that telaprevir given twice daily was non inferior to telaprevir taken every 8 h [37]. The response rate was lower in cirrhotics according to the real-world CUPIC trial where SVR rates for prior null, partial and relapse responders were 19%, 40% and 74% for telaprevir and 0%, 38% and 54% for boceprevir, respectively (overall SVR rate was very similar between the 2 therapies: 40% for telaprevir plus PR and 41% for boceprevir plus PR) [38]. Safety data drawn from the CUPIC cohort study in cirrhotic patients demonstrated a high incidence of morbidity and mortality in IFN-based therapies with telaprevir or boceprevir especially in patients with specific risk factors, including serum albumin <3.5 g/dL and/or platelets < 100,000 cells/mm [39].
An interim analysis of the HCV-TARGET longitudinal observational study of sequentially enrolled patients in academic and community medical centers in North America who were treated with triple therapy including either telaprevir or boceprevir with PR showed that there was a virologic breakthrough rate of approximately 8% to 10%, and early discontinuation in approximately 1 in 4 patients, due to a variety of reasons including efficacy, adverse events (AEs), and lack or failure of stopping rules. Deaths were relatively uncommon, occurring in only 2% of the cirrhotic population, but early discontinuation and AE rates were higher in these patients. The key challenge was decompensation, which occurred in 11% of patients with cirrhosis [40].
A recent meta-analysis of boceprevir plus PR in patients with genotype 1 HCV infection and compensated cirrhosis including patients from the large phase III studies SPRINT-2 and RESPOND-2, as well as the PEG IFNa-2a, PROVIDE studies, and the Anemia Management Study showed that patients with cirrhosis would require better therapeutic options to improve their SVR rate. In this meta-analysis, patients with F3 and F4 fibrosis or cirrhosis had comparable SVR rates, at 54% and 55%, although both of these were substantially better than the SVR rates for F3 (26%) or F4 (17%) in patients treated with PR [41].
Vertex pharmaceuticals Inc will be discontinuing the sale and distribution of telaprevir (INCIVEK) in the United States by October 16th, 2014. The Company claims that this decision has been taken in view of alternative treatments and the diminishing market demand for the drug (BostonGlobe.com/Business).
Drugs recently approved or awaiting approval
Simeprevir (TMC435)
It is a second generation PI with antiviral activity in genotypes 1, 2, 4, 5 and 6. It is administered as a once daily tablet orally and has limited drug-drug interactions (DDIs). It is safe and well tolerated. It was approved by the FDA for genotype 1 treatment in November 2013 under the name of “OLYSIO”, in Japan in September 2013 and Europe in May 2014 (European Medical Agency approval).
PILLAR, a phase IIb study evaluated simeprevir in 386 treatment-naïve genotype 1 HCV-infected patients [42]. The study comprised 5 arms (75-79 patients each). The data demonstrated the superiority of simeprevir given at 2 different doses (75 and 150 mg) and durations (12 and 24 weeks) plus PR vs. PR alone. Treatment ended at week 24 if a rapid virological response (RVR) was achieved and maintained; all others continued on PR to week 48. Patients in the simeprevir arms achieved SVR rates of 75-86% versus 65% in patients with the classical 48-week PR regimen. Patients with the unfavorable IL28B genotypes CT or TT, achieved high rates of SVR (73% to 78%) with simeprevir, a finding that was first seen in boceprevir and telaprevir trials.
The randomized ASPIRE trial evaluated several different schedules of simeprevir; 100 mg or 150 mg daily in combination with PR for the treatment of 452 patients with genotype 1 infection who failed previous PR therapy [43]. Approximately 16% to 20% of patients in each treatment arm had cirrhosis. The study had 7 arms (61-65 patients each) and simeprevir with PR was given for 12 weeks followed by PR alone for a total of 48 weeks. SVR rates were 61-80% vs. 23% in the PR group alone, irrespective of daily simeprevir dosage. Virologic efficacy differed according to previous response such that SVR rates were substantially higher among previous relapsers (77-89% in simeprevir plus PR groups vs. 37% in the PR group alone) compared with previous non-responders (38-59% in simeprevir plus PR groups vs. 19% in the PR group alone).
PROMISE, a phase III trial evaluated PR and once-daily simeprevir (150 mg) for 12 weeks in 260 treatment-experienced genotype 1 infected patients [44], followed by PR alone for 12 or 36 weeks based on response-guided therapy (RGT) criteria. Patients on simeprevir and PR achieved 79% SVR vs. 36% rates with PR alone given for 48 weeks. Most patients receiving simeprevir were able to shorten therapy length to 24 weeks. Patients on simeprevir did not have AEs beyond those that occurred in patients given PR alone.
The randomized, double-blind, placebo-controlled phase III QUEST-1 clinical trial evaluated an RGT approach in the simeprevir arm, such that every patient received 12 weeks of simeprevir plus PR followed by PR alone for another 12 or 36 weeks, depending on the early on-treatment response. The majority of patients achieved undetectable HCV RNA at week 4, and the overall SVR rate at 12 weeks post-treatment was superior in the simeprevir-containing treatment arm: 80% vs. 50% in the PR control arm [45].
In QUEST-2, a trial with a similar design to QUEST-1, a very high overall SVR rate was seen with simeprevir plus PR: 81% compared with 50% to those receiving PR treatment. Again, a high proportion of patients qualified for RGT: 91% of individuals who received simeprevir were able to truncate therapy, with a high SVR rate of 86% in this subgroup. Similar to QUEST-1, the SVR rate in those who remained on treatment through 48 weeks was low, at 32%, although the number of patients was small [46].
