

Abstract
AIM: To determine the diagnostic accuracy and radiation dose of conventional radiography and multidetector computed tomography (MDCT) in suspected scaphoid fractures.
METHODS: One hundred twenty-four consecutive patients were enrolled in our study who had suffered from a wrist trauma and showed typical clinical symptoms suspicious of an acute scaphoid fracture. All patients had initially undergone conventional radiography. Subsequent MDCT was performed within 10 d because of persisting clinical symptoms. Using the MDCT data as the reference standard, a fourfold table was used to classify the test results. The effective dose and impaired energy were assessed in order to compare the radiation burden of the two techniques. The Wilcoxon test was performed to compare the two diagnostic modalities.
RESULTS: Conventional radiography showed 34 acute fractures of the scaphoid in 124 patients (42.2%). Subsequent MDCT revealed a total of 42 scaphoid fractures. The sensitivity of conventional radiography for scaphoid fracture detection was 42.8% and its specificity was 80% resulting in an overall accuracy of 59.6%. Conventional radiography was significantly inferior to MDCT (P < 0.01) concerning scaphoid fracture detection. The mean effective dose of MDCT was 0.1 mSv compared to 0.002 mSv of conventional radiography.
CONCLUSION: Conventional radiography is insufficient for accurate scaphoid fracture detection. Regarding the almost negligible effective dose, MDCT should serve as the first imaging modality in wrist trauma.
Keywords: Musculoskeletal imaging, Scaphoid fracture, Multidetector computed tomography, Biplane radiography, Emergency radiology, Diagnostic accuracy, Wrist trauma, Dose calculation
Core tip: Correct diagnosis of acute wrist trauma with suspected scaphoid fractures is a challenging topic in every emergency department. Based on our data, conventional radiography has to be considered as insufficient for accurate scaphoid fracture detection. Regarding the high diagnostic accuracy and low effective dose of multidetector computed tomography, it should be implemented as the imaging modality of first choice in suspected fractures of the scaphoid.
INTRODUCTION
Acute wrist trauma with suspected fracture of the scaphoid is a common presentation in an emergency department (ED) around the world. It is considered as the most common fracture of the carpal bones[1-3].
Acute scaphoid fractures are widely seen in young, active adults[1-5] or sportsmen[6,7] who have experienced a fall on the outstretched hand. Usually, clinical examination and biplane radiography are the first diagnostic steps[8]. Although snuffbox tenderness, limited range of motion and swelling are 3 any evidence of an acute fracture[5,9,10].
Conversely, in a patient with only mild symptoms subsequent diagnostic imaging may demonstrate a dislocated fracture[11].
In clinical practice, following a negative standard radiography patients are initially treated with immobilization using a plaster cast and an appointment is scheduled 7-14 d later including repeated biplane radiography[12,13].
In a recent review study, Brookes-Fazakerley et al[14] compared the imaging protocols between 130 institutions within the United Kingdom and demonstrated a huge inconsistency concerning the imaging practice in suspected scaphoid fractures[14]. Thirty-one percent of the institutions tend to perform a repeat radiograph at the first clinic review, within two weeks post-injury, although the limited value of this approach has been underlined before[11,15].
In contrast to the international treatment, the German society of trauma (DGU) supports early cross-sectional imaging [multidetector computed tomography (MDCT)] in their guidelines[8,16,17].
During the last decade, cross-sectional imaging has gained in prominence in the detection of scaphoid fractures. In particular, MDCT has achieved acceptance due to its high resolution, diagnostic accuracy and comparatively low cost[18,19]. Further, due to consistent technical development the radiation burden of MDCT can be limited to a minimum, enhancing the use of MDCT in trauma imaging even in younger adults.
The purpose of the present study was to assess the diagnostic accuracy of standard radiography in patients with suspected scaphoid fracture in an intra-individual comparison to MDCT. Depending on these results, we intended to re-evaluate the diagnostic algorithm applied in acute wrist trauma with regard to time to recovery, radiation dose and financial cost estimation.
