

Abstract
Cardiac angiosarcoma is the most common primary cardiac sarcoma in adults. Primary cardiac tumors are rare and have nonspecific clinical presentation, thus making its diagnosis challenging. Clinically, patients present with advanced disease demonstrating metastatic disease at initial presentation itself. It commonly metastasizes to lung, liver, brain, and bone; however metastases to lymph nodes, adrenal glands, spleen and skin has also been seen. We describe a case of right atrial angiosarcoma with extensive visceral metastases involving brain, lungs, liver, pancreas, kidney, and lymph nodes, demonstrated on contrast-enhanced 18F-fluoro-deoxyglucose positron emission tomography-computed tomography (FDG PET-CT). To the best of our knowledge metastases to pancreas and kidney have not been reported so far in the literature. With our report, we emphasize on the initial use of FDG PET-CT in workup of cardiac angiosarcoma for accurate staging and prognostication of this disease.
Keywords: Atrial angiosarcoma, fluoro-deoxyglucose positron emission tomography SUVmax
INTRODUCTION
Angiosarcoma is an uncommon, highly aggressive neoplasm with propensity to metastasize. Primary cardiac angiosarcoma is most common primary cardiac sarcoma in adults accounting for 30–37% of cases.[1,2] Its prevalence in autopsy series is 0.001–0.3%.[1] About 66–89% of patients demonstrate metastases at initial presentation.[2] The prognosis is poor with a median survival of 9–10 months. Early diagnosis is a necessity, as surgical resection remains the mainstay. With widespread metastases, treatment is mainly aimed at palliation. We describe a case of right atrial angiosarcoma with extensive visceral metastases demonstrated on contrast-enhanced fluoro-deoxyglucose positron emission tomography-computed tomography (FDG PET-CT).
CASE REPORT
A 50-year-old female, known case of multinodular goiter, presented with chest discomfort, hemoptysis, and dyspnea to emergency. Electrocardiogram showed left bundle branch block. Hemoglobin was 8.8 g/dl. Chest X-ray showed multiple soft tissue opacities in both lung fields. Two-dimensional transthoracic echocardiography with color Doppler showed a mass of approximately 5.6 cm × 2.2 cm, attached to the right atrium [Figure 1] with mild pericardial effusion and global hypokinesia of left ventricle. The findings on echocardiography were of the opinion for primary cardiac myxoma. High-resolution computed tomography thorax showed multiple discrete soft tissue attenuated nodular lesions in peripheral lung fields with few irregular thick walled cavitatory lesions. The sputum and tuberculosis quantiferon test were negative for acid fast bacilli. Her serum thyroid stimulating hormone was 0.3 mIU/L. Ultrasound (USG) guided fine needle aspiration cytology (FNAC) from solid component of thyroid swelling was suggestive of colloid goiter.
Figure 1.

Transthoracic echocardiography in 4-chamber view showing mass in right atrium (arrows) attached to wall, measuring approximately 5.6 cm × 2.2 cm
The patient was subjected to FDG PET-CT whole body study for work up. PET-CT showed a well-defined heterogeneously enhancing hypodense mass in the right atrium with intense FDG uptake (SUVma × 19.2) along with pericardial infiltration and minimal pericardial effusion [Figure 2]. A non-FDG avid thrombus was seen in right superior pulmonary vein extending up to left atrium [Figure 3]. Multiple FDG avid parenchymal and subpleural nodules were seen in both lungs (SUVma × 3.0–12.5). The mediastinal and right hilar nodes were enlarged with increased FDG uptake (SUVma × 3.3–9.2). Liver showed multiple hypodense lesions in both lobes (SUVma × 4.0–12.2). Hypermetabolic ill-defined hypodense lesions were seen in head, uncinate process and body of pancreas (SUVma × 9.7). A well-defined heterogeneously enhancing lesion was seen in inter-polar region of the right kidney (SUVma × 3.6). Hypermetabolic enlarged peripancreatic (SUVma × 9.5) and aortocaval (SUVma × 10.5) nodes were also seen. A peripherally enhancing hypodense lesion measuring 1.5 cm × 1.4 cm with minimal perilesional edema and no significant FDG uptake was seen in left frontal cortex [Figure 4]. A lobulated mass with solid and cystic areas, calcification, and septations was seen in the right lobe of thyroid with hypermetabolic solid component (SUVma × 14.2) extending up to suprasternal region.
Figure 2.
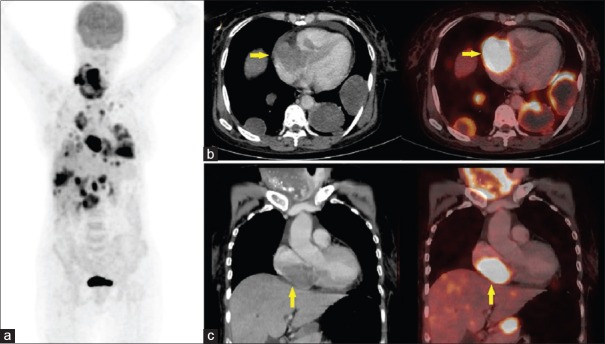
18F-fluoro-deoxyglucose (FDG) contrast enhanced positron emission tomography-computed tomography (PET-CT) images. (a) Whole body maximum intensity projection images showing intense FDG uptake in cardiac mass with multiple FDG avid metastases, (b) transaxial CT and corresponding fused PET-CT, (c) coronal CT and corresponding fused PET-CT sectional images showing very high FDG uptake in a hypodense mass in right atrium (SUVmax 19.2) with associated pericardial infiltration and minimal pericardial effusion
Figure 3.