The baseline Q80K polymorphism (Table 1) was present in 41% of patients with genotype 1a and associated with lower SVR12 rate in QUEST-1. Emergent NS3 protease mutations were detected in >90% of patients without SVR (genotype 1a: R155K alone, with mutations at positions 80 and/or 168; genotype 1b: most common mutation D168V, Q80R + D168E) [41,42].
Recent EASL Recommendations stated that patients with genotype 1 and 4 can be treated with a combination of weekly PEG-IFN-a, daily weight-based RBV and daily simeprevir (150 mg) for 12 weeks. PR should then be administered for an additional 12 weeks in treatment naïve and prior relapsers and for an additional 36 weeks in prior partial and null responders. Treatment should be stopped if HCV RNA level is >25 IU/mL at treatment week 4, 12 or 24. The combination is not recommended in patients infected with subtype 1a who have a detectable Q80K substitution at baseline [47].
In simeprevir trials, anemia was not significantly increased in contrast to the currently approved PIs boceprevir and telaprevir. There was some increase in rash with simeprevir exposure, although almost all cases of rash were grade 1/2 in severity. Serious AEs were reported at a rate of 3%. In both QUEST-1 and QUEST-2, transient bilirubin increases were noted; however, no other changes in liver parameters were seen.
Sofosbuvir
This is an NI of the RNA-dependent RNA polymerase with a high barrier to resistance and favorable clinical pharmacology profile. It has pan-genotypic activity. It is administered orally as a 400 mg tablet daily and has neither a food effect nor significant DDIs. It has proved safe and was well tolerated in several clinical studies (>2000 patients). The drug was approved by FDA for genotype 1 in combination with PR, and in genotypes 2 and 3 in IFN free regimens in December 2013 (SOVALDI), in Canada during the same month and Europe in Jan 2014 (European Medical Agency approval).
The randomized phase II ATOMIC study compared 3 different schedules of 400 mg of sofosbuvir (GS-7977) once daily plus PR in treatment-naïve patients with chronic genotype 1 HCV infection [48]. Three treatment arms were included in the study: 1) 12 weeks of the triple combination regimen; 2) 24 weeks of triple therapy; and 3) 12 weeks of sofosbuvir plus PR and then re-randomized to 12 additional weeks of sofosbuvir monotherapy or 12 weeks of sofosbuvir plus RBV. The study evaluated the shortest duration of IFN-based therapy examined to date. The results demonstrated that sofosbuvir plus PR for a total of 12 weeks yielded an SVR rate of 89%, equal to that achieved with extended treatment regimens. Sofosbuvir in combination with PR was generally well tolerated with no serious AEs attributable to sofosbuvir (only anemia, nausea and headache were recorded). In addition, among 4 patients with virologic relapse, none had evidence of the S282T resistance mutation by population sequencing.
The NEUTRINO study is an open-label, single-arm phase III registration trial in 327 treatment-naïve patients evaluating a regimen comprising sofosbuvir plus PR for 12 weeks [49]. The overall patient population included mainly those infected with genotype 1 (89%) as well as a few patients infected with genotypes 4, 5 and 6; 17% of patients in this trial had cirrhosis. This sofosbuvir-based triple-therapy regimen resulted in a very RVR, with the week 4 RVR rates approaching 99%. Typical of treatment regimens including sofosbuvir, on-treatment response was very high, with 99% of patients achieving virologic response at the end of treatment. The SVR rate from the entire trial population remained high at 90%, 12 weeks after the end of treatment.
Analyzing the groups based on viral genotype, patients with genotype 1 had an SVR rate of 89%, and the small number of patients with genotype 4, 5 and 6 had SVR rates between 96% and 100%. Overall, this sofosbuvir-based triple-therapy regimen resulted in very high SVR rates across all genotypes that were evaluated. Another important point from the NEUTRINO trial was the relative decrease in the overall response rates for patients with cirrhosis (SVR 80%) compared with non-cirrhotics (SVR 92%). No data with this regimen has been presented in treatment-experienced populations. Whether longer treatment duration is needed in the most difficult-to-treat population is unknown.
LONESTAR-2 was a phase III trial in which sofosbuvir was combined with PR for 47 treatment-experienced genotype 2 and 3 patients. This was a rather difficult population as approximately 50% had compensated cirrhosis. On the other hand, most of the treatment-experienced patients were relapsers, so we know that they have had a good response to PR. This study once again showed that genotype 2 patients are easier to cure. Interestingly, the SVR rate was similar to the IFN-free regimen of sofosbuvir plus RBV, with close to 100% overall SVR. Although the numbers are small, this trial has the highest SVR rate observed to date in treatment-experienced genotype 3 patients at 83%. Of note, cirrhotic treatment-experienced genotype 3 patients achieved the same 83% SVR rate as their non-cirrhotic counterparts [50].
Recent EASL Recommendations stated that patients with genotype 1, 2, 3 and 4 can be treated with a combination of weekly PEG-IFN-a, daily weight-based RBV and daily sofosbuvir (400 mg) for 12 weeks in total including naïve and treatment-experienced patients. No futility rules have been described for this drug [43].
No S282T mutations were detected in the sofosbuvir studies. Other NS5B genetic variants were not associated with change in phenotypic susceptibility. Regarding safety issues, sofosbuvir was generally well tolerated. Serious AEs were recorded in only 2% of patients. Low rates of treatment discontinuation due to AEs were reported.
Faldaprevir
This is a potent NS3/NS4 PI with antiviral activity against genotypes 1, 2, 4, 5 and 6 in vitro. The pharmacokinetics of faldaprevir allows oral, once-daily administration.
