

Abstract
Purpose
We examined the efficacy of an extended-release drug delivery system, nanosponge (NS) encapsulated compounds, administered intravitreally to lower intraocular pressure (IOP) in mice.
Methods
Bilateral ocular hypertension was induced in mice by injecting microbeads into the anterior chamber. Hypertensive mice received NS loaded with ocular hypotensive drugs via intravitreal injection and IOP was monitored. Retinal deposition and retinal ganglion cell (RGC) uptake of Neuro-DiO were examined following intravitreal injection of Neuro-DiO-NS using confocal microscopy.
Results
Brimonidine-loaded NS lowered IOP 12% to 30% for up to 6 days (P < 0.02), whereas travoprost-NS lowered IOP 19% to 29% for up to 4 days (P < 0.02) compared to saline injection. Three bimatoprost NS were tested: a 400-nm NS and two 700-nm NS with amorphous (A-NS) or amorphous/crystalline (AC-NS) crosslinkers. A single injection of 400 nm NS lowered IOP 24% to 33% for up to 17 days compared to saline, while A-NS and AC-NS lowered IOP 22% to 32% and 18% to 26%, respectively, for up to 32 days (P < 0.046). Over time retinal deposition of Neuro-DiO increased from 19% to 71%; Neuro-DiO released from NS was internalized by RGCs.
Conclusions
A single injection of NS can effectively deliver ocular hypotensive drugs in a linear and continuous manner for up to 32 days. Also, NS may be effective at targeting RGCs, the neurons that degenerate in glaucoma.
Translational Relevance
Patient compliance is a major issue in glaucoma. The use of NS to deliver a controlled, sustained release of therapeutics could drastically reduce the number of patients that progress to vision loss in this disease.
Keywords: Glaucoma, Nanoparticle, Neuroprotection
Introduction
Glaucoma is a chronic disease that results in vision loss as retinal ganglion cell (RGC) neurons and their axons in the optic nerve degenerate over time.1,2 Globally, glaucoma is the leading cause of irreversible blindness, and the second leading cause of blindness behind cataract.3 As of 2010, an estimated 60 million people worldwide had glaucoma, a number that will reach almost 80 million by 2020. Of those 80 million people, 11.2 million will be blind by 2020.3 Glaucoma patients face not only a decline in their quality of life, but a large economic burden as well. A recent study estimated Medicare paid out $748 million in total glaucoma-related payments in 2009.4 As the diseases progresses, medical costs for glaucoma patients rise. Annual eye care–related costs for glaucoma patients with no vision loss were $8157 (2007 US dollars); this increased to $14,237 for moderate to severe vision loss before reaching $18,670 for patients blinded by the disease.5
A major risk factor for glaucoma is age; however, the only modifiable risk factor – and the sole target for clinical intervention – is elevated intraocular pressure (IOP).6 First line treatment for glaucoma is the use of topical eye drops containing IOP-lowering drugs.7 While lowering IOP can slow disease progression, it does not necessarily prevent RGC degeneration.6,8 In fact, glaucomatous progression may continue in as many as 50% of glaucoma patients on a regimen to lower IOP.9 Poor patient compliance likely contributes to this continued progression.10–14 Factors that influence adherence to glaucoma therapy include visual impairment, total number of medications a patient is taking, the number of doses per day, time of day doses are taken, poor health literacy (understanding of the disease), and substandard doctor-patient communication.11,13–18 An association between patient compliance and glaucoma progression has been observed, with noncompliant patients showing higher ocular pressures, greater disc cupping, and increased visual field loss compared to compliant patients.13
Multiple strategies have been used to increase compliance in glaucoma patients; however, poor drug adherence remains a major barrier to treatment.15,17,19–23 To address this issue and improve clinical outcomes, delivery systems for glaucoma drugs are being developed that would ideally provide prolonged drug effects while decreasing systemic exposure, side effects, and patient discomfort (reviewed by Knight and Lawrence24). A recent study by Chong et al.25 determined the willingness of patients to accept intraocular injections in lieu of current glaucoma therapies. More than 74% of the patients interviewed were willing to receive subconjunctival injection every three months.25 This treatment plan is not unheard of; intraocular injection of vascular endothelial growth factor inhibitors to treat age-related macular degeneration (AMD) has emerged as a major therapeutic breakthrough for these patients.26–28 A study of over 500 patients receiving intraocular injections to treat AMD showed that 31% of these patients were still receiving injections 4 years later, and showed no loss of visual acuity and very few ocular complications over this time frame.29
Recently, nanoparticles have been used for targeted drug delivery in chemotherapeutics and their use in the treatment of other diseases, such as Alzheimer's disease, inflammatory intestinal disease, and lupus, has been promising.30–35 Given the issues with patient compliance in glaucoma, the use of nanoparticles to deliver a controlled, sustained release of therapeutics to the retina or other ocular structures via topical drops, contact lenses, and intravitreal injection could drastically reduce the number of patients who have progression to vision loss in this disease.36–39 To address the need for extended-release treatments that minimize patient nonadherence and discomfort, we examined the efficacy of four types of nanoparticle-encapsulated compounds, or nanosponges (NS), administered intravitreally to lower IOP in mice with microbead-induced ocular hypertension. A series consisting of organic, fully degradable polyester NS differing in their nanoscopic size dimension (50, 400, and 700 nm) and crosslinking density (7% and 14%) were synthesized to create a polymeric network for ocular hypotensive drug entrapment and to influence release and solubility in the physiological environment. Moreover, the chemical nature of the crosslinker used to create the polymeric network was increased in its crystallinity in the 700 nm particle and was added as a third parameter of variation to study the effect on IOP in mice. Finally, we also encapsulated Neuro-DiO dye to study the fate of a therapeutic with regard to uptake and delivery within the retina.
Materials and Methods
Animals and Induction of Acute Ocular Hypertension
This study was conducted in accordance with regulations set forth in the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research. All experimental procedures were approved by the Vanderbilt University Medical Center Institutional Animal Care and Use Committee. The C57BL/6 (C57) mice were obtained from Jackson Laboratories (Bar Harbor, ME) and were maintained in a 12-hour light/dark cycle with standard rodent chow available ad libitum as described.40,41 Ocular hypertension was induced bilaterally in C57 mice by injecting 1.5 μL of polystyrene microbeads (15 μm, 1 × 106 microbeads/mL solution; Molecular Probes, Eugene, OR) into the anterior chamber of both eyes as described previously.41 Using this model, we induced ocular pressure elevations of 30% for 23 days and 33% for 36 days in C57 mice following one 1.0 μL injection.41,42 Injection of 1.5 μL of microbeads in C57 mice has produced ocular pressure elevations of 31% to 34% for up to 7 weeks.43 The IOP was measured in anesthetized mice using a Tono-Pen (Reichert, Inc., Depew, NY) as described.
NS Generation
The series of the NSs were prepared by a one-pot procedure in which a linear polymer precursor with pendant epoxide groups is crosslinked with a difunctional diamine PEG crosslinker or with a difunctional diaminooctane crosslinker for one of the 700 nm NS.44
Nanoparticle Size Characterization
The nanoparticle size was obtained via transmission electron microscopy (TEM). Samples for TEM imaging were prepared by dissolving 0.5 mg nanoparticles in 1 mL isopropanol, 0.4 mL acetonitrile. The samples were sonicated for 5 minutes and were stained with 5 drops of 3% phosphotungstic acid. The carbon grids were prepared by slowly dipping an Ultrathin Carbon Type-A 400 Mesh Copper Grid (Ted Pella, Inc., Redding, CA) into the particle solutions three times and drying the grid at ambient temperature. A Philips CM20T transmission electron microscope operating at 200 kV in bright-field mode was used for detection of the nanoparticles.
50 nm Nanosponges with 7% Crosslinking
To a 100-mL round bottom flask equipped with a stir bar, poly(vl-evl) (0.1001 g, Mw = 2350 Da, 7% cross-linking) and 20.2 mL CH2Cl2 were added, followed by 2,2′-(ethylenedioxy)diethylamine (9.6 μL, 6.55 × 10−5 mol). The mixture was refluxed at 44°C for 12 hours and promptly transferred to SnakeSkin Pleated Dialysis Tubing (molecular weight cutoff [MWCO] = 10,000; Thermo Fisher Scientific, Waltham, MA) and dialyzed against dichloromethane to remove residual diamine. 1H NMR (400MHz), CDCl3/TMS, ppm) δ: The significant change, proving conversion from the linear polymer to the nanoparticle, is the disappearance of epoxide protons at 2.96, 2.75, and 2.47 ppm and the appearance of signals at 3.5 and 2.9 ppm due to the protons near the secondary amine of the PEG linker. The spectrum is otherwise similar in all aspects.