MATERIALS AND METHODS
Patient population
In this retrospective study the data sets of all patients admitted to the ED of our university medical center after acute wrist trauma and suspected scaphoid fracture between January 2011 and January 2013 were included. The local institutional review board approved this study, and informed consent was waived owing to the retrospective nature of the study.
The inclusion criteria were defined as follows: (1) Acute wrist trauma with suspected scaphoid fracture; (2) Snuffbox tenderness in the clinical examination; and (3) Initial biplane projection radiography and a MDCT scan of the wrist within an interval of less than 10 d. The exclusion criteria were set as follows: (1) Prior history of scaphoid fracture; and (2) Follow-up imaging after surgical intervention.
Applying this approach, a total of 124 patients were identified who met all inclusion criteria. Their mean age was 49 years ± 21 (range 16-91 years) to a high extent representing working population. Sixty-six patients were male and fifty-eight patients were female.
Biplane radiography
Within the ED, biplane radiography was performed using a commercially available flat detector direct digital system (Digital Diagnost; Philips, Best, The Netherlands). Anterior-posterior, lateral and oblique projections were conducted. The central ray was centered on the proximal carpal bones. The imaging parameters were set as follows: tube current 1.9 mAs, 115 cm film-focus distance and voltage 50 kVp. Imaging was performed with the patient seated on a chair, placing his hand on the bucky table in three to four different positions. If present, casts were removed by a trauma surgeon for the imaging procedure.
MDCT
A 256-slice MDCT (Brilliance iCT; Philips Healthcare, Best, the Netherlands) was performed (voltage, 120 kVp; eff. current-time product, 70 mAs) on each patient, who was placed in the swimmer’s position. Transverse images were reconstructed with a 1 mm slice thickness and an increment of 0.5 mm, creating an overlap of 50%. Further, coronal and sagittal reconstructions were post-processed with a slice thickness of 2 mm in standard bone window settings (Center, 1000 HU; Width, 2500 HU).
Key findings for scaphoid fractures at biplane radiography and MDCT: In the anterior-posterior and lateral view the three arcs of Gilula were analyzed searching for signs of carpal instability[20]. The bone pattern, discontinuity of the cortex, avulsion fracture and subluxation of any carpal bone were examined.
The scapholunate joint space was analyzed as well as the soft tissues surrounding the scaphoid bone. In an acute scaphoid fracture the para scaphoid fat stripe can be obliterated and dorsal swelling can be observed[21,22].
Dose calculation
For all MDCT data sets the dose length product (mGy × cm) was determined. In biplane radiography we recorded the dose field product (dGy × cm2). For comparative reasons, as in imaging studies of the wrist only skin and bones contribute to the effective dose, other organs can be seen as irrelevant due to their distance from the cone-beam. Hence, the effective dose (Sv) of biplane radiography was assessed by calculating the impaired energy.
Image analysis
A maximum of ten days between the two imaging modalities was defined. All conventional radiographs and MDCT images were examined during daily practice by resident radiologists with two to five years of experience in musculoskeletal radiology. Afterwards, all images were reviewed and confirmed by an attending radiologist with 10 years of experience in musculoskeletal Radiology. Finally, the consensus of the clinical examination and MDCT data was defined as the reference standard and the conventional reports were compared to these.
The focus of this study was to assess the relative sensitivities and specificities of the two modalities in a biased population i.e. those who in retrospect had both investigations within 10 d of each other.
A classification of the detected scaphoid fractures was not part of this investigation and therefore not analyzed.
Statistical analysis
A fourfold table was used to appraise the test results. The statistical analysis included sensitivity, specificity, positive and negative predictive value and the Wilcoxon test.
The authors confirm that the statistical analysis has been carried out with the help of a biomedical statistician prior to the initiation of the study as well as after image readout and final manuscript preparation.
