

Abstract
Background: Scarring is an unfortunate and frequent complication of acne, resulting in significant psychological distress for patients. Fortunately, numerous treatment options exist for acne scarring. Objectives: To extensively review the literature on treatment options for atrophic acne scarring. Materials and methods: A comprehensive literature search was conducted on the following topics: dermabrasion, subcision, punch techniques, chemical peels, tissue augmentation, and lasers. Results: The literature supports the use of various treatment modalities; superior results may be achieved when multiple modalities are combined for a multi-step approach to scarring. Conclusion: The safety and efficacy of various treatment devices for acne scarring is well established, but there is a paucity of split-face trials comparing modalities.
Acne vulgaris is a common skin disease, affecting nearly all adolescents and 12 to 51 percent of adults aged 20 to 49.1-3 Scarring is a common sequela, estimated to occur in up to 95 percent of acne patients4 and resulting in significant psychological distress for many individuals. Given its impact on self-esteem, social interactions, and even the ability to obtain employment,5 early and effective treatment of acne scarring is paramount.
Acne scarring may be either atrophic or hypertrophic. Atrophic acne scars are further subdivided morphologically into boxcar, icepick, or rolling, with the choice of treatment modality often based on scar type. Over the past few decades, a wide variety of therapeutic interventions have been developed to treat acne scars, including dermabrasion, subcision, punch techniques, chemical peels, tissue augmentation, and laser. Herein, the authors review the various treatments available for atrophic acne scarring.
DERMABRASION
Dermabrasion, a treatment utilized since the 1950s, involves the use of a serrated wheel, diamond embedded fraises, sterilized sandpaper or wire brush attached to a rapidly rotating handpiece that evenly abrades the skin to the papillary dermis. In contrast, microdermabrasion utilizes aluminum oxide crystals delivered through a nozzle to superficially abrade the stratum corneum through a series of microlacerations.6 For acne scarring, dermabrasion may be particularly helpful in softening sharper scar edges. The technique, however, is highly operator-dependent, with error resulting in significant scarring. Additional disadvantages include postoperative pain and healing times of up to one month, with the tendency to form milia.6 As a result of these disadvantages, dermabrasion has largely been replaced by resurfacing lasers. In a prospective, split-scar study comparing diamond-fraise dermabrasion to fractionated CO2 laser, two laser treatments resulted in equivalent improvement of acne scarring at three months, with significantly less adverse events than in the dermabrasion-treated group.7 In the authors’ opinion, the poor safety profile, long recovery time, and operator-dependent technique make dermabrasion an inferior choice to laser therapy.
SUBCISION
Subcutaneous incisionless surgery (subcision) was first introduced in 1995 as an effective treatment for rolling scars.8 In this procedure, a hypodermic, tribevelled, or filter needle is introduced into the subdermal plane to undermine the scar through a series of backward and forward motions, followed by horizontally rotating the needle in a fanning motion.9 These motions loosen the fibrotic adhesions that cause the bound-down appearance of rolling scars and create a wound environment amenable to collagen deposition. The bleeding and subsequent clot formation that result from the procedure aid in elevating the skin from the underlying scar tissue, generating a potential space for neocollagenesis. In a study of 40 patients undergoing subcision for rolling scars, the overall degree of improvement was rated 51 percent by patients and 50 to 60 percent by investigators.10 Although there were no serious adverse events in this study, 5 to 10 percent of patients in other studies have developed hypertrophic scarring requiring treatment with intralesional steroids.11
Figure 1.