400 nm Nanosponges with 13% Crosslinking
To a 200-mL round bottom flask equipped with a stir bar, poly(vl-evl) (0.1210 g, Mw = 2325 Da, 13% cross-linking) and 45.1 mL CH2Cl2 were added, followed by 2,2′-(ethylenedioxy)diethylamine (75.1 μL, 5.13x10−4 mol). The mixture was refluxed at 44°C for 12 hours and promptly transferred to SnakeSkin Pleated Dialysis Tubing (MWCO = 10,000) and dialyzed against dichloromethane to remove residual diamine. 1H NMR (400MHz), CDCl3/TMS, ppm) δ: The significant change is the disappearance of epoxide protons at 2.93, 2.76, and 2.47 ppm and the appearance of signals at 3.5 and 2.9 ppm, correlating to the protons of the PEG linker. The spectrum is otherwise similar in all aspects.
700 nm Nanosponges with 15% Crosslinking (Amorphous, A-NS)
To a 200-mL round bottom flask equipped with a stir bar, poly(vl-evl-avl) (0.1057 g, Mw = 7200 Da, 15% cross-linking) and 46.4 mL CH2Cl2 were added, followed by 2,2′-(ethylenedioxy)diethylamine (82.5 μL, 5.64x10−4 mol). The mixture was refluxed at 44°C for 12 hours and promptly transferred to SnakeSkin Pleated Dialysis Tubing (MWCO = 10,000) and dialyzed against dichloromethane to remove residual diamine. 1H NMR (400MHz), CDCl3/TMS, ppm) δ: The significant change is the disappearance of epoxide protons at 2.94, 2.75, and 2.48 ppm and the appearance of signals at 3.5 and 2.9 ppm, correlating to the protons of the PEG linker. The spectrum is otherwise similar in all aspects.
700 nm Nanosponges with 15% Crosslinking (with Amorphous and Crystalline Crosslinkers, AC-NS)
To a 200-mL round bottom flask equipped with a stir bar, poly(vl-evl-avl) (0.1001 g, Mw = 7200 Da, 15% cross-linking) and 43.9 mL CH2Cl2 were added, followed by 2,2′-(ethylenedioxy)diethylamine (39.1 μL, 2.67x10−4 mol) and 1,8-diaminooctane (38.5 mg, 2.67x10−4 mol). The mixture was refluxed at 44°C for 12 hours and transferred to SnakeSkin Pleated Dialysis Tubing (MWCO = 10,000) and dialyzed against dichloromethane to remove residual diamines. 1H NMR (400MHz), CDCl3/TMS, ppm) δ: The significant change, confirming incorporation of 1,8-diaminooctane, is the appearance of a signal at 1.32 ppm corresponding to the protons between the secondary amines of the cross-linker. The spectrum shows otherwise similar shifts.
Encapsulation and Determination of Percent Loading
Therapeutics or Neuro-DiO were encapsulated using a previously described procedure.45 The NS and drug/dye were weighed accurately together into a vial. The two solids were dissolved in a minimal amount of dimethyl sulfoxide (DMSO, 150 μL) and added drop-wise to a vigorously stirring solution of water (8.3 mL) and vitamin E (0.125 g). The solution turned cloudy and was immediately centrifuged at 8500 rpm for 20 minutes. The supernatant was carefully removed, fresh water was added and the pellet disturbed to ensure thorough washing of the drug-loaded particles. The centrifugation wash was repeated for a total of three washes. Finally, the NS were frozen and lyophilized to lend the drug-loaded NS as a light and fluffy white solid.
Approximately 1.0 mg of drug-loaded NS was weighed and dissolved in 100 μL DMSO. Two μL of sample solution was pipetted onto the pedestal of a UV-VIS spectrometer (NanoDrop; Thermo Fisher Scientific) and the absorbance measured at 262 nm. A calibration curve between concentration of drug and absorbance was made using a spread of samples with known concentrations of drug. Using the calibration curve, the amount of drug within the NS could be quantified and reported as a weight percent. Before use, lyophilized NS were weighed and diluted into PBS for an overall concentration of 16 mg/mL. Five drug encapsulated NS and one Neuro-DiO NS were generated (Fig. 1).
Figure 1. .

The NSs generated to test IOP-lowering drug delivery and delivery to retina. Six NSs were generated and varied by nanoscopic size, the crosslinker used, and crosslinker density. Also shown for each NS are the drug encapsulated in the NS, the drug load and drug concentration.
Delivery of Hypotensive Drugs
Brimonidine Tartrate
Mice receiving brimonidine to lower IOP were separated into three groups based on delivery method: topical application, intravitreal injection, and NS. Mice in the topical group received 3 μL of brimonidine (0.1% brimonidine tartrate) applied to the cornea of one eye daily beginning four days after microbead injection (day 4) and ending on day 6. Daily topical treatment was resumed on day 12 and continued until day 18. The fellow eye was treated with an equivalent volume of saline on the same dosing schedule. On day 4, mice in the intravitreal injection group received 1 μL brimonidine (0.1% brimonidine tartrate) in one eye and 1 μL saline in the fellow eye via intravitreal injection as previously described.40 Mice in the NS group received 1 μL brimonidine NS (Fig. 1) in one eye and 1 μL saline in the fellow eye via intravitreal injection on day 2.40
Travoprost
Mice in the topical group received 3 μL of travoprost (0.004% wt/vol) applied to the cornea of one eye on days 4 and 7. The fellow eye received an equivalent volume of saline on days 4 and 7. Mice in the NS group received 1 μL travoprost NS (Fig. 1) in one eye and 1 μL saline in the fellow eye via intravitreal injection on day 4.
Bimatoprost
Mice received 1 μL of the 400 nm NS in one eye and 1 μL saline in the fellow eye via intravitreal injection on day 5. Mice received 1 μL of the 700 nm A-NS, or the 700 nm AC-NS (Fig. 1) in one eye and 1 μL saline in the fellow eye via intravitreal injection on day 4.
Toxicity of NS similar to those used in this study has been examined previously using an MTT assay.32,45 The experimental TC50 value of the NS was determined to be 0.97 to 1 mg/ml. Following intravitreal injection of drug loaded-NS, mice were monitored daily by the authors or by Vanderbilt Division of Animal Care technicians for signs of distress and/or physical impairment. At no point during the study did the mice that received NS appear impaired or in distress. Clinical assessment (e.g., slit-lamp examination) of mice before or after intravitreal injection was not performed; no fundus photography or electroretinography was performed on these mice at any time during the study.
NS Delivery to RGCs
Mice received 1 μL of the Neuro-DiO embedded NS (Fig. 1) in both eyes via intravitreal injection. Mice were transcardially perfused with 4% paraformaldehyde at the following time points after injection: 3 days, 1 week, 2 weeks, or 4 weeks. Retinas were separated from the eyecup and processed for whole mount immunohistochemistry as described previously using an antibody against phosphorylated heavy-chain neurofilament (SMI31, 1:1,000; Sternberger Monoclonal) to visualize RGCs.46 AlexaFluor–conjugated secondary antibodies (1:200; Invitrogen, Carlsbad, CA) were used and images captured using an Olympus FV-1000 inverted confocal microscope. Neuro-DiO signal in whole mounted retinas was quantified using ImagePro (Media Cybernetics).
Results
For the mice used in this study, ocular pressure averaged 14.24 ± 0.08 mm Hg before microbead injection. Following injection of microbeads (1.5 μL) into the anterior chamber ocular pressure increased 42.8% to 20.32 ± 0.16 mm Hg. Over the course of this study, IOP of the saline treated eye averaged 19.35 ± 0.06 mm Hg, resulting in a 36% increase over baseline IOP levels (P < 0.001). This increase in IOP is similar to other studies using this model in C57 mice.41–43
Brimonidine
Ocular pressure in C57 mice before microbead injection averaged 14.44 ± 0.10 mm Hg (Fig. 2). Microbead injection into the anterior chamber increased IOP 36.4% to 19.55 ± 0.32 mm Hg in the topical group one day post-injection (Fig. 2A). Topical application of brimonidine beginning on day 4 lowered IOP from 19.37 ± 0.63 mm Hg to 13.28 ± 0.56 mm Hg on day 5 (30% decrease) and to 14.28 ± 0.20 mm Hg on day 6 (26% decrease). These decreases in IOP were significant when compared to saline treated eyes (P < 0.001). Brimonidine treatment was stopped on day 7, resulting in an IOP increase from 14.28 ± 0.20 mm Hg on day 6 to 19.83 ± 0.88 mm Hg on day 11. Treatment was resumed on day 12 and IOP decreased to 14.70 ± 0.95 mm Hg on day 13 (21% decrease), 13.76 ± 0.30 mm Hg on day 15 (25% decrease), and 13.26 ± 0.14 mm Hg on day 18 (26% decrease). Ocular pressure at each of these time points was significantly lower when compared to saline treated eyes (P < 0.017).
