

Abstract
Gliomatosis cerebri (GC) is a rare condition in which an infiltrative glial neoplasm spreads through the brain with preservation of the underlying structure. F-18 fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) has an important role in demonstrating the appropriate metabolism and differentiating pathologies mimicking GC on CT and magnetic resonance imaging. We describe imaging findings of FDG PET/CT in GC in a 9-year-old male child mimicking encephalitis.
Keywords: Biopsy, encephalitis, F-18 fluorodeoxyglucose-positron emission tomography/computed tomography, gliomatosis cerebri
A 9-year-old male child presented with high-grade fever, followed by partial seizures and low mood. Initial magnetic resonance imaging (MRI) showed features suggestive of encephalitis, and he was treated with anti-epileptics. He further presented with multiple seizure episodes and repeat MRI showed white matter hyperintensities in bilateral temporal lobes and insular cortex with features suggestive of gliomatosis cerebri (GC) [Figure 1a]. Brain fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) images showed hypometabolism of bilateral temporal lobes (right > left) [Figure 1b and c]. Biopsy was taken from right presylvian fissure through temporal craniotomy. Histopathological evaluation showed GC (World Health Organization [WHO] grade III). Patient underwent radiotherapy to the whole brain. However, the patient's clinical status declined rapidly and died before further follow-up.
Figure 1.
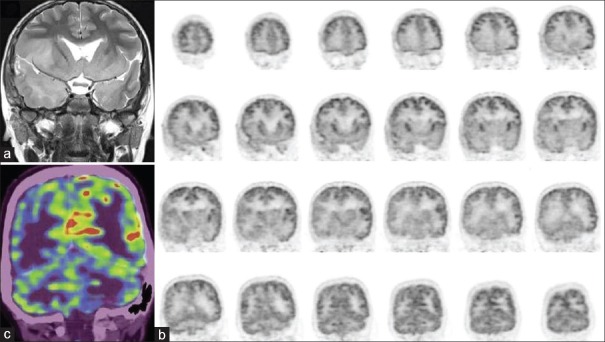
(a) Magnetic resonance imaging of the brain showing hyperintensity in bilateral temporal lobes and insular cortex. Coronal positron emission tomography (PET) images (b) and fused coronal PET/computed tomography (c) Hypometabolism of bilateral temporal lobes (right > left)
Gliomatosis cerebri is a rare primary diffuse brain tumor first described by Nevin in 1938.[1] According to the WHO classification, GC is recognized as a specific entity among neuroepithelial tumors of uncertain origin.[2] The presenting symptoms of GC in the literature are nonspecific. CT also often does not demonstrate specific morphologic changes in this condition and demyelinating conditions often cause confusion. MRI is superior to CT in the diagnosis showing the extent of disease, and CT has low sensitivity and specificity in the diagnosis.[3] MRI studies indicate a diffuse infiltrative process, high signal particularly on T2-weighted images, and the diagnosis is made by a stereotactic or open biopsy.[4,5]
F-18 FDG PET/CT has an important role in demonstrating the appropriate biopsy areas and differentiating pathologies mimicking GC on CT and MRI.
Dexter et al. described a case of GC showing marked reduction in FDG uptake in the right temporal and both frontal lobes, relative glucose hypometabolism in right thalamus and striatum when compared with the left and focal areas of increased FDG uptake were not seen in the white matter.[6] C-11 methionine and C-11 choine with PET/CT also has been utilized with this condition.[7] However, the findings with this radiotracer are nonspecific and benign conditions cannot be differentiated from malignant conditions as increased uptake can be present in both high and low-grade gliomas. Shintani et al.[8] presented a case report of PET changes in a patient with GC treated with radiation. C-11 methionine PET images showed hypermetabolism, whereas O-15 water PET images showed a marked increase in cerebral blood flow in GC lesions. However, the PET images revealed marked improvement 6 months subsequent to radiotherapy. Our case report demonstrated hypometabolism in temporal lobes and was helpful in the diagnosis and guiding therapy. There is currently no effective treatment for GC. Surgical treatment of GC is limited due to the extensive diffuse infiltrative process; therefore, treatment generally comprises anticonvulsants and steroids. The literature contains several anecdotal reports of radiation therapy.[9] Despite treatment, the prognosis is poor.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Nevin S. Gliomatosis cerebri. Brain. 1938;61:170–91. [Google Scholar]
- 2.Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007;114:97–109. doi: 10.1007/s00401-007-0243-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rippe DJ, Boyko OB, Fuller GN, Friedman HS, Oakes WJ, Schold SC. Gadopentetate-dimeglumine-enhanced MR imaging of gliomatosis cerebri: Appearance mimicking leptomeningeal tumor dissemination. AJNR Am J Neuroradiol. 1990;11:800–1. [PMC free article] [PubMed] [Google Scholar]
- 4.Felsberg GJ, Silver SA, Brown MT, Tien RD. Radiologic-pathologic correlation. Gliomatosis cerebri. AJNR Am J Neuroradiol. 1994;15:1745–53. [PMC free article] [PubMed] [Google Scholar]
- 5.Artigas J, Cervos-Navarro J, Iglesias JR, Ebhardt G. Gliomatosis cerebri: Clinical and histological findings. Clin Neuropathol. 1985;4:135–48. [PubMed] [Google Scholar]
- 6.Dexter MA, Parker GD, Besser M, Ell J, Fulham MJ. MR and positron emission tomography with fludeoxyglucose F 18 in gliomatosis cerebri. AJNR Am J Neuroradiol. 1995;16:1507–10. [PMC free article] [PubMed] [Google Scholar]
- 7.Cai L, Gao S, Li Y, Lu D. 11C-Methionine or 11C-Choline PET is superior to MRI in the evaluation of gliomatosis cerebri. Clin Nucl Med. 2011;36:127–9. doi: 10.1097/RLU.0b013e318203bc08. [DOI] [PubMed] [Google Scholar]
- 8.Shintani S, Tsuruoka S, Shiigai T. Serial positron emission tomography (PET) in gliomatosis cerebri treated with radiotherapy: A case report. J Neurol Sci. 2000;173:25–31. doi: 10.1016/s0022-510x(99)00296-8. [DOI] [PubMed] [Google Scholar]
- 9.Horst E, Micke O, Romppainen ML, Pyhtinen J, Paulus W, Schäfer U, et al. Radiation therapy approach in gliomatosis cerebri – case reports and literature review. Acta Oncol. 2000;39:747–51. doi: 10.1080/028418600750063839. [DOI] [PubMed] [Google Scholar]