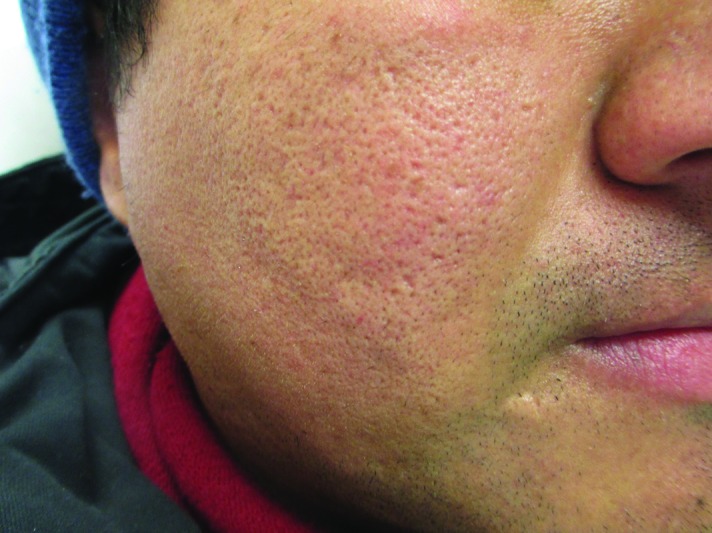



Atrophic acne scar types: (A) icepick, (B) boxcar, (C) icepick (black arrow) and boxcar (blue arrow), (D) rolling.
Figure 2.
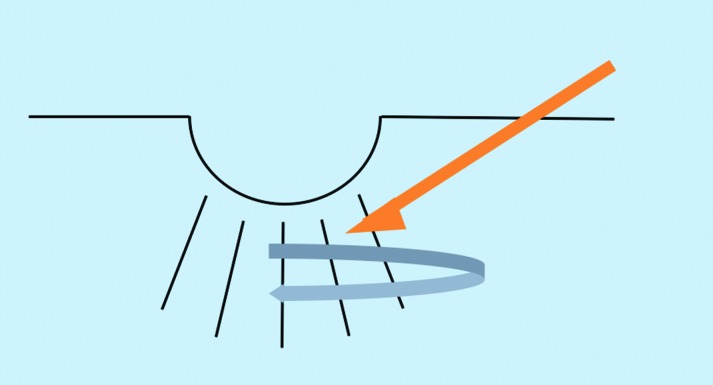
Schematic demonstrating subcision. A hypodermic, tribevelled, or filter needle is inserted into the subdermal plane and rotated in a fanning motion to undermine the scar, disrupting fibrous attachments.
Figure 3.

Acne scars treated with skin needling: a revolving barrel equipped with multiple rows of needles is rolled across the skin.
(Adapted with permission from Fabbrocini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scarring treatment using skin needling. Clin Exp Dermatol. 2009;34:874-879).
Figure 4.

The CROSS technique (A) before and (B) shortly after the procedure.
(Adapted with permission from Lee JB, Chung WG, Kwahck H, Lee KH. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg. 2002;28:1017-1021.)
Figure 5.

Diagram of the Airgent handpiece used for subdermal minimal surgery. A needleless hypodermic inoculator delivers hyaluronic acid subdermally through a high pressure jet.
(Adapted with permission from Halachmi S, Ben Amitai D, Lapidoth M. Treatment of acne scars with hyaluronic acid: an improved approach. J Drugs Dermatol. 2013;12:e121—e123.)
Compared to other modalities, subcision was recently rated statistically significantly higher among patients than dermal fillers in a randomized, prospective, split-face comparison at three months (p=0.03) and trended toward increased satisfaction at six months (p=0.12). Blinded evaluators leaned toward subcision at three months (p=0.12) and showed no preference at six months (p=0.69).12
Although subcision is adequate stand-alone treatment, improved results are achieved when it is combined with other modalities. In a split-face, single-patient trial of subcision alone versus subcision and the nonablative 1320nm neodymium-doped:yttrium aluminum garnet (Nd:YAG) laser at two-week intervals, the combination treatment was superior.13 By loosening deep fibrous attachments, subcision may make acne scars more amenable to other treatment modalities as part of a multi-step approach.