RESULTS
Biplane radiography vs MDCT in patients who were analyzed in both modalities within 10 d because of a suspected scaphoid fracture:
Reading the conventional radiographs, 34 acute fractures of the scaphoid were diagnosed in 124 patients (42.2%, Figure 1). Sixteen fractures were classified as false positive in adjacent MDCT. A total of 42 scaphoid fractures were diagnosed in subsequent MDCT. The sensitivity of conventional radiography for scaphoid fracture detection was therefore 42.8% (18/42) with a specificity of 80.5% (66/82). Hence, the positive predictive value was 52.9% (18/34) whereas the negative predictive value was 73.3% (66/90), resulting in an overall accuracy of 59.6%.
Figure 1.
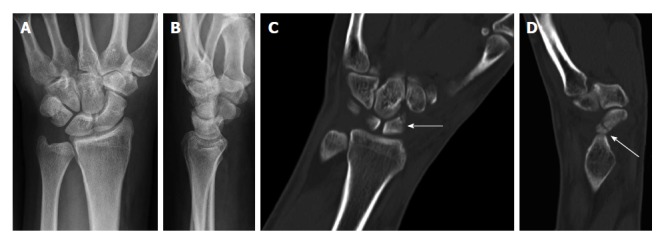
Non-dislocated fissural fracture of the scaphoid that had not been detected by initial conventional radiography (A and B). Cross-sectional multidetector computed tomography clearly depicted the oblique fissural fracture line in the middle third of the scaphoid with coronal (C) and sagittal (D) reformation on the same day.
In this intra-individual comparison, the statistical analysis revealed a distinct inferiority of scaphoid fracture detection by biplane radiography compared to the reference standard of MDCT (P < 0.01).
Secondary findings
Apart from 42 scaphoid fractures, MDCT revealed 66 further fractures in other locations in our patient population. MDCT depicted three fractures of the lunate, 11 fractures of the triquetrum, six of the trapezoid, three fractures of the capitate, three of the hamate, seven fractures of the metacarpals, 27 fractures of the distal radius and six fractures of the distal ulna.
In 27 patients a total of 33 additional fractures apart from a scaphoid fracture were diagnosed. Three fractures of the lunate, two fractures of the triquetrum, four fractures of the trapezoid, three fractures of the capitate, three of the hamate, two fractures of the metacarpals, 12 fractures of the distal radius and four fractures of the distal ulna were accompanied by a scaphoid fracture.
Biplane radiography depicted 41 of these 66 fractures. Twenty-five fractures were misdiagnosed as false negatives, including two lunate, seven triquetrum, four trapezoid, two capitate, three hamate (Figure 2), two metacarpal, four radius and one ulnar fracture. Twenty fractures were treated conservatively with a plaster cast and ambulatory treatment. One capitate, two hamate and two metacarpal fractures underwent subsequent surgery at the trauma department of our university medical center.
Figure 2.
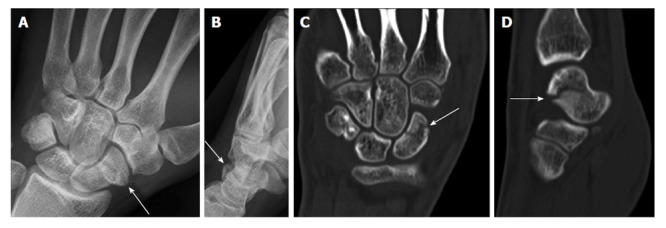
Diagonal fracture line of the scaphoid detected by conventional radiography (A and B) and subsequently confirmed by multidetector computed tomography (C and D) for preoperative planning.
Estimation of radiation doses from radiography and MDCT
The mean effective dose at MDCT was 0.1 mSv. Conventional radiography included only 0.2% of the impaired energy compared to MDCT. Therefore, the effective dose of radiography was determined to be distinctly lower at 0.002 mSv.