Faldaprevir, when administered for 24 weeks in combination with PR in treatment-naïve patients (SILEN-C1) achieved SVR rates of 72-84% [51]. SILEN-C3 [52] a phase 2a randomized, open-label, parallel group study compared the efficacy and safety of 12 vs. 24 weeks of 120 mg of faldaprevir administered once daily combined with 24 vs. 48 weeks of PR in 160 treatment-naïve patients with genotype 1 infection. Patients who achieved and maintained RVR stopped all treatment at week 24, otherwise they continued with PR to week 48. SVR was achieved by 67% and 74% of patients in the 12-week and 24-week groups, respectively. Most AEs were mild or moderate, and 6% of patients in each treatment group discontinued treatment due to AEs. Once-daily faldaprevir at 120 mg for 12 or 24 weeks with PR resulted in high SVR rates, and the regimen was well tolerated.
In the SILEN-C2 trial [53], 290 non-cirrhotic genotype 1 patients with prior null or partial response were randomized to different doses of faldaprevir plus PR on an RGT basis. SVR rates were 32-50%, in prior partial responders, and 21-35% in prior null responders in all faldaprevir groups.
STARTVerso 1 and 2 are PHASE III, registration trials evaluating faldaprevir, administered at 2 different doses in combination with PR in 24- vs. 48-week RGT regimens in genotype 1 treatment-naïve patients. SVR rates of 73% and 72% were achieved with 120 mg and 240 mg of faldaprevir plus PR vs. 50% with the classical PR regimen [54,55].
The baseline Q80K substitution was present in 23% of patients with genotype 1a but was not associated with the SVR12 rate [50]. Faldaprevir was generally safe and well tolerated with serious AE recorded in 7% of patients. Rates of gastrointestinal disorders, jaundice, dry skin, and photosensitivity were increased with the 240 mg b.i.d. dosage compared with the 240 mg q.d. dose.
Recently the German pharmaceutical company Boehringer Ingelheim has ceased development of its investigatory HCV drug faldaprevir. The company stated that “This decision was taken as there is no longer an unmet medical need for the faldaprevir IFN-based regimen that was the subject of the application.” (MedPage Today June 20, 2014).
Other triple or quadruple drug schedules
Other drugs in phase II trials are shown in Tables 2 and 3. The DAUPHINE trial evaluated the investigational protease inhibitor danoprevir boosted with ritonavir at several different doses and treatment schedules plus PR in treatment-naïve patients with genotype 1 or 4 infection. The results of this study demonstrated an 89% SVR12 rate with the highest danoprevir dose tested but with a high incidence of AEs mostly related to PR [56]. Other drugs which were evaluated in combination with PR are vaniprevir, daclatasvir, asunaprevir, MK-5172, and mericitabine.
Table 2.
Other combinations of one DAA with PEG-IFN/RBV (PR)
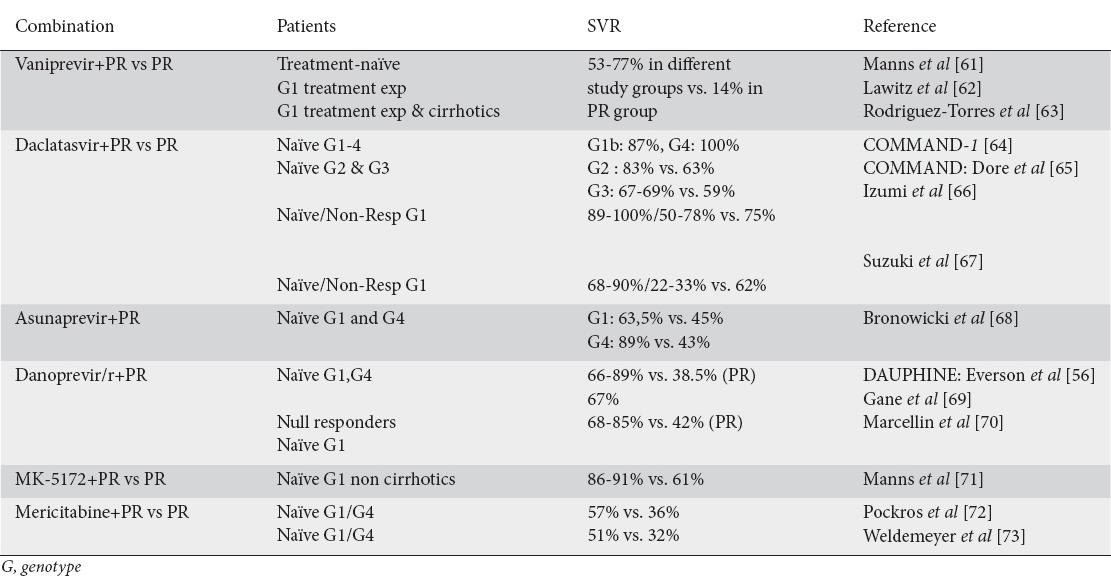
Table 3.
Quadruple therapy with two DAAs and PEG-IFN/RBV (PR)

A study in null responders treated with daclatasvir + asunaprevir combined with PR showed high response rates with the 4-drug regimen involving daclatasvir + asunaprevir + PR but lower with the daclatasvir + asunaprevir regimen. A better response rate was demonstrated with asunaprevir 200 mg b.i.d. vs. asunaprevir 200 mg q.d. [57].
Recent EASL Recommendations included sofosbuvir, simeprevir, and daclatasvir, each in combination treatment with PR. It is stated that patients with genotype 1b and 4 can be treated with a combination of weekly PEGF-IFN-a, daily weight-based RBV and daily daclatasvir (60 mg) for 24 weeks. Daclatasvir should be administered 12 weeks in combination with PR. Daclatasvir should be continued in combination with PR for an additional 12 weeks in patients who do not achieve an HCV RNA level <25 IU/mL at week 4 and undetectable at week 10. PR should be continued alone between week 12 and 24 in patients who achieve an HCV RNA level <25 IU/mL at week 4 and undetectable at week 10 [47].
