

Abstract
Introduction: To study the effects of Polarized Polychromatic Noncoherent Light (Bioptron) therapy on patients with carpal tunnel syndrome (CTS).
Methods: This study was designed as a randomized clinical trial. Forty four patients with mild or moderate CTS (confirmed by clinical and electrodiagnostic studies) were assigned randomly into two groups (intervention and control goups). At the beginning of the study, both groups received wrist splinting for 8 weeks. Bioptron light was applied for the intervention group (eight sessions, for 3/weeks). Bioptron was applied perpendicularly to the wrist from a 10 centimeter sdistance. Pain severity and electrodiagnostic measurements were compared from before to 8 weeks after initiating each treatment.
Results: Eight weeks after starting the treatments, the mean of pain severity based on Visual Analogue Scale (VAS) scores decreased significantly in both groups. Median Sensory Nerve Action Potential (SNAP) latency decreased significantly in both groups. However, other electrophysiological findings (median Compound Motor Action Potential (CMAP) latency and amplitude, also SNAP amplitude) did not change after the therapy in both groups. There was no meaningful difference between two groups regarding the changes in the pain severity.
Conclusion: Bioptron with the above mentioned parameters led to therapeutic effects equal to splinting alone in patients with carpal tunnel syndrome. However, applying Bioptron with different therapeutic protocols and light parameters other than used in this study, perhaps longer duration of therapy and long term assessment may reveal different results favoring Bioptron therapy.
Keywords: syndrome, carpal tunnel, noncoherent light, electrodiagnostic study
Introduction
The carpal tunnel syndrome (CTS), caused by compression of the median nerve at the wrist, is considered as the most common entrapment neuropathy 1-3 . According to different studies, the prevalence of this disease is about 2.7% based on clinical and electrodiagnostic findings 2, 3. Patients complain of paresthesia (with or without numbness or pain) involving the fingers innervated by the median nerve, and a weakness of thumb abduction mostly in severe cases. Carpal Tunnel Syndrome not only causes discomfort for the patient, but can also interfere with social and occupational activities as well as activities of daily living 3. Therefore, assessment of preventive and therapeutic strategies in this field is becoming increasingly a matter of interest for physicians and therapists 3, 4. Electrodiagnostic studies are the best diagnostic tool to both diagnose and determine the severity of the disease with 85-90% sensitivity and 85 % specificity for diagnosing CTS 2.
There are several treatments recommended for this disease 1-5. Currently, wrist splinting, local corticosteroid injection and surgical decompression are considered the standard treatments for the CTS 1-4.
Recently, light therapy including low level laser as a coherent source of light and Polarized Polychromatic Noncoherent Light (Bioptron) therapy as a polychromatic and non-coherent light have been proposed as a nonaggressive therapeutic option for the treatment of several musculoskeletal disorders including CTS 5, 6.
The Bioptron Light Therapy System is a device with an optical unit emitting light that is similar to a part of the electromagnetic spectrum produced by the sun but with no UV radiation 6, 7 . The light emitted by Bioptron light therapy system can be characterized as polarized (its waves oscillate on parallel planes), polychromatic (wavelength: 480-3400 nm), incoherent (out of phase light, unlike laser light) and low energy light 7.
Bioptron Light has so-called bio-stimulative effects: When applied to the skin, it stimulates light-sensitive intracellular biomolecules. This initiates cellular chain reactions and also triggers secondary responses not only limited to the treated skin area but can affect the whole body 7-9. Bio-positive effects attributed to Bioptron include reducing plasma levels of pro-inflammatory cytokines, increasing anti-inflammatory cytokine levels and fibroblast proliferating factors and modifying lymphocyte proliferation and 9, 10. However, the exact mechanism of action of bioptron at cellular level remains unknown 10. Bioptron therapy has been recommended for the management of lateral elbow tendinopathy, chronic venous and pressure ulcers and acne vulgaris 8, 11, 12, 13. Bioptron therapy was shown to be an effective short term treatment for lateral epicondylitis 14. Bioptron therapy speeds healing following cosmetic facial procedures, and large wounds following major abdominal surgery. There is stronger evidence from a moderate quality RCT that Bioptron improves healing of skin graft donor site wounds, and venous and pressure ulcers 8, 11, 12.