Figure 2. .

Intravitreal injection of brimonidine NS lowers IOP. (A) Topical application of brimonidine once daily lowered IOP on days 5 and 6 compared to saline-treated eyes (*P < 0.001, n = 3). Stopping treatment on day 7 caused IOP to increase. Resuming treatment on day 12 lowered IOP compared to saline-treated eyes by day 18 (**P < 0.017). (B) Intravitreal injection of brimonidine on day 4 lowered IOP compared to intravitreal saline injection (*P < 0.027, n = 3). (C) Intravitreal injection of brimonidine NS on day 2 lowered IOP by day 4 compared to intravitreal saline injection (*P < 0.002, n = 5). The IOP in the NS eye remained lower than saline-injected eyes until day 10 (**P < 0.02). inj, microbead injection; trx, brimonidine treatment. (D) Line graph comparing the difference in IOP between saline- and brimonidine-treated eyes (Δ IOP) for each delivery method. Treatment began on day 0. *P = 0.029 (topical versus intravitreal delivery) or **P = 0.0363 (topical versus NS delivery). n = 3 for topical and intravitreal, n = 5 for NS.
Similar to the topical group, microbead injection increased IOP 42.1% to 20.11 ± 0.17 mm Hg in the intravitreal group one day post-injection (Fig. 2B). One intravitreal injection of brimonidine on day 4 lowered IOP to 15.11 ± 0.73 mm Hg on day 5 (20% decrease) and 15.00 ± 1.21 mm Hg on day 6 (23% decrease) compared to intravitreal saline injection (P < 0.027). On day 11, IOP in the brimonidine-treated eye had increased to 18.08 ± 0.85 mm Hg, and continued to increase until it reached saline levels (19.61 ± 0.16 mm Hg) on day 15 (P = 0.864).
In the brimonidine NS group, microbead injection increased IOP 35.3%, from 14.73 ± 0.13 to 19.92 ± 0.33 mm Hg on post-injection day 1 (Fig. 2C). Intravitreal injection of brimonidine-loaded NS on day 2 lowered IOP to 12.3 ± 0.83 mm Hg on day 3 (34% decrease) and 13.66 ± 0.24 mm Hg on day 4 (27% decrease) compared to saline injection (P < 0.002). Ocular pressure in NS-treated eyes increased slightly to 15.95 ± 0.45 mm Hg on days 7 (12% decrease) and to 15.94 ± 0.10 mm Hg on day 8 (13% decrease), but was still significantly lower than saline-injected eyes (18.15 ± 0.38 and 18.39 ± 0.41 mm Hg, respectively; P < 0.02). By day 15, ocular pressure in the brimonidine NS-treated eyes had returned to saline levels (18.42 ± 0.70 mm Hg; P = 0.290).
Comparing the difference in IOP between saline- and brimonidine-treated eyes by delivery method shows that topical and NS delivery lowered IOP to similar levels in the first two days following treatment (day 0; Fig. 2D). Topical delivery lowered IOP 5.92 ± 0.57 and 5.07 ± 0.49 mm Hg on treatment days 1 and 2, while NS delivery lowered IOP 6.16 ± 1.21 and 5.29 ± 0.62 mm Hg (P > 0.40). Intravitreal delivery lowered IOP 3.70 ± 0.62 mm Hg on the first day following treatment; this was as effective as NS delivery (P = 0.0954), but less effective than topical delivery (P = 0.029). By treatment day 2, intravitreal delivery was as effective at lowering IOP (4.40 ± 1.63 mm Hg) as topical and NS delivery methods (P > 0.281). By treatment day 7, one topical application of brimonidine no longer lowered IOP compared to the saline treated eye (IOP difference of −0.72 ± 0.59 mm Hg). The difference in IOP following intravitreal delivery and NS delivery steadily decline with time, reaching 1.48 ± 1.00 and 0.88 ± 0.45 mm Hg at treatment days 7 and 8, respectively. By treatment day 8, NS delivery was more effective at lowering IOP than topical delivery (P = 0.0363), and as effective as intravitreal delivery (P = 0.272).
Travoprost
Baseline IOP in C57 mice averaged 14.47 ± 0.14 mm Hg (Fig. 3). In the topical travoprost group, IOP increased 41.6% to 20.58 ± 0.49 mm Hg following microbead injection (Fig. 3A). One topical treatment with travoprost on day 4 lowered IOP from 20.53 ± 0.47 to 15.30 ± 0.23 mm Hg on day 5 (26.7% decrease) compared to topical saline treatment (P = 0.013). Ocular pressure increased to 17.48 ± 0.86 mm Hg on day 6 and had returned to saline-treated levels (19.67 ± 0.42 mm Hg) by day 7 (P = 0.714). Mice received another single application of topical Travatan on day 7 that reduced IOP to 14.43 ± 0.39 mm Hg on day 8 (26.9% decrease, P = 0.001), with IOP again returning to saline-treated levels (19.82 ± 0.22 mm Hg) by day 10 (P = 0.927).
Figure 3. .

Intravitreal injection of travoprost NS lowers IOP. (A) A single topical application of travoprost on day 4 and day 7 reduced IOP compared to saline-treated eyes (*P < 0.013, n = 3). (B) Intravitreal injection of Travatan NS on day 4 lowered IOP on day 5 compared to intravitreal saline injection (*P = 0.003, n = 3). IOP in the NS-treated eye remained lower than the saline eye (**P < 0.02) until day 10. trx: travoprost treatment. (C) Line graph comparing the difference in IOP between saline- and travoprost-treated eyes (Δ IOP) for topical and NS delivery. Treatment began on day 0. *P < 0.023 topical versus NS delivery. n = 3 for topical and NS.
In the travoprost NS group, microbead injection increased IOP 54.1% to 22.19 ± 0.31 mm Hg (Fig. 3B). Intravitreal injection of travoprost-loaded NS on day 4 lowered IOP to 14.40 ± 0.89 mm Hg (29.2% decrease) on day 5 compared to intravitreal saline injection (P = 0.003). Ocular pressure in NS-treated eyes increased slightly to 16.12 ± 0.34 mm Hg on days 6 to 8, but was still 19.6 ± 0.5% lower compared to saline-injected eyes (P < 0.02) before returning to saline IOP levels (18.53 ± 0.66 mm Hg) by day 10 (P = 0.515).
The difference in IOP between saline- and travoprost-treated eyes by delivery method is shown in Figure 3C. Topical travoprost delivery lowered IOP 5.58 ± 1.51 and 2.16 ± 0.64 mm Hg on treatment days 1 and 2, which was similar to NS travoprost delivery (5.93 ± 0.93 and 3.93 ± 0.76 mm Hg, P > 0.152). One topical application of travoprost was no longer effective at lowering IOP compared to the saline-treated eye by treatment day 3 (IOP difference of −0.18 ± 0.61 mm Hg). In contrast, NS delivery remained effective at lowering IOP up to treatment day 4 (4.06 ± 0.03 and 3.80 ± 0.92 mm Hg for treatment days 3 and 4, respectively; P < 0.023). However, by treatment day 6 NS delivery was no longer effective at lowering IOP (IOP difference of 0.55 ± 0.44 mm Hg).
Bimatoprost
Ocular pressure in C57 mice before microbead injection averaged 13.86 ± 0.19 mm Hg (Fig. 4). Microbead injection into the anterior chamber increased IOP 44% to 19.96 ± 0.32 mm Hg in the 400 nm NS group 1 day post-injection (Fig. 4A). Intravitreal injection of 400 nm bimatoprost-NS on day 5 lowered IOP to 13.05 ± 1.04 mm Hg on day 6; IOP ranged between 12.15 ± 0.81 and 14.17 ± 0.59 mm Hg (33.2 ± 1.2% decrease compared to saline injection) from days 6 to 13 (P < 0.041). Ocular pressure increased slightly to 14.31 ± 0.28 mm Hg in NS-injected eyes from days 14 to 19, but was still 24.5% ± 1.2% lower than saline-injected eyes, (P = 0.047 at day 17; all other time points P > 0.063). Pressure returned to saline IOP levels (18.63 ± 0.69 mm Hg) by day 22 (P > 0.468).
