

Abstract
Background
Few studies have used spatially resolved ambient particulate matter with an aerodynamic diameter of <10 μm (PM10) to examine the impact of PM10 on ischemic heart disease (IHD) mortality in China. The aim of our study is to evaluate the short-term effects of PM10 concentrations on IHD mortality by means of spatiotemporal analysis approach.
Methods
We collected daily data on air pollution, weather conditions and IHD mortality in Beijing, China during 2008 and 2009. Ordinary kriging (OK) was used to interpolate daily PM10 concentrations at the centroid of 287 township-level areas based on 27 monitoring sites covering the whole city. A generalized additive mixed model was used to estimate quantitatively the impact of spatially resolved PM10 on the IHD mortality. The co-effects of the seasons, gender and age were studied in a stratified analysis. Generalized additive model was used to evaluate the effects of averaged PM10 concentration as well.
Results
The averaged spatially resolved PM10 concentration at 287 township-level areas was 120.3 ± 78.1 μg/m3. Ambient PM10 concentration was associated with IHD mortality in spatiotemporal analysis and the strongest effects were identified for the 2-day average. A 10 μg/m3 increase in PM10 was associated with an increase of 0.33% (95% confidence intervals: 0.13%, 0.52%) in daily IHD mortality. The effect estimates using spatially resolved PM10 were larger than that using averaged PM10. The seasonal stratification analysis showed that PM10 had the statistically stronger effects on IHD mortality in summer than that in the other seasons. Males and older people demonstrated the larger response to PM10 exposure.
Conclusions
Our results suggest that short-term exposure to particulate air pollution is associated with increased IHD mortality. Spatial variation should be considered for assessing the impacts of particulate air pollution on mortality.
Electronic supplementary material
The online version of this article (doi:10.1186/1476-069X-13-109) contains supplementary material, which is available to authorized users.
Keywords: Spatiotemporal analysis, Ischemic heart disease, Particulate matter, Ordinary kriging, Generalized additive mixed model
Background
Ischemic heart disease (IHD) is one of the most common causes of death worldwide, causing 7,249,000 deaths in 2008, 12.7% of total global mortality [1]. According to Global Burden of Disease Study in 2010, the number of ischemic heart disease deaths rose from 450.3 million in 1990 to 948.7 million in 2010, ranking the second leading causes of death in China in 2010 [2]. A number of risk factors for ischemic heart disease have been suggested, such as age, gender, hypertension, obesity and smoking [1–3].
Some studies have indicated that exposure to air pollution was associated with IHD mortality [4–6], morbidity [7], and hospital admissions [8, 9]. Studies on the impacts of ambient particles less than 10 μm in aerodynamic diameter (PM10) on health have also been performed in China, but most have used non-spatial data of daily PM10, e.g. monitoring values from one station or the average concentrations of a limited number of monitor stations, to estimate the association between PM10 and IHD mortality [10–12]. This may result in inaccuracies, specifically exposure misclassification, as PM10 may vary over a specific area due to expected differences in PM10 levels by the impact of local sources and meteorology. It is not clear how this uncertainty would impact risk estimations, either toward overestimation or underestimation, but it does make such evaluations much more difficult [13–15].
Various techniques (e.g. inverse distance weighting, land use regression analysis and geo-statistical methods such as kriging) have been developed to interpolate air pollution values at the locations where data are unavailable using data collected at multiple sites [16, 17]. Some studies have applied the interpolation methods to examine the health effects of air pollution in studies [18, 19]. There also has been evidence that the methods used to generate estimates of exposure to air pollution could affect the health risk estimates in epidemiological studies [20, 21].
Studies have applied interpolation methods to estimate the air pollutant concentrations in China [22, 23]. However, there is no study that has used spatially resolved PM10 concentrations to quantify the impact of PM10 on IHD mortality in China. The goal of this research is to apply a generalized additive mixed model to examine the association between spatially resolved PM10 concentrations and IHD mortality in Beijing.
Methods
Study area
Beijing is the capital of China, and located in the northern tip of the roughly triangular North China Plain. It has an area of 16,410 square kilometers, with 14 urban and suburban administrative districts (Dongcheng, Xicheng, Chaoyang, Haidian, Changping, Fengtai, Shijingshan, Mentougou, Daxing, Fangshan, Tongzhou, Shunyi, Huairou and Pinggu District) and two rural counties (Minyun and Yanqing County) which included 304 township-level areas. The population is 1.96 million (The Sixth National Population Census, Beijing, 2010). For townships, the size ranges from 1 to 390 square kilometers and the population ranges from 2000 to 359400 (The Sixth National Population Census, Beijing, 2010). It has a dry, monsoon-influenced humid continental climate, characterized by hot, humid summers and cold, windy, dry winters. Average annual temperature and precipitation was 14.0°C and 483.9 mm, respectively. Ambient air pollution is seriously elevated along with the increasing of fuel consumption (including vehicles, power plants and industries) and construction projects in the city.
Data collection
Daily numbers of IHD deaths between 1 January 2008 and 31 December 2009 were obtained from China Centers for Disease Control and Prevention (China CDC) for 287 township-level areas. The IHD death data were unavailable in Minyun and Yanqing Counties. The deaths at each area were residents of the corresponding area. IHD was defined according to the International Classification of Diseases, 10th version (ICD-10:I20-I25). The data were classified by gender (female and male) and age (<65 and ≥65 years).
PM10 data of 27 ambient air quality monitoring sites in Beijing city were collected from the Beijing Municipal Environmental Protection Bureau (Figure 1). The missing rate during the study period was from 0.4% to 6.7%. Imputation will produce error so we did not fill the missing value before interpolating. For SO2/NO2, only a single daily average concentration for the whole city was available from the Beijing Public Net for Environmental Protection. To control for the effect of weather conditions on IHD mortality, daily meteorological data on mean temperature and relative humidity from one station (located at N39°48′ E116°28′) were obtained from China Meteorological Data Sharing Service System.
Figure 1.
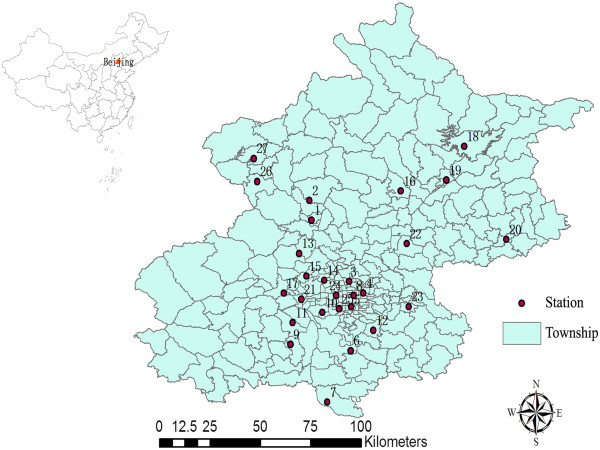
The 27 monitoring stations for PM 10 in Beijing.
Data analysis
Spatial interpolation for PM10 concentration
We selected two methods, inverse distance weighting (IDW) and ordinary kriging (OK), to interpolate the daily PM10 concentrations from the values of 27 monitoring sites to the centroids of the 304 township-level areas across Beijing city. IDW and kriging are the most common interpolation methods. About the performance of IDW and kriging, the findings have been mixed [24].