SKIN NEEDLING
Skin needling, sometimes referred to as collagen induction therapy (CIT), involves vertically puncturing the skin to release scar tissue and promote neocollagenesis in a manner analogous to subcision. Specific tools have been designed for the purpose of skin needling, comprised of a rolling barrel equipped with multiple rows of needles. The needling tool is rolled across the skin in multiple directions, penetrating to a depth of 0.1 to 1.3mm, depending upon the pressure applied. The creation of small holes by the needling tool is analogous to the way in which fractional ablative lasers create noncontiguous columns of thermal injury, with healthy tissue interspersed to promote healing. Several authors have also described the use of a tattoo gun to “needle abrade” small acne scars.14 In a study of 33 patients, analysis by photography as well as cutaneous casts of the scars made before and after two sessions of skin needling showed improvement in scar depth of up to 25 percent.15
PUNCH TECHNIQUES
Many treatment modalities do not effectively correct icepick scars with depths that reach up to 2mm. For these scars, punch techniques—including punch excision, elevation, and grafting—may be more suitable. In punch excision, a scar is removed with a punch biopsy tool and the site is sutured or allowed to heal by secondary intention. In punch elevation, the punched-out scar is elevated to the level of the surrounding skin and secondarily heals like a graft. In the case of punch grafting, the scar is first excised and discarded as with punch excision; in its place, a full-thickness skin graft is positioned, taken from an inconspicuous site, such as the postauricular scalp. Studies on the effectiveness of punch techniques are largely limited to dated, small case reports involving few patients. In these reports, the grafts were placed slightly elevated above surrounding skin, with dermabrasion performed 4 to 6 weeks later to correct any residual surface abnormalities.16,17 One disadvantage of this procedure is that it is often a painstakingly slow process. Complications may also arise, including graft depression, failure of the graft to take, or formation of sinus tracts.16 When combined with other modalities, punch techniques allow for the treatment of deep icepick scars so that less aggressive resurfacing may subsequently be performed to achieve optimal cosmetic results. For example, Grevelink et al18 demonstrated that excellent results may be achieved when punch excision is combined with concurrent CO2 laser resurfacing.
CHEMICAL PEELS AND THE CROSS TECHNIQUE
Although there is some data to support the use of superficial chemical peels for acne,19 in the authors’ experience, results are modest at best. Medium-depth peels, such as trichloroacetic acid (TCA) have shown varying results for acne scars, but are limited by their unpredictable degree of penetration beyond the papillary dermis. In a study of 15 patients receiving 1 to 3 peels consisting of Jessner’s solution followed by 35% TCA for “crateric” or icepick scarring, at least some improvement was observed in 14 of 15 patients; however, significant improvement was seen in only one patient. Furthermore, 73.4 percent of patients experienced postinflammatory hyperpigmentation, which lasted up to three months in some individuals.20 Deeper peels, such as phenol, can also treat acne scars. In one study, 7 out of 11 patients achieved more than 50-percent improvement. However, significant side effects, such as scar formation and hypopigmentation, persisted beyond six months.21 Given the high risk of side effects coupled with only modest results, it is the authors’ opinion that deep peels rarely be employed to treat acne scars.
In 2002, Lee et al22 reported a new technique using focal application of TCA which they called the chemical reconstruction of skin scars (CROSS) method. This technique was designed to take advantage of the dermal thickening and collagen production that occurs when higher concentrations of TCA are applied, while minimizing such side effects as scarring and dyspigmentation. TCA is applied to the epithelial lining of the scar until frosting occurs. In the original study, 65 patients with skin types IV to V were treated with either 65 or 100% TCA using the CROSS method. Eighty-two percent of patients in the 65% TCA group and 94 percent of patients in the 100% TCA group achieved improvement of 50 to 70 percent. Furthermore, all patients in the 100% group who received 5 to 6 treatments achieved improvement greater than 70 percent.22 Subsequent studies have further elucidated the effectiveness of the CROSS technique, particularly for icepick scarring.23,24 In a comparative study of 100% TCA CROSS to skin needling, there was a trend toward increased improvement in the TCA CROSS group—75.3 percent improvement versus 68.3 percent after four sessions of either treatment.25
TISSUE AUGMENTATION
Soft tissue augmentation is aimed at replacing tissue volume as well as stimulating collagen production by native fibroblasts in acne scars.26 Over the years, collagen fillers have fallen out of favor, replaced by products with less allergenic potential, including hyaluronic acid (HA), calcium hydroxyapatite, poly-L-lactic acid (PLLA), polymethylmethacrylate, and autologous fat transfer. Typically, dermal fillers are reserved for larger, rolling scars given the size of the injected molecules and the degree of precision required for delivery.