Role of IL28B genotyping in treatment-naïve patients
Many trials have investigated the role of IL28B polymorphisms in triple therapy combining PR with PIs. The ADVANCE trial showed that telaprevir combined with PR increased SVR rates across all IL28B genotypes, but CC still achieved better SVR. It was demonstrated that CC patients tended to have better opportunity for RVR and shorter duration of therapy [31].
The above results were confirmed in SPRINT-2 [33] and RESPOND-2 [35] (triple combination with boceprevir) where 90% and 80% of patients respectively, with the favorable CC genotype were eligible for short duration therapy according to RGT criteria. However, post hoc analysis showed that similar SVR rates were obtained in patients with favorable genotype whether these received dual or triple therapy including boceprevir.
The prospective CONCISE study [58] which evaluated whether non-cirrhotic patients with the IL28B CC genotype who are infected with genotype 1 can receive a shortened 12-week regimen of PR plus telaprevir showed an SVR rate of 87% while those who continued PR for an additional 12 weeks reached an SVR rate of 97%.
In the PILAR study [42], among patients with non-CC genotype SVR rates were higher for patients on triple therapy of simeprevir plus PR, while in CC genotype patients the SVR rates were similar in both triple therapy and the standard of care (approximately 100%). These data once again underscore the influence of the unfavorable IL28B genotype associated with poor response to PR was ameliorated by the addition of simeprevir. However, the benefit of triple therapy compared to standard of care was not evident in patients with the favorable CC genotype.
For the aforementioned reasons, the EASL guidelines do not consider IL28B genotyping as a prerequisite for treating hepatitis C [47]. However, they suggest that in patients with the favorable CC genotype, achievement of RVR with PR in a lead-in period could justify the continuation of PR treatment without the addition of a PI.
Concluding remarks
In treatment-naïve chronically HCV-infected patients, an approximate 30% increase in SVR rates was achieved with the addition in PR of a PI like telaprevir, boseprevir, simeprevir or a NS5A inhibitor daclatasvir. A higher success rate of 40% was achieved with the addition of the NS5B polymerase inhibitor sofosbuvir. In treatment-experienced patients, the response rates for virologic relapsers were excellent, but these were lower for previous PR partial and null responders, particularly those with more advanced liver disease. It is obvious that IFN-based triple combination therapy still depends on the IFN sensitivity of individual patients and is absolutely contraindicated in certain groups of patients. To overcome these limitations, IFN-free therapy regimens should be administered including two or more different DAAs, which will make such treatments very expensive for poor resource countries.
Low and middle-income countries account for more than 80% of patients with chronic hepatitis C and most of the patients remain untreated even in the era of standard of care regimens. The sofosbuvir 12-week regimen costs approximately $84,000 but treatment (Sovaldi costs $1000 per pill, and Harvoni costs $1125 per pill) regimens with a PR backbone and a PI are less expensive. Drug costs are the biggest barrier to treatment since traditionally more than two thirds of the drug costs in low-income countries are not covered by health insurance but are borne by the patient. It is hoped that the approval of drugs from several pharmaceutical companies and the ensuing competition may result in lower drug costs in the future. Unless an important decrease in the cost of IFN-free regimens is achieved in the near future, the regimens with a PR backbone remain more easily affordable. In addition, in patients with the favorable IL28B CC genotype, achievement of RVR with PR, in a lead-in period, could justify the continuation of PR treatment, leading to less expenditure with maximum effectiveness.
Combinations of PR with first generation PIs require strict follow up with multiple measurements of viral load due to several stopping rules and a meticulous treatment algorithm. Moreover a 6-12 pill burden is needed per day contributing to poor adherence and severe side effects such as anemia. These PIs have limited efficacy in patients with cirrhosis and those with previous partial or null response to PR treatment. Apart from cirrhotics, treatment of special populations (e.g., patients with kidney disease, concurrent HIV infection, patients undergoing solid organ transplantation) remains a challenge, as data are still limited; thus, it seems we need to wait a while longer before a dramatic improvement in SVR rates is achieved for these special groups of patients.
New generation DAAs have better efficacy or non-inferiority, easy once daily dosing, low pill burden, simple regimen, simple stopping rules and pan-genotypic activity. The new drugs are more tolerable with fewer and easy manageable side effects. In particular, sofosbuvir needs shorter treatment duration. However, the IFN-containing DAA regimens may be an intermediate step towards development of strong and “breakthrough” IFN-free regimens. At present, there is increasing interest for IFN-free regimens achieving high SVR rates with short duration of treatment without serious AEs or DDIs.