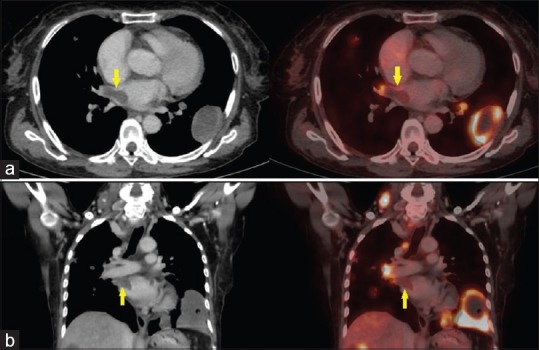
18F-fluoro-deoxyglucose (FDG) contrast enhanced positron emission tomography-computed tomography (PET-CT) images. (a) Transaxial CT and corresponding fused PET-CT, (b) coronal CT and corresponding fused PET-CT sectional images showing non-FDG avid thrombus in right superior pulmonary vein extending upto the left atrium (arrow)
Figure 4.
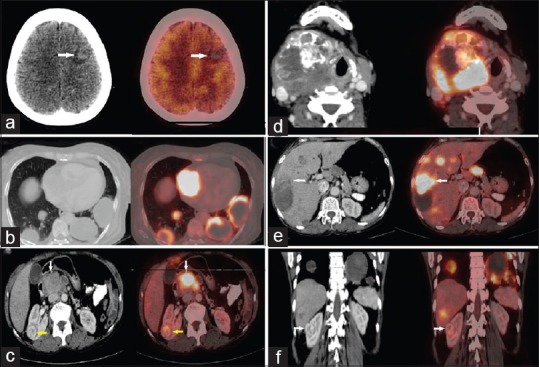
18F-fluoro-deoxyglucose (FDG) contrast enhanced positron emission tomography-computed tomography (PET-CT) images. Transaxial CT and corresponding fused PET-CT sectional images showing (a) non-FDG avid neuroparenchymal metastasis, (b) goiter in neck (c) hypermetabolic pulmonary metastases (d) hypermetabolic hepatic metastases (e) hypermetabolic pancreatic (white arrow) and renal (yellow arrow) metastases (f) Coronal CT and fused PET-CECT sectional images showing renal metastasis (arrow)
The imaging diagnosis was an aggressive right atrial angiosarcoma with neuroparenchymal, pulmonary, hepatic, pancreatic, renal and nodal metastases as the USG guided FNAC of thyroid swelling was suggestive of colloid goiter. After explaining the nature of the disease and poor prognosis, patient did not give consent for biopsy. Palliative chemotherapy with ifosfamide (7500 mg/m2, every 3 weeks) was instituted. Unfortunately, patient passed away after treatment with three cycles of chemotherapy.
DISCUSSION
Primary cardiac malignant tumors include angiosarcomas, leiomyosarcomas, rhabdomyosarcoma, malignant fibrous histiocytomas, undifferentiated sarcomas, fibrosarcomas and malignant lymphomas, of which angiosarcomas are common. 90% of angiosarcomas arise in the right atrium, involving the lateral wall of the right atrium and mostly sparing the septum. Due to this location, diagnosis is often delayed with an average time interval from presentation to the correct diagnosis of 3 years.[3] The right sided cardiac tumors are fast growing tumors and metastasize early in the course of disease. Echocardiography is the first modality of choice. The sensitivity and specificity of transthoracic and transesophageal echocardiography for detection of cardiac masses are 93% and 97% respectively.[4] Cardiac MR with contrast identifies tumors such as pseudotumors, thrombi, lipomas, etc., with high specificity, but it cannot differentiate fibrous tissue from residual disease. However, PET-CT provides the metabolic information to differentiate amidst the two.
Few isolated reports regarding the use of PET-CT in patients with primary cardiac angiosarcomas have described its use in deciding the malignant potential of mass, preoperative staging and metastatic workup, assessment of response to treatment, detection of residual/recurrent disease and in restaging the disease.[5,6,7,8] Rahbar et al.[9] in his analysis of various cardiac tumors proposed that SUV cut off of 3.5 helps in differentiating benign versus malignant tumors with sensitivity of 100%, specificity of 86%, and negative predictive value of 100%. Semi-quantification of FDG uptake thus supports noninvasive, pretreatment differentiation between benign and malignant cardiac tumors. Malignant cardiac tumors exhibit high grade FDG uptake.