Although HA fillers are commonly used for scars,27 there is little data in the literature regarding the use of HA fillers specifically for acne scars. Even for depressed scars, reports in the literature are limited to small case studies, albeit with excellent results achieved.28 In the authors’ experience, HA represents an exceptional option for treatment of rolling acne scars. Belotero (Merz Aesthetics, Greenborough, North Carolina), a relatively new HA filler on the market, is a good choice for acne scars as it does not carry the risk of the Tyndall effect, as do other HA fillers. More recently, a new technique known as subdermal minimal surgery (Airgent, PerfAction, Inc., Rehovot, Israel) has been developed in which a needleless hypodermic inoculator delivers HA through a high pressure jet, allowing for more precise and even radial dispersion into the dermal planes. In a study of 10 patients, eight had at least 50-percent improvement in acne scar appearance.29
PLLA (Sculptra, Galderma, Fort Worth, Texas) is a synthetic dermal filler originally approved for the treatment of human immunodeficiency virus (HIV) lipoatrophy, but also used with some success for the treatment of atrophic acne scars. While one study found PLLA to improve acne scars after seven treatments, the trend toward increased patient satisfaction over time was not significant.30 Disadvantages of PLLA include the number of treatments and the difficulty in achieving accuracy, with risk of overcorrection.
Calcium hydroxyapatite (Radiesse, Merz Aesthetics) is a semi-permanent filler that has been shown to improve rolling scars; improvement can be seen after just one treatment and at least some degree of improvement maintained for up to 12 months.31
An alternative to temporary fillers, which require repeated treatments at significant cost to the patient, is a permanent filler composed of polymethylmethacryalate microspheres in a water-based gel with 3.5% bovine collagen (Artefill). In a study of 14 patients with atrophic acne scars treated with 1 to 2 sessions of Artefill immediately following subcision, 2 of 14 reported significant improvement (76-100%) and 8 of 16 reported moderate improvement (51-75%).32 Given the permanence of this filler, it is not typically a first choice for acne scars.
FAT TRANSFER
Fat transfer (FT) offers the advantage over synthetic fillers because of its autologous nature. Acne scars are often subcised immediately prior to treatment with FT. Some fat does not survive the transfer process, and survival is often practitioner-dependent. Thus, most patients require subsequent transfer procedures.33 In one study comparing three sessions of fractional CO2 laser to one session of FT in 22 acne scar patients, FT proved more effective.34 In the fractional CO2 laser group, less than 20 percent of patients had excellent scar improvement and 0 had marked scar improvement. Alternatively, in the FT group, scar improvement was graded as 30 percent excellent and 30 percent marked. These studies are weakened by short follow-up periods, as other studies have revealed limited duration of effect when FT is used for other applications.35 Thus, although FT may be effective for acne scarring, results are not permanent and the procedure is highly operator- dependent.