Biography
University of Athens Medical School, Hippokration General Hospital, Athens, Greece; University of Nicosia Medical School, Nicosia, Cyprus
Footnotes
Conflict of Interest: None
References
- 1.Dienstag JL, McHutchison JG. American Gastroenterological Association technical review on the management of hepatitis C. (214-217).Gastroenterology. 2006;130:231–264. doi: 10.1053/j.gastro.2005.11.010. [DOI] [PubMed] [Google Scholar]
- 2.Brown RS. Hepatitis C and liver transplantation. Nature. 2005;436:973–978. doi: 10.1038/nature04083. [DOI] [PubMed] [Google Scholar]
- 3.European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatitis C virus infection. J Hepatol. 2011;55:245–264. doi: 10.1016/j.jhep.2011.02.023. [DOI] [PubMed] [Google Scholar]
- 4.Ghany MG, Strader DB, Thomas DL, Seeff LB. American Association for the Study of Liver Diseases Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49:1335–1374. doi: 10.1002/hep.22759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jacobson IM. Treatment options for patients with chronic hepatitis C not responding to initial antiviral therapy. Clin Gastroenterol Hepatol. 2009;7:921–930. doi: 10.1016/j.cgh.2009.03.033. [DOI] [PubMed] [Google Scholar]
- 6.Moradpour D, Penin F, Rice CM. Replication of hepatitis C virus. Nat Rev Microbiol. 2007;5:453–463. doi: 10.1038/nrmicro1645. [DOI] [PubMed] [Google Scholar]
- 7.Penin F, Dubuisson J, Rey FA, Moradpour D, Pawlotsky JM. Structural biology of hepatitis C virus. Hepatology. 2004;39:5–19. doi: 10.1002/hep.20032. [DOI] [PubMed] [Google Scholar]
- 8.Jones CT, Murray CL, Eastman DK, Tassello J, Rice CM. Hepatitis C virus p7 and NS2 proteins are essential for production of infectious virus. J Virol. 2007;81:8374–8383. doi: 10.1128/JVI.00690-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Steinmann E, Penin F, Kallis S, Patel AH, Bartenschlager R, Pietschmann T. Hepatitis C virus p7 protein is crucial for assembly and release of infectious virions. PLoS Pathog. 2007;3:e103. doi: 10.1371/journal.ppat.0030103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Appel N, Schaller T, Penin F, Bartenschlager R. From structure to function: new insights into hepatitis C virus RNA replication. J Biol Chem. 2006;281:9833–9836. doi: 10.1074/jbc.R500026200. [DOI] [PubMed] [Google Scholar]
- 11.Ma Y, Yates J, Liang Y, Lemon SM, Yi M. NS3 helicase domains involved in infectious intracellular hepatitis C virus particle assembly. J Virol. 2008;82:7624–7639. doi: 10.1128/JVI.00724-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jones DM, Patel AH, Targett-Adams P, McLauchlan J. The hepatitis C virus NS4B protein can trans-complement viral RNA replication and modulates production of infectious virus. J Virol. 2009;83:2163–2177. doi: 10.1128/JVI.01885-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tellinghuisen TL, Foss KL, Treadaway J. Regulation of hepatitis C virion production via phosphorylation of the NS5A protein. PLoS Pathol. 2008;4:e1000032. doi: 10.1371/journal.ppat.1000032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ghany MG, Nelson DR, Strader DB, Thomas DL, Seeff LB American Association for Study of Liver Diseases. An update on treatment of genotype 1 chronic hepatitis C virus infection:2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology. 2011;54:1433–1444. doi: 10.1002/hep.24641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sarrazin C, Kieffer TL, Bartels D, et al. Dynamic hepatitis C virus genotypic and phenotypic changes in patients treated with the protease inhibitor telaprevir. Gastroenterology. 2007;132:1767–1777. doi: 10.1053/j.gastro.2007.02.037. [DOI] [PubMed] [Google Scholar]
- 16.Susser S, Welsch C, Wang Y, et al. Characterization of resistance to the protease inhibitor boceprevir in hepatitis C virus-infected patients. Hepatology. 2009;50:1709–1718. doi: 10.1002/hep.23192. [DOI] [PubMed] [Google Scholar]
- 17.Halfon P, Locarnini S. Hepatitis C virus resistance to protease inhibitors. J Hepatol. 2011;55:192–206. doi: 10.1016/j.jhep.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 18.Bühler S, Bartenschlager R. New targets for antiviral therapy of chronic hepatitis C. Liver Int. 2012;32(Suppl 1):9–16. doi: 10.1111/j.1478-3231.2011.02701.x. [DOI] [PubMed] [Google Scholar]
- 19.Romano KP, Ali A, Aydin C, et al. The molecular basis of drug resistance against hepatitis C virus NS3/4A protease inhibitors. PLoS Pathog. 2012;8:e1002832. doi: 10.1371/journal.ppat.1002832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Koch U, Narjes F. Recent progress in the development of inhibitors of the hepatitis C virus RNA-dependent RNA polymerase. Curr Top Med Chem. 2007;7:1302–1329. doi: 10.2174/156802607781212211. [DOI] [PubMed] [Google Scholar]
- 21.Kwong AD, McNair L, Jacobson I, George S. Recent progress in the development of selected hepatitis C virus NS3.4A protease and NS5B polymerase inhibitors. Curr Opin Pharmacol. 2008;8:522–531. doi: 10.1016/j.coph.2008.09.007. [DOI] [PubMed] [Google Scholar]