DISCUSSION
The results of this study underline the limited diagnostic value of conventional radiography in acute scaphoid fractures. Investigating 124 subjects who underwent conventional radiography and MDCT within 10 d we determined a sensitivity of radiography for scaphoid fracture detection of only 42.8%. The positive predictive value was as low as 52.9%. Moreover, in 24 patients conventional radiography suggested no fracture although subsequent MDCT could clearly demonstrate a fracture line (Figure 3). Therefore, it can be assumed that early diagnosis and treatment planning cannot be assured if diagnosis relies on biplane radiography only.
Figure 3.
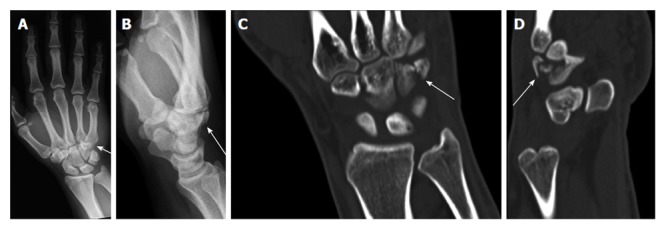
Conventional radiography (A and B) and multidetector computed tomography (C and D) revealed an acute hamate fracture as a secondary finding.
This is in concordance with recent reports supporting MDCT as a diagnostic modality of high diagnostic accuracy in scaphoid fracture detection[23-26] whereas in these reports radiography also was of limited value[23,25,27]. Stevenson et al[24] showed that using initial MDCT an occult scaphoid fracture can be ruled out with the patient returning to regular activity immediately. Acute scaphoid fractures are typically seen in young adults who fall on the outstretched hand[7,25]. Patients who suffer from an acute scaphoid fracture are almost always part of the working population[25,28]. Therefore an early identification of the injury can help to enable a fast return to work and therefore reduce the injury related socioeconomic impact.
The rate of late complications such as osteonecrosis, pseudarthrosis or chronic pain can be decreased. For example, the blood supply to the scaphoid is predominantly provided by dorsal branches of the radial artery which enter at the waist of the scaphoid[29]. Therefore, dislocated and proximal pole fractures in particular need surgical treatment within a narrow time frame in order to prevent osteonecrosis. In concordance with other investigators, we therefore underline the shortcomings of relying on radiography exclusively[23] and postulate the broad application of MDCT in the acute trauma setting of the wrist. The gains of a rapidly initialized therapy prevail over the possibility of any missed fracture and possible consequences. Based on the German medical fee schedule, comparing the costs of the diagnostic modalities, MDCT is about six times more expensive than conventional radiography (110.75 € vs 17.48 €). Concerning the adverse impact of severe complications and a delayed healing process on medical care expenses and socioeconomic ramifications, these costs can be considered as irrelevant.
There are many factors contributing to the poor results of conventional radiography: First of all, the geometric structure of the scaphoid is complex and fractures are difficult to assess[27,30]. Low inter-observer agreement[7,31] is a known problem and even experienced radiologists may overlook scaphoid fractures[30].
Taking the radiation burden into account, we investigated the impaired energy and effective dose values of radiography and MDCT in the diagnostic workup of the wrist. Indeed, the impaired energy of MDCT exceeded conventional radiography by far. Nevertheless, the effective dose of MDCT was calculated to be approximately 0.1 mSv. Compared to the yearly natural background radiation of approximately 2 mSv in Germany, the radiation dose of an MDCT of the wrist can be considered negligible as evaluated in a recent report[32]. In addition to that, the common issue of radiation exposure from MDCT has been countered by the implementation of iterative reconstruction techniques which allow for a significant dose reduction of up to 75% without loss of anatomical information[6,7,33].
We have not included magnetic resonance imaging[11,15] or bone scintigraphy[8,16,17] into our study design. Both modalities represent complementary imaging approaches which can be used to assess mid-hand fractures with a sensitivity comparable to MDCT[11,15-17], but their availability within the emergency room setup is clearly limited. Therefore, the approach of image acquisition at 256 slice MDCT resembles the optimum most practical setting that can routinely be applied in daily trauma care.