Figure 4. .

Intravitreal injection of bimatoprost NS lowers IOP. (A) Intravitreal injection of bimatoprost NS (400 nm) on day 4 lowered IOP on days 6 to 13 compared to intravitreal saline injection (*P < 0.041, n = 2). IOP in the NS-treated eye remained lower than the saline eye until day 19 (**P = 0.047). (B) Intravitreal injection of bimatoprost 700 nm A-NS on day 4 lowered IOP from day 5 to day 35 compared to intravitreal saline injection (*P < 0.046, n = 2). (C) Intravitreal injection of bimatoprost 700 nm AC-NS on day 4 lowered IOP from day 5 to day 35 compared to intravitreal saline injection (*P < 0.049, n = 2). trx: treatment with bimatoprost. (D) Line graph comparing the difference in IOP between saline- and bimatoprost-treated eyes (Δ IOP) for each NS. Treatment began on day 0. By treatment week 3, 700 nm A-NS and AC-NS were more effective than the 400 nm NS (*P < 0.0184). Both 700 nm NS remained more effective than the 400 nm NS during treatment weeks 4 and 5 (**P < 0.0299). n = 2 for each NS group.
In the 700 nm A-NS group IOP increased 47.8% to 20.14 ± 0.36 mm Hg one day after microbead injection (Fig. 4B). Injection of A-NS on day 4 lowered IOP to 15.13 ± 0.90 mm Hg on day 5 (20.2% decrease) and 14.73 ± 0.73 mm Hg on day 6 (26.7% decrease) compared to intravitreal saline injection (P > 0.073). Ocular pressure in A-NS–injected eyes stabilized between 13.25 ± 0.85 and 15.40 ± 0.86 mm Hg from days 5 to 35, while IOP in saline-injected eyes ranged between 18.95 ± 1.01 and 20.43 ± 0.66 mm Hg over the same time frame. This resulted in IOP decreases of 22.6 to 32.7% in bimatoprost-700 nm A-NS–treated eyes (P < 0.046). By day 41, IOP in 700 nm A-NS–injected eyes had increased to 18.58 ± 0.71 mm Hg and remained similar to saline injected eyes (18.93 ± 0.64 mm Hg) through day 48 (P > 0.401).
Microbead injection increased IOP 41.5% to 19.97 ± 0.37 mm Hg in the bimatoprost 700 nm AC-NS group 1 day post-injection (Fig. 4C). Intravitreal injection of bimatoprost-AC-NS on day 4 lowered IOP 25.0 ± 0.7% compared to intravitreal saline injected eyes on days 5 to 8 (P = 0.04 for day 7; P > 0.053 for all other days). During this time IOP ranged from 14.50 ± 0.96 to 15.43 ± 0.68 mm Hg in the 700 nm AC-NS–treated eyes and 19.80 ± 1.17 to 20.43 ± 0.99 mm Hg in saline-treated eyes. From days 11 to 15, IOP in AC-NS–injected eyes was 26.5% ± 0.7% lower than saline-injected eyes (P < 0.046), with an average IOP of 14.39 ± 0.78 mm Hg compared to 19.59 ± 0.77 mm Hg. Ocular pressure held steady in AC-NS–treated eyes at 14.51 ± 0.71 mm Hg (25.3 ± 0.8% decrease) from days 19 to 22 (P < 0.022 on days 21 and 22; all others P > 0.051) before increasing slightly to an average IOP of 15.91 ± 0.81 mm Hg from days 25 to 36 (18.0 ± 1.3% decrease compared to saline, P = 0.049 for day 28, P > 0.068 for all other days). By day 41, IOP in AC-NS–injected eyes had returned to saline levels (18.18 ± 0.68 mm Hg, P > 0.255).
Comparing the difference in IOP between the three bimatoprost-NS (Fig. 4D) shows that all three NS were equally effective at lowering IOP during the first two treatment weeks. The 400 nm NS produced IOP differences of 6.44 ± 0.41 and 5.00 ± 0.34 mm Hg compared to 4.93 ± 0.43 and 5.87 ± 0.42 mm Hg for 700 nm A-NS and 5.14 ± 0.42 and 5.09 ± 0.39 mm Hg for 700 nm AC-NS (P > 0.129). By treatment week 3, the IOP difference in 400 nm NS-injected eyes approached zero (0.89 ± 0.37 mm Hg) while IOP differences of 5.10 ± 0.44 and 4.67 ± 0.36 mm Hg were observed in 700 nm A-NS– and 700 nm AC-NS–injected eyes, respectively (P < 0.0184). Both 700 nm NS were equally effective at lowering IOP during treatment weeks 4 through 6 (4.66 ± 0.47, 3.75 ± 0.44, and 1.03 ± 0.34 mm Hg for A-NS versus 3.97 ± 0.39, 2.96 ± 0.37, and 1.24 ± 0.34 mm Hg for AC-NS; P > 0.308), and were more effective than the 400 nm NS for treatment weeks 4 and 5 (P < 0.0299). By treatment week 7, neither 700 nm NS were effective a lowering IOP (IOP differences of 0.10 ± 0.33 and 0.08 ± 0.37 mm Hg, respectively).
Nanoparticle Delivery to RGCs
To examine the use of NS to deliver neuroprotective drugs directly to RGCs, C57 mice were intravitreally injected with a 50 nm NS loaded with Neuro-DiO. The retinal deposition of Neuro-DiO was quantified in whole mounted retinas at 3, 7, 14, and 28 days post-injection (Fig. 5). After 3 days, 19.6% to 28.5% of the retinal surface was covered with Neuro-DiO (see left image, Fig. 5A). With increasing time, the percentage of retinal surface covered by Neuro-DiO increased, ranging from 25.6% to 52.1% at 7 to 14 days post-injection (see right image, Fig. 5B). Not surprisingly, the greatest deposition of Neuro-DiO was observed 28 days after injection, with 60.2% and 71.4% of the retina covered (Fig. 5B). High magnification confocal images of whole mounted retinas 1 week following injection of Neuro-DiO NS shows deposition of Neuro-DiO on the retinal surface (arrows, Figs. 6A, 6B). In addition, Neuro-DiO was taken up by RGCs as shown by the colocalization of Neuro-DiO (green) and phosphorylated neurofilament (pNF; red) indicated by the dotted lines. Orthogonal projections through a pNF-positive RGCs show Neuro-DiO puncta within the cell (Figs. 6C, 6D), suggesting internalization of Neuro-DiO by RGCs.
Figure 5. .
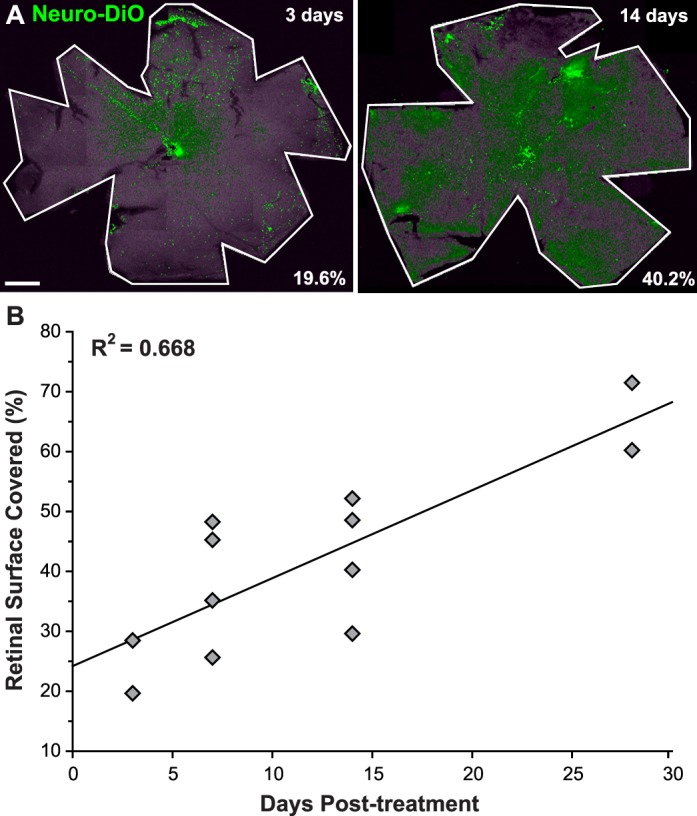
Retinal deposition of Neuro-DiO released from 50 nm NS increases with time. (A) Confocal micrographs of whole mounted retina demonstrating Neuro-DiO (green) deposition after 3 days (left) and 14 days (right). The percentage of retinal surface covered by Neuro-DiO was measured and is shown in the lower right corner. (B) Scatter plot showing a linear increase in the percentage of retinal surface covered by Neuro-DiO with increasing time. Each diamond represents one retina. Scale bar: 500 μm.