- 22.Gane EJ, Pockros PJ, Zeuzem S, et al. Mericitabine and ritonavir-boosted danoprevir with or without ribavirin in treatment-naive HCV genotype 1 patients: INFORM-SVR study. Liver Int. 2014 doi: 10.1111/liv.12588. doi:10.1111/liv.12588. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 23.Lok AS, Gardiner DF, Lawitz E, et al. Preliminary study of two antiviral agents for hepatitis C genotype 1. N Engl J Med. 2012;366:216–224. doi: 10.1056/NEJMoa1104430. [DOI] [PubMed] [Google Scholar]
- 24.McPhee F, Hernandez D, Yu F, et al. Resistance analysis of hepatitis C virus genotype 1 prior treatment null responders receiving daclatasvir and asunaprevir. Hepatology. 2013;58:902–911. doi: 10.1002/hep.26388. [DOI] [PubMed] [Google Scholar]
- 25.Nakamoto S, Kanda T, Wu S, et al. Hepatitis C virus NS5A inhibitors and drug resistance mutations. World J Gastroenterol. 2014;20:2902–2912. doi: 10.3748/wjg.v20.i11.2902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kosaka K, Imamura M, Hayes CN, et al. Emergence of resistant variants detected by ultra-deep sequencing after asunaprevir and daclatasvir combination therapy in patients infected with hepatitis C virus genotype 1. J Viral Hepat. 2014 doi: 10.1111/jvh.12271. doi:10.1111/jvh.12271. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 27.Schneider MD, Sarrazin C. Antiviral therapy of hepatitis C in 2014:do we need resistance testing? Antiviral Res. 2014;105:64–71. doi: 10.1016/j.antiviral.2014.02.011. [DOI] [PubMed] [Google Scholar]
- 28.Flisiak R, Feinman SV, Jablkowski M, et al. The cyclophilin inhibitor DEBIO-025 combined with PEG IFN-alpha2a significantly reduces viral load in treatment naive hepatitis C patients. Hepatology. 2009;49:1460–1468. doi: 10.1002/hep.22835. [DOI] [PubMed] [Google Scholar]
- 29.Patel H, Heathcote EJ. Sustained virological response with 29 days of DEBIO-025 monotherapy in hepatitis C virus genotype 3. Gut. 2011;60:879. doi: 10.1136/gut.2010.217323. [DOI] [PubMed] [Google Scholar]
- 30.Flisiak R, Pawlotsky JM, Crabbe R, et al. Once-daily alisporivir (DEB025) plus peginterferon alfa-2a/ribavirin results in superior sustained virologic response in chronic hepatitis C genotype 1 treatment-naive patients. J Hepatol. 2011;54(Suppl 1):S2. [Google Scholar]
- 31.Jacobson IM, McHutchison JG, Dusheiko G, et al. ADVANCE Study Team. Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med. 2011;364:2405–2416. doi: 10.1056/NEJMoa1012912. [DOI] [PubMed] [Google Scholar]
- 32.Sherman KE, Flamm SL, Afdhal NH, et al. ILLUMINATE Study Team. Response-guided telaprevir combination treatment for hepatitis C virus infection. N Engl J Med. 2011;365:1014–1024. doi: 10.1056/NEJMoa1014463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Poordad F, McCone J, Jr, Bacon BR SPRINT-2 Investigators. Boceprevir for untreated chronic HCV genotype 1 infection. N Engl J Med. 2011;364:1195–1206. doi: 10.1056/NEJMoa1010494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zeuzem S, Andreone P, Pol S, et al. REALIZE Study Team. Telaprevir for retreatment of HCV infection. N Engl J Med. 2011;364:2417–2428. doi: 10.1056/NEJMoa1013086. [DOI] [PubMed] [Google Scholar]
- 35.Bacon BR, Gordon SC, Lawitz E RESPOND-2 Investigators. Boceprevir for previously treated chronic HCV genotype 1 infection. N Engl J Med. 2011;364:1207–1217. doi: 10.1056/NEJMoa1009482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Vierling JM, Davis M, Flamm S, et al. Boceprevir for chronic HCV genotype 1 infection in patients with prior treatment failure to peginterferon/ribavirin, including prior null response. J Hepatol. 2014;60:748–756. doi: 10.1016/j.jhep.2013.12.013. [DOI] [PubMed] [Google Scholar]
- 37.Buti M, Agarwal K, Horsmans Y, et al. Telaprevir twice daily is noninferior to telaprevir every 8 hours for patients with chronic hepatitis C. Gastroenterology. 2014;146:744–753. doi: 10.1053/j.gastro.2013.11.047. [DOI] [PubMed] [Google Scholar]
- 38.Hézode C, Fontaine H, Dorival C, et al. CUPIC Study Group. Effectiveness of telaprevir or boceprevir in treatment-experienced patients with HCV genotype 1 infection and cirrhosis. Gastroenterology. 2014;147:132–142. doi: 10.1053/j.gastro.2014.03.051. [DOI] [PubMed] [Google Scholar]
- 39.Hézode C, Fontaine H, Dorival C, et al. CUPIC Study Group. Triple therapy in treatment-experienced patients with HCV-cirrhosis in a multicentre cohort of the French Early Access Programme (ANRS CO20-CUPIC) - NCT01514890. J Hepatol. 2013;59:434–441. doi: 10.1016/j.jhep.2013.04.035. [DOI] [PubMed] [Google Scholar]
- 40.Fried MW, Reddy KR, Di Bisceglie AM, et al. HCV-TARGET: A longitudinal, observational study of North American patients with chronic hepatitis C (HCV treated with boceprevir or telaprevir. J Hepatol. 2013;58:S335. [Google Scholar]
- 41.Vierling JM, Zeuzem S, Poordad F, et al. Safety and efficacy of boceprevir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-analysis of 5 trials. J Hepatol. 2014;61:200–209. doi: 10.1016/j.jhep.2014.03.022. [DOI] [PubMed] [Google Scholar]