AUTOLOGOUS FIBROBLAST TRANSFER
Autologous fibroblast transfer (AFT) (Laviv, Fibrocell Science, Inc., Exton, Pennsylvania) represents one of the newest filler techniques for treatment of acne scarring. Similar to FT, AFT offers the advantage over other dermal fillers in its low allergenicity potential. Furthermore, although the permanence of FT has been debated,32 AFT has the potential to offer permanent results. In this technique, the patient first undergoes punch biopsies from an inconspicuous site such as the postauricular scalp. From these specimens, fibroblasts are isolated and cultured over several weeks and then injected dermally at the site of the acne scar, where these cells provide a reservoir for new collagen formation and assist in the remodeling of pre-existing extracellular matrix.36 In two double-blind, placebo-controlled trials, AFT led to significant improvement of acne scars compared to placebo, with most patients showing sustained benefit at 12 months. Side effects were limited to temporary erythema and edema.37,38 AFT is an innovative addition to our armamentarium for acne scar revision, but further studies are warranted.
LASER RESURFACING
Over the past decade, laser resurfacing has emerged at the forefront of acne scar treatment. The first lasers to be used for acne scarring were the ablative CO2 and Er:YAG lasers, which emit radiation at wavelengths of 10,600 and 2,940nm, respectively, targeting water in the epidermis to stimulate collagen synthesis. In 1996, Alster et al40 published the largest study to date on the use of ablative CO2 for acne scarring, showing a mean improvement of 81.4 percent in 50 patients with moderate-to-severe acne scars. These results are quite staggering, and it should be noted that in the authors’ experience, such high rates of improvement are not always observed.
Response rates to the original short-pulse Er:YAG lasers ranged from 25 to 90 percent,39 with the largest study of 21 patients reporting mean improvement in acne scarring of 40 percent. Despite the results with these lasers, adverse events, such as postinflammatory hyperpigmentation and prolonged erythema were pronounced.40 Furthermore, for both the CO2 and Er:YAG lasers, more serious complications, including infection and scarring, have been reported.41
Because the traditional 2940nm Er:YAG laser has 12 to 18 times the absorption in water-containing tissue than the CO2 laser, it does not penetrate as deeply into the skin as the CO2 laser. Furthermore, hemostasis is difficult to achieve with the Er:YAG, with increased intraoperative bleeding. In order to address these shortcomings, longer pulsed Er:YAG lasers were developed. In a prospective study of 35 patients with pitted acne scars, results were excellent (>75% improvement) in 36 percent of patients and good (50-75% improvement) in 57 percent.42
Following the advent of ablative lasers, efforts were made to develop devices with a better safety profile, leading to the introduction of the nonablative, long-pulsed 1450nm diode and 1320nm Nd:YAG lasers. These mid-infrared wavelengths target water in the dermis to stimulate collagen synthesis. Both lasers showed modest efficacy after 3 to 6 treatments in improvement of acne scarring.43-45 In a prospective, split-face comparison of 20 patients with atrophic acne scarring treated with the nonablative long-pulsed 1450nm diode and 1320nm NdYAG, all patients demonstrated mild improvement after three treatment sessions, with a trend toward greater scar improvement in the 1450 nm diode group.46
Although side effects were minimal with the nonablative lasers, their efficacy did not compare to traditional ablative laser therapy. In 2004, the introduction of fractional photothermolysis (FP) revolutionized acne scar treatment, as multiple treatments could offer results comparable to ablative resurfacing, but with less downtime and fewer side effects.47 These islands of normal epidermis and dermis interspersed between the columns of laser-treated skin provide a reservoir of healthy cells that may migrate into the injured tissue, thus expediting healing. The first fractional laser (Fraxel, Solta Medical, Mountain View, California) was a 1550nm erbium-doped laser. Geronemus et al48 reported its efficacy in 17 acne patients with ice-pick, boxcar, and rolling scars who received a series of five treatments. Mean clinical improvement ranged from 25 to 50 percent using digital photography and from 22 to 66 percent using typographic imaging. Side effects were limited to temporary postprocedure erythema and edema, with no dyspigmentation or scarring observed.48 In another study of 53 patients, 90 percent achieved clinical improvement of 51 to 75 percent after 2 to 5 monthly treatments.49 Finally, in the largest study to date for non-ablative fractional laser (NAFL), 500 acne scar patients were treated with the 1540nm fractionated laser (Lux 1540, Palomar, Burlington, Massachusetts), with a median improvement of 50 to 75 percent after three treatments.50
In 2007, a second-generation erbium-doped 1550 nm laser (Fraxel SR1500) was approved by the FDA, which delivers a higher pulse energy of up to 70mJ, resulting in deeper tissue penetration. In one study, 18 of 29 patients achieved 50- to 75-percent improvement in acne scarring, while five achieved greater than 75-percent improvement. As with earlier reports, side effects were minimal.