Figure 6. .

RGCs take up Neuro-DiO released from 50 nm NS. Confocal micrographs of whole mount retina 1 week after intravitreal injection of Neuro-DiO loaded NS. (A) Neuro-DiO (green) was released from NS and deposited on the retinal surface (arrows). (B) Uptake of Neuro-DiO by phosphorylated neurofilament-positive RGCs (pNF; red) was observed (dotted circles). (C) Confocal micrograph and orthogonal projections showing Neuro-DiO surrounding pNF-positive RGC somas. The yellow dotted lines indicate the position of the orthogonal views. (D) An orthogonal view rotated about the Z-axis shows Neuro-DiO deposits surrounding a pNF-positive RGC. Scale bar: 10 μm.
Discussion
In the next 10 years, glaucoma will affect nearly 80 million people worldwide, 3.4 million in the United States.3 As the disease progresses to blindness, the cost of treatment increases. It is estimated that $2.5 billion dollars are spent annually to treat patients with glaucoma.47 The majority of these treatments target elevated IOP; however, lowering IOP doesn't necessarily halt disease progression.6,8 This is most likely due to poor treatment adherence, suggesting alternative therapeutic options or delivery systems that increase patient compliance could be beneficial.10,13,15,19,20,24,25 We developed a series of NSs (Fig. 1) that encapsulate ocular hypotensive drugs to provide extended-release treatments that could minimize patient noncompliance.44 The efficacy of these NS administered intravitreally was tested in mice following microbead-induced ocular hypertension. Smaller NS (50 nm) containing brimonidine or travoprost were as effective at lowering IOP as topical application of drug or intravitreal injection of drug alone immediately following treatment, with effects that lasted up to 6 days (Figs. 2, 3). Larger NS (400 to 700 nm) were effective at lowering IOP 27% for almost 3 weeks post-injection (Fig. 4). Eyes that received 700 nm bimatoprost-NS continued to show a difference in IOP of at least 4 mm Hg out to 4 weeks (P > 0.0299). Our data suggesed NS can effectively deliver ocular hypotensive drugs in a linear and sustained manner following one intravitreal injection.
The overall goal of this study is to provide proof-of-concept data for an extended-release drug delivery system that could be developed further for use in the treatment of glaucoma. As an initial step, we wanted to show efficacy of our NS in a well characterized animal model of glaucoma.41,42,48 Moving forward with our NS drug delivery system will require multiple animal models, including those more suited for intravitreal pharmacokinetic studies, so that all aspects of treatment (safety, potential side effects, less invasive delivery methods) can be examined thoroughly. Injection of Neuro-DiO loaded NS was an extension of this proof-of-concept to determine if the NS could deliver a payload to the retinal surface and to RGCs. Having shown that it is possible to get a payload to cross the inner limiting membrane and be taken up by RGCs (Fig. 6), the next step would be to deliver a neuroprotective drug to these cells using the NS. In those studies, electroretinography or other functional outcome measures could be used to examine the effectiveness of the neuroprotection. Although more studies using our NS are required, we do feel the data presented here add to the growing body of work examining more effective ocular drug delivery methods for the treatment of diseases, like glaucoma and AMD.24,49–54
Compared to noncompliant patients, patients who adhere to treatment plans have lower ocular pressures, less disc cupping, and less visual field loss over time.13 Given that glaucoma progresses to blindness, and this progression occurs faster with no treatment, one would think adherence rates for glaucoma therapy would be quite high. In fact, compliance rates near 90% have been reported in some studies, with 85% to 92% of patients reporting no to very few missed doses during the study period.55,56 However, these studies relied on patient self-reporting, which has been shown to overestimate compliance dramatically.17,19,57 Another study found that in the 3 years following a glaucoma diagnosis, less than 10% of patients refilled their initial prescription regularly.10 For patients who filled at least one prescription, half discontinued therapy within 6 months.10 To increase compliance in glaucoma patients, approaches like electronic dosing aids, motivational- and patient-centered communication strategies, and video documentation are being used, but so far the results have been mixed.15,17,19–22 A study examining patient compliance for 3 months after providing an electronic dosing aid showed 96% adherence within the first 10 days; this decreased slightly to 86% compliance for the remainder of the study.19 In a similar study, Dreer et al.20 found that when using an electronic dosing aid 80% of patients took some amount of drops within 6 hours of their prescribed dosing time, but only 64% took the prescribed amount of drops within 3 hours of the prescribed dosing time. Hermann et al.57 determined adherence in patients aware of electronic monitoring was no different than in patients who were unaware (67.5% compared to 69.5%), while Okeke et al.58 showed 45% of study participants who were provided free medications and were aware they were being monitored took less than 75% of intended doses during the 3 month study. In addition to using dosing aids to improve patient compliance, the development of extended-release therapeutics could eliminate many of the barriers patients report as contributing to nonadherence.11,13–18
While topical administration of drug is the preferred method of delivery for most ocular diseases, including glaucoma, this route is very inefficient.7,49 In fact, less than 5% of drug applied topically reaches its target tissue within the eye, which necessitates the frequent dosing (up to 3 times daily) required for most topical ocular drugs.50,59–61 Many factors, including ocular anatomy, blinking, and tear film, limit the bioavailability of topical ocular drugs.50,51,62,63 Additionally, a significant portion of drug (∼80%) may be absorbed by blood vessels in the conjunctiva, passing into systemic circulation to cause adverse off-target effects.64 Targeting tissues in the posterior globe, like RGCs, proves even more difficult as drugs must penetrate the vitreous and inner limiting membrane of the retina.52 Due to these challenges, more efficient drug delivery systems are being developed for ocular tissues that include ocular inserts, lipid-based nanocarriers, nanoparticles, and punctum inserts.24,49–54 Recent studies using topically applied nanoparticles loaded with ocular hypotensive drugs have shown promise. For example, topical administration of nanoparticles (256 nm) containing the carbonic anhydrase inhibitor methazolamide lowered IOP for 18 hours, with the maximal effect observed 2 to 8 hours after dosing.36 In vitro drug release studies, however, showed that 99% of the drug had been released from the nanoparticle after 4 hours, suggesting a “burst” of drug rather than sustained release.36 Similarly, brimonidine-loaded nanoparticles (117 to 131 nm) delivered via eye drops lowered IOP for 5 to 7 hours after dosing.37 The amount of brimonidine released in vitro after 24 hours ranged from 37% to 62%. A study using betaxolol-loaded nanoparticles (168 to 260 nm) saw a 36% reduction in IOP 5 hours after dosing. This nanoparticle had a biphasic release pattern of an initial burst followed by sustained release of drug for about 12 hours.65 The NS used in this study have been characterized previously.45 In vitro release studies using taxol-loaded NS similar to the ones used in this study showed that 4% to 7% of the drug was released by 6 hours. Drug continued to be released in a steady linear fashion, resulting in approximately 50% of the drug remaining in the particle at 60 days.45 In our study, we observed IOP-lowering effects within 24 hours that were sustained for 4 to 6 days for smaller NS (Figs. 2, 3) and up to 32 days for larger NS (Figs. 4B, 4C). This suggests glaucoma patients could manage their ocular pressure by receiving NS drug therapy once a month.