The efficacy of light therapy mainly low level laser as a coherent light on carpal tunnel syndrome has been investigated in some previous studies favoring laser therapy versus splinting 5,13, 14. However, there are only few studies evaluating the effect of bioptron therapy as an incoherent, polychromatic, polarized light on relieving symptoms in CTS 5, 14. The major limitation in these studies was lack of control group 14, furthermore, they lacked any objective evaluations of symptoms improvement after treatment by electrodiagnostic studies 5.
We sought to investigate the clinical efficacy of Polarized Polychromatic Noncoherent Light (Bioptron) therapy in idiopathic carpal tunnel syndrome concerning short term pain relief and nerve conduction characteristic improvement.
Methods
Patients & Setting
In this randomized controlled clinical trial, we included all the patients with mild and moderate CTS referred to the physical medicine and rehabilitation clinic of Shahid Modarres general and educational Hospital during 2012. Inclusion criterion for the study was idiopathic mild to moderate and the presence of CTS symptoms including hand‘s pain paresthesia and numbness for more than 6 months.
We diagnosed CTS based on clinical and electrodiagnostic studies by using standard electrophysiological criteria 4.
Exclusion criteria
Patients were excluded if they had secondary entrapment neuropathies, cervical radiculopathies, electroneurographic and clinical signs for axonal degeneration of the median nerve; had history of surgical release of CTS, ultrasound therapy or steroid injections into the carpal tunnel; or recent regular use of analgesic or antiinflammatory drugs.
Definitions of disease severity based on electrodiagnostic findings were as follow 4:
Mild CTS: Only the sensory fibers were involved without further involvement of the motor fibers, which means the sensory peak latency ≥ 3.5 ms and the motor onset latency ≤ 4.2 ms.
Moderate CTS: Defined as simultaneous involvement of both sensory and motor fibers in such condition that neither of the sensory nor the motor waves were absent, which means the sensory peak latency ≥3.5 ms and the motor onset latency of > 4.2 ms;
In severe cases, there might be absent sensory or motor waves, motor wave decreased amplitude and denervation potential in electromyography (EMG) of median innervated thenar muscles.
All Electrophysiological studies before and after therapy were performed by the same physiatrist. All electrophysiologic measurements were performed with a two channel Caldwell-Sierra wave EMG-NCV device, USA.
Patients’ recruitment
After describing the study to the patients and signing of the written consent, we randomly divided the subjects into Biotptron group and control group.
Randomization and patients’ enrollment
The block covariate adaptive randomization method is designed to randomize subjects into the treatment groups. This led to equal sample sizes within each group and balanced the important covariates. Thus, a new participant is sequentially assigned to particular treatment groups by taking into account the specific matched covariates and previous assignments of participants.
Bioptron light treatment intervention
Bioptron is a low energy light which is a part of the electromagnetic spectrum with no UV radiation 6, 7. The light emitted by Bioptron light therapy is characterized as polarized (its waves oscillate on parallel planes), polychromatic (wavelength: 480-3400 nm), incoherent (out of phase light, unlike laser light) and low energy light. Polychromacy means bioptron contains not only one wavelength (like laser light) but a wide range, including visible light and a portion of the infrared range. Unlike laser light, BIOPTRON Light is incoherent, or out-of phase light. This means that the light waves are not synchronized. BIOPTRON Light has a low energy density. This energy density has bio-stimulative effects 6,7.
Bioptron 2 device (Harrier Inc.) was used to deliver the Bioptron light with the following output characteristics: rated power of halogen = 90 W; light wavelength = 480– 3400 nm; degree of polarization = 95%; specific power density = 40mW/cm2; and energy density = 2.4 J/cm2.
Patients attended the physical medicine clinic three times each week over a 4-weeks period for each Bioptron light treatment. Bioptron light was administered by a physiatrist following the advice provided in the manufacturer’s user guide. Patients sat in a comfortable chair with the hand placed on an armrest in an extended and supinated position.
The Bioptron light probe was held at a 90° angle 5–10 cm above the clean bare skin of the carpal tunnel area, as this is reported to achieve maximal penetration of light, for exactly 8 min.
Wrist splint in neutral position was also administered simultaneously with Bioptron therapy for patients in this group for 8 weeks.
Splinting group (control group)
Wrist splint in neutral position was applied for 8 weeks. It was ethically reasonable to administer wrist splint for control group identically.
Patients in both groups did not receive further treatments during the follow-up period. We instructed the patients to apply the splints during day and night for 8 weeks. They were allowed to don off the splints for personal hygiene.
Outcome measures
Electrophysiological parameters and pain intensity were evaluated before the first treatment session and 8 weeks after initiating the therapy which means at the end of 10 sessions of Bioptron therapy accompanied by 8 weeks splinting in Bioptron group and after 8 weeks of wrist splinting in control group. Electrodiagnostic studies were performed by a physician not informed about the treatment.
Pain intensity
Pain severity was assessed using Visual Analogue Scale (VAS). The patient marked the relative severity of pain on a 10-cm scaled tape. The zero point represented no pain and the 10 point represented the maximal pain severity. We determined the pain severity by calculating the distance between the zero point and the marked point.
Electrophysiological measurements
All electrophysiological assessments were made according to electrodiagnostic medicine by Daneil Dumitru 4.
The skin temperature of the forearm was kept constant at 3233° C during all electrophysiological measurements.
Data analysis
Data analysis was performed using SPSS 18 software. According to the Shapiro-Wilks normality tests, patients’ age, pain scores and duration were not normally distributed and therefore non-parametric tests were used. Mann-whitney-tests were utilized to declare the need of comparisons of each two independent groups. Fisher’s exact test and Qui-two were run to compare the ordinal scales.
The assessors including the statistician and physician performed electrodiagnostic studies were blinded to the group of the patients.
Ethics
From the ethical point of view, the written consent form was signed or fingerprinted by the patient. The institutional review board of Shahid Beheshti University of Medical Sciences approved the protocol of this study. The process of treatment had no harm for their health, and they had authority to stop the process of treatment freely.
Results
Patients’ characteristics
In this study, fifty six patients were initially evaluated but finally fifty patients were assessed. Twenty seven and twenty three patients were initially allocated to study group (splinting+Bioptron) and control group (Splinting), respectively (Flow chart diagram). As it can be read from the flow chart, 21(91%) and 23 (85%) of patients in control and intervention groups remained in the study until the end respectively.
The patients’ characteristics at study entry were shown in Table 1. There were no between-group differences at baseline in demographic characteristics and electrophysiological findings (Tables 1 and 2).
Table 1. Demographic characteristics and pain scores at the beginning of the study and comparison of two groups .
| Variable | ||||||
| treatment |
age*
(yr) |
Female
†
/total |
Side ratio
†
RT/total |
Pain*
(VAS) |
Pain* duration (m) | Severity † (Mild) |
| Control | 42.3 ± 8.2 | 71.4 | 61.9 | 5.9 ± 1.3 | 8.8 ± 10.1 | 61.9% |
| Bioptron | 43.9 ± 9.8 | 78.3 | 69.6 | 6.2 ± 1.4 | 8.3 ± 5.7 | 65.2% |
| Total | 42.79 ± 8.6 | 75 | 65.9 | 6.09 ± 1.35 | 7.6 ± 5.2 | 61.3% |
*Mann-Whitney test:P>0.05
†Fishers Exact test: P>0.05
Table 2. Electrophysiological parameters at study entry compared between two groups.
| Variable | ||||
| treatment |
DSL
(ms) |
SNAP
Amplitude (μv) |
DML
(ms) |
CMAP
Amplitude (μv) |
| Control | 4.01 ± 0.37 | 43.14 ± 13.13 | 4.02 ± 0.38 | 9.38 ± 3.28 |
| Bioptron | 4.01 ± 0.35 | 42.13 ± 6.94 | 3.98 ± 0.49 | 8 ± 1.12 |
| Total | 4.01 ± 0.36 | 42.67 ± 10.37 | 4 ± 0.4 | 8.6 ± 2.5 |
*Mann-Whitney test:P>0.05
†Fishers Exact test: P>0.05
Pain severity
Pain severity based on VAS decreased significantly after therapy in both control and intervention groups (Figure 1) but there was no statistically meaningful difference between two groups regarding pain improvement (Table 3).
Figure 1 .
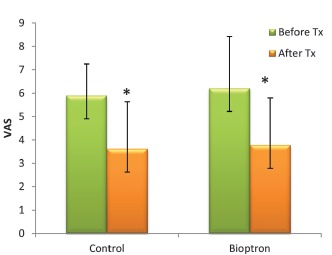
Pain intensity changes after therapy in two groups.
Table 3. Pain severity before (VAS1) and after accomplishing the treatments (VAS2) accompanied by the comparison of two groups .
| Group | Variable | ||
| Pain (VAS 1) | Pain (VAS 2) | P-value † | |
| Control | 5.9 ± 1.34 3 | 3.62 ± 2.01 | P<0.05 |
| Bioptron | 6.2 ± 1.38 | 3.78 ± 2.19 | P<0.05 |
| P>0.05 | P>0.05* | ||
*between groups after the trial: P=0.685(Kruskal-wallis)
†within each group (before & after the trial)(Willcoxon-signed rank)
Electrophysiological findings
The median nerve distal sensory latency improved significantly after therapy in both groups (Table 4), but there was no statistically meaningful difference between two groups regarding median SNAP latency improvement.
Table 4. The median nerve distal sensory latency before and after accomplishing the treatments and comparison of two groups .
| Group | Variable | ||
|
DSL(ms)
(Before therapy) |
DSL(ms)
(After therapy) |
P-value † | |
| Control | 4.01 ± 0.37 | 3.78 ± 0.35 | P<0.05 |
| Bioptron | 4.01 ± 0.35 | 3.83 ± 0.34 | P<0.05 |
| P>0.05 | P>0.05* | ||
*between groups after the trial: P=0.636(Kruskal-wallis)
†within each group (before & after the trial) (Willcoxon-signed rank)
Median nerve distal motor latency and amplitude, also sensory amplitude didn’t change significantly after therapy in both groups (Figure 2).
Figure 2 .
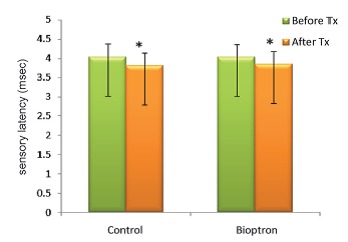
The median nerve distal sensory latency before and after accomplishing the treatments and comparison of two groups
Disease severity improvement
Bioptron group:
Before the treatment, the severity of the disease in Bioptron group based on electrodiagnostic findings were mild in 65% and moderate in the others. Eight weeks after initiating the therapy, electrophysiological findings became normal in 26% of patients %, mild in 56 % and moderate in 17% (Table 5).
Table 5. Severity of disease before (Severity 1) and after (Severity 2) accomplishing the treatments and comparison of two groups .
| Group | Variable | ||||
|
Severity 1(%)
(Before therapy) |
Severity 2(%)
(After therapy) |
||||
| Mild | Moderate | Normal | Mild | Moderate | |
| Control | 61.9% | 38.1% | 28.5% | 52.5% | 19% |
| Bioptron | 65.2% | 34.8% | 26.1% | 56.5% | 17.4% |
| Total | 61.36% | 38.64% | 27.27% | 54.55% | 18.18% |
Control group:
Before the treatment, the severity of the disease in the control group based on electrodiagnostic findings were mild in 61% and moderate in the others. Eight weeks after initiating the therapy, electrophysiological findings were normal in 28% of patients, mild in 52 % and moderate in 19% (Table 5).
Between group comparisons:
Comparing different severities of the disease before (Severity 1) and after accomplishing the treatment (Severity2) were mentioned in Table 4 . There was no meaningful difference between disease severity changes in both groups.
Discussion
In the present study, pain severity based on VAS score as well as sensory distal latency variable were improved significantly in eight weeks after initiating the treatments in both the intervention and control groups. Furthermore, no significant difference was observed between two groups comparing pain severity and electrodiagnostic variables. There was no improvement in other electrophysiological findings including the sensory and motor amplitude, as well as distal motor latency. Also, 8 weeks after treatment, 26% of the patients in the Bioptron group and 28% of the patients in control group became normal electrodignostically which confirmed this fact that both of these treatments were quite equally effective in short term.
There is rarity of studies evaluating the effect of Bioptron light therapy on patients with carpal tunnel syndrome or inflammatory conditions such as tendinitis. Generally, the results regarding the effectiveness of the laser therapy are different in several studies 12, 15.
Stasinopoulos conducted a preliminary, prospective, open clinical trial to assess the efficacy of polarized polychromatic noncoherent light (Bioptron light) in the treatment of idiopathic CTS. In that study, 25 patients with mild to moderate CTS lasting >3 months received bioptron light three times weekly for 4 weeks. Outcome measures used were the participants’ global assessments of nocturnal pain and paresthesia at 4 weeks and 6 months, respectively. Nocturnal pain and paresthesia associated with CTS improved during Bioptron light treatment. However, due to the absence of control group, they could not conclude that these findings were due to the Bioptron light treatment intervention itself rather than to probable natural improvements in symptoms. Furthermore, they evaluated symptoms improvement only subjectively and no electrophysiological studies were included 16. The strong point of our study was that we evaluated the efficacy of Bioptron both clinically via VAS score and by performing electrophysiological studies.
The efficacy of bioptron in the management of lateral epicondylitis has been evaluated in a number of studies. In a study by Stasinopoulos, Bioptron therapy for 4 weeks led to significant functional and pain improvement in patients with lateral epicondylitis 15, again that study lacked control group.
Bioptron is a new therapeutic modality which efficacy has been investigated for the following conditions: burns, carpal tunnel syndrome, lateral epicondylitis 15, postsurgical healing 7, and ulcers.
Like laser therapy, Bioptron is also a low-power light source, but differs in that it is polychromatic and incoherent rather than monochromatic and coherent. Low-power laser light, compared to Bioptron, has higher cost, needs more safety considerations for both the patient and therapist, requires user’s skills, and because of the small diameter of the laser beam, allows only a limited area to be treated 5, 9, 11.
There are several theories about Bioptron’s mechanism of action. It is probable that Bioptron light accelerates the cellular mechanisms and improves the blood supply, decreases pro inflammatory cytokines, and increases plasma level of anti-inflammatory and fibroblast growth factors 11, 17, 18, 19 but research is needed to investigate its exact mechanism of action.
In our investigation, splinting the wrist in neutral position alone leaded to significant improvement in pain scores and electrophysiological parameters in patients with CTS. In agreement with our results, therapeutic effects of splinting for CTS have been shown in previous studies 16. Splinting used to be a traditional treatment for CTS with the aim of reducing repetitive wrist motion to promote healing of irritated nerve 19, 16, 20.
It is important to mention that no side effects were reported during or after the treatment period. In line with our results, no side effects were reported for Bioptron in previous studies 14, 15 . As there is no ultraviolet light in the Bioptron spectrum, there is no excessive heating effect and it is totally safe for the eyes or for pregnant women.
Even though, very few studies evaluated the Bioptron therapy as a polychromatic light therapy on patients with CTS, but short term and long term effectiveness of low-level laser therapy as a monochromatic coherent light in reducing pain and severity of CTS (based on electrodiagnostic medicine classification) in patients with mild and moderate CTS was demonstrated in some studies concluding that low laser can be as effective as local steroid injection 22-27.
Yagci and his colleagues investigated the short-term efficacy of splinting and splinting plus low-level laser therapy in mild or moderate CTS. In the third-month control, Laser group had significant improvements on both clinical and NCS parameters (median motor nerve distal latency, median sensory nerve conduction velocities) 21.
Also in another study, pain and electrophysiological parameters of CTS were improved by combined 830- 1064 high-intensity LASER in symptomatic carpal tunnel syndrome 26.
In conclusion, the application of Bioptron in this study with the aforementioned parameters and the duration of therapy led to pain and electrophysiological improvement in patients with mild to moderate CTS. However, these improvements were similar to splinting in short term follow up.
One explanation for improvement of symptomsin control group similar to Bioptron group was the implementation of splinting in both groups. According to ethical considerations, it was impossible to omit therapeutics interventions such as splinting in one group. Although this variable was identical in both groups, but its presence might dilute the effects of Bioptron.
Applying Bioptron with different therapeutic protocols and light parameters other than used in the study, longer duration of light therapy and long term assessment, and finally larger sample size are suggested to get final conclusion about the efficacy of Bioptron therapy in carpal tunnel syndrome.
Limitations: One of the limitations of our study was that the other parameters such as functional improvements assessed by different validated questionnaires as well as the satisfaction of patients from the therapeutic processes had not been considered. Also patients were not matched according to their occupation to evaluate the effects of hand work on symptoms recovery.
Acknowledgment
This manuscript was supported by the research grant from Laser Application in Medical Sciences Research Center. The authors would like to thank Mrs Razaghi and Dr. Leyla Khodakarim for their important contributions in this project. In addition, the authors would like to thank the nurses who helped the enrolment of patients and the patients who were willing to participate in this study.