All of the aforementioned studies on NAFL included patients with Fitzpatrick skin type IV and V, with no postinflammatory hyperpigmentation (PIH) observed. However, a more recent study found that even at energies as low as 10mJ, PIH can occur.51 Thus, caution should still be exercised when treating darker skinned individuals with NAFL.
As technology has advanced, ablative fractionated CO2 and erbium lasers have also been developed to achieve more prolonged collagen remodeling. The effectiveness of ablative fractional laser (AFL) was first demonstrated by Chapas et al,52 in which 13 patients with acne scarring received 2 or 3 monthly treatments with fractional CO2 (Fraxel Re:pair Laser Prototype, Solta Medical, Mountain View, California), resulting in a mean scar depth improvement by topographic analysis of 66.8 percent. Side effects included post-procedure erythema, edema, and petechiae, which resolved by seven days. Unlike traditional ablative resurfacing, no delayed onset pigmentary changes were observed.52 Similar results in terms of efficacy and safety have been observed in subsequent studies.53-55 In one study, when AFL was used at a low energy followed by nonablative 1064nm Nd:YAG, clinical efficacy was better than that of AFL alone at a higher energy, with fewer adverse events.56
More recently, Cho et al57 conducted a randomized, blinded, split-face comparison of NAFL to AFL for atrophic acne scarring. Eight patients had half their face treated with a single 1550nm erbium-glass NAFL session, while the other half was treated with a single 10,600nm CO2 AFL session. Three months later, all patients demonstrated equal or greater improvement in scarring with the AFL than NAFL. The benefits of AFL are that it more closely rivals the efficacy of traditional ablative laser therapy than does NAFL, yet without the long downtime and risk of permanent scarring or dyspigmentation seen with ablative lasers.57
MANAGEMENT OF ACNE SCARS DURING TREATMENT WITH CONCOMITANT ISOTRETINOIN
Decades ago, a handful of case series reported the development of keloids and hypertrophic scars after acne scar revision with dermabrasion, argon laser, and the 585nm pulsed dye laser in patients on or having recently completed isotretinoin.58-61 In other instances, patients on isotretinoin were reported to develop spontaneous keloids.62,63 Several authors hypothesized that isotretinoin may lead to exaggerated scarring through stimulation of angiogenesis and the production of collagen inhibitors, with subsequent collagen accumulation. These case reports led to the recommendation that resurfacing of acne scars be delayed for 6 to 12 months after the completion of isotretinoin.64 More recently, however, reports on the successful treatment of acne scarring utilizing such methods as dermabrasion, chemical peels, and laser resurfacing have challenged this recommendation.65,66 For example, Yoon et al67 reported successful treatment of acne scars using the 1550nm erbium-doped fiber laser in 35 patients taking isotretinoin. Similarly, the authors have experienced successful revision of acne scars with various modalities—including fractional CO2 laser—in patients taking isotretinoin. Studies suggest that the immunologic and inflammatory pathways responsible for acne scarring vary among individuals, helping to explain differences in severity and type of acne scarring. Thus, it is possible that the exaggerated scarring observed in earlier case reports may be attributed to individual factors, such as genetics or anatomic location, and not the use of isotretinoin. Early treatment of acne scars is critical for improved patient quality of life. Given the recent cumulative data on the safety of various resurfacing techniques in patients taking isotretinoin, it is the authors’ opinion that current or recent therapy with isotretinoin should not be an absolute contraindication to acne scar revision. At the same time, there are potential legal repercussions should resurfacing treatment during isotretinoin therapy lead to complications; thus, such treatment warrants caution, particularly for less experienced practitioners. Decisions should be made on a case-by-case basis, and a test area should always be performed.