The success of intraocular injection to treat ocular disorders and the complex topical dosing schedules required for adequate management of IOP have resulted in more patients willing to receive ocular injection in lieu of traditional glaucoma therapy.25–28,66 The advantages of intraocular injection are that high concentrations of drug can be achieved near the target tissue while minimizing systemic adverse effects.66 However, repeated intraocular injection significantly increases the risk of ocular complications, including discomfort or pain, subconjunctival or vitreal hemorrhage, acute and sterile intraocular inflammation, uveitis, and endophthalmitis.66,67 Reviews of clinical trials and patient charts to determine the safety of AMD intravitreal therapies have found that incidence rates for endophthalmitis range from 0 to 0.16%.68–73 A longitudinal study by Rasmussen et al.29 showed that of 600 eyes that began AMD intravitreal treatment, a third of the eyes still were receiving treatment after 4 years with no change in visual activity.29 For 7584 injections given (average of 5.5 injections per year), two eyes were diagnosed with endophthalmitis, one eye with retinal detachment; no major hemorrhage or traumatic cataracts were observed. Similar reviews have shown increased visual acuity with continued AMD intravitreal treatment and a low incidence of adverse side effects.74,75 While some patients respond to intravitreal injection with sustained elevation of IOP, most do not even after multiple injections.76–82 In our study, we performed intravitreal injection of drug-loaded NS once and observed IOP-lowering effects out to 32 days (Fig. 4). While intravitreal injection of NS to lower IOP would remove some hurdles to patient compliance, the increased risk for adverse outcomes following repeated injections argue against this delivery method as a replacement for first line glaucoma treatment (topical drops). Ideally, our NS delivery system could be adapted to deliver IOP-lowering drugs via topical routes. If one dose of topical drug-loaded NS could lower IOP for the same length of time as intravitreal injection, patients would only need to dose once per month. This could drastically reduce patient nonadherence while also reducing many negative side effects from repeated intravitreal injections.
The main benefit of intravitreal delivery of our NS would be in delivering neuroprotective therapies directly to posterior ocular tissues, like RGCs. Therapeutics that enhance RGC survival or function could be loaded into NS and, if release could be sustained for at least 4 months,45 patients would require only three injections per year. Koo et al.39 injected various fluorescently-labeled nanoparticles intravitreally into rat eyes and examined their distribution. Particles with anionic surface properties penetrated deeper into the retina than cationic particles.39 Similarly, nanoparticles (150–180 nm) carrying fluorescently-labeled cargo injected into the vitreous were deposited in the nerve fiber layer of the retina 48 hours post-injection.83 We injected Neuro-DiO-NS (50 nm) into the vitreous cavity and examined retinal distribution up to 28 days post-injection (Fig. 5). The percentage of Neuro-DiO on the retinal surface increased from nearly 20% at 3 days to 71% at 28 days, suggesting release of Neuro-DiO from the NS occurred linearly over time. The released Neuro-DiO was taken up by RGCs as shown by colocalization with phosphorylated neurofilament (Figs. 6C, 6D). Directly targeting the cells that degenerate in glaucoma, the RGCs, using nanoparticles or NS loaded with neuroprotective agents could potentially preserve vision in the 5.9 million people estimated to lose their sight to this disease in the next 10 years.3
Acknowledgments
Supported by the National Science Foundation (NSF-CHEM-0645737; EH), the National Institute of Health (NIH-NIBIB R21 EB009223-01; EH), the National Eye Institute (5R01EY017427-03; DJC), the Melza M. and Frank Theodore Barr Foundation through the Glaucoma Research Foundation (DJC), Senior Scientific Investigator and Departmental Unrestricted Award from Research to Prevent Blindness, Inc. (DJC), a BrightFocus Foundation (formerly American Health Assistance Foundation) National Glaucoma Research Award (DJC). Imaging supported through the Vanderbilt University Medical Center Cell Imaging Shared Resource core facility (CTSA Grant UL1 RR024975 from NCRR/NIH) and the Vanderbilt Vision Research Center (P30EY008126).
References
- 1.Nickells RW, Howell GR, Soto I, John SW. Under pressure: cellular and molecular responses during glaucoma, a common neurodegeneration with axonopathy. Annu Rev Neurosci. 2012;35:153–179. doi: 10.1146/annurev.neuro.051508.135728. [DOI] [PubMed] [Google Scholar]
- 2.Calkins DJ. Critical pathogenic events underlying progression of neurodegeneration in glaucoma. Prog Retin Eye Res. 2012;31:702–719. doi: 10.1016/j.preteyeres.2012.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. doi: 10.1136/bjo.2005.081224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Quigley HA, Cassard SD, Gower EW, Ramulu PY, Jampel HD, Friedman DS. The cost of glaucoma care provided to Medicare beneficiaries from 2002 to 2009. Ophthalmology. 2013;120:2249–2257. doi: 10.1016/j.ophtha.2013.04.027. [DOI] [PubMed] [Google Scholar]
- 5.Bramley T, Peeples P, Walt JG, Juhasz M, Hansen JE. Impact of vision loss on costs and outcomes in medicare beneficiaries with glaucoma. Arch Ophthalmol. 2008;126:849–856. doi: 10.1001/archopht.126.6.849. [DOI] [PubMed] [Google Scholar]
- 6.Heijl A, Leske MC, Bengtsson B, Hyman L, Hussein M. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120:1268–1279. doi: 10.1001/archopht.120.10.1268. [DOI] [PubMed] [Google Scholar]
- 7.Shih GC, Calkins DJ. Secondary neuroprotective effects of hypotensive drugs and potential mechanisms of action. Expert Rev Ophthalmol. 2012;7:161–175. doi: 10.1586/eop.12.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Investigators TA. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration.The AGIS Investigators. Am J Ophthalmol. 2000;130:429–440. doi: 10.1016/s0002-9394(00)00538-9. [DOI] [PubMed] [Google Scholar]
- 9.Leske MC, Heijl A, Hussein M, et al. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121:48–56. doi: 10.1001/archopht.121.1.48. [DOI] [PubMed] [Google Scholar]
- 10.Nordstrom BL, Friedman DS, Mozaffari E, Quigley HA, Walker AM. Persistence and adherence with topical glaucoma therapy. Am J Ophthalmol. 2005;140:598–606. doi: 10.1016/j.ajo.2005.04.051. [DOI] [PubMed] [Google Scholar]
- 11.Gurwitz JHM, Glynn RJ, Monane M, et al. Treatment for glaucoma: adherence by the elderly. Am J Public Health. 1993;83:711–716. doi: 10.2105/ajph.83.5.711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rotchford AP, Murphy KM. Compliance with timolol treatment in glaucoma. Eye (Lond) 1998;12((Pt 2)):234–236. doi: 10.1038/eye.1998.56. [DOI] [PubMed] [Google Scholar]
- 13.Konstas AG, Maskaleris G, Gratsonidis S, Sardelli C. Compliance and viewpoint of glaucoma patients in Greece. Eye (Lond) 2000;14((Pt 5)):752–756. doi: 10.1038/eye.2000.197. [DOI] [PubMed] [Google Scholar]
- 14.Patel SC, Spaeth GL. Compliance in patients prescribed eyedrops for glaucoma. Ophthalmic surgery. 1995;26:233–236. [PubMed] [Google Scholar]
- 15.Cook PF, Bremer RW, Ayala AJ, Kahook MY. Feasibility of motivational interviewing delivered by a glaucoma educator to improve medication adherence. Clin Ophthalmol. 2010;4:1091–1101. doi: 10.2147/OPTH.S12765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma results from the Glaucoma Adherence and Persistency Study. Ophthalmology. 2008;115:1320–1327. doi: 10.1016/j.ophtha.2007.11.023. [DOI] [PubMed] [Google Scholar]