The IDW interpolation method is to estimate the value of a given location by a weighted average of data at nearby monitors, where interpolation weights for each monitor’s value are computed as a function of distance between observed sample sites and the site to be predicted [16]. We used λi = 1/di2 as a weighting factor for the monitor site i, where di is the distance between the monitor site i and the point to be predicted (i.e., the centroid of each township).
The kriging method is a geo-statistical technique and also a weighted combination of monitor values that uses spatial autocorrelation among data to determine the weights [16]. OK is the most common kriging method. It assumes a constant but unknown mean, which allows construction of an unbiased estimator that does not require prior knowledge of the stationary mean of the observed values [23]. In this study, we estimated the data at the centroid of each township using OK.
To test the validity of the interpolation methods and provide a more quantitative comparison of the two models, we conducted "leave-one-out cross-validation" (LOOCV). This method involves using a single monitor values as the validation data and the remaining monitor values as the training data. This is then repeated such that each monitor is used once as the validation data. The difference (including the root-mean-square error (RMSE) and the mean) and the correlation between the observed and predicted values were calculated as the measure indices of LOOCV.
Modeling the association between PM10 and IHD mortality
A generalized addictive mixed model (GAMM) was applied to analyze the effects of PM10 on IHD mortality, which uses additive nonparametric functions to formulate covariate effects and adds random effects to the additive predictor accounting for over-dispersion and correlation [25, 26]. We put the township-level IHD deaths as the dependent variable and the corresponding township-level PM10 estimates as the main independent variable in GAMM. Penalized Quasi-likelihood method [27, 28], accounting for the over-dispersion of daily death counts, was used in GAMM framework to model the natural logarithm of the expected daily death counts as a function of the predictor variables. A random area-level intercept in GAMM can be used to model those areas with higher death rates [29, 30].
First, the basic model was built excluding the air pollution variables. The penalized spline functions of time and weather variables for accommodating nonlinear relationships of mortality with these variables were incorporated. The partial autocorrelation function was used to guide the selection of degrees of freedom (df) for time trend [31]. We used squared Pearson scaled residuals to compare the fit of the models [30]. In this way, a penalized spline with seven degrees of freedom per year for time trend, which had the smallest sum of the absolute partial autocorrelation values over a 30-day lag period, was used to control for the seasonal and long-term trends. Because temperature’s effects on health may be lagged for more than 10 days [32, 33], the 14-day moving average temperature was controlled in our model [34, 35]. The present-day relative humidity was incorporated in the models because no evidence of confounding by this variable was shown in air pollution epidemiology [35]. Three degrees of freedom for temperature and relative humidity were chosen based on the model fitting [36]. The day of the week (DOW) and public holiday (PH) was adjusted as a categorical variable in the basic model. After the basic model was established, the pollutant variables were introduced. The final model was:
 |
Where i is the township (township = 1, ……, 287); t is the day; Yi,t is the number of IHD deaths in township i on day t. α is the intercept. PM10i,t is the daily PM10 concentration in township i on day t. S(.) is a penalized spline; Tempt is the mean temperature on day t; RHt is relative humidity on day t; a spline with 3 degrees of freedom (df) was used for temperature and relative humidity. A spline with 7 degrees of freedom per year for time was used to control for season and long-term trend. DOWt is the categorical variable day of the week on day t. PHt is the indicator of public holiday on day t. Zi is a random intercept for township i.
In order to compare the effects of spatial resolved PM10 and averaged PM10 of 27 monitoring stations in Beijing, we also used GAMM and generalized additive model (GAM) to examine the impacts of averaged PM10. The same confounders as GAMM were adjusted in GAM as follows:
 |
We next analyzed the associations between PM10 and IHD mortality with different lag structures, i.e. single-day lags (from lag 0 to lag 5) and multiday lags (lag 0–1 to 0–5). In single-day lag models, lag 0 referred to the current-day air pollutants concentration, and lag 1 corresponded to the previous-day concentration; while in multiday lag models, lag 0–1 meant the 2-day moving average concentration of current day and the previous day.
Single and multiple air pollutant models were also fitted to examine the effects of PM10 on IHD mortality in GAMM. In the single-pollutant model, PM10 was put alone in the model; in the two-pollutant models, SO2 (lag0-1) or NO2 (lag0-1)) were jointly included. SO2 or NO2 at lag 0–1 was controlled because this lag was shown to be more strongly associated with health effects [37, 38].
Stratified analyses by gender, age and season also were conducted. For season—spring, summer, autumn and winter are defined as March–May, June–August, September–November and December–February, respectively. The Z test was used to detect statistically differences between effect estimates from stratified analyses [39].
Sensitivity analyses were conducted to check the impacts of PM10 on IHD mortality using the different degrees of freedom (4–9) for time trend, temperature (4–6) and relative humidity (4–6) as well as controlling 14-day moving average relative humidity in the model. All the sensitivity analyses were done only for the whole population.
All the data analysis was performed in statistical software R version 3.0.1 (R Development Core Team, 2013). The "gstat" package was used to interpolate spatial PM10. The "mgcv" package was used to fit GAMM and GAM. All statistical tests were two-sided and P-values with less than 0.05 were considered statistically significant. The results are presented as the percent change and 95% confidence intervals (95%CIs) in daily IHD mortality per 10-μg/m3 increase in PM10 concentrations.
Results
Table 1 showed the descriptive statistics for IHD deaths, air pollutants and weather data in Beijing during the study period. There were a total of 26,653 IHD deaths (14,240 males and 12,413 females) from Jan 1 2008 to Dec 31 2009. The average daily deaths of IHD were about 40, with the most occurring in the winter months and the least in the summer, of which 17.7% were for <65 years old and 82.3% for ≥ 65 years old.
Table 1.