Certain limitations of the presented study have to be addressed. First, the selection bias based on the exclusive investigation of patients with aggravated symptoms who underwent initial conventional radiography prior to MDCT has to be considered. Second, the retrospective study design has to be considered as a further limitation. Hence, a prospective evaluation of MDCT may be required to prospectively underline the presented findings of our study.
In conclusion, the results of the presented study underline the exceeding value of 256 slice MDCT in the diagnostic workup of acute wrist trauma in suspected scaphoid fractures. If trauma and clinical presentation are suggestive of any fracture, conventional radiography should be ignored and replaced by MDCT as the diagnostic imaging approach of first choice and any hesitation due to elevated costs or radiation dose should no longer be sustained.
COMMENTS
Background
Scaphoid fractures are a challenging topic in every emergency department. In daily routine, initial X-ray often does not securely rule out a fracture and consequent multidetector computed tomography (MDCT) is added. In the presented study the authors analyzed the diagnostic accuracy of both entities and tried to formulate a new algorithm for daily clinical routine.
Research frontiers
Scaphoid fractures occur mainly in young and active people. They need an accurate and early diagnosis in order to minimize days of absence from work. Undetected or delayed diagnosed scaphoid fractures can lead to pseudarthrosis and prolonged pain.
Innovations and breakthroughs
Based on the authors’ data, initial X-ray, which is requested in almost every patient suspected of a scaphoid fracture, is not necessary. The diagnostic accuracy of conventional radiography in scaphoid fractures is very poor. Many fractures are missed and not securely ruled out. MDCT is clearly superior and should be considered as necessary in every patient.
Applications
To the authors’ opinion, MDCT should serve as the imaging modality of first choice in the diagnostic workup of suspected fractures of the scaphoid. The effective doses of MDCT of the wrist can be regarded as negligible and the patients benefit clearly supports the implementation.
Terminology
To knowledge, all unusual terms or abbreviations are explained in the context and should be understandable to the reader.
Peer review
This is a good paper suitable for publication.
Footnotes
P- Reviewer: Pinto A S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Ethics approval: The study was reviewed and approved by the local ethics committee (WF-061/13).
Informed consent: Due to the retrospective study design exclusively involving data sets from past examinations taken from the local PACS system, no written informed consent was assessable.
Conflict-of-interest: None of the authors has to declare any conflict of interest in the presented study.
Data sharing: Technical appendix, statistical code, and dataset available from the corresponding author at c.behzadi@uke.de. Informed consent was not obtained but the presented data are anonymized and risk of identification is low.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: September 24, 2014
First decision: November 19, 2014
Article in press: December 31, 2014
References
- 1.Munk PL, Lee MJ, Logan PM, Connell DG, Janzen DL, Poon PY, Worsley DF, Coupland D. Scaphoid bone waist fractures, acute and chronic: imaging with different techniques. AJR Am J Roentgenol. 1997;168:779–786. doi: 10.2214/ajr.168.3.9057534. [DOI] [PubMed] [Google Scholar]