- 17.Hennessy AL, Katz J, Covert D, Protzko C, Robin AL. Videotaped evaluation of eyedrop instillation in glaucoma patients with visual impairment or moderate to severe visual field loss. Ophthalmology. 2010;117:2345–2352. doi: 10.1016/j.ophtha.2010.03.040. [DOI] [PubMed] [Google Scholar]
- 18.Muir KW, Santiago-Turla C, Stinnett SS, et al. Health literacy and adherence to glaucoma therapy. Am J Ophthalmol. 2006;142:223–226. doi: 10.1016/j.ajo.2006.03.018. [DOI] [PubMed] [Google Scholar]
- 19.Ajit RR, Fenerty CH, Henson DB. Patterns and rate of adherence to glaucoma therapy using an electronic dosing aid. Eye (Lond) 2010;24:1338–1343. doi: 10.1038/eye.2010.27. [DOI] [PubMed] [Google Scholar]
- 20.Dreer LE, Girkin C, Mansberger SL. Determinants of medication adherence to topical glaucoma therapy. J Glaucoma. 2012;21:234–240. doi: 10.1097/IJG.0b013e31821dac86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hahn SR. Patient-centered communication to assess and enhance patient adherence to glaucoma medication. Ophthalmology. 2009;116((11 Suppl)):S37–42. doi: 10.1016/j.ophtha.2009.06.023. [DOI] [PubMed] [Google Scholar]
- 22.Kowing D, Messer D, Slagle S, Wasik A. V-POAG Group. Programs to optimize adherence in glaucoma. Optometry. 2010;81:339–350. doi: 10.1016/j.optm.2009.09.021. [DOI] [PubMed] [Google Scholar]
- 23.Tsai JC. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology. 2009;116((11 Suppl)):S30–36. doi: 10.1016/j.ophtha.2009.06.024. [DOI] [PubMed] [Google Scholar]
- 24.Knight OJ, Lawrence SD. Sustained drug delivery in glaucoma. Curr Opin Ophthalmol. 2014;25:112–117. doi: 10.1097/ICU.0000000000000031. [DOI] [PubMed] [Google Scholar]
- 25.Chong RS, Su DH, Tsai A, et al. Patient acceptance and attitude toward an alternative method of subconjunctival injection for the medical treatment of glaucoma. J Glaucoma. 2013;22:190–194. doi: 10.1097/IJG.0b013e318237c6c4. [DOI] [PubMed] [Google Scholar]
- 26.Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1419–1431. doi: 10.1056/NEJMoa054481. [DOI] [PubMed] [Google Scholar]
- 27.Brown DM, Kaiser BK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1432–1444. doi: 10.1056/NEJMoa062655. [DOI] [PubMed] [Google Scholar]
- 28.Gillies MC, Walton RJ, Arnold JJ, et al. Comparison of outcomes from a phase 3 study of age-related macular degeneration with a matched, observational cohort. Ophthalmology. 2013;121:676–681. doi: 10.1016/j.ophtha.2013.09.050. [DOI] [PubMed] [Google Scholar]
- 29.Rasmussen A, Bloch SB, Fuchs J, et al. A 4-year longitudinal study of 555 patients treated with ranibizumab for neovascular age-related macular degeneration. Ophthalmology. 2013;120:2630–2636. doi: 10.1016/j.ophtha.2013.05.018. [DOI] [PubMed] [Google Scholar]
- 30.Chiorean EG, Von Hoff DD. Taxanes: impact on pancreatic cancer. Anticancer Drugs. 2014;25:584–592. doi: 10.1097/CAD.0000000000000073. [DOI] [PubMed] [Google Scholar]
- 31.Blanco E, Ferrari M. Emerging nanotherapeutic strategies in breast cancer. Breast. 2014;23:10–18. doi: 10.1016/j.breast.2013.10.006. [DOI] [PubMed] [Google Scholar]
- 32.Passarella RJ, Spratt DE, van der Ende AE, et al. Targeted nanoparticles that deliver a sustained, specific release of Paclitaxel to irradiated tumors. Cancer Res. 2010;70:4550–4559. doi: 10.1158/0008-5472.CAN-10-0339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Meister S, Zlatev I, Stab J, et al. Nanoparticulate flurbiprofen reduces amyloid-beta42 generation in an in vitro blood-brain barrier model. Alzheimer Res Ther. 2013;5:51. doi: 10.1186/alzrt225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Laroui H, Geem D, Xiao B, et al. Targeting intestinal inflammation with CD98 siRNA/PEI-loaded nanoparticles. Mol Ther. 2014;22:69–80. doi: 10.1038/mt.2013.214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Look M, Stern E, Wang QA, et al. Nanogel-based delivery of mycophenolic acid ameliorates systemic lupus erythematosus in mice. J Clin Invest. 2013;123:1741–1749. doi: 10.1172/JCI65907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Chen R, Qian Y, Li R, et al. Methazolamide calcium phosphate nanoparticles in an ocular delivery system. Yakugaku zasshi. 2010;130:419–424. doi: 10.1248/yakushi.130.419. [DOI] [PubMed] [Google Scholar]
- 37.Ibrahim MM, Abd-Elgawad AE, Soliman OA, Jablonski MM. Novel topical ophthalmic formulations for management of glaucoma. Pharm Res. 2013;30:2818–2831. doi: 10.1007/s11095-013-1109-1. [DOI] [PubMed] [Google Scholar]
- 38.Jung HJ, Abou-Jaoude M, Carbia BE, Plummer C, Chauhan A. Glaucoma therapy by extended release of timolol from nanoparticle loaded silicone-hydrogel contact lenses. J Control Release. 2013;165:82–89. doi: 10.1016/j.jconrel.2012.10.010. [DOI] [PubMed] [Google Scholar]
- 39.Koo H, Moon H, Han H, et al. The movement of self-assembled amphiphilic polymeric nanoparticles in the vitreous and retina after intravitreal injection. Biomaterials. 2012;33:3485–3493. doi: 10.1016/j.biomaterials.2012.01.030. [DOI] [PubMed] [Google Scholar]
- 40.Crish SD, Sappington RM, Inman DM, Horner PJ, Calkins DJ. Distal axonopathy with structural persistence in glaucomatous neurodegeneration. Proc Natl Acad Sci U S A. 2010;107:5196–5201. doi: 10.1073/pnas.0913141107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sappington RM, Carlson BJ, Crish SD, Calkins DJ. The microbead occlusion model: a paradigm for induced ocular hypertension in rats and mice. Invest Ophthalmol Vis Sci. 2010;51:207–216. doi: 10.1167/iovs.09-3947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ward NJ, Ho KW, Lambert WS, Weitlauf C, Calkins DJ. Absence of transient receptor potential vanilloid-1 accelerates stress-induced axonopathy in the optic projection. J Neurosci. 2014;34:3161–3170. doi: 10.1523/JNEUROSCI.4089-13.2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Weitlauf C, Ward NJ, Lambert WS, et al. Short-term increases in transient receptor potential vanilloid-1 mediate stress-induced enhancement of neuronal excitation. J Neurosci. 2014;34:15369–15381. doi: 10.1523/JNEUROSCI.3424-14.2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.van der Ende AE, Kravitz EJ, Harth E. Approach to formation of multifunctional polyester particles in controlled nanoscopic dimensions. J Am Chem Soc. 2008;130:8706–8713. doi: 10.1021/ja711417h. [DOI] [PubMed] [Google Scholar]
- 45.van der Ende AE, Sathiyakumar V, Diaz R, Hallahan DE, Harth E. Linear release nanoparticle devices for advanced targeted cancer therapies with increased efficacy. Polymer Chemistry. 2010;1:93–96. [Google Scholar]
- 46.Sappington RM, Sidorova T, Long DJ, Calkins DJ. TRPV1: contribution to retinal ganglion cell apoptosis and increased intracellular Ca2+ with exposure to hydrostatic pressure. Invest Ophthalmol Vis Sci. 2009;50:717–728. doi: 10.1167/iovs.08-2321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Traverso CE, Walt JG, Kelly SP. Direct costs of glaucoma and severity of the disease: a multinational long term study of resource utilisation in Europe. Br J Ophthalmol. 2005;89:1245–1249. doi: 10.1136/bjo.2005.067355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chen H, Wei JX, Cho KS, et al. Optic neuropathy due to microbead-induced elevated intraocular pressure in the mouse. Invest Ophthalmol Vis Sci. 2010;52:36–44. doi: 10.1167/iovs.09-5115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Souza JG, Dias K, Pereira TA, Bernardi DS, Lopez RF. Topical delivery of ocular therapeutics: carrier systems and physical methods. J Pharm Pharmacol. 2014;66:507–530. doi: 10.1111/jphp.12132. [DOI] [PubMed] [Google Scholar]
- 50.Gan L, Wang J, Jiang M, et al. Recent advances in topical ophthalmic drug delivery with lipid-based nanocarriers. Drug Discov Today. 2013;18:290–297. doi: 10.1016/j.drudis.2012.10.005. [DOI] [PubMed] [Google Scholar]