- 42.Fried MW, Buti M, Dore GJ, et al. Once-daily simeprevir (TMC435) with pegylated interferon and ribavirin in treatment-naïve genotype 1 hepatitis C: the randomized PILLAR study. Hepatology. 2013;58:1918–1929. doi: 10.1002/hep.26641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Zeuzem S, Berg T, Gane E, et al. Simeprevir increases rate of sustained virologic response among treatment-experienced patients with HCV genotype-1 infection: a phase IIb trial. Gastroenterology. 2014;146:430–441. doi: 10.1053/j.gastro.2013.10.058. [DOI] [PubMed] [Google Scholar]
- 44.Forns X, Lawitz E, Zeuzem S, et al. Simeprevir with peginterferon and ribavirin leads to high rates of SVR in patients with HCV genotype 1 Who relapsed after previous therapy: a phase 3 trial. Gastroenterology. 2014;146:1669–1679. doi: 10.1053/j.gastro.2014.02.051. [DOI] [PubMed] [Google Scholar]
- 45.Jacobson IM, Dore GJ, Foster GR, et al. Simeprevir with pegylated interferon alfa 2a plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1infection (QUEST-1):a phase 3, randomised, double-blind, placebo-controlled trial. Lancet. 2014;384:403–413. doi: 10.1016/S0140-6736(14)60494-3. [DOI] [PubMed] [Google Scholar]
- 46.Manns M, Marcellin P, Poordad F, et al. Simeprevir with pegylated interferon alfa 2a or 2b plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1 infection (QUEST-2):a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2014;384:414–426. doi: 10.1016/S0140-6736(14)60538-9. [DOI] [PubMed] [Google Scholar]
- 47.EASL recommendations on treatment of hepatitis C 2014. J Hepatol. 2014;61:373–395. doi: 10.1016/j.jhep.2014.05.001. [DOI] [PubMed] [Google Scholar]
- 48.Kowdley KV, Lawitz E, Crespo I, et al. Sofosbuvir with pegylated interferon alfa-2a and ribavirin for treatment-naïve patients with hepatitis C genotype-1 infection (ATOMIC):an open-label, randomised, multicentre phase 2 trial. Lancet. 2013;381:2100–2107. doi: 10.1016/S0140-6736(13)60247-0. [DOI] [PubMed] [Google Scholar]
- 49.Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med. 2013;368:1878–1887. doi: 10.1056/NEJMoa1214853. [DOI] [PubMed] [Google Scholar]
- 50.Lawitz E, Poordad F, Brainard D, et al. Sofosbuvir in combination with PegIFN and ribavirin for 12 weeks provides wigh SVR rates in HCV-infected genotype 2 or 3 treatment-experienced patients with and without compensated cirrhosis: results from the LONESTAR-2 study. Hepatology. 2013;58:1380A. [Google Scholar]
- 51.Sulkowski MS, Asselah T, Lalezari J, et al. Faldaprevir combined with pegylated interferon alfa-2a and ribavirin in treatment-naïve patients with chronic genotype 1 HCV: SILEN-C1 trial. Hepatology. 2013;57:2143–2154. doi: 10.1002/hep.26276. [DOI] [PubMed] [Google Scholar]
- 52.Dieterich D, Asselah T, Guyader D, et al. SILEN-C3, a Phase 2 Randomized Trial with Faldaprevir plus Pegylated Interferon α-2a and Ribavirin in Treatment-Naive Hepatitis C Virus Genotype 1-Infected Patients. Antimicrob Agents Chemother. 2014;58:3429–3436. doi: 10.1128/AAC.02497-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Sulkowski MS, Bourlière M, Bronowicki JP, et al. Faldaprevir combined with peginterferon alfa-2a and ribavirin in chronic hepatitis C virus genotype-1 patients with prior nonresponse: SILEN-C2 trial. Hepatology. 2013;57:2155–2163. doi: 10.1002/hep.26386. [DOI] [PubMed] [Google Scholar]
- 54.Jensen D, Asselah T, Dieterich DT, et al. A pooled analysis of two randomized double blind placebo-controlled phase III trials (START Verso 1 and 2) of faldaprevir plus pegylated interferon a-2a and ribavirin in treatment naïve patients with chronic hepatitis C genotype 1 infection background. Hepatology. 2013;58:734. [Google Scholar]
- 55.Ferenci P, Asselah T, Foster GR, et al. Faldaprevir plus pegylated interferon a-2a and ribavirin in chronic HCV genotype 1 treatment naïve patients. Final results from STARTVERSO1 a randomized double blind placebo-controlled phase III trial. J Hepatol. 2013;58:S569–S570. [Google Scholar]
- 56.Everson G, Cooper C, Hézode C, et al. DAUPHINE: a randomized phase II study of danoprevir/ritonavir plus peginterferon alpha-2a/ribavirin in HCV genotypes 1 or 4. Liver Int. 2014 doi: 10.1111/liv.12471. doi:10.1111/liv.12471. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 57.Lok AS, Gardiner DF, Hézode C, et al. Randomized trial of daclatasvir and asunaprevir with or without PegIFN/RBV for hepatitis C virus genotype 1 null responders. J Hepatol. 2014;60:490–499. doi: 10.1016/j.jhep.2013.10.019. [DOI] [PubMed] [Google Scholar]
- 58.Nelson DR, Poordad F, Feld JJ, et al. High SVR rates (SVR4) for 12-week total telaprevir combination therapy in IL28B CC treatment-naives and prior relapsers with G1 chronic hepatitis C: CONCISE interim analysis. J Hepatol. 2013;58:S362. [Google Scholar]
- 59.De luca A, Bianco C, Rossetti B. Treatment of HCV infection with the novel NS3/4A protease inhibitors. Curr Opin Pharmacol. 2014;18C:9–17. doi: 10.1016/j.coph.2014.07.016. [DOI] [PubMed] [Google Scholar]