Summary statistics for PM 10 , spatially resolved PM 10 , SO 2 , NO 2 , daily mean temperature, daily mean relative humidity and daily IHD death counts in Beijing between 2008 and 2009
| Season | Min | 25% | Median | 75% | Max | Mean | SD | |
|---|---|---|---|---|---|---|---|---|
| PM10(μg/m3)*a | Spring | 7.0 | 80.0 | 124.0 | 184.0 | 600.0 | 144.5 | 96.3 |
| Summer | 5.0 | 64.0 | 98.0 | 134.0 | 463.2 | 101.4 | 52.2 | |
| Autumn | 7.0 | 54.0 | 94.0 | 148.0 | 553.0 | 110.1 | 75.9 | |
| Winter | 7.0 | 62.0 | 108.0 | 170.0 | 600.0 | 127.7 | 88.7 | |
| Overall | 5.0 | 64.0 | 104.0 | 150.0 | 600.0 | 120.8 | 81.6 | |
| Spatially resolved PM10(μg/m3)b | Spring | 13.1 | 84.9 | 125.4 | 186.7 | 593.1 | 147.6 | 93.4 |
| Summer | 17.3 | 69.0 | 98.8 | 1338 | 432.0 | 103.7 | 50.4 | |
| Autumn | 11.3 | 61.3 | 99.1 | 150.8 | 489.9 | 114.9 | 75.1 | |
| Winter | 13.2 | 61.6 | 96.9 | 144.4 | 600.0 | 114.9 | 78.8 | |
| Overall | 11.3 | 68.0 | 104.2 | 150.7 | 600.0 | 120.3 | 78.1 | |
| SO2(μg/m3) | Spring | 6 | 14.0 | 25.0 | 39.8 | 138 | 30.7 | 22.7 |
| Summer | 6 | 8.0 | 11.0 | 14.0 | 44 | 12.5 | 6.7 | |
| Autumn | 6 | 12.0 | 16.0 | 29.0 | 136 | 24.9 | 21.8 | |
| Winter | 10 | 39.3 | 72.0 | 102.0 | 202 | 75.7 | 42.3 | |
| Overall | 6 | 12.0 | 21.0 | 46.0 | 202 | 36.0 | 35.6 | |
| NO2(μg/m3) | Spring | 16 | 41.6 | 49.6 | 59.2 | 152 | 51.6 | 18.4 |
| Summer | 14.4 | 28.8 | 40.0 | 44.8 | 62.4 | 37.9 | 11.0 | |
| Autumn | 19.2 | 40.0 | 52.8 | 67.2 | 142.4 | 58.2 | 26.6 | |
| Winter | 9.6 | 40.0 | 59.2 | 80.6 | 140.8 | 60.6 | 25.9 | |
| Overall | 9.6 | 36.8 | 48.0 | 60.8 | 152 | 52.2 | 23.2 | |
| T(°C) | Spring | -0.1 | 10.0 | 15.6 | 20.6 | 26.8 | 15.2 | 6.5 |
| Summer | 17.5 | 24.3 | 26.0 | 28.0 | 31.6 | 26.0 | 2.7 | |
| Autumn | -2 | 7.1 | 15.1 | 19.9 | 25.4 | 13.4 | 7.6 | |
| Winter | -9.4 | -3.5 | -1.5 | 0.5 | 9.4 | -1.3 | 3.4 | |
| Overall | -9.4 | 2.3 | 15.4 | 23.55 | 31.6 | 13.4 | 11.1 | |
| RH(%) | Spring | 15 | 30.0 | 44.0 | 56.0 | 95 | 44.8 | 18.2 |
| Summer | 19 | 57.0 | 68.0 | 76.0 | 90 | 64.8 | 15.5 | |
| Autumn | 19 | 44.0 | 60.5 | 71.0 | 88 | 57.2 | 18.0 | |
| Winter | 11 | 24.0 | 38.0 | 53.0 | 82 | 39.8 | 17.4 | |
| Overall | 11 | 35 | 53 | 68 | 95 | 51.7 | 19.9 | |
| IHD(N) | Spring | 20 | 32.8 | 37 | 42 | 57 | 37.3 | 7.3 |
| Summer | 19 | 28 | 32 | 37 | 49 | 32.5 | 6.4 | |
| Autumn | 18 | 34 | 40 | 46 | 67 | 41.0 | 9.8 | |
| Winter | 29 | 43 | 49 | 55 | 75 | 49.1 | 8.4 | |
| Overall | 18 | 33 | 39 | 46 | 75 | 39.9 | 10.1 |
Note: PM10: Particulate matter with an aerodynamic diameter of <10 μm; SO2: sulfur dioxide; NO2: nitrogen dioxide; T: Temperature; RH: Relative humidity; IHD: Ischemic heart disease; N: Number of death.
*The maximum limit of detection for PM10 concentration is 600 μg/m3.
aRepresenting the average of the 27 monitoring stations.
bRepresenting the average of the 287 townships where health data was available.
The average temperature and relative humidity were 13.4 ± 11.1°C and 51.7 ± 19.9% during the study period. The mean values of SO2 and NO2 were 36.0 μg/m3 and 52.2 μg/m3, respectively. The air pollution levels varied across seasons. The mean daily SO2 level was higher in winter and spring than in autumn and summer while the mean daily NO2 level was higher in winter and autumn than in spring and summer.
In summary, the mean daily PM10 concentrations were 120.8 ± 81.6 μg/m3. There were higher PM10 concentrations in spring and winter than in autumn and summer. At 27 monitoring stations, the daily means of PM10 ranged from 72.6 μg/m3 to 144.9 μg/m3; 67.9% ~25.7% days had higher PM10 level than the China ambient air quality standard level-II (150 μg/m3) (Additional file 1: Table S1).The correlations in daily PM10 concentrations between stations were strong (Additional file 1: Table S2).
To estimate PM10 concentration more precisely, we adopted "leave-one-out" cross-validations to provide a more quantitative comparison of the interpolation methods (Additional file 1: Table S3). Every index of cross-validations indicated OK gave more accurate spatial PM10 estimates than IDW. The estimated PM10 using OK were strongly correlated with observed PM10, with the correlation coefficient ranging from 0.90 to 0.99 (P < 0.01). Generally, the differences between observed and spatially resolved PM10 were small.
The averaged spatially resolved PM10 concentration at 287 township-level areas was 120.3 ± 78.1 μg/m3, following the same trend in seasons as the observed PM10 levels. During the study period, the average daily PM10 concentration in the south of Beijing was higher than that in the north of Beijing (Figure 2).
Figure 2.
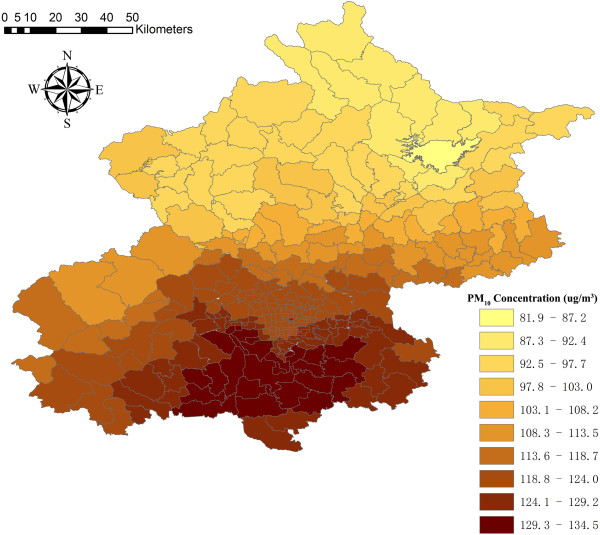
The averaged spatially resolved PM 10 concentrations at 304 towns in Beijing during 2008–2009.
The Spearman correlations between air pollutants and meteorological variables during the whole study were presented (Additional file 1: Table S4). PM10 was positively associated with other air pollutants and meteorological variables. The correlation between PM10 and NO2 (r = 0.55) was stronger than that between PM10 and SO2 (r = 0.43).
Figure 3 shows the association between PM10 and IHD mortality using spatially resolved PM10 concentrations. We observed statistically significant associations of daily IHD mortality with PM10 on the current day (lag 0), the previous day (lag 1), the moving average 2 days (lag 0–1) and the moving average 3 days (lag 0–2). We estimated an increase of 0.26% (95% CI: 0.09%, 0.43%), 0.23% (95% CI: 0.06%, 0.39%), 0.33% (95% CI: 0.13%, 0.52%) and 0.26% (95% CI: 0.04%, 0.47%) in IHD mortality associated with a 10-μg/m3 increase in PM10 at lag 0, lag 1, lag 0–1 and lag 0–2, respectively. The largest effects was observed for 2-day average.
Figure 3.
