

Abstract
We report the case of a young woman presenting with recurrent urticaria. The episodes occurred both in and out of the workplace. On three occasions it presented as urticaria-angioedema, requiring emergency care on one occassion. A thorough clinical history along with serological and allergological tests allowed a diagnosis of caffeine-induced urticaria-angioedema. We advised the patient to follow a caffeine-free diet and to avoid all caffeine or methylxanthine-containing drugs. After two years of caffeine abstinence, she had not experienced any further episodes of urticaria-angioedema. Only a few cases of caffeine-induced urticaria and/or anaphylaxis have been reported till date, with varying outcomes in allergologic investigations. Moreover, several cases are probably undiagnosed or misdiagnosed as idiopathic urticaria or as occupational allergy. We speculate that hypersensitivity to caffeine rather than autoimmine reaction may be the probable cause of urticaria. Caffeine should considered as a potential urticaria-inducing agent and should be included in the allergological test series.
Keywords: Angioedema, caffeine hypersensitivity, urticarial
INTRODUCTION
Coffee, tea, chocolate, and cola drinks are consumed by millions of people every day. All these beverages and foods contain caffeine, a methylxanthine closely-related to theophylline and theobromine, that are popular natural stimulants. Caffeine acts on the central nervous system (temporarily warding off drowsiness and restoring alertness), kidneys (promoting urine formation), lungs (favoring bronchodilation) and muscles. Moreover, caffeine has a mild transitory, concentration-dependent, vasoconstrictor effect, whereas the main effect is vasodilating. Caffeine's maximum blood concentration is reached within 30-45 min of ingestion, being reduced to half within 4-6 h. One cup of 100 ml of coffee (or cappuccino) has around 90-120 mg of caffeine, whereas a cup of black tea or a cola beverage have has just 70 mg and 23 mg, respectively. Moreover, the amount of caffeine is usually greater in brewed coffee (between 80 and 100 mg/cup) than in instant coffee (60-80 mg/cup) and in espresso (40-80 mg/cup).[1,2]
CASE REPORT
We present the case of a 24-year-old woman who suffered from 2006 to 2011 from recurrent urticaria (i.e., six episodes), occurring while she was working as an employee in the cheese-and-gastronomy section of a supermarket. From 2009, the reactions grew in frequency and intensity, presenting with wheals localized on the lips, neck, groin, hands and foots, itching of the eyelids, ears, and tongue. During this time, the patient received a diagnosis of occupational allergy. Consequently, she moved to another section of the supermarket, where she has no more in contact with foods. In 2010, she developed three urticarial reactions at the workplace - in one case, edema of the glottis, diarrhea and loss of consciousness occurred, requiring emergency resuscitation. On this occasion, the patient presented with leukocytosis (14.4 × 103/uL) and increased neutrophils (86%). First aid included corticosteroids, adrenaline, and intravenous antihistamines administration. Later, she was referred to our department.
A thorough anamnesis revealed that, before symptoms development in the workplace, she had drunk a cup of coffee (nearly 80 ml). Prior to the three reactions that occurred at the workplace, on two occasions she recollected drinking a cup of brewed coffee; before the third episode, she had drunk a cup of brewed cappuccino (nearly 100 ml) during breakfast.
We analyzed the composition of the instant coffee that the patient used to take from the automatic dispenser at the workplace. The composition was the following: Coffee component (90%), artificial sweeteners (aspartame) (5%), flavoring component (vanilla, amaretto) (3%), aroma enhancers (spices) (2%). There was neither personal nor familiar history of atopy or allergies. Total IgE paper radio immunosorbent test (PRIST) was normal (28 kU/L) and specific IgE radio allergosorbent tests (RAST) for coffee, caffeine, cow-milk, lactoglobulin and caseine-specific IgE (CAP system) were negative. Tests for C1q inhibitor, C4, circulating immunocomplexes, antinuclear antibodies and extractable nuclear antigen autoantibodies, blood protein, hemochrome, C-reactive protein and erythrocyte sedimentation rate were normal. Both prick test (PT) with common allergens and caffeine (10 mg/mL) and prick-by-prick tests (PBP) with espresso coffee, decaffeinate coffee and cappuccino, tested negative. Five control subjects underwent PT with caffeine and PBP with coffee, with negative results. Open scratch test (OST) was performed with the molds of the cheese and of the ham, starch salami and baked bread that the patient used to handle during her work: They all tested negative. A double blind placebo-controlled oral challenge test (OCT) with 50 mg of caffeine elicited, after 1-2 min, urticarial lesions on the lips, neck, trunk, hands and feet, followed by dyspnea and voice change [Figure 1]. The patient was treated with intravenous infusions of epinephrine, corticosteroids and antihistamines (ranitidine and chlorpheniramine) and monitored (electrocardiography, blood pressure and diuresis) for 48 h. Symptoms resolved within 2 hours. OCT performed after 4 weeks with 50 mg of theophylline was positive after 9 hours, with appearance of wheals on the neck and upper trunk.
Figure 1.