CONCLUSION
Scarring is an unfortunate and frequent complication of acne, resulting in significant psychosocial distress for many patients. Fortunately, there are numerous treatment options available for acne scarring, and often several modalities may be combined to achieve maximum results. Successful treatment of acne scarring requires not only an understanding of appropriate treatments for different scar types, but also skilled execution of the procedure by the physician. In addition, dermatologists must be knowledgeable regarding side effects, post-procedure down-time, and general efficacy of each treatment modality in order to counsel and optimally treat patients. Realistic expectations must be emphasized to achieve patient satisfaction and it is important to counsel patients that there is no single treatment, or even combination thereof, that can achieve 100-percent improvement of acne scarring.
Footnotes
DISCLOSURE:Dr. Hession reports no relevant conflicts of interest. Dr. Graber is a consultant for Medicis.
REFERENCES
- 1.Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity and severity risk factors of acne in high school pupils: a community based study. J Invest Dermatol. 2009;129:2136–2141. doi: 10.1038/jid.2009.47. [DOI] [PubMed] [Google Scholar]
- 2.Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56–59. doi: 10.1016/j.jaad.2007.06.045. [DOI] [PubMed] [Google Scholar]
- 3.Golden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in adults. J Am Acad Dermatol. 1999;41:577–580. [PubMed] [Google Scholar]
- 4.Layton AM, Henderson CA, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303–308. doi: 10.1111/j.1365-2230.1994.tb01200.x. [DOI] [PubMed] [Google Scholar]
- 5.Cunliffe WJ. Unemployment and acne. Br J Dermatol. 1986;115:386. doi: 10.1111/j.1365-2133.1986.tb05757.x. [DOI] [PubMed] [Google Scholar]
- 6.Goodman G. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857–871. doi: 10.1046/j.1524-4725.2000.99232.x. [DOI] [PubMed] [Google Scholar]
- 7.Christophel JJ, Elm C, Endrizzi BT, Hilger PA, Zelickson B. A randomized controlled trial of fractional laser therapy and dermabrasion for scar resurfacing. Dermatol Surg. 2012;38:595–602. doi: 10.1111/j.1524-4725.2011.02283.x. [DOI] [PubMed] [Google Scholar]
- 8.Orentreich DS. Subcutaneous incisionless (subcision) surgery for the correction of depressed acne scars and wrinkles. Dermatol Surg. 1995;21:543–549. doi: 10.1111/j.1524-4725.1995.tb00259.x. [DOI] [PubMed] [Google Scholar]
- 9.Goodman G, Baron J. The management of postacne scarring. Dermatol Surg. 2007;33:1175–1188. doi: 10.1111/j.1524-4725.2007.33252.x. [DOI] [PubMed] [Google Scholar]
- 10.Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005;31:310–317. doi: 10.1111/j.1524-4725.2005.31080. [DOI] [PubMed] [Google Scholar]
- 11.Goodman G. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857–871. doi: 10.1046/j.1524-4725.2000.99232.x. [DOI] [PubMed] [Google Scholar]
- 12.Sage R, Lopiccolo M, Liu A, et al. Subcuticular incision versus naturally sourced porcine collagen filler for acne scars: a randomized split-face comparison. Dermatol Surg. 2011;37:426–431. doi: 10.1111/j.1524-4725.2011.01918.x. [DOI] [PubMed] [Google Scholar]
- 13.Fulchiero G, