

Abstract
Background:
The most common definitions of large volume liposuction refer to total 5 l volume aspiration during a single procedure (fat plus wetting solution). Profound haemodynamic and metabolic alterations can accompany large volume liposuction. Due to paucity of literature on the effect of different tumescent solutions on the electrolyte balance and haematological changes during large volume liposuction, we carried out this study using two different wetting solutions to study the same.
Materials and Methods:
Total 30 patients presenting with varying degrees of localized lipodystrophy in different body regions were enrolled for the study. Prospective randomized controlled trial was conducted by Department of Plastic and Cosmetic Surgery, Sir Ganga Ram Hospital, New Delhi from January 2011 to June 2012. Patients were randomized into two groups of 15 patients each by using computer generated random numbers. Tumescent formula used for Group A (normal saline [NS]) was our modification of Klein's Formula and Tumescent formula used for Group B (ringer lactate [RL]) was our modification of Hunstadt's formula. Serum electrolytes and hematocrit levels were done at preinduction, immediate postoperative period and postoperative day 1.
Result:
Statistical analysis was performed using SPSS software version 15.0. Which showed statistically significant electrolytes and hematocrit changes occur during large volume liposuction.
Conclusion:
Statistically significant electrolytes and hematocrit changes occur during large volume liposuction and patients should be kept under observation of anaesthesist for at least 24 h. Patients require strict monitoring of vital parameters and usually Intensive Care Unit is not required. There was no statistical difference in the electrolyte changes using NS or RL as tumescent solution and both solutions were found safe for large volume liposuction.
KEY WORDS: Electrolyte changes during liposuction, haemogram changes during liposuction, large volume liposuction
INTRODUCTION
The most common definitions of large volume liposuction refer to total 5 l volume removed during the procedure (fat plus wetting solution).[1] Profound haemodynamic and metabolic alterations can accompany large volume liposuction.[2,3,4,5]
Due to paucity of literature on the effect of different tumescent solutions on the electrolyte balance and haematological changes during large volume liposuction, we carried out this study using two different wetting solutions (normal saline [NS] and ringer lactate [RL]) to study the same.
Aims and objectives
To study the effect of large volume liposuction on haematological changes and electrolyte balance using NS and RL in the tumescent solution.
MATERIALS AND METHODS
Study site: Department of Plastic and Cosmetic Surgery, Sir Ganga Ram Hospital, New Delhi.
Study duration: January 2011 to June 2012.
Study design: Prospective Randomized Controlled Trial.
Inclusion criteria
Patients with localized fat deposits with.
-
American Society Of Anaesthesiologist Grading
- Normal healthy patient
- Patients with mild systemic disease.
Realistic expectations regarding the outcome of the procedure.
Exclusion criteria
Patients undergoing concomitant procedures.
Presence of significant medical diseases such as diabetes mellitus, cardiac, renal, hepatic, gastrointestinal or endocrinal diseases (American Society of Anaesthesiologist Grading III and IV) (Patients with severe systemic disease and Patients with severe systemic disease that is a constant threat to life).
Methodology and measurement
A total of 47 patients came during the study period, out of which 7 were excluded on the basis of exclusion criteria, 6 patients did not give consent for blood test during and after procedures and 4 patients did not fulfil the inclusion criteria. A total of 30 patients were enrolled for the procedure.
Each patient was subjected to the full history and systemic examination, and an informed written consent was taken.
Group allocation
Patients were randomised into two groups of 15 patients each by using computer generated random numbers.
Group A (NS): Those patients receiving NS in the tumescent fluid during liposuction.
Group B (RL): Those patients are receiving RL in the tumescent fluid during liposuction.
Tumescent formula used for Group A (NS) was our modification of Klein's Formula that consists of:
30 ml of 2% lignocaine.
1 ml adrenaline (1:1000).
5 ml of 7.5% sodium bicarbonate.
Mixed in 1 l of NS.
Tumescent formula used for Group B (RL) was our modification of Hunstadt's formula which consists of:
30 ml of 2% lignocaine.
1 ml adrenaline (1:1000).
Mixed in 1 l of RL.
The total dose of lidocaine in both the groups did not exceed 55 mg/kg.
Operative details
Tumescent solution (Superwet technique where the ratio of wetting solution to desired aspirate is 1:1) according to the group in which the patient belonged, was injected till the skin became firm and turgid.
-
Intra-operative intravenous (IV) fluid requirement was guided by
-
Rohrich's formula to maintain an intraoperative fluid ratio of about 1.2[6]
 and
and - Urine output of 1-1.2 ml/kg/(body weight per h).
-
Serum electrolytes (sodium, potassium, calcium and ionized calcium), haemoglobin, packed cell volume (PCV) and arterial blood gases (pH, pCO2, HCO3) were done at preinduction and in the immediate postoperative period, (within half hour of extubation) in the recovery room.
Serum electrolytes (sodium, potassium, calcium and ionized calcium), haemoglobin and PCV were repeated on postoperative day 1 (24 h postoperatively).
Postoperative care
All patients were kept in the recovery room for 1.5-2 h for close monitoring of vital parameters and fluid management before shifting toward. Postoperative IV RL was given as maintenance fluid, requirements being adjusted to vital signs and urine output of 1-1.2 ml/kg/h.
Discharge was planned at 24 h after the general condition of the patient was found satisfactory.
Statistics
Statistical analysis was performed using SPSS software version 15.0 (IBM Corporation). Continuous variables are presented as mean ± standard deviation. For comparison of parameters between two groups, we have used the unpaired t-test/Mann-Whitney t-test. For comparison of parameters within each of the groups, we have used the paired t-test/Wilcoxon test. A P < 0.05 was considered as significant.
OBSERVATIONS AND RESULTS
Total infiltrate, aspirate and the intraoperative intravenous fluid
The mean infiltrate in Group A was 8 ± 1.55 l and in Group B was 9.17 ± 2.50 l (P > 0.05). The mean total aspirate in Group A was 7.39 ± 1.49 l and in Group B was 8.51 ± 3.13 l (P > 0.05). The mean intraoperative fluid given in Group A was 1.07 ± 0.96 l and in Group B was 0.69 ± 0.47 l (P > 0.05). Both groups were comparable in the above parameters.
Changes in serum sodium
The average preoperative sodium in the Group A was 140 ± 2.65 mEq/L, immediate postoperative was 139 ± 2.30 mEq/L and on postoperative day 1 was 138 ± 2.47 mEq/L. The fall in sodium was statistically significant in the pre versus postoperative day 1 period (P - 0.04) in Group A. The average preoperative sodium in the Group B was 140 ± 2.78 mEq/L, in the immediate postoperative period was 139.07 ± 1.91 mEq/L and on postoperative day 1 was 137.8 ± 1.74 mEq/L. The fall in sodium was statistically significant in the pre versus immediate postoperative (P - 0.02) and the pre versus postoperative day 1 group (P - 0.005) and in the immediate postoperative versus the postoperative day 1 (P - 0.01) in the Group B. The preoperative, immediate postoperative and postoperative day 1 values for sodium were comparable between the groups (P - 0.5, P - 0.46, P - 0.22 respectively) that is, there was no statistically significant difference between the two groups [Table 1 and Figure 1].
Table 1.
Changes in serum sodium in both the groups

Figure 1.

Changes in serum potassium
Changes in serum potassium
The average preoperative potassium in the Group A was 4.31 ± 0.40 mEq/L, in the immediate postoperative period was 4.12 ± 0.39 mEq/L and on postoperative day 1 was 4.07 ± 0.37 mEq/L. The fall in potassium was statistically significant in the pre versus immediate postoperative period (P - 0.04) and in the pre versus postoperative day 1 period (P - 0.03) in Group A. The average preoperative potassium in Group B was 4.04 ± 0.31 mEq/L, in the immediate postoperative period was 3.83 ± 0.24 mEq/L and on postoperative day 1 was 3.85 ± 0.32 mEq/L. The fall in potassium was statistically significant in the pre versus immediate postoperative period (P - 0.009) and the pre versus postoperative day 1 group (P - 0.04) in Group B. The preoperative and immediate postoperative values for potassium were not comparable between the groups (P - 0.02, 0.01 respectively) that is, there was a difference in the values in both the groups. In Group B, the average preoperative potassium was lower than that in Group A [Table 2 and Figure 2].
Table 2.
Changes in serum potassium in both the groups

Figure 2.

Changes in serum calcium
Changes in serum calcium
The average preoperative calcium in Group A was 8.97 ± 0.40 mg/dl, in the immediate postoperative period was 8.31 ± 0.32 mg/dl and on postoperative day 1 was 8.01 ± 0.51 mg/dl. The fall in calcium was statistically significant in the pre versus immediate postoperative period (P - 0.001), pre versus postoperative day 1 (P - 0.0006) and in the immediate postoperative versus postoperative day 1 period (P - 0.003) in Group A. The average preoperative calcium Group B was 8.77 ± 0.37 mg/dl, in the immediate postoperative period was 8.30 ± 0.65 mg/dl and on postoperative day 1 was 8.0 ± 0.53 mg/dl. The fall in calcium was statistically significant in the pre versus immediate postoperative day 1 period (P - 0.0006) and the pre versus postoperative day 1 group (P - 0.0003) and in the immediate postoperative versus postoperative day 1 period (P - 0.01) in the Group B. The preoperative, immediate postoperative and postoperative day 1 values for calcium were comparable between the groups (P - 0.08, P - 0.4, P - 0.4 respectively) that is, there was no statistically significant difference between the two groups [Table 3 and Figure 3].
Table 3.
Changes in serum calcium in both the groups

Figure 3.

Changes in ionised calcium
Changes in ionised calcium
The average preoperative ionised calcium in the Group A was 1.29 ± 0.04 mg/dl, in the immediate postoperative period was 1.28 ± 0.03 mg/dl and on postoperative day 1 was 1.28 ± 0.03 mg/dl. The fall in ionised calcium was not statistically significant in the pre versus immediate postoperative period (P-0.13), pre versus postoperative day 1 (P - 0.15) and in the immediate postoperative versus postoperative day 1 group (0.32) in Group A. The average preoperative ionised calcium in Group B was 1.30 ± 0.03 mg/dl, 09 in the immediate postoperative period was 1.28 ± 0.09 mg/dl and on postoperative day 1 was 1.28 ± 0.08 mg/dl. The fall in ionized calcium was not statistically significant in the pre versus immediate postoperative day 1 period (P - 0.16) and the pre versus postoperative day 1 group (P - 0.14) and in the immediate postoperative versus postoperative day 1 period (P - 0.21) in Group B. The preoperative, immediate postoperative and postoperative day 1 values for ionized calcium were comparable between the groups (P - 0.17, P - 0.39, P - 0.38 respectively) that is, there was no statistically significant difference between the two groups [Table 4 and Figure 4].
Table 4.
Changes in ionised calcium in both the groups

Figure 4.

Changes in haemoglobin level
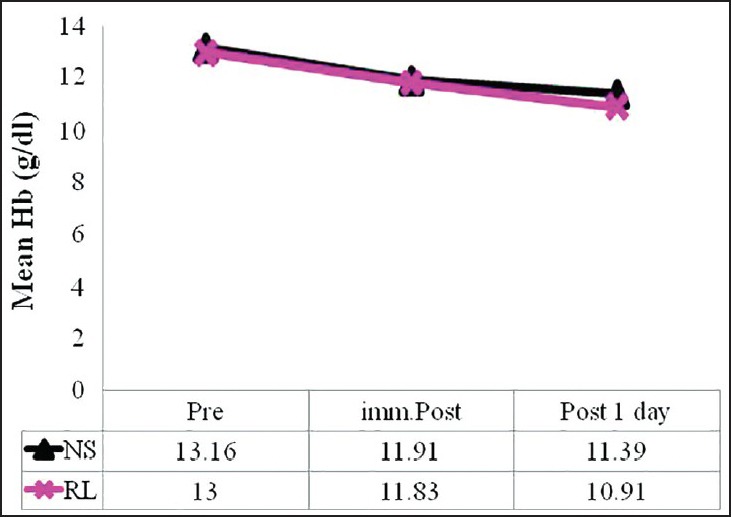
Changes in haemoglobin level
The average preoperative haemoglobin in Group A was 13.16 ± 1.08 g/dl, in the immediate postoperative period was 11.91 ± 1.21 g/dl and on postoperative day 1 was 11.39 ± 1.15 g/dl. The fall in haemoglobin was statistically significant in the pre versus immediate postoperative period (P - 0.00001), pre versus postoperative day 1 (P - 0.00002) and in the immediate postoperative versus postoperative day 1 period (P - 0.002) in Group A. The average preoperative haemoglobin in the Group B was 13.0 ± 1.30, in the immediate postoperative period was 11.83 ± 1.69 g/dl and on postoperative day 1 was 10.91 ± 1.97 g/dl. The fall in haemoglobin was statistically significant in the pre versus immediate postoperative day 1 period (P - 0.0004) and the pre versus postoperative day 1 group (P - 0.00002) and in the immediate postoperative versus postoperative day 1 period (P - 0.000004) in Group B. The preoperative, immediate postoperative and postoperative day 1 values for haemoglobin were comparable between the groups (P - 0.35, P - 0.44, P - 0.211 respectively) that is, there was no statistically significant difference between the two groups [Table 5 and Figure 5].
Table 5.
Changes in haemoglobin in both the groups

Figure 5.
Changes in haematocrit
CHANGES IN HAEMATOCRIT
The average preoperative haematocrit in Group A was 38.81 ± 2.61%, in the immediate postoperative period was 35.86 ± 3.87% and on postoperative day 1 was 34.48 ± 3.05%. The fall in haematocrit was statistically significant in the pre versus immediate postoperative period (P - 0.00001), pre versus postoperative day 1 (P - 0.000007) and in the immediate postoperative versus postoperative day 1 period (P - 0.008) in Group A. The average preoperative haematocrit in Group B was 39.33 ± 3.85%, in the immediate postoperative period was 36.11 ± 5.06% and on postoperative day 1 was 32.92 ± 6.06%. The fall in haematocrit was statistically significant in the pre versus immediate postoperative day 1 period (P - 0.0005) and the pre versus postoperative day 1 group (P - 0.00001) and in the immediate postoperative versus postoperative day 1 period (P - 0.000007) in Group B. The preoperative, immediate postoperative and postoperative day 1 values for haematocrit were comparable between the groups (P - 0.33, P - 0.43, P - 0.19 respectively) that is, there was no statistically significant difference between the two groups [Table 6 and Figure 6].
Table 6.
Changes in haematocrit in both the groups

Figure 6.

Changes in haematocrit in both the groups
DISCUSSION
Refinements in the surgical technique of liposuction now allow large volume liposuction to be performed; however, concern has been expressed regarding the safety of removing such large lipoaspirates.[7,8,9,10] Tumescent anaesthesia (i.e., very diluted lidocaine anaesthesia) became popular and is now the standard anaesthesia for liposuction. A safe dose of lidocaine using the tumescent solution has been estimated to be 35 mg/kg. On the basis of clinical investigations of plasma liodcaine, they concluded that most patients can be discharged approximately 8 h after surgery as long as the tumescent lidocaine dose is 35 mg/kg or less. Nevertheless, it is important to keep in mind that dose-independent lidocaine toxicity may also occur in the early postoperative period. Such early lidocaine toxicity may be involved in the drug interaction with lidocaine and sedative agents.[11]
Substantial fluid shifts occur both as fluid is infiltrated subcutaneously with resultant hypodermoclysis and as fat is removed, which Hetter compared with an internal burn injury with possible third space fluid loss.[12] In most other studies, RL was used in the tumescent solution.[2,3,13] The purpose of Ringer's lactate was to reduce the load of sodium as well as to provide a more neutral pH of 6.5 when compared to saline.[14] Hence in our study we compared the two tumescent solutions.
Changes in sodium levels
Though the lowering of the serum sodium was statistically significant in both the groups, in Group A the fall was not statistically significant in the immediate postoperative period which could be due to use of NS in Group A. But as there was more absorption of the infiltrate leading to haemodilution, on the postoperative day one, both the groups showed a fall in the sodium levels from the baseline values, though the values still remained in the physiologically normal range (135-145 mEq/l). The fall in sodium levels on postoperative day one were comparable in both the groups.
In a similar study conducted by Lipschitz et al. on 5 patients using RL as the tumescent solution, mild hyponatremia (135 ± 1.1 mmol/L) was observed at 4 h postoperative in four patients.[3] Mild hyponatremia (134-136 mmol/L) was also evident between 10 h and 25 h after induction in 4 patients. In our study, we also observed a fall in sodium levels from the baseline levels but the values remained in the normal range. Lipschitz et al. study group included 5 patients that were small compared to our study group which included 30 patients.
Changes in potassium levels
In our study, a fall in serum potassium concentration from baseline occurred in both the NS as well as the RL groups in the immediate postoperative period as well as the postoperative day 1. The lowering was statistically significant but was within the normal range (3.5-5.5 mEql/L) and the patients were asymptomatic clinically. The preoperative potassium values in Group B were lower compared to Group A, though both the groups have shown a fall in the potassium from the baseline levels, which could be due to haemodilution. In Group B however, the serum potassium levels on postoperative day one were higher compared to the immediate postoperative period, which could be due to use of RL in the tumescent solution in Group B.
In a similar study conducted by Lipschitz et al. on 5 patients using RL as the tumescent solution, the rapid onset of hypokalaemia intra operatively (3.3 ± 0.16 mmol/L) was significant for all patients.[3] In the same study levels, 20% greater than baseline occurred 8 h postoperatively, but no hyperkalaemia occurred.
There was no hyperkalaemia in our study. The reason for an increase in the potassium levels 8 h postoperatively, as stated by Lipschitz et al. in their study, could be due to release of intracellular potassium from the lysed adipocytes.
CHANGES IN CALCIUM LEVELS
In our study, a lowering of serum calcium concentration from baseline occurred in both the groups in the immediate postoperative period as well as the postoperative day 1 and the values were comparable. To confirm true hypocalcemia, we measured the ionised calcium values in the preoperative, immediate postoperative period as well as the postoperative day. We found that the changes in the value of ionised calcium in both the groups in the immediate postoperative as well as postoperative day one periods were not statistically significant and the values remained in the physiologically normal range (1.1-1.4 mmol/L), and most patients were asymptomatic, requiring no active intervention.
One patient in Group A and 2 patients in Group B, in the immediate postoperative period had serum calcium values below the normal range (<8 mg/dl), out of which only 1 patient in Group B who underwent 12.6 L liposuction had clinically significant hypocalcaemia and ionized calcium of 0.97 which is below the normal range. She also developed hypotension which did not improve with a fluid challenge. She was supplemented with IV calcium and the hypocalcaemia as well as the hypotension was corrected within 2-3 h.
Even on the postoperative day one, 6 patients in Group A and 5 patients in Group B (11 out of 13 had total aspirate more than 8 L) had serum calcium values below the normal range (<8 mg/dl), but the ionised calcium remained in the normal range and the patients were asymptomatic, hence no action was taken.
Change in hematocrit
The preoperative, immediate postoperative and postoperative day 1 values for haematocrit were comparable between the groups and no blood transfusion was required.
SUMMARY AND CONCLUSIONS
Statistically significant electrolytes and haematocrit changes occur during large volume liposuction and patients should be kept under observation for at least 24 h.
There was no statistical difference in the electrolyte changes using NS or RL as tumescent solution and both solutions were found safe for large volume liposuction.
Extreme care should be taken in patients with borderline electrolytes and hematocrit levels. These patients can manifest signs of electrolytes imbalance, so close monitoring should be done for clinical symptoms. Intra operative and postoperative fluid replacements with relation to the vital parameters and urine output will decrease the chances of fluid overload and electrolyte imbalances.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Iverson RE, Lynch DJ. American society of plastic surgeons committee on patient safety. Plast Reconstr Surg. 2004;113:1478–90. doi: 10.1097/01.prs.0000111591.62685.f8. [DOI] [PubMed] [Google Scholar]
- 2.Trott SA, Beran SJ, Rohrich RJ, Kenkel JM, Adams WP, Jr, Klein KW. Safety considerations and fluid resuscitation in liposuction: An analysis of 53 consecutive patients. Plast Reconstr Surg. 1998;102:2220–9. doi: 10.1097/00006534-199811000-00063. [DOI] [PubMed] [Google Scholar]
- 3.Lipschitz AH, Kenkel JM, Luby M, Sorokin E, Rohrich RJ, Brown SA. Electrolyte and plasma enzyme analyses during large-volume liposuction. Plast Reconstr Surg. 2004;114:766–75. doi: 10.1097/01.prs.0000131022.98481.6e. [DOI] [PubMed] [Google Scholar]
- 4.Kenkel JM, Lipschitz AH, Luby M, Kallmeyer I, Sorokin E, Appelt E, et al. Hemodynamic physiology and thermoregulation in liposuction. Plast Reconstr Surg. 2004;114:503–13. doi: 10.1097/01.prs.0000132676.19913.a3. [DOI] [PubMed] [Google Scholar]
- 5.Basile AR, Fernandes F, Basile VV, Basile FV. Fluid resuscitation in liposuction: A prospective analysis of infiltrate-to-total aspirate ratios lower than used for the superwet technique. Aesthetic Plast Surg. 2006;30:659–65. doi: 10.1007/s00266-006-0118-4. [DOI] [PubMed] [Google Scholar]
- 6.Jain AK, Khan AM. Stroke volume variation as a guide for fluid resuscitation in patients undergoing large-volume liposuction. Plast Reconstr Surg. 2012;130:462e–9. doi: 10.1097/PRS.0b013e31825dc381. [DOI] [PubMed] [Google Scholar]
- 7.Rao RB, Ely SF, Hoffman RS. Deaths related to liposuction. N Engl J Med. 1999;340:1471–5. doi: 10.1056/NEJM199905133401904. [DOI] [PubMed] [Google Scholar]
- 8.Platt MS, Kohler LJ, Ruiz R, Cohle SD, Ravichandran P. Deaths associated with liposuction: Case reports and review of the literature. J Forensic Sci. 2002;47:205–7. [PubMed] [Google Scholar]
- 9.Klein JA, Kassarjdian N. Lidocaine toxicity with tumescent liposuction. A case report of probable drug interactions. Dermatol Surg. 1997;23:1169–74. [PubMed] [Google Scholar]
- 10.Grazer FM, de Jong RH. Fatal outcomes from liposuction: Census survey of cosmetic surgeons. Plast Reconstr Surg. 2000;105:436–46. doi: 10.1097/00006534-200001000-00070. [DOI] [PubMed] [Google Scholar]
- 11.Oba H. Large-volume tumescent anesthesia for extensive liposuction in oriental patients: Lidocaine toxicity and its safe dose level. Plast Reconstr Surg. 2003;111:945–6. doi: 10.1097/00006534-200302000-00085. [DOI] [PubMed] [Google Scholar]
- 12.Hetter GP. Blood and fluid replacement for lipoplasty procedures. Clin Plast Surg. 1989;16:245–8. [PubMed] [Google Scholar]
- 13.Commons GW, Halperin B, Chang CC. Large-volume liposuction: A review of 631 consecutive cases over 12 years. Plast Reconstr Surg. 2001;108:1753–63. doi: 10.1097/00006534-200111000-00050. [DOI] [PubMed] [Google Scholar]
- 14.Toledo LS. Superficial syringe liposculpture. In: Toledo LS, editor. Annals of the II International Symposium: Recent Advances in Plastic Surgery – RAPS/90, Sao Paulo, Brazil: 1990. p. 446. [Google Scholar]