Frequent sites of metastases include lung, liver, brain and bone, although metastases to lymph nodes, adrenal glands, spleen and skin have also been reported.[10,11] Ramadhan et al.[12] reported a case of right atrial tumor metastasizing to lung, liver and mandible. Erpolat et al.[13] has reported right atrial angiosarcoma with metastases to jejunum, brain and lung. Hou et al.[5] had shown multiple FDG avid skeletal and pulmonary metastases in a case of right cardiac angiosarcoma. In concordance with the literature, our case also had neuroparenchymal, pulmonary and hepatic metastases. To our surprise, pancreatic and renal metastases were also seen, which have not been reported so far.
This case highlights the role of PET-CT in work up of patient with cardiac angiosarcoma. A very high FDG uptake in a tumor located in the right atrium usually points toward primary malignant tumor. Due to high aggressiveness, they present with advanced disease, as seen in our case. Surgery remains the best option for resectable tumors. Hence, it is of paramount importance to rule out extracardiac sites of metastases. PET-CT permits whole body computed tomographic survey to confirm the diagnosis, detect metastatic spread and has implication in therapeutic management. It can be used to assess response to treatment, detect residual disease and also in restaging of disease.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Burke AP, Virmani R. Primary cardiac sarcomas. In: Rosai J, Sobin LH, editors. Atlas of Tumor Pathology. Tumors of the Heart and Great Vessels. 3rd Series, fascicle 16. Armed Forces Institute of Pathology: Washington DC; 1996. pp. 127–70. [Google Scholar]
- 2.Best AK, Dobson RL, Ahmad AR. Best cases from the AFIP: Cardiac angiosarcoma. Radiographics. 2003;23:S141–5. doi: 10.1148/rg.23si035140. [DOI] [PubMed] [Google Scholar]
- 3.McMannus B. Primary tumors of heart. In: Bonow RO, Mann DL, Zipes DP, Libby P, editors. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 9th ed. Philadelphia: Elseviers Saunders; 2012. pp. 1638–50. [Google Scholar]
- 4.Meng Q, Lai H, Lima J, Tong W, Qian Y, Lai S. Echocardiographic and pathologic characteristics of primary cardiac tumors: A study of 149 cases. Int J Cardiol. 2002;84:69–75. doi: 10.1016/s0167-5273(02)00136-5. [DOI] [PubMed] [Google Scholar]
- 5.Hou CH, Shen DH, Lin LF, Gao HW, Hsu YC, Cheng CY. Aggressive right atrial tumor with extensive FDG-avid metastases in a case of cardiac angiosarcoma. Ann Nucl Med Mol Imaging. 2012;25:201–5. [Google Scholar]
- 6.Bilski M, Kaminski G, Dziuk M. Metabolic activity assessment of cardiac angiosarcoma by 18FDG PET-CT. Nucl Med Rev Cent East Eur. 2012;15:83–4. doi: 10.5603/nmr-18736. [DOI] [PubMed] [Google Scholar]
- 7.Tan H, Jiang L, Gao Y, Zen Z, Shi H. 18F-FDG PET/CT imaging in primary cardiac angiosarcoma: Diagnosis and follow up. Clin Nucl Med. 2013;38:1002–5. doi: 10.1097/RLU.0000000000000254. [DOI] [PubMed] [Google Scholar]
- 8.Manohar K, Kashyap R, Bhattacharya A, Mittal BR. Initial staging and treatment monitoring of right atrial sarcoma with F-18 fluorodeoxyglucose positron emission tomography/computed tomography. Indian J Nucl Med. 2013;28:188–9. doi: 10.4103/0972-3919.119525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rahbar K, Seifarth H, Schäfers M, Stegger L, Hoffmeier A, Spieker T, et al. Differentiation of malignant and benign cardiac tumors using 18F-FDG PET/CT. J Nucl Med. 2012;53:856–63. doi: 10.2967/jnumed.111.095364. [DOI] [PubMed] [Google Scholar]
- 10.Sabolek M, Bachus-Banaschak K, Bachus R, Arnold G, Storch A. Multiple cerebral aneurysms as delayed complication of left cardiac myxoma: A case report and review. Acta Neurol Scand. 2005;111:345–50. doi: 10.1111/j.1600-0404.2005.00413.x. [DOI] [PubMed] [Google Scholar]
- 11.Pomper GJ, Gianani R, Johnston RJ, Rizeq MN. Cardiac angiosarcoma: An unusual presentation with cutaneous metastases. Arch Pathol Lab Med. 1998;122:273–6. [PubMed] [Google Scholar]
- 12.Ramadhan A, Willen H, Thor A. Angiosarcoma of the mandible: Metastasis from a primary tumor of the right atrium of the heart. Case Rep Clin Med. 2013;2:53–7. [Google Scholar]
- 13.Erpolat OP, Icli F, Dogan OV, Gokaslan G, Akmansu M, Erekul S, et al. Primary cardiac angiosarcoma: A case report. Tumori. 2008;94:892–7. doi: 10.1177/030089160809400624. [DOI] [PubMed] [Google Scholar]