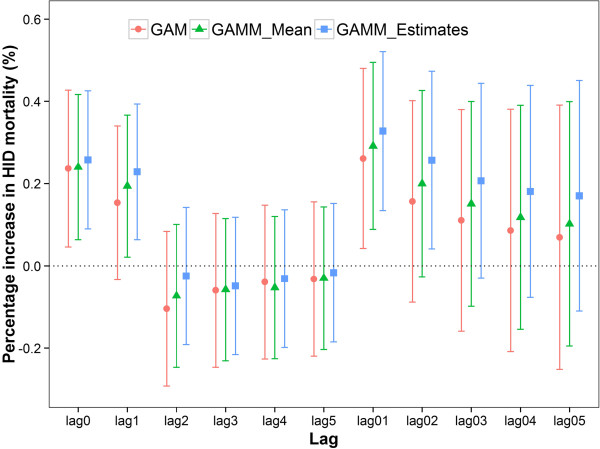
Percentage increase of IHD mortality associated with a 10-μg/m 3 increase in PM 10 concentration in Beijing, China. Note: GAM: Estimated effects in GAM using averaged PM10; GAMM_Mean: Estimated effects in GAMM using averaged PM10; GAMM_Estimates: Estimated effects in GAMM using spatially resolved PM10.
For the effects of averaged PM10 on IHD mortality, we also observed the largest effects at lag 0–1 using GAMM and GAM. However, the effect estimates were smaller and the confidence intervals were larger than those using spatially resolved PM10 (Figure 3).
In the two-pollutant model, the association of PM10 with IHD mortality was seen to be reduced at all lag patterns after adjustment for SO2 or NO2 (Figure 4), but still remained significant at lag 0–1 day.
Figure 4.
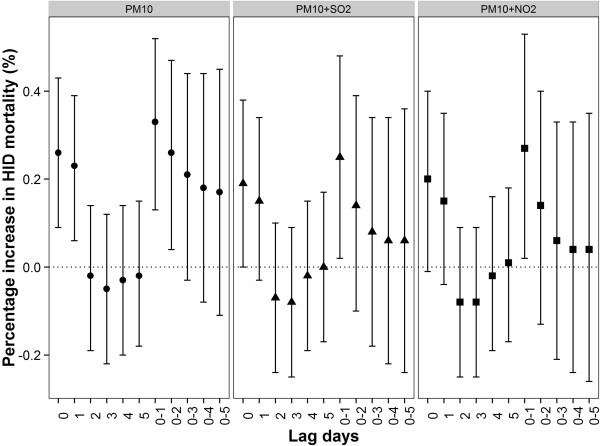
Percent increase in IHD mortality associated with a 10-μg/m 3 increase in PM 10 concentrations using the single- and two-pollutant models in GAMM.
The associations between PM10 and IHD mortality differed by season (Table 2). The effects of PM10 on IHD mortality were the strongest in summer, with a 10-μg/m3 increase associated with a 0.83% (95% CI: 0.31%, 1.35%), 0.88% (95% CI: 0.31%, 1.45%) increase of IHD mortality at lag 0–1 and lag 0–2 days, respectively. The differences of effect estimates between summer and spring as well as between summer and winter were statistically significant.
Table 2.
Percentage increase in IHD mortality associated with a 10-μg/m 3 increase in PM 10 concentrations by four seasons using the single-pollutant model in GAMM
| Lag | Season | Percent change (95% CI) |
|---|---|---|
| lag0 | Spring | 0.17(-0.07,0.40) |
| Summer | 0.60(0.13,1.06)* | |
| Autumn | 0.35(0.06,0.64)* | |
| Winter | 0.23(-0.06,0.51) | |
| lag1 | Spring | 0.19(-0.05,0.43) |
| Summer | 0.68(0.22,1.14)*b | |
| Autumn | 0.27(-0.01,0.56) | |
| Winter | 0.12(-0.16,0.41) | |
| lag2 | Spring | 0.03(-0.21,0.27) |
| Summer | 0.43(-0.03,0.90)b | |
| Autumn | -0.08(-0.37,0.21) | |
| Winter | -0.16(-0.44,0.12) | |
| lag01 | Spring | 0.24(-0.02,0.51) |
| Summer | 0.83(0.31,1.35)*a | |
| Autumn | 0.41(0.08,0.73)* | |
| Winter | 0.27(-0.06,0.60) | |
| lag02 | Spring | 0.22(-0.06,0.51) |
| Summer | 0.88(0.31,1.45)*ab | |
| Autumn | 0.29(-0.06,0.65) | |
| Winter | 0.14(-0.22,0.51) |
Note: *P < 0.05.
aThe difference of effect estimate between summer and spring was statistically significant (p < 0.05).
bThe difference of effect estimate between summer and winter was statistically significant (p < 0.05).
CI: confidence interval.
The association of PM10 with IHD mortality also varied by gender and age group (Figures 5 and 6). The largest effects of PM10 were observed on the current day for females and at lag 0–1 for males. The effect estimates of PM10 among females were higher than those among males on the current day while the effect estimates of PM10 among males were higher than those among females at lag 1 day and lag 0–1 days. However, the between-gender differences were not statistically significant. We observed the effect estimates among people aged ≥65 years were significant and approximately 3 times higher than those aged < 65 years at lag 0–1, but the differences of effect estimates between age groups were not statistically significant.
Figure 5.
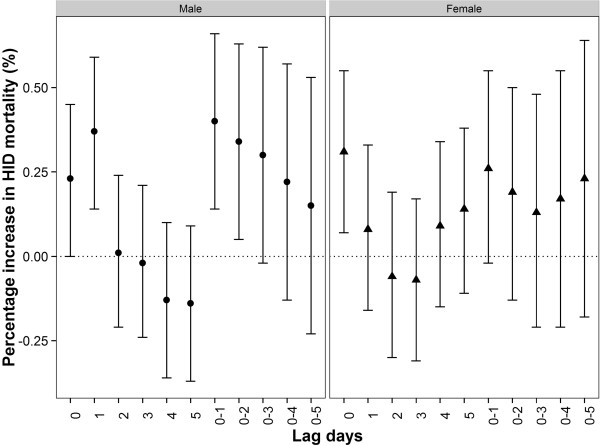
Percent increase (95% CI) in IHD mortality associated with a 10-μg/m 3 increase in PM 10 concentrations by sex using the single-pollutant model in GAMM.
Figure 6.
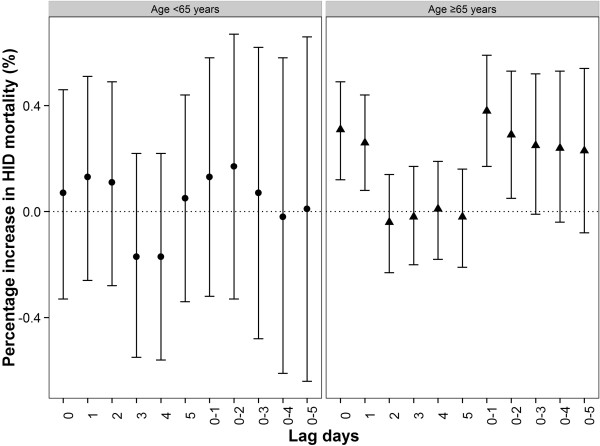
Percent increase (95% CI) in IHD mortality associated with a 10-μg/m 3 increase in PM 10 concentrations by age using the single-pollutant model in GAMM.
Sensitivity analysis was conducted to check our findings. Changing the degrees of freedom for time, temperature and relative humidity did not substantially affect the association of PM10 with IHD mortality. The effects estimates were hardly changed when 14-day moving average relative humidity was controlled in our model. These results suggested that our findings are statistically robust.
Discussion
We found that there were statistically significant associations between spatially resolved estimated PM10 mass concentration and increased risk of IHD death of the exposed population in Beijing, China. To our knowledge, it is the first time to use the spatiotemporal analysis method to examine the acute effects of ambient PM10 on IHD mortality, and also the first study to show spatial variation of ambient PM10 level in township-level of Beijing. We also examined whether the effect estimates varied by age, gender and season.
Studies [40, 41] have shown that the concentrations of air pollutants varied spatially across a specific area. Capturing the spatial variation using spatial modeling methods have been used to estimate air pollutants values from multiple monitor stations to the whole study region or exposure at the individual level. However, there was no consistent conclusions on which method was the best. Air pollution exposure estimates using spatial methods are affected by several factors, including the density and location of monitors and the available variables affecting air pollutants concentrations. Firstly, governmental monitor stations usually are placed in urban region, while fewer monitors are available in rural areas. This may result in misestimating the exposure in rural areas when using the values from nearby urban areas. Secondly, industrial and traffic emissions that may be more important in the urban areas, land use patterns and meteorological factors can influence the spatial and temporal distribution of air pollutants. Some models, such as land use regression model (LUR) [24, 42] and generalized addictive mix model (GAMM) [43–45] allowing for those variables, have been utilized to estimate the air pollutants exposure. Studies showed LUR or GAMM performed better than the conventional spatial interpolation methods (inverse distance weighting, nearest neighbor method or kriging) [43–47]. Those variables were unavailable in our study, so we are left only to estimate PM10 using the simple spatial interpolation methods. We found that the OK produced more accurate and less biased estimates than inverse distance weighting based on cross-validation results; therefore, we applied OK to interpolate PM10 concentrations over each township in Beijing.
Particulate matter may trigger ischemic heart disease through several possible mechanisms, including increasing inflammation [48], abnormal regulation of cardiac autonomic system [49], increasing blood viscosity [50] and vasoconstrictor such as endothelins [51]. Previous studies have reported inconsistent association between PM10 and ischemic heart disease mortality [10, 11, 52]. In our analysis, the largest effect was observed for 2-day average, with a 0.33% (95% CI: 0.13%, 0.52%) increase of IHD mortality per 10-μg/m3 increase of 2-day moving average PM10. The magnitude of our estimates was smaller than previous findings [10, 11] . For example, Li et al. [11] found IHD mortality increased by 0.53% (95% CI: 0.30%, 0.84%) for a 10 μg/m3 increment PM10 on the same day in Tianjin. However, in Netherlands, Hoek et al. [52] did not observed statistically significant association between PM10 and IHD mortality. The heterogeneity of these findings may be explained by the different characteristics of the study sites such as PM10 level, components of PM10, sensitivity of local residents to PM10, indoor air pollution, weather patterns [53, 54]. In addition, the df selection decisions and the different lag patterns in GAM and the number of study years could affect the estimated effects [55, 56].
Our study observed harvesting effects although the effects have no statistically significance. This means that PM10 may hasten the deaths of persons who were extremely frail. But the effect sizes of PM10 rebound because PM10 could exacerbate ischemic heart disease [57], potentially increasing the number of sensitive persons whose illness is life threatening.
Consistent with previous reports [15, 58], we found that the effect estimates using spatially resolved PM10 were larger than that using averaged PM10 from multiple stations. This suggested that previous time-series studies using the average levels may underestimate the effects of PM10. Although the effects difference using different exposure metrics was not too large, it still needs be considered especially in cities with large spatial variation of air pollutants and cannot be ignored because the association between air pollution and mortality itself was weak.
In the two-pollutant models, the associations between PM10 and IHD mortality adjusting for SO2 or NO2 were attenuated and become insignificant at some lag patterns, which may be caused by the collinearity between PM10 and NO2 as well as SO2 (Additional file 1: Table S4). The findings are consistent with previous studies [58]. So far it is still an unresolved scientific question to separate the independent effects of individual air pollutant from multiple-pollutant models in short-term effects studies of air pollution. Moreover, in order to better examine the effects of spatial resolved PM10 in multiple-pollutant model, the other air pollutants also needed to be estimated spatially because between-pollutant relationships may not be characterized well just by the averaged value in one area. Further studies are needed to resolve these problems.
Seasonal differences in the short-term effects of PM10 on IHD mortality were found in this study. The association in the summer period was stronger than in the other seasons. Li et al. [11] also identified the strongest effects of PM10 on IHD mortality in summer in Tianjin, China. However, Chen et al. [59] observed the largest estimates of PM10 on daily mortality in winter and summer in northern cities of China which have similar meterological conditions to Beijing. There are several explanations for the inconsistent findings in the studies. Firstly, the particulate matter constituents may vary by season in these cities. We cannot obtain the data of the PM10 components, which hinders further study on how the different particulate matter constituents affect the effects by season. In additional, socioeconomic characteristics, activity patterns of local residents and statistical models used could partially account for the discrepant finding.
We found the effect estimate of PM10 on IHD mortality in females was larger than those in males on the current day. This suggested that females were more sensitive to PM10, which was possibly due to higher airway hyper-responsiveness to oxidants, more deposition of fine particles or relatively lower socioeconomic status [54]. The larger lag effects in males may be partly explained by the higher incidence of heart disease in males than in females, particularly pre-menopausal females. Studies have shown that biological factors, such as hormone levels, help protect women against heart disease [60].
Our study also found the elderly were more susceptible to PM10 exposure than the younger group. This is consistent with previous reports [54, 61]. Preexisting chronic disease such as cardiorespiratory disease in the elderly are more prevalent than in the younger group.
This study has several limitations. Firstly, we cannot obtain daily data on SO2, NO2, temperature and relative humidity from multiple stations, so the township-based spatial distributions of the covariates cannot be estimated. Consequently, we did not control for the spatial variation of these variable in our model, which may result in a bias in effect estimates. Secondly, our exposure assignment approach assumed that the subjects lived and worked at the same township, and considered outdoor air concentrations at the centroid of the corresponding township as personal exposure, which might result in exposure misclassification. Thirdly, studies have shown that exposure measurement error may affect the effect estimations when exposure predictions as explanatory variables are incorporated into a regression model for health effects analyses [62, 63]. The exposure measurement error contains a Berkson-like component that increases the variance of the effect estimate and a classical-type component that not only increase the variance but also bias the effect estimates [64]. Szpiro and his colleagues developed a method for measurement error correction based on asymptotic approximations that derived for linear regression for the exposure and health models [64, 65]. To date, there has been no methods for measurement error correction used in the nonlinear regression models and assessing health effects of multiple predicted pollutants exposure [65]. Thus, we did not correct the measurement error in our study, which may have an impact on the effect estimates.
Conclusions
Ambient PM10 concentration was statistically significant associated with IHD mortality of the population in spatiotemporal analysis in Beijing, China. The stronger association occurred for the 2-day average. Season, gender and age appear to modify the effects of PM10 on IHD mortality. GAMM considering spatial variations of ambient PM10 produced greater effect estimates than GAM using averaged PM10 concentrations. It implies that spatial variation should be considered for assessing the impacts of air pollution on mortality. Our findings may have implication for primary prevention of IHD deaths in China and guiding future work on more advanced methods of estimated exposure and health effects.
