

Abstract
Enteric duplication cysts (EDCs) are uncommon congenital anomalies, which can occur anywhere along the gastrointestinal tract and vary greatly in presentation, size, location and symptoms. Ectopic gastric mucosa is reported to be found in 20-30% of these duplications. 99mTc-pertechnetate scintigraphy is a useful modality for preoperative localization of the ectopic functioning gastric mucosa in the EDCs. We report a case where 99mTc-pertechnetate scintigraphy was useful in detecting synchronous thoracic and abdominal duplication cysts with functioning gastric mucosa thus having an impact on the patient management.
Keywords: Duplication cyst, enteric, 99mTc-pertechnetate, ectopic gastric mucosa
INTRODUCTION
Enteric duplication cysts (EDCs) are uncommon congenital anomalies of unknown etiology.[1,2] The presentation of duplication cysts depends on their location, size and other factors such as the presence of the gastric mucosa.[3,4] Ectopic gastric mucosa is reported to be found in 20-30% of these duplications.[1,4,5] The ileum is the most common site for duplication of the alimentary tract whereas rectal, duodenal, gastric and thoraco-abdominal locations are extremely rare.[3] Synchronous multiple duplications are found in up to 15% of the cases.[3,4] 99mTc-pertechnetate scintigraphy helps in preoperative localization of the ectopic functioning gastric mucosa (EFGM) present in these cysts.[6]
CASE REPORT
We report a case of a 4-month-old male child, born at full term by lower segment caesarean section, weighing 3.6 kg, without any history of adverse antenatal or perinatal events. The child was apparently normal until 6 weeks of age when he developed cough (wet type, no postural or diurnal variation, no aggravating or relieving factors). There was no history of fever, fast breathing or chest retraction. He had a single episode of blood-tinged sputum. On general physical examination, the child was anemic (hemoglobin – 5.5 g/dl) requiring one unit of blood transfusion. Bilateral crepitations were heard on chest auscultation. Blood and sputum cultures were negative. Chest X-ray was suggestive of right sided pneumonia. Ultrasound thorax showed a collection along the right posterior chest. The child was started on intravenous antibiotics but showed no improvement. Later on, the child developed abdominal distension, which was insidious in onset and progressive. Shifting dullness was elicited on per abdomen examination. Ultrasound abdomen revealed mild ascites and diffuse wall thickening of the small bowel. Contrast-enhanced computed tomography (CECT) chest showed a cystic lesion in the right lung lower lobe [Figure 1a]. CECT abdomen revealed multiple cystic lesions in the small intestine [Figure 1b]. The child was then referred to our department for 99mTc-pertechnetate study in order to rule out intestinal duplication cysts with EFGM. 99mTc-pertechnetate study was performed, dynamic and serial delayed static images were acquired. In the dynamic images an area of increased radiotracer activity was seen in the right lower abdomen, which appeared earlier than the stomach activity and increased progressively with time (along with the stomach activity). An additional area of radiotracer activity was noticed in the right lung lower lobe region after appearance of the stomach activity which became more apparent in the delayed 24 h images [Figure 2]. Thus, 99mTc-pertechnetate study was consistent with EFGM in synchronous abdominal and thoracic duplication cysts. The child was taken up for surgery. Right posterolateral thoracotomy and exploratory laparotomy were performed in the same setting to remove the thoracic and multiple ileal cysts. Single well-defined thoracic cyst (4 × 3 cm) was excised from the right posterolateral hemithorax. Three duplication cysts of the ileum; proximal (2 × 2 cm, blind end), middle (6 × 2 cm, blind end), and distal (6 × 2 cm, exiting into mesenteric border) were excised during the exploratory laparotomy. The histopathology report confirmed the presence of the gastric mucosa in these duplication cysts [Figure 3].
Figure 1.
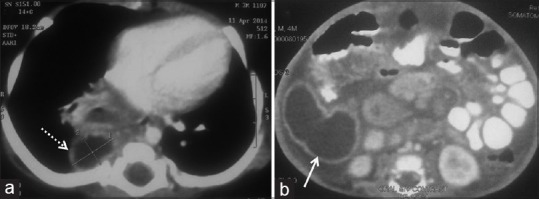
Contrast enhanced computed tomography (CECT) chest showing a well-defined cystic lesion measuring 4 × 3 cm in the right lung lower lobe with a thin wall that shows enhancement after intravenous contrast (a; dotted arrow). CECT abdomen showing cystic lesion measuring 6 × 2 cm in the ileum with a well-defined wall that also shows enhancement after intravenous contrast (b; arrow)
Figure 2.

Early static images (a, anterior; b, posterior; c, right lateral; d, left lateral) and delayed static images at 24 h (e, anterior; f, posterior) show intense area of radiotracer activity (greater than equal in intensity to the stomach activity) in the region of the distal small intestine predominantly right side (arrows). Also noted faint focus of radiotracer uptake in the right lower thoracic region, paravertebral in location that is more obvious in the early posterior and lateral views (b, c, d; dotted arrows) as well as in the delayed 24 h images (e, f; dotted arrows)
Figure 3.
