

A 28-year-old female, apparently healthy and thinly built, presented with mildly itchy hyperpigmented hyperkeratotic plaques on her feet since three years. There were no systemic features suggestive of diabetes or other endocrinopathies associated with acanthosis nigricans (AN). She was not on any medication prior to onset of lesions. On examination, multiple well-defined hyperpigmented, hyperkeratotic plaques were present on the dorsum of several toes in a bilateral symmetrical manner [Figure 1]. Other skin sites, the scalp, palms, soles and mucosae were spared. Routine blood investigations, fasting and postprandial blood sugar and routine urine analysis were within normal limits. The liver enzymes, thyroid hormones and growth hormone were within normal range. Serum leptin and insulin level estimation could not be done as these were not available in our institute. Radiographic examination of the chest, skull and hands did not reveal any abnormality. Abdominal and pelvic ultrasonography was non-contributory. Biopsy of the skin showed hyperkeratosis, papillomatosis, increased pigmentation of the basal cell layer and mild acanthosis, with a sparse inflammatory infiltrate of mononuclear cells in the upper dermis [Figure 2a and b]. These histopathological findings were consistent with the diagnosis of AN. A final diagnosis of acral AN was made, considering clinical and histopathological findings.
Figure 1.

Hyperpigmented hyperkeratotic plaques on dorsal surface of toes
Figure 2.
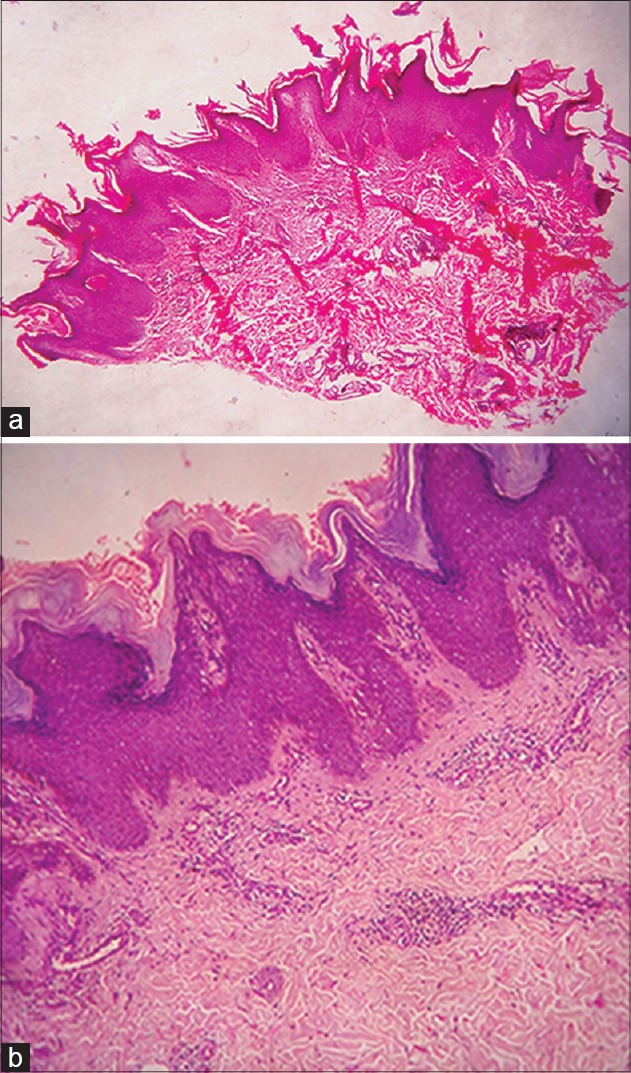
(a) Hyperkeratosis, acanthosis, papillomatosis and sparse mononuclear cell infiltration in dermis (H and E, ×40) (b) Higher magnification (H and E, ×100)
AN is a common presentation in the out-patient department and usually affects the neck, axillae, groin, inner aspects of the thighs, flexor and extensor surface of the elbows and knees, dorsal joints of the hands, umbilicus and anus. Schwartz has categorized the entity into the following eight types: benign, malignant, associated with obesity, syndromic, unilateral, drug induced, mixed and acral.[1] In acral AN, also called as acral acanthotic anomaly, the lesions are localized to the knee, ankle, phalangeal joints and tarsophalangeal joints.[1] It is apparently more common in persons with a dark complexion and affects acral areas without prominent affection of axilla and other flexures.[2] The clinical significance of acral AN is ambiguous and more studies are needed to settle this issue. According to Schwartz, this type of AN essentially occurs in healthy black people and does not, on its own, call for a vigilant work-up of those afflicted; for the possible presence of an internal malignancy. However, recently it has been reported in association with dermatofibrosarcoma protuberans, non-Hodgkin's lymphoma[3] and gastric adenocarcinoma.[4]
Diagnosis is mostly clinical and can be confirmed by histopathology. In the majority of cases, improvement of the skin lesions is the primary concern of patients presenting to dermatologists. Treatment of its underlying condition often results in improvement of AN. The type occurring with obesity usually improves with weight loss. Etretinate, metformin, tretinoin, calcipotriol, urea, salicyclic acid, CO2 laser ablation and long pulsed alexandrite laser therapy have been reported as successful treatments in individual cases.[1,2]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Schwartz RA. Acanthosis nigricans. J Am Acad Dermatol. 1994;31:1–19;20. doi: 10.1016/s0190-9622(94)70128-8. [DOI] [PubMed] [Google Scholar]
- 2.Schwartz RA. Acral acanthotic anomaly (AAA) J Am Acad Dermatol. 1981;5:345–6. doi: 10.1016/s0190-9622(81)80155-7. [DOI] [PubMed] [Google Scholar]
- 3.Song JY, Lim JH, Kim CW, Kim HO. A case of acral type acanthosis nigricans associated with lymphoma. Korean J Dermatol. 2002;40:841–3. [Google Scholar]
- 4.Lee SS, Jung NJ, Im M, Lee Y, Seo YJ, Lee JH. Acral-type Malignant Acanthosis Nigricans associated with gastric adenocarcinoma. Ann Dermatol. 2011;23:S208–10. doi: 10.5021/ad.2011.23.S2.S208. [DOI] [PMC free article] [PubMed] [Google Scholar]