Please cite this article as follows:
Raeissadat SA, Rayegani SA, Rezaei S, Sedighipour L, Bahrami MH, Eliaspour D, Karimzadeh A. The Effect of Polarized Polychromatic Noncoherent Light (Bioptron) Therapy on Patients with Carpal Tunnel Syndrome. J Lasers Med Sci 2014;5(1):39-46
References
- 1.Salaffi F, De Angelis R, Grassi W , Arche M . Prevalence of Musculoskeletal conditions in an Italian population sample. Clin Exp Rheumatol. 2005;23:819–28. [PubMed] [Google Scholar]
- 2.Robert A, Werner R, Andray M. Electrodiagnostic evaluation of carpal tunnel syndrome. Muscle Nerve. 2011;44:597–607. doi: 10.1002/mus.22208. [DOI] [PubMed] [Google Scholar]
- 3.Bonfiglioli R, Mattioli S, Fiorentini C, Graziosi F, Curti S, Violante FS. Relationship between repetitive work and the prevalence of carpal tunnel syndrome in part-time and full-time female supermarket cashiers: a quasi-experimental study. Int Arch Occup Environ Health. 2007;80:248–53. doi: 10.1007/s00420-006-0129-0. [DOI] [PubMed] [Google Scholar]
- 4. Dumitru D, Amato A.A, Zwart M.J:Electrodiagnostic Medicine. 2nd ed. Philadelphia:Hanley & Belfus, Inc 2002;p1058-70.
- 5.Naeser MA. Photobiomodulation of pain in Carpal tunnel syndrome: review of seven studies. Photomed Laser Surg. 2006;24:101–10. doi: 10.1089/pho.2006.24.101. [DOI] [PubMed] [Google Scholar]
- 6.Nobuta S, Sato K, Nakagawa T, Hatori M, Itoi E. Effects of wrist splinting for Carpal Tunnel syndrome and motor nerve conduction measurements. Ups J Med Sci. 2008;113:181–92. doi: 10.3109/2000-1967-228. [DOI] [PubMed] [Google Scholar]
- 7.Reddy M, Gill SS, Kalkar SR, Wu W, Anderson PJ, Rochon PA. Treatment of pressure ulcers: a systematic review. JAMA. 2008;300:2647–62. doi: 10.1001/jama.2008.778. [DOI] [PubMed] [Google Scholar]
- 8.Jasmina Begic-Rahic, Sanja Vranic. The Application of Bioptron Light Therapy in Dermatology and Wound Healing. European Dermatolo. 2010;5:57–60. [Google Scholar]
- 9.Kubasova T, Horváth M, Kocsis K, Fenyö M. Effect of visible light on some cellular and immune parameters. Immunol Cell Biol. 1988;73:239–44. doi: 10.1038/icb.1995.39. [DOI] [PubMed] [Google Scholar]
- 10.Zhevago NA, Samoilova KA. Pro- and Anti-inflammatory Cytokine Content in Human Peripheral Blood after Its Transcutaneous (in Vivo) and Direct (in Vitro) Irradiation with Polychromatic Visible and Infrared Light. Photomed Laser Surg. 2006;24:129–39. doi: 10.1089/pho.2006.24.129. [DOI] [PubMed] [Google Scholar]
- 11.Medenica L, Lens M. The use of ploarised polychromatic non-coherent light alone as a therapy for venous leg ulceration. J Wound Care. 2003;12:37–40. doi: 10.12968/jowc.2003.12.1.26456. [DOI] [PubMed] [Google Scholar]
- 12.Iordanou P, Baltopoulos G, Giannakopoulou M, Bellou P, Ktenas E. Effect of polarized light in the healing process of pressure ulcers. Int J Nurs Pract. 2002;8:49–55. doi: 10.1046/j.1440-172x.2002.00338.x. [DOI] [PubMed] [Google Scholar]
- 13.Charakida A, Seaton ED, Charakida M, Mouser P, Avgerinos A, Chu AC. Phototherapy in the treatment of acne vulgaris: what is its role? . Am J Clin Dermatol. 2004;5:211–6. doi: 10.2165/00128071-200405040-00001. [DOI] [PubMed] [Google Scholar]
- 14.Stasinopoulos D, Stasinopoulos I. Comparison of effects of Cyriax physiotherapy, a supervised exercise programme and polarized polychromatic non-coherent light (Bioptron light) for the treatment of lateral epicondylitis. Clin Rehabil. 2006;20:12–23. doi: 10.1191/0269215506cr921oa. [DOI] [PubMed] [Google Scholar]