- 60.Fridell RA, Wang C, Sun JH, et al. Genotypic and phenotypic analysis of variants resistant to hepatitis C virus nonstructural protein 5A replication complex inhibitor BMS-790052 in humans. in vitro and in vivo correlations. Hepatology. 2011;54:1924–1935. doi: 10.1002/hep.24594. [DOI] [PubMed] [Google Scholar]
- 61.Manns MP, Gane E, Rodriguez-Torres M, et al. MK-7009 Protocol 007 Study Group. Vaniprevir with pegylated interferon alpha-2a and ribavirin in treatment-naïve patients with chronic hepatitis C: a randomized phase II study. Hepatology. 2012;56:884–893. doi: 10.1002/hep.25743. [DOI] [PubMed] [Google Scholar]
- 62.Lawitz E, Rodriguez-Torres M, Stoehr A, et al. A phase 2B study of MK-7009 (vaniprevir) in patients with genotype 1 HCV infection who have failed previous pegylated interferon and ribavirin treatment. J Hepatol. 2013;59:11–17. doi: 10.1016/j.jhep.2013.02.008. [DOI] [PubMed] [Google Scholar]
- 63.Rodriguez-Torres M, Stoehr A, Gane EJ, et al. Combination of vaniprevir with peginterferon and ribavirin significantly increases the rate of SVR in treatment-experienced patients with chronic HCV genotype 1 infection and cirrhosis. Clin Gastroenterol Hepatol. 2014;12:1029–1037. doi: 10.1016/j.cgh.2013.09.067. [DOI] [PubMed] [Google Scholar]
- 64.Hezode C, Hirschfield GM, Ghesquiere W, et al. Daclatasvir, an NS5A replication complex inhibitor, combined with Peginterferon alfa-2a and ribavirin in treatment naïve HCV genotype 1 and 4 subjects: phase 2b COMMAND 1 SVR12 results. Hepatology. 2012;56:553A–555A. [Google Scholar]
- 65.Dore GJ, Lawitz E, Hezode E, et al. Daclatasvir combined with Peginterferon alfa-2a and ribavirin for 12 or 16 weeks in patients with HCV genotype 2 or 3 infection: COMMAND Gt2/3 study. J Hepatol. 2013;58(Suppl 1):S570–S571. [Google Scholar]
- 66.Izumi N, Yokosuka O, Kawada N, et al. Daclatasvir combined with peginterferon alfa-2a and ribavirin in Japanese patients infected with hepatitis C genotype 1. Antivir Ther. 2014;19:501–510. doi: 10.3851/IMP2731. [DOI] [PubMed] [Google Scholar]
- 67.Suzuki F, Toyota J, Ikeda K, et al. A randomized trial of daclatasvir with peginterferon alfa-2b and ribavirin for HCV genotype 1 infection. Antivir Ther. 2014;19:491–499. doi: 10.3851/IMP2730. [DOI] [PubMed] [Google Scholar]
- 68.Bronowicki JP, Pol S, Thuluvath PJ, et al. Randomized study of asunaprevir plus pegylated interferon-α and ribavirin for previously untreated genotype 1 chronic hepatitis C. Antivir Ther. 2013;18:885–893. doi: 10.3851/IMP2660. [DOI] [PubMed] [Google Scholar]
- 69.Gane EJ, Rouzier R, Wiercinska-Drapalo A, et al. Efficacy and safety of danoprevir-ritonavir plus peginterferon alfa-2a-ribavirin in hepatitis C virus genotype 1 prior null responders. Antimicrob Agents Chemother. 2014;58:1136–1145. doi: 10.1128/AAC.01515-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Marcellin P, Cooper C, Balart L, et al. Randomized controlled trial of danoprevir plus peginterferon alfa-2a and ribavirin in treatment-naïve patients with hepatitis C virus genotype 1 infection. Gastroenterology. 2013;145:790–800. doi: 10.1053/j.gastro.2013.06.051. [DOI] [PubMed] [Google Scholar]
- 71.Manns MP, Vierling JM, Bacon BR, et al. The Combination of MK-5172, peginterferon, and ribavirin is effective in treatment-naive patients with hepatitis C virus genotype 1 infection without cirrhosis. Gastroenterology. 2014;147:366–376.e6. doi: 10.1053/j.gastro.2014.04.006. [DOI] [PubMed] [Google Scholar]
- 72.Pockros PJ, Jensen D, Tsai N, et al. JUMP-C investigators. JUMP-C: a randomized trial of mericitabine plus pegylated interferon alpha-2a/ribavirin for 24 weeks in treatment-naïve HCV genotype 1/4 patients. Hepatology. 2013;58:514–523. doi: 10.1002/hep.26275. [DOI] [PubMed] [Google Scholar]
- 73.Wedemeyer H, Jensen D, Herring R, Jr, et al. PROPEL investigators. PROPEL: a randomized trial of mericitabine plus peginterferon alpha-2a/ribavirin therapy in treatment-naïve HCV genotype 1/4 patients. Hepatology. 2013;58:524–537. doi: 10.1002/hep.26274. [DOI] [PubMed] [Google Scholar]
- 74.Nelson DR, Gane EJ, Jacobson IM, et al. VX-222/telaprevir in combination with peginterferon-alfa-2a and ribavirin in treatment naïve patients treated for 12 weeks. Zenith study. SVR12 interim analysis. Hepatology. 2011;54:S1442. [Google Scholar]
- 75.Feld JJ, Jacobson I, Jensen DM, et al. Up to 100% SVR4 rates with ritonavir-boosted danoprevir mericitabine and ribavirin +/- peginterferon-alfa-2a in HCV genotype 1-infected partial and null responders: results from the NATTERHORN study. Hepatology. 2012;56:S231. [Google Scholar]
- 76.Thompson A, Han S, Shiffman MI, et al. GS-5885 +GS-9451 +peginterferon and ribavirin for 6 or 12 weeks achieves high SVR rates in treatment naïve genotype 1 IL28B CC patients. J Hepatol. 2013;58:S29. [Google Scholar]
- 77.Everson GT, Di Bisceglie AM, Vierling JM, et al. Combination of the NS5A inhibitor, GS-5885, the NS3 protease inhibitor GS-9451 and pegylated interferon plus ribavirin in treatment experienced patients with genotype 1 hepatitis C infection. J Hepatol. 2013;58:S6. [Google Scholar]