

Abstract
A 68-year-old gentleman presented with abdominal distension and faeculent vomiting. He had a background of cerebral palsy with learning difficulties making history taking problematic. A CT scan suggested small bowel obstruction secondary to gallstone ileus. The most likely differential diagnosis was an inguinal hernia which was noted adjacent to the transition point. Laparotomy revealed grossly dilated small bowel with a 3-cm intraluminal gallstone. The gallstone was freely mobile within the lumen on the ileum and thus could not be causing obstruction. A caecal mass was also found, which was determined to be the cause of the obstruction. Limited ileocaecectomy was performed, which revealed a Duke's A adenocarcinoma. Gallstone ileus and caecal tumour can commonly be confused prior to surgery. There are however no previous reports of concurrent gallstone ileus and caecal tumour. Communication issues with the patient are likely to have contributed to the difficulty in diagnosis.
INTRODUCTION
A gentleman with cerebral palsy presented with abdominal distension and vomiting. History was very difficult due to his communication issues and thus decisions had to be based on examination and investigations alone. As will be seen as the case progresses the diagnosis became very different when the patient was operated upon. This emphasizes the importance of history and the difficulties presented by patients with learning difficulties and/or communication barriers.
CASE REPORT
A 68-year-old gentleman presented to A&E with a 3-day history of nausea and faeculent vomiting. He was also reported to have not opened his bowels for 4 days, which was normal for him. He had no abdominal pain and had no fever or rigours.
His background was that he had cerebral palsy with severe learning difficulties. He has also had transient ischaemic attacks in the past. He is a nursing home resident and mobilizes with sticks.
On examination he was found to be mildly distended with a soft painless abdomen, per rectum examination was refused. A provisional diagnosis of constipation was made and he was referred to the Medical Assessment Unit. He was reviewed by the medical team who agreed with the previous diagnosis, and they also began treatment for biliary sepsis based on his blood results which suggested obstructive jaundice.
The following day his constipation had not resolved despite laxative treatment; thus, an abdominal X-ray was ordered which revealed dilated small bowel loops with collapsed large bowel suggestive of small bowel obstruction. This resulted in referral to the general surgery team who arranged a CT scan to determine the cause of his apparent obstruction.
CT abdomen revealed the following:
Dilated jejunum and proximal ileum with no obvious transition point.
Inguinal hernia with a closely related small bowel loop, raising the possibility of resolved obstruction (Fig. 1).
Figure 1:
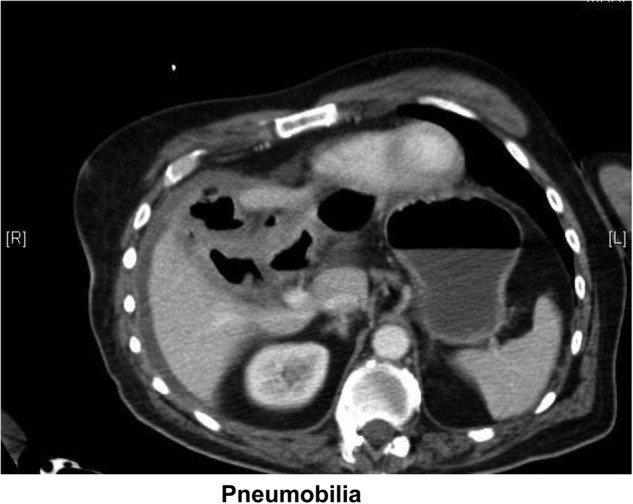
Transverse section from abdominal CT showing pneumobilia.
This was then re-reviewed by a specialist GI radiologist who added the following:
Pneumobilia with cholecystoduodenal fistula secondary to gallstone passage.
Small bowel obstruction with transition in the distal ileum probably due to obstructing gallstone (Fig. 2).
Figure 2:

Transverse section from abdominal CT showing a small bowel obstruction with arrow indicating an intraluminal gallstone.
Given the paucity of information elicited from the patient in terms of history, the differential diagnoses were based on the results of the CT scan. The patient has small bowel obstruction the causes of which appeared to be either secondary to inguinal hernia or gallstone ileus. The treatment of which is very different, hernia being treated with an inguinal repair and gallstone ileus being treated with either laparoscopic resection or laparotomy. The decision was made to proceed to laparotomy on the basis that if the obstruction was secondary to hernia, a resection may well need to be performed, the same approach would also allow the resection for gallstone ileus. In addition, gallstone ileus was felt to be the more likely diagnosis given the presence of pneumobilia.
He was taken for laparotomy with the intention to perform an enterotomy to remove the gallstone and relieve the obstruction. On opening the abdomen, he was found to have a grossly dilated small bowel with a 3-cm gallstone which was freely mobile in the distal ileum. This was abutting a large caecal mass in keeping with a tumour, which had not previously been reported on a CT scan (Figs 3 and 4).
Figure 3:

Intraoperative image indicating a caecal mass.
Figure 4:

Intraoperative image indicating a 3-cm gallstone abutting the ileocaecal valve.
Ileocaecectomy was performed with double-barrelled ileo-colostomy formation. A formal right hemi-colectomy was not performed due to the presence of a cholecystoduodenal fistula making mobilization of the hepatic flexure hazardous.
Histology of the specimen confirmed a mucinous adenocarcinoma of the caecum extending into the distal ileum arising from an area of extensive carpet villous adenoma. The lesion was extending into the muscularis propria with no extramural spread. On this basis it was staged as a Dukes A pT2pN0 tumour.
The gentleman has recovered well postoperatively and was transferred back to his nursing home following a 10-day postoperative stay.
DISCUSSION
Gallstone ileus is an uncommon complication of gallstone disease, occurring in ∼0.5% of cases. It is however a more common cause of non-strangulating mechanical small bowel obstruction, accounting for 1–4%, increasing to 25% of cases in the elderly [1].
It commonly occurs as a result of chronic cholecystitis causing adhesion of the gallbladder to the small bowel. This leads to fistulation and release of gallstones into the bowel. This then results in impaction of the released stone at the ileocaecal valve [2].
As a result of the site of obstruction being the same, it is not uncommon for gallstone ileus and caecal mass to be confused prior to surgery. The main distinguishing features of gallstone ileus over caecal mass are small bowel obstruction with the presence of pneumobilia and a gallstone in the right iliac fossa on X-ray/CT, referred to as Rigler's Triad [3].
This case has all the features of Rigler's triad suggestive of gallstone ileus, but the intraluminal gallstone proved to be incidental with the stone moving freely within the lumen. The cause of the obstruction was the caecal tumour, which was not evident on preoperative imaging. There have been no previously reported cases of concurrent gallstone ileus and caecal tumour in the literature.
Conflict of interest statement
None declared
REFERENCES
- 1.Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60:441. [PubMed] [Google Scholar]
- 2.Summerton SL, Hollander AC, Stassi J, Rosenberg HK, Carroll SF. US case of the day. Gallstone ileus. Radiographics. 1995;15:493–5. doi: 10.1148/radiographics.15.2.7761654. [DOI] [PubMed] [Google Scholar]
- 3.Lassandro F, Romano S, Ragozzino A, Rossi G, Valente T, Ferrara I, et al. Role of helical CT in diagnosis of gallstone ileus and related conditions. AJR Am J Roentgenol. 2005;185:1159–65. doi: 10.2214/AJR.04.1371. [DOI] [PubMed] [Google Scholar]