- 2.Dunn AW. Fractures and dislocations of the carpus. Surg Clin North Am. 1972;52:1513–1538. doi: 10.1016/s0039-6109(16)39895-4. [DOI] [PubMed] [Google Scholar]
- 3.Brøndum V, Larsen CF, Skov O. Fracture of the carpal scaphoid: frequency and distribution in a well-defined population. Eur J Radiol. 1992;15:118–122. doi: 10.1016/0720-048x(92)90135-v. [DOI] [PubMed] [Google Scholar]
- 4.Ring D, Jupiter JB, Herndon JH. Acute fractures of the scaphoid. J Am Acad Orthop Surg. 1999;8:225–231. doi: 10.5435/00124635-200007000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Parvizi J, Wayman J, Kelly P, Moran CG. Combining the clinical signs improves diagnosis of scaphoid fractures. A prospective study with follow-up. J Hand Surg Br. 1998;23:324–327. doi: 10.1016/s0266-7681(98)80050-8. [DOI] [PubMed] [Google Scholar]
- 6.Geyer LL, Körner M, Hempel R, Deak Z, Mueck FG, Linsenmaier U, Reiser MF, Wirth S. Evaluation of a dedicated MDCT protocol using iterative image reconstruction after cervical spine trauma. Clin Radiol. 2013;68:e391–e396. doi: 10.1016/j.crad.2012.11.025. [DOI] [PubMed] [Google Scholar]
- 7.Barton N. Sports injuries of the hand and wrist. Br J Sports Med. 1997;31:191–196. doi: 10.1136/bjsm.31.3.191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stürmer KMH. Leitlinie Skaphoidfraktur. S1 Leitlinie, Deutsche Gesellschaft für Unfallchirurgie: 2008. pp. 1–17. [Google Scholar]
- 9.Waizenegger M, Barton NJ, Davis TR, Wastie ML. Clinical signs in scaphoid fractures. J Hand Surg Br. 1994;19:743–747. doi: 10.1016/0266-7681(94)90249-6. [DOI] [PubMed] [Google Scholar]
- 10.Kozin SH. Incidence, mechanism, and natural history of scaphoid fractures. Hand Clin. 2001;17:515–524. [PubMed] [Google Scholar]
- 11.Hunter JC, Escobedo EM, Wilson AJ, Hanel DP, Zink-Brody GC, Mann FA. MR imaging of clinically suspected scaphoid fractures. AJR Am J Roentgenol. 1997;168:1287–1293. doi: 10.2214/ajr.168.5.9129428. [DOI] [PubMed] [Google Scholar]
- 12.Mulkens TH, Marchal P, Daineffe S, Salgado R, Bellinck P, te Rijdt B, Kegelaers B, Termote JL. Comparison of low-dose with standard-dose multidetector CT in cervical spine trauma. AJNR Am J Neuroradiol. 2007;28:1444–1450. doi: 10.3174/ajnr.A0608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Steinmann SP, Adams JE. Scaphoid fractures and nonunions: diagnosis and treatment. J Orthop Sci. 2006;11:424–431. doi: 10.1007/s00776-006-1025-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brookes-Fazakerley SD, Kumar AJ, Oakley J. Survey of the initial management and imaging protocols for occult scaphoid fractures in UK hospitals. Skeletal Radiol. 2009;38:1045–1048. doi: 10.1007/s00256-008-0640-3. [DOI] [PubMed] [Google Scholar]
- 15.Tiel-van Buul MM, Roolker W, Broekhuizen AH, Van Beek EJ. The diagnostic management of suspected scaphoid fracture. Injury. 1997;28:1–8. doi: 10.1016/S0020-1383(96)00127-1. [DOI] [PubMed] [Google Scholar]
- 16.Beeres FJ, Rhemrev SJ, den Hollander P, Kingma LM, Meylaerts SA, le Cessie S, Bartlema KA, Hamming JF, Hogervorst M. Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid fractures. J Bone Joint Surg Br. 2008;90:1205–1209. doi: 10.1302/0301-620X.90B9.20341. [DOI] [PubMed] [Google Scholar]
- 17.Rhemrev SJ, Ootes D, Beeres FJ, Meylaerts SA, Schipper IB. Current methods of diagnosis and treatment of scaphoid fractures. Int J Emerg Med. 2011;4:4. doi: 10.1186/1865-1380-4-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kusano N, Churei Y, Shiraishi E, Kusano T. Diagnosis of occult carpal scaphoid fracture: a comparison of magnetic resonance imaging and computed tomography techniques. Tech Hand Up Extrem Surg. 2002;6:119–123. doi: 10.1097/00130911-200209000-00004. [DOI] [PubMed] [Google Scholar]
- 19.Hindman BW, Kulik WJ, Lee G, Avolio RE. Occult fractures of the carpals and metacarpals: demonstration by CT. AJR Am J Roentgenol. 1989;153:529–532. doi: 10.2214/ajr.153.3.529. [DOI] [PubMed] [Google Scholar]
- 20.Gilula LA. Carpal injuries: analytic approach and case exercises. AJR Am J Roentgenol. 1979;133:503–517. doi: 10.2214/ajr.133.3.503. [DOI] [PubMed] [Google Scholar]
- 21.Terry DW, Ramin JE. The navicular fat stripe: a useful roentgen feature for evaluating wrist trauma. Am J Roentgenol Radium Ther Nucl Med. 1975;124:25–28. doi: 10.2214/ajr.124.1.25. [DOI] [PubMed] [Google Scholar]
- 22.Banerjee B, Nashi M. Abnormal scaphoid fat pad: is it a reliable sign of fracture scaphoid. Injury. 1999;30:191–194. doi: 10.1016/s0020-1383(98)00240-x. [DOI] [PubMed] [Google Scholar]
- 23.Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008;190:10–16. doi: 10.2214/AJR.07.2699. [DOI] [PubMed] [Google Scholar]
- 24.Stevenson JD, Morley D, Srivastava S, Willard C, Bhoora IG. Early CT for suspected occult scaphoid fractures. J Hand Surg Eur Vol. 2012;37:447–451. doi: 10.1177/1753193411428993. [DOI] [PubMed] [Google Scholar]
- 25.Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg. 1999;33:423–426. doi: 10.1080/02844319950159145. [DOI] [PubMed] [Google Scholar]
- 26.Cruickshank J, Meakin A, Breadmore R, Mitchell D, Pincus S, Hughes T, Bently B, Harris M, Vo A. Early computerized tomography accurately determines the presence or absence of scaphoid and other fractures. Emerg Med Australas. 2007;19:223–228. doi: 10.1111/j.1742-6723.2007.00959.x. [DOI] [PubMed] [Google Scholar]
- 27.Puopolo SM, Rettig ME. Management of acute scaphoid fractures. Bull Hosp Jt Dis. 2003;61:160–163. [PubMed] [Google Scholar]
- 28.Krasin E, Goldwirth M, Gold A, Goodwin DR. Review of the current methods in the diagnosis and treatment of scaphoid fractures. Postgrad Med J. 2001;77:235–237. doi: 10.1136/pmj.77.906.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Filan SL, Herbert TJ. Herbert screw fixation of scaphoid fractures. J Bone Joint Surg Br. 1996;78:519–529. [PubMed] [Google Scholar]
- 30.Gale SC, Gracias VH, Reilly PM, Schwab CW. The inefficiency of plain radiography to evaluate the cervical spine after blunt trauma. J Trauma. 2005;59:1121–1125. doi: 10.1097/01.ta.0000188632.79060.ba. [DOI] [PubMed] [Google Scholar]
- 31.Dorsay TA, Major NM, Helms CA. Cost-effectiveness of immediate MR imaging versus traditional follow-up for revealing radiographically occult scaphoid fractures. AJR Am J Roentgenol. 2001;177:1257–1263. doi: 10.2214/ajr.177.6.1771257. [DOI] [PubMed] [Google Scholar]
- 32.Biswas D, Bible JE, Bohan M, Simpson AK, Whang PG, Grauer JN. Radiation exposure from musculoskeletal computerized tomographic scans. J Bone Joint Surg Am. 2009;91:1882–1889. doi: 10.2106/JBJS.H.01199. [DOI] [PubMed] [Google Scholar]
- 33.Laqmani A, Buhk JH, Henes FO, Klink T, Sehner S, von Schultzendorff HC, Hammerle D, Nagel HD, Adam G, Regier M. Impact of a 4th generation iterative reconstruction technique on image quality in low-dose computed tomography of the chest in immunocompromised patients. Rofo. 2013;185:749–757. doi: 10.1055/s-0033-1335577. [DOI] [PubMed] [Google Scholar]