Electronic supplementary material
Additional file 1: Table S1: Summary statistics for daily PM10 (μg/m3) at 27 monitoring stations in Beijing, China between 2008 and 2009 (see Figure 1 for the locations). Table S2 Spearman correlations between daily PM10 concentrations at 27 monitoring stations in Beijing city between 2008 and 2009. Table S3 The comparison between the predicted and observed PM10 concentrations using different interpolation methods at 27 monitoring stations during 2008-2009. Table S4 The correlation between pollutants and meteorological variables. (DOC 164 KB)
Acknowledgment
This study was funded by the National Natural Science Foundation of China (#81273033).We thank the China Centers for Disease Control and Prevention, Beijing Municipal Environmental Protection Bureau, China Meteorological Data Sharing Service System and Institute of Geographic Sciences and Natural Resources Research, Chinese Academy of Sciences for providing the data.
Abbreviations
- PM10
Particulate matter with an aerodynamic diameter of <10 μm
- GAM
Generalized additive model
- GAMM
Generalized additive mixed model
- CI
Confidence interval
- ICD-10
International classification of diseases 10th version
- CDC
China centers for disease control and prevention
- SO2
Sulfur dioxide
- NO2
Nitrogen dioxide
- T
Temperature
- RH
Relative humidity
- SD
Standard deviation
- df
Degree of freedom
- IDW
Inverse distance weighting
- OK
Ordinary Kriging
- LOOCV
Leave-one-out cross-validation
- DOW
Day of the week
- RMSE
Root-mean-square error.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MX designed the study and directed its implementation, including data analysis, writing the paper, and quality assurance and control. YG, YZ and YM helped analyze the data. XP and DW reviewed and helped edit the paper, FL helped prepare the database and conduct the data quality assurance. All authors read and approved the final manuscript.
Contributor Information
Meimei Xu, Email: xumeimei2005@163.com.
Yuming Guo, Email: y.guo1@uq.edu.au.
Yajuan Zhang, Email: zhyj830515@126.com.
Dane Westerdahl, Email: danewest03@gmail.com.
Yunzheng Mo, Email: moyunzheng@gmail.com.
Fengchao Liang, Email: liangfengchao126@126.com.
Xiaochuan Pan, Email: xcpan@hsc.pku.edu.cn.
References
- 1.Ockene J. Relationship between baseline risk factors and coronary heart disease and total mortality in the Multiple Risk Factor Intervention Trial. Multiple Risk Factor Intervention Trial Research Group. Prev Med. 1986;15:254–273. doi: 10.1016/0091-7435(86)90045-9. [DOI] [PubMed] [Google Scholar]
- 2.Wilson PW, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162:1867–1872. doi: 10.1001/archinte.162.16.1867. [DOI] [PubMed] [Google Scholar]
- 3.Yusuf HR, Giles WH, Croft JB, Anda RF, Casper ML. Impact of multiple risk factor profiles on determining cardiovascular disease risk. Prev Med. 1998;27:1–9. doi: 10.1006/pmed.1997.0268. [DOI] [PubMed] [Google Scholar]
- 4.Evans J, van Donkelaar A, Martin RV, Burnett R, Rainham DG, Birkett NJ, Krewski D. Estimates of global mortality attributable to particulate air pollution using satellite imagery. Environ Res. 2013;120:33–42. doi: 10.1016/j.envres.2012.08.005. [DOI] [PubMed] [Google Scholar]
- 5.Balluz L, Wen XJ, Town M, Shire JD, Qualter J, Mokdad A. Ischemic heart disease and ambient air pollution of particulate matter 2.5 in 51 counties in the U.S. Public Health Rep. 2007;122:626–633. doi: 10.1177/003335490712200510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Breitner S, Liu L, Cyrys J, Bruske I, Franck U, Schlink U, Leitte AM, Herbarth O, Wiedensohler A, Wehner B, Hu M, Pan XC, Wichmann HE, Peters A. Sub-micrometer particulate air pollution and cardiovascular mortality in Beijing, China. Sci Total Environ. 2011;409:5196–5204. doi: 10.1016/j.scitotenv.2011.08.023. [DOI] [PubMed] [Google Scholar]
- 7.Pope CR, Muhlestein JB, May HT, Renlund DG, Anderson JL, Horne BD. Ischemic heart disease events triggered by short-term exposure to fine particulate air pollution. Circulation. 2006;114:2443–2448. doi: 10.1161/CIRCULATIONAHA.106.636977. [DOI] [PubMed] [Google Scholar]
- 8.Schwartz J, Morris R. Air pollution and hospital admissions for cardiovascular disease in Detroit, Michigan. Am J Epidemiol. 1995;142:23–35. doi: 10.1093/oxfordjournals.aje.a117541. [DOI] [PubMed] [Google Scholar]
- 9.Lee JT, Kim H, Cho YS, Hong YC, Ha EH, Park H. Air pollution and hospital admissions for ischemic heart diseases among individuals 64+ years of age residing in Seoul, Korea. Arch Environ Health. 2003;58:617–623. doi: 10.3200/AEOH.58.10.617-623. [DOI] [PubMed] [Google Scholar]
- 10.Wong TW, Tam WS, Yu TS, Wong AH. Associations between daily mortalities from respiratory and cardiovascular diseases and air pollution in Hong Kong, China. Occup Environ Med. 2002;59:30–35. doi: 10.1136/oem.59.1.30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li G, Zhou M, Zhang Y, Cai Y, Pan X. Seasonal effects of PM10 concentrations on mortality in Tianjin, China: a time-series analysis. J Public Health. 2013;21:135–144. doi: 10.1007/s10389-012-0529-4. [DOI] [Google Scholar]
- 12.Chang G, Pan X, Xie X, Gao Y. Time-series analysis on the relationship between air pollution and daily mortality in Beijing. Wei Sheng Yan Jiu. 2003;32:565–568. [PubMed] [Google Scholar]
- 13.Ito K, Kinney PL, Thurston GD. Variations in PM-10 Concentrations Within two Metropolitan Areas and Their Implications for Health Effects Analyses. Inhal Toxicol. 1995;7:735–745. doi: 10.3109/08958379509014477. [DOI] [Google Scholar]
- 14.Sarnat SE, Sarnat JA, Mulholland J, Isakov V, Ozkaynak H, Chang HH, Klein M, Tolbert PE. Application of alternative spatiotemporal metrics of ambient air pollution exposure in a time-series epidemiological study in Atlanta. J Expo Sci Environ Epidemiol. 2013;23:593–605. doi: 10.1038/jes.2013.41. [DOI] [PubMed] [Google Scholar]
- 15.Chen L, Mengersen K, Tong S. Spatiotemporal relationship between particle air pollution and respiratory emergency hospital admissions in Brisbane, Australia. Sci Total Environ. 2007;373:57–67. doi: 10.1016/j.scitotenv.2006.10.050. [DOI] [PubMed] [Google Scholar]
- 16.Wong DW, Yuan L, Perlin SA. Comparison of spatial interpolation methods for the estimation of air quality data. J Expo Anal Environ Epidemiol. 2004;14:404–415. doi: 10.1038/sj.jea.7500338. [DOI] [PubMed] [Google Scholar]
- 17.Moore DK, Jerrett M, Mack WJ, Kunzli N. A land use regression model for predicting ambient fine particulate matter across Los Angeles, CA. J Environ Monit. 2007;9:246–252. doi: 10.1039/b615795e. [DOI] [PubMed] [Google Scholar]