- 15.Stasinopoulos D. The use of polarized polychromatic non-coherent light as therapy for acute tennis elbow/ lateral epicondylalgia: a pilot study. Photomed Laser Surg. 2005;23:66–9. doi: 10.1089/pho.2005.23.66. [DOI] [PubMed] [Google Scholar]
- 16.Stasinopoulos D, Stasinopoulos I, Johnson MI. Treatment of carpal tunnel syndrome with polarized polychromatic noncoherent light (Bioptron light): a preliminary, prospective, open clinical trial. Photomed Laser Surg. 2005;23:225–8. doi: 10.1089/pho.2005.23.225. [DOI] [PubMed] [Google Scholar]
- 17.Huisstede BM, Hoogvliet P, Randsdorp MS, Glerum S, van Middelkoop M, Koes BW. Carpal tunnel syndromePart I: effectiveness of nonsurgical treatments-a systematic review. Arch Phys Med Rehabil. 2010;91:981–1004. doi: 10.1016/j.apmr.2010.03.022. [DOI] [PubMed] [Google Scholar]
- 18.Zhevago NA, Samoilova KA. Modulation of proliferation of peripheral blood lymphocytes after irradiation of volunteers with polychromatic visible and infrared light . Tsitologiia. 2004;46(6):567–77. [PubMed] [Google Scholar]
- 19.O’Connor D, Marshall S, Massy-Westropp N. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome. Cochrane Database Syst Rev. 2003;(1):CD003219. doi: 10.1002/14651858.CD003219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Annette A, M Gerritsen, IBC Korthls, De Bos. Splinting for carpal tunnel syndrome: prognostic indicator of success. J NeurolNeurosurg Psych. 2003;74:1342–4. doi: 10.1136/jnnp.74.9.1342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yagci I, Elmas O, Akcan E, Ustun I, Gunduz OH, Guven Z. Comparison of splinting and splinting plus low-level laser therapy in idiopathic carpal tunnel syndrome. Clin Rheumatol. 2009;28:1059–65. doi: 10.1007/s10067-009-1213-0. [DOI] [PubMed] [Google Scholar]
- 22.Barbosa RI, da Silva Rodrigues EK, Tamanini G, Marcolino AM, Elui VM, de Jesus Guirro RR. et al. Effectiveness of low-level laser therapy for patients with carpal tunnel syndrome: design of a randomized single-blinded controlled trial. BMC Musculoskelet Disord. 2012;13:248. doi: 10.1186/1471-2474-13-248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Reza Soltani Z, Ghayoomi AA, Raeissadat SA, Azam K, Kazempoor M, Najafi Sh. Study of short term effects of low level laser therapy [LLLT] vslocal steroid injection on patients with carpal tunnel Syndrome . Sci Res J Army Univ Med Sci. 2008;6:91–7. [Google Scholar]
- 24.Raeissadat SA, Reza Soltani Z. Study of Long Term Effects of Laser Therapy Versus Local Corticosteroid Injection in Patients with Carpal Tunnel Syndrome. J Lasers Med Sci. 2010;1:24–30. [Google Scholar]
- 25.Piazzini DB, Aprile I, Ferrara PE, Bertolini C, Tonali P, Maggi L. et al. systematic review of conservative treatment of carpal tunnel syndrome. Clin Rehabil. 2007;21:299–314. doi: 10.1177/0269215507077294. [DOI] [PubMed] [Google Scholar]
- 26.Casale R, Damiani C, Maestri R, Wells CD. Pain and electrophysiological parameters are improved by combined 830-1064 high-intensity LASER in symptomatic carpal tunnel syndrome versus Transcutaneous Electrical Nerve StimulationA randomized controlled study . Eur J Phys Rehabil Med. 2013;49:205–11. [PubMed] [Google Scholar]
- 27.Rayegani SM, Bahrami MH, Eliaspour D, Raeissadat SA, Shafi Tabar Samakoosh M, Sedihgipour L, Kargozar E. The Effects of Low Intensity Laser on Clinical and Electrophysiological Parameters of Carpal Tunnel Syndrome. J Lasers Med Sci. 2013;4:182–9. [PMC free article] [PubMed] [Google Scholar]