- 51.Gaudana R, Ananthula HK, Parenky A, Mitra AK. Ocular drug delivery. AAPS J. 2010;12:348–360. doi: 10.1208/s12248-010-9183-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Pita-Thomas DW, Goldberg JL. Nanotechnology and glaucoma: little particles for a big disease. Curr Opin Ophthalmol. 2013;24:130–135. doi: 10.1097/ICU.0b013e32835cfe92. [DOI] [PubMed] [Google Scholar]
- 53.Baranowski P, Karolewicz B, Gajda M, Pluta J. Ophthalmic drug dosage forms: characterisation and research methods. Sci World J. 2014;2014:861904. doi: 10.1155/2014/861904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kim NJ, Harris A, Gerber A, et al. Nanotechnology and glaucoma: a review of the potential implications of glaucoma nanomedicine. Br J Ophthalmol. 2014;98:427–431. doi: 10.1136/bjophthalmol-2013-304028. [DOI] [PubMed] [Google Scholar]
- 55.Jampel HD, Schwartz GF, Robin AL, et al. Patient preferences for eye drop characteristics: a willingness-to-pay analysis. Arch Ophthalmol. 2003;121:540–546. doi: 10.1001/archopht.121.4.540. [DOI] [PubMed] [Google Scholar]
- 56.Tsai JC, McClure CA, Ramos SE, Schlundt DG, Pichert JW. Compliance barriers in glaucoma: a systematic classification. J Glaucoma. 2003;12:393–398. doi: 10.1097/00061198-200310000-00001. [DOI] [PubMed] [Google Scholar]
- 57.Okeke CO, Quigley HA, Jampel HD, et al. Adherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid study. Ophthalmology. 2009;116:191–199. doi: 10.1016/j.ophtha.2008.09.004. [DOI] [PubMed] [Google Scholar]
- 58.Hermann MM, Papaconstantinou D, Muether PS, Georgopoulos G, Diestelhorst M. Adherence with brimonidine in patients with glaucoma aware and not aware of electronic monitoring. Acta Ophthalmol. 2011;89:e300–305. doi: 10.1111/j.1755-3768.2010.02050.x. [DOI] [PubMed] [Google Scholar]
- 59.Zarbin MA, Montemagno C, Leary JF, Ritch R. Nanomedicine for the treatment of retinal and optic nerve diseases. Curr Opin Pharmacol. 2013;13:134–148. doi: 10.1016/j.coph.2012.10.003. [DOI] [PubMed] [Google Scholar]
- 60.Loch C, Zakelj S, Kristi A, et al. Determination of permeability coefficients of ophthalmic drugs through different layers of porcine, rabbit and bovine eyes. Eur J Pharm Sci. 2012;47:131–138. doi: 10.1016/j.ejps.2012.05.007. [DOI] [PubMed] [Google Scholar]
- 61.Rittenhouse KD, Peiffer RL, Jr, Pollack GM. Evaluation of microdialysis sampling of aqueous humor for in vivo models of ocular absorption and disposition. J Pharm Biomed Anal. 1998;16:951–959. doi: 10.1016/s0731-7085(97)00060-5. [DOI] [PubMed] [Google Scholar]
- 62.Pahuja P, Arora S, Pawar P. Ocular drug delivery system: a reference to natural polymers. Exp Opin Drug Deliv. 2012;9:837–861. doi: 10.1517/17425247.2012.690733. [DOI] [PubMed] [Google Scholar]
- 63.Gaudana R, Jwala J, Boddu SH, Mitra AK. Recent perspectives in ocular drug delivery. Pharm Res. 2009;26:1197–1216. doi: 10.1007/s11095-008-9694-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Lavik E, Kuehn MH, Kwon YH. Novel drug delivery systems for glaucoma. Eye (Lond) 2011;25:578–586. doi: 10.1038/eye.2011.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Jain K, Kumar RS, Sood S, Dhyanandhan G. Betaxolol hydrochloride loaded chitosan nanoparticles for ocular delivery and their anti-glaucoma efficacy. Currj Drug Delivery. 2013;10:493–499. doi: 10.2174/1567201811310050001. [DOI] [PubMed] [Google Scholar]
- 66.Peyman GA, Lad EM, Moshfeghi DM. Intravitreal injection of therapeutic agents. Retina. 2009;29:875–912. doi: 10.1097/IAE.0b013e3181a94f01. [DOI] [PubMed] [Google Scholar]
- 67.Marticorena J, Romano V, Gomez-Ulla F. Sterile endophthalmitis after intravitreal injections. Med Inflamm. 2012;2012:928123. doi: 10.1155/2012/928123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Gragoudas ES, Adamis AP, Cunningham ET, Jr, et al. Pegaptanib for neovascular age-related macular degeneration. N Engl J Med. 2004;351:2805–2816. doi: 10.1056/NEJMoa042760. [DOI] [PubMed] [Google Scholar]
- 69.Fintak DR, Shah GK, Blinder KJ, et al. Incidence of endophthalmitis related to intravitreal injection of bevacizumab and ranibizumab. Retina. 2008;28:1395–1399. doi: 10.1097/IAE.0b013e3181884fd2. [DOI] [PubMed] [Google Scholar]
- 70.Diago T, McCannel CA, Bakri SJ, et al. Infectious endophthalmitis after intravitreal injection of antiangiogenic agents. Retina. 2009;29:601–605. doi: 10.1097/IAE.0b013e31819d2591. [DOI] [PubMed] [Google Scholar]
- 71.Ladas ID, Karagiannis DA, Rouvas AA, Kotsolois AI, Liotsou L, Vergados I. Safety of repeat intravitreal injections of bevacizumab versus ranibizumab: our experience after 2,000 injections. Retina. 2009;29:313–318. doi: 10.1097/IAE.0b013e31819a5f98. [DOI] [PubMed] [Google Scholar]
- 72.Day S, Acquah K, Murthyunjaya P, et al. Ocular complications after anti-vascular endothelial growth factor therapy in Medicare patients with age-related macular degeneration. Am J Ophthalmol. 2011;152:266–272. doi: 10.1016/j.ajo.2011.01.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Biagi C, Conti V, Montanaro N, et al. Comparative safety profiles of intravitreal bevacizumab, ranibizumab and pegaptanib: the analysis of the WHO database of adverse drug reactions. Eur J Pharmacol. 2014;70:1505–1512. doi: 10.1007/s00228-014-1755-1. [DOI] [PubMed] [Google Scholar]
- 74.Kwon OW, Lee FL, Chung H, et al. EXTEND III: efficacy and safety of ranibizumab in South Korean and Taiwanese patients with subfoveal CNV secondary to AMD. Graefes Arch Clin Exp Ophthalmol. 2012;250:1467–1476. doi: 10.1007/s00417-012-1970-3. [DOI] [PubMed] [Google Scholar]
- 75.Solomon SD, Lindsley K, Vedula SS, Krzystolik MG, Hawkins BS. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Cochrane Database Syst Rev. 2014;8 doi: 10.1002/14651858.CD005139.pub3. CD005139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Adelman RA, Zheng Q, Mayer HR. Persistent ocular hypertension following intravitreal bevacizumab and ranibizumab injections. J Ocul Pharmacol Ther. 2010;26:105–110. doi: 10.1089/jop.2009.0076. [DOI] [PubMed] [Google Scholar]
- 77.Bakri SJ, McCannel CA, Edwards AO, Moshfeghi DM. Persisent ocular hypertension following intravitreal ranibizumab. Graefes Arch Clin Exp Ophthalmol. 2008;246:955–958. doi: 10.1007/s00417-008-0819-2. [DOI] [PubMed] [Google Scholar]
- 78.Good TJ, Kimura AE, Mandava N, Kahook MY. Sustained elevation of intraocular pressure after intravitreal injections of anti-VEGF agents. Br J Ophthalmol. 2011;95:1111–1114. doi: 10.1136/bjo.2010.180729. [DOI] [PubMed] [Google Scholar]
- 79.Kahook MY, Kimura AE, Wong LJ, et al. Sustained elevation in intraocular pressure associated with intravitreal bevacizumab injections. Ophthalmic Surg Lasers Imaging. 2009;40:293–295. doi: 10.3928/15428877-20090430-12. [DOI] [PubMed] [Google Scholar]
- 80.Tseng JJ, Vance SK, Della Torre KE, et al. Sustained increased intraocular pressure related to intravitreal antivascular endothelial growth factor therapy for neovascular age-related macular degeneration. J Glaucoma. 2012;21:241–247. doi: 10.1097/IJG.0b013e31820d7d19. [DOI] [PubMed] [Google Scholar]
- 81.Pershing S, Bakri SJ, Moshfeghi DM. Ocular hypertension and intraocular pressure asymmetry after intravitreal injection of anti-vascular endothelial growth factor agents. Ophthalmic Surg Lasers Imaging Retina. 2013;44:460–464. doi: 10.3928/23258160-20130909-07. [DOI] [PubMed] [Google Scholar]
- 82.Bakri SJ, Moshfeghi DM, Francom S, et al. Intraocular pressure in eyes receiving monthly ranibizumab in 2 pivotal age-related macular degeneration clinical trials. Ophthalmology. 2014;121:1102–1108. doi: 10.1016/j.ophtha.2013.11.029. [DOI] [PubMed] [Google Scholar]
- 83.Alqawlaq S, Sivak JM, Huzil JT, et al. Preclinical development and ocular biodistribution of gemini-DNA nanoparticles after intravitreal and topical administration: towards non-invasive glaucoma gene therapy. Nanomedicine. 2014;10:1637–1647. doi: 10.1016/j.nano.2014.05.010. [DOI] [PubMed] [Google Scholar]