- 18.Lee D, Shaddick G. Spatial modeling of air pollution in studies of its short-term health effects. Biometrics. 2010;66:1238–1246. doi: 10.1111/j.1541-0420.2009.01376.x. [DOI] [PubMed] [Google Scholar]
- 19.Jerrett M, Burnett RT, Ma R, Pope CR, Krewski D, Newbold KB, Thurston G, Shi Y, Finkelstein N, Calle EE, Thun MJ. Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology. 2005;16:727–736. doi: 10.1097/01.ede.0000181630.15826.7d. [DOI] [PubMed] [Google Scholar]
- 20.Jerrett M, Arain A, Kanaroglou P, Beckerman B, Potoglou D, Sahsuvaroglu T, Morrison J, Giovis C. A review and evaluation of intraurban air pollution exposure models. J Expo Anal Environ Epidemiol. 2005;15:185–204. doi: 10.1038/sj.jea.7500388. [DOI] [PubMed] [Google Scholar]
- 21.Son JY, Bell ML, Lee JT. Individual exposure to air pollution and lung function in Korea: spatial analysis using multiple exposure approaches. Environ Res. 2010;110:739–749. doi: 10.1016/j.envres.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 22.Chen L, Baili Z, Kong S, Han B, You Y, Ding X, Du S, Liu A. A land use regression for predicting NO2 and PM10 concentrations in different seasons in Tianjin region, China. J Environ Sci (China) 2010;22:1364–1373. doi: 10.1016/S1001-0742(09)60263-1. [DOI] [PubMed] [Google Scholar]
- 23.Zhang A, Qi Q, Jiang L, Zhou F, Wang J. Population exposure to PM2.5 in the urban area of Beijing. PLoS One. 2013;8:e63486. doi: 10.1371/journal.pone.0063486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li L, Losser T, Yorke C, Piltner R. Fast inverse distance weighting-based spatiotemporal interpolation: a web-based application of interpolating daily fine particulate matter PM2:5 in the contiguous U.S. using parallel programming and k-d tree. Int J Environ Res Public Health. 2014;11:9101–9141. doi: 10.3390/ijerph110909101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Coull BA, Schwartz J, Wand MP. Respiratory health and air pollution: additive mixed model analyses. Biostatistics. 2001;2:337–349. doi: 10.1093/biostatistics/2.3.337. [DOI] [PubMed] [Google Scholar]
- 26.Lin X, Zhang D. Inference in generalized additive mixed modelsby using smoothing splines. Journal of the Royal Statistical Society: Series B (Statistical Methodology) 1999;61:381–400. doi: 10.1111/1467-9868.00183. [DOI] [Google Scholar]
- 27.Breslow NE, Clayton DG. Approximate inference in generalized linear mixed models. J Am Stat Assoc. 1993;88:9–25. [Google Scholar]
- 28.Likhvar V, Honda Y, Ono M. Relation between temperature and suicide mortality in Japan in the presence of other confounding factors using time-series analysis with a semiparametric approach. Environ Health Prev Med. 2011;16:36–43. doi: 10.1007/s12199-010-0163-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ruppert D, Wand MP, Carroll RJ. Semiparametric Regression. New York: Cambridge University Press; 2003. [Google Scholar]
- 30.Guo Y, Barnett AG, Tong S. Spatiotemporal model or time series model for assessing city-wide temperature effects on mortality? Environ Res. 2013;120:55–62. doi: 10.1016/j.envres.2012.09.001. [DOI] [PubMed] [Google Scholar]
- 31.Qian Z, Lin HM, Stewart WF, Kong L, Xu F, Zhou D, Zhu Z, Liang S, Chen W, Shah N, Stetter C, He Q. Seasonal pattern of the acute mortality effects of air pollution. J Air Waste Manag Assoc. 2010;60:481–488. doi: 10.3155/1047-3289.60.4.481. [DOI] [PubMed] [Google Scholar]
- 32.Ma W, Chen R, Kan H. Temperature-related mortality in 17 large Chinese cities: How heat and cold affect mortality in China. Environ Res. 2014;134C:127–133. doi: 10.1016/j.envres.2014.07.007. [DOI] [PubMed] [Google Scholar]
- 33.Guo Y, Barnett AG, Pan X, Yu W, Tong S. The impact of temperature on mortality in Tianjin, China: a case-crossover design with a distributed lag nonlinear model. Environ Health Perspect. 2011;119:1719–1725. doi: 10.1289/ehp.1103598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Guo Y, Li S, Tawatsupa B, Punnasiri K, Jaakkola JJ, Williams G. The association between air pollution and mortality in Thailand. Sci Rep. 2014;4:5509. doi: 10.1038/srep05509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Chen R, Cai J, Meng X, Kim H, Honda Y, Guo YL, Samoli E, Yang X, Kan H. Ozone and daily mortality rate in 21 cities of East Asia: how does season modify the association? Am J Epidemiol. 2014;180:729–736. doi: 10.1093/aje/kwu183. [DOI] [PubMed] [Google Scholar]
- 36.Samet JM, Zeger SL, Dominici F, Curriero F, Coursac I, Dockery DW, Schwartz J, Zanobetti A. The National Morbidity, Mortality, and Air Pollution Study. Part II: Morbidity and mortality from air pollution in the United States. Res Rep Health Eff Inst. 2000;94(Pt 2):5–70. [PubMed] [Google Scholar]
- 37.Chen R, Samoli E, Wong CM, Huang W, Wang Z, Chen B, Kan H. Associations between short-term exposure to nitrogen dioxide and mortality in 17 Chinese cities: the China Air Pollution and Health Effects Study (CAPES) Environ Int. 2012;45:32–38. doi: 10.1016/j.envint.2012.04.008. [DOI] [PubMed] [Google Scholar]
- 38.Wong CM, Vichit-Vadakan N, Kan H, Qian Z. Public Health and Air Pollution in Asia (PAPA): a multicity study of short-term effects of air pollution on mortality. Environ Health Perspect. 2008;116:1195–1202. doi: 10.1289/ehp.11257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ. 2003;326:219. doi: 10.1136/bmj.326.7382.219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Levy JI, Hanna SR. Spatial and temporal variability in urban fine particulate matter concentrations. Environ Pollut. 2011;159:2009–2015. doi: 10.1016/j.envpol.2010.11.013. [DOI] [PubMed] [Google Scholar]
- 41.Burton RM, Suh HH, Koutrakis P. Spatial variation in particulate concentrations within Metropolitan Philadelphia. Environ Sci Technol. 1996;30:400–407. doi: 10.1021/es950030f. [DOI] [Google Scholar]
- 42.Cesaroni G, Porta D, Badaloni C, Stafoggia M, Eeftens M, Meliefste K, Forastiere F. Nitrogen dioxide levels estimated from land use regression models several years apart and association with mortality in a large cohort study. Environ Health. 2012;11:48. doi: 10.1186/1476-069X-11-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Yanosky JD, Paciorek CJ, Suh HH. Predicting chronic fine and coarse particulate exposures using spatiotemporal models for the Northeastern and Midwestern United States. Environ Health Perspect. 2009;117:522–529. doi: 10.1289/ehp.11692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Yanosky JD, Paciorek CJ, Schwartz J, Laden F, Puett R, Suh HH. Spatio-temporal modeling of chronic PM10 exposure for the Nurses’ Health Study. Atmos Environ. 2008;42:4047–4062. doi: 10.1016/j.atmosenv.2008.01.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Hart JE, Yanosky JD, Puett RC, Ryan L, Dockery DW, Smith TJ, Garshick E, Laden F. Spatial modeling of PM10 and NO2 in the continental United States, 1985-2000. Environ Health Perspect. 2009;117:1690–1696. doi: 10.1289/ehp.0800503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Briggs DJ, de Hoogh C, Gulliver J, Wills J, Elliott P, Kingham S, Smallbone K. A regression-based method for mapping traffic-related air pollution: application and testing in four contrasting urban environments. Sci Total Environ. 2000;253:151–167. doi: 10.1016/S0048-9697(00)00429-0. [DOI] [PubMed] [Google Scholar]
- 47.Pouliou T, Kanaroglou PS, Elliott SJ, Pengelly LD. Assessing the health impacts of air pollution: a re-analysis of the Hamilton children’s cohort data using a spatial analytic approach. Int J Environ Health Res. 2008;18:17–35. doi: 10.1080/09603120701844290. [DOI] [PubMed] [Google Scholar]
- 48.Pope CR, Hansen ML, Long RW, Nielsen KR, Eatough NL, Wilson WE, Eatough DJ. Ambient particulate air pollution, heart rate variability, and blood markers of inflammation in a panel of elderly subjects. Environ Health Perspect. 2004;112:339–345. doi: 10.1289/ehp.6588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Whitsel EA, Quibrera PM, Christ SL, Liao D, Prineas RJ, Anderson GL, Heiss G. Heart rate variability, ambient particulate matter air pollution, and glucose homeostasis: the environmental epidemiology of arrhythmogenesis in the women’s health initiative. Am J Epidemiol. 2009;169:693–703. doi: 10.1093/aje/kwn400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Peters A, Doring A, Wichmann HE, Koenig W. Increased plasma viscosity during an air pollution episode: a link to mortality? Lancet. 1997;349:1582–1587. doi: 10.1016/S0140-6736(97)01211-7. [DOI] [PubMed] [Google Scholar]
- 51.Bouthillier L, Vincent R, Goegan P, Adamson IY, Bjarnason S, Stewart M, Guenette J, Potvin M, Kumarathasan P. Acute effects of inhaled urban particles and ozone: lung morphology, macrophage activity, and plasma endothelin-1. Am J Pathol. 1998;153:1873–1884. doi: 10.1016/S0002-9440(10)65701-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hoek G, Brunekreef B, Fischer P, van Wijnen J. The association between air pollution and heart failure, arrhythmia, embolism, thrombosis, and other cardiovascular causes of death in a time series study. Epidemiology. 2001;12:355–357. doi: 10.1097/00001648-200105000-00017. [DOI] [PubMed] [Google Scholar]
- 53.Samet JM. Air pollution risk estimates: determinants of heterogeneity. J Toxicol Environ Health A. 2008;71:578–582. doi: 10.1080/15287390801997666. [DOI] [PubMed] [Google Scholar]
- 54.Kan H, London SJ, Chen G, Zhang Y, Song G, Zhao N, Jiang L, Chen B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ Health Perspect. 2008;116:1183–1188. doi: 10.1289/ehp.10851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Peng RD, Dominici F, Louis TA. Model choice in time series studies of air pollution and mortality. Journal of the Royal Statistical Society: Series A (Statistics in Society) 2006;169:179–203. doi: 10.1111/j.1467-985X.2006.00410.x. [DOI] [Google Scholar]
- 56.Chen R, Zhang Y, Yang C, Zhao Z, Xu X, Kan H. Acute effect of ambient air pollution on stroke mortality in the China air pollution and health effects study. Stroke. 2013;44(4):954–960. doi: 10.1161/STROKEAHA.111.673442. [DOI] [PubMed] [Google Scholar]
- 57.Peters A, Dockery DW, Muller JE, Mittleman MA. Increased particulate air pollution and the triggering of myocardial infarction. Circulation. 2001;103:2810–2815. doi: 10.1161/01.CIR.103.23.2810. [DOI] [PubMed] [Google Scholar]
- 58.Zhang Y, Guo Y, Li G, Zhou J, Jin X, Wang W, Pan X. The spatial characteristics of ambient particulate matter and daily mortality in the urban area of Beijing, China. Sci Total Environ. 2012;435–436:14–20. doi: 10.1016/j.scitotenv.2012.06.092. [DOI] [PubMed] [Google Scholar]
- 59.Chen R, Peng RD, Meng X, Zhou Z, Chen B, Kan H. Seasonal variation in the acute effect of particulate air pollution on mortality in the China Air Pollution and Health Effects Study (CAPES) Sci Total Environ. 2013;450–451:259–265. doi: 10.1016/j.scitotenv.2013.02.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Jousilahti P, Vartiainen E, Tuomilehto J, Puska P. Sex, age, cardiovascular risk factors, and coronary heart disease: a prospective follow-up study of 14 786 middle-aged men and women in Finland. Circulation. 1999;99:1165–1172. doi: 10.1161/01.CIR.99.9.1165. [DOI] [PubMed] [Google Scholar]
- 61.Zeka A, Zanobetti A, Schwartz J. Individual-level modifiers of the effects of particulate matter on daily mortality. Am J Epidemiol. 2006;163:849–859. doi: 10.1093/aje/kwj116. [DOI] [PubMed] [Google Scholar]
- 62.Basagana X, Aguilera I, Rivera M, Agis D, Foraster M, Marrugat J, Elosua R, Kunzli N. Measurement error in epidemiologic studies of air pollution based on land-use regression models. Am J Epidemiol. 2013;178:1342–1346. doi: 10.1093/aje/kwt127. [DOI] [PubMed] [Google Scholar]
- 63.Gryparis A, Paciorek CJ, Zeka A, Schwartz J, Coull BA. Measurement error caused by spatial misalignment in environmental epidemiology. Biostatistics. 2009;10:258–274. doi: 10.1093/biostatistics/kxn033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Szpiro AA, Sheppard L, Lumley T. Efficient measurement error correction with spatially misaligned data. Biostatistics. 2011;12:610–623. doi: 10.1093/biostatistics/kxq083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Szpiro AA, Paciorek CJ. Measurement error in two-stage analyses, with application to air pollution epidemiology. Environmetrics. 2013;24:501–517. doi: 10.1002/env.2233. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1: Summary statistics for daily PM10 (μg/m3) at 27 monitoring stations in Beijing, China between 2008 and 2009 (see Figure 1 for the locations). Table S2 Spearman correlations between daily PM10 concentrations at 27 monitoring stations in Beijing city between 2008 and 2009. Table S3 The comparison between the predicted and observed PM10 concentrations using different interpolation methods at 27 monitoring stations during 2008-2009. Table S4 The correlation between pollutants and meteorological variables. (DOC 164 KB)