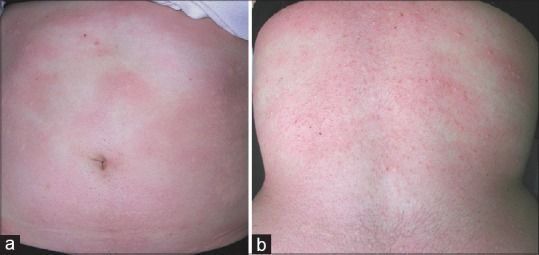
Urticarial lesions on the abdomen (a) and the back (b) of the patient, developed few minutes after caffeine oral challenge test
We concluded that caffeine was the cause of our patient's symptoms, and we advised her to follow a caffeine-free diet, avoiding all caffeine-containing beverages and drugs or methylxanthine-containing drugs (e.g., theophylline, aminophylline, paraxanthine, theobromine), in order to prevent possible cross-reactions. Periodic follow-ups were conducted at 1, 3 and 6 months, and then once a year from 2010 to 2012: The patient never experienced urticaria or angioedema again.
DISCUSSION
Despite its high consumption, only few cases (to our knowledge, seven) of urticaria-anaphylaxis from caffeine have been reported till date.[3,4,5,6,7,8,9] Five patients experienced urticaria[3,4,5,6,7] and two patients anaphylaxis,[8,9] with different outcomes in allergologic investigations. PT with caffeine tested positive in four cases[3,5,8,9] and negative in three.[4,6,7] OCT was positive with caffeine 50 mg,[7] 150 mg[6] or 160 mg,[5] but negative with theophylline.[5] Hence, caffeine-induced urticaria can be classified as allergic and not-allergic: The first type include those cases with an underlying IgE-mediated mechanism, (with specific IgE determination in skin or blood tests)[3,5,8,9] while hypersensitivity reaction seems to occur in the other cases.[6,7] In most of reported cases, the urticarial reaction is dose-dependent.[6,7,9]
According to the allergologic investigations’ results (i.e., PRIST, RAST, PT, PBP and OST), we have no evidence to implicate an IgE-mediated mechanism as being responsible for our patients’ symptoms. Hence, we hypothesized that an hypersensitivity reaction to caffeine may be the cause of our patient's symptoms.[6,7] Unlike some authors,[6,7,9] we have not assessed whether the symptoms were dose-dependent or not because our patient developed urticarial lesion with the first caffeine-dose during OCT. The slow reaction to theophylline that we have observed after performing OCT could be explained by two factors: First, a personal susceptibility to theophylline and to other methylxantines; second, a common hypersensitivity pathway involving both theophylline and caffeine molecules. However, further investigations are needed to assess the exact pathogenesis of caffeine-induced urticaria. Nowadays, this remains a diagnosis of exclusion and numerous cases are probably undiagnosed or misdiagnosed as idiopathic urticaria or as occupational allergy. Therefore, caffeine should be considered a potential urticaria-inducing agent.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Echeverri D, Montes FR, Cabrera M, Galán A, Prieto A. Caffeine's vascular mechanisms of action. Int J Vasc Med. 2010;2010:834060. doi: 10.1155/2010/834060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mandel HG. Update on caffeine consumption, disposition and action. Food Chem Toxicol. 2002;40:1231–4. doi: 10.1016/s0278-6915(02)00093-5. [DOI] [PubMed] [Google Scholar]
- 3.Pola J, Subiza J, Armentia A, Zapata C, Hinojosa M, Losada E, et al. Urticaria caused by caffeine. Ann Allergy. 1988;60:207–8. [PubMed] [Google Scholar]
- 4.Quirce Gancedo S, Freire P, Fernández Rivas M, Dávila I, Losada E. Urticaria from caffeine. J Allergy Clin Immunol. 1991;88:680–1. doi: 10.1016/0091-6749(91)90163-i. [DOI] [PubMed] [Google Scholar]
- 5.Caballero T, García-Ara C, Pascual C, Diaz-Pena JM, Ojeda A. Urticaria induced by caffeine. J Investig Allergol Clin Immunol. 1993;3:160–2. [PubMed] [Google Scholar]
- 6.Hinrichs R, Hunzelmann N, Ritzkowsky A, Zollner TM, Krieg T, Scharffetter-Kochanek K. Caffeine hypersensitivity. Allergy. 2002;57:859–60. doi: 10.1034/j.1398-9995.2002.23575_2.x. [DOI] [PubMed] [Google Scholar]
- 7.Fernández-Nieto M, Sastre J, Quirce S. Urticaria caused by cola drink. Allergy. 2002;57:967–8. doi: 10.1034/j.1398-9995.2002.23832_13.x. [DOI] [PubMed] [Google Scholar]
- 8.Przybilla B, Ring J, Burg G. Anaphylaxis following ingestion of coffee, chronic urticaria and analgesics idiosyncrasy. Hautarzt. 1983;34:73–6. [PubMed] [Google Scholar]
- 9.Infante S, Baeza ML, Calvo M, De Barrio M, Rubio M, Herrero T. Anaphylaxis due to caffeine. Allergy. 2003;58:681–2. doi: 10.1034/j.1398-9995.57.s73.24_53.x. [DOI] [PubMed] [Google Scholar]