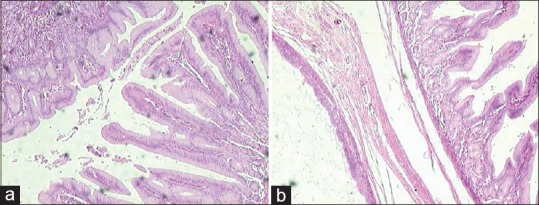
Cyst bound by a layer of smooth muscle and fibroconnective tissue and lined by pseudostratified ciliated columnar epithelium (respiratory; left side) along with the glandular epithelium comprising of foveolae (pits) and gastric glands (gastric mucosa; right side) (a; H and E stain, ×40). Areas from the cyst showing well developed gastric mucosa (b; H and E stain, ×40)
DISCUSSION
Gastrointestinal duplications are found in 1 of every 4500 autopsies.[7] Thoracic and thoraco-abdominal duplications makeup 24% of all the gastrointestinal duplications.[1] Thoracic duplication cyst presents with respiratory distress in younger patients, whereas older patients may report heartburn and malena probably because of the gastric mucosa. Peptic ulceration of these cysts with erosion into the adjacent lung, bronchus and esophagus can cause hemorrhage.[8] Small intestinal duplication cyst usually presents with abdominal distension, vomiting, bleeding, and palpable abdominal mass. Complications like perforation, intussusception, bowel obstruction and volvulus can be associated with these cysts. 99mTc-pertechnetate is a useful modality in the preoperative localization of EDC with EFGM with a sensitivity approaching 75%.[4,9,10] Functional gastric ectopic tissue is visualized simultaneously with the stomach activity in gastric duplication while in intestinal duplication tracer activity can be visualized in the dynamic sequence or even before the appearance of the stomach activity.[5] Delayed imaging acquisitions (6 h and 24 h) are found to be useful when the initial images are equivocal or negative in suspected intrathoracic duplication cyst.[5] Additional lateral and oblique views are also recommended in suspected equivocal cases. In the present case, delayed imaging, and additional lateral views were helpful in correctly detecting the multiple duplication cysts present at different locations in the same patient.
The present case highlights the importance of 99mTc-pertechnetate scintigraphy in correctly detecting and localizing multiple synchronous EDCs with EFGM in the same patient. This guided the treating surgeons to excise all the cysts in the same setting thus having a significant impact on the clinical management. It also emphasizes the importance of imaging protocols for localizing EFGM in EDC.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Gross RE, Holcomb GW, Jr, Farber S. Duplications of the alimentary tract. Pediatrics. 1952;9:448–68. [PubMed] [Google Scholar]
- 2.Bower RJ, Sieber WK, Kiesewetter WB. Alimentary tract duplications in children. Ann Surg. 1978;188:669–74. doi: 10.1097/00000658-197811000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kiratli PO, Aksoy T, Bozkurt MF, Orhan D. Detection of ectopic gastric mucosa using 99mTc pertechnetate: Review of the literature. Ann Nucl Med. 2009;23:97–105. doi: 10.1007/s12149-008-0204-6. [DOI] [PubMed] [Google Scholar]
- 4.Kumar R, Tripathi M, Chandrashekar N, Agarwala S, Kumar A, Dasan JB, et al. Diagnosis of ectopic gastric mucosa using 99Tcm-pertechnetate: Spectrum of scintigraphic findings. Br J Radiol. 2005;78:714–20. doi: 10.1259/bjr/16678420. [DOI] [PubMed] [Google Scholar]
- 5.Bhattacharya A, Samujh R, Rao KL, Mittal BR. Long segment jejuno-ileal duplication cyst with ectopic gastric mucosa detected on 99mTc-pertechnetate scintigraphy. Indian J Nucl Med. 2013;28:96–8. doi: 10.4103/0972-3919.118260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rose JS, Gribetz D, Krasna IH. Ileal duplication cyst: The importance of sodium pertechnetate Tc 99m scanning. Pediatr Radiol. 1978;6:244–6. doi: 10.1007/BF00975547. [DOI] [PubMed] [Google Scholar]
- 7.Amoury RA, Snyder CL. Meckels diverticulum. In: O’Neill JA Jr, Rowe MI, Grtosfeld JL, Fonkalsrud EW, Coran AD, editors. Pediatric Surgery. 5th ed. St. Louis: Mosby; 1998. pp. 1173–84. [Google Scholar]
- 8.Superina RA, Ein SH, Humphreys RP. Cystic duplications of the esophagus and neurenteric cysts. J Pediatr Surg. 1984;19:527–30. doi: 10.1016/s0022-3468(84)80096-2. [DOI] [PubMed] [Google Scholar]
- 9.Lecouffe P, Spyckerelle C, Venel H, Meuriot S, Marchandise X. Use of pertechnetate 99mTc for abdominal scanning in localising an ileal duplication cyst: Case report and review of the literature. Eur J Nucl Med. 1992;19:65–7. doi: 10.1007/BF00178310. [DOI] [PubMed] [Google Scholar]
- 10.Yang JG, Ma DQ, Hao RR, Li CL, Zou LF. Detection of double cystic intestinal duplication by Meckel's scan. Clin Nucl Med. 2009;34:105–6. doi: 10.1097/RLU.0b013e318192c45c. [DOI] [PubMed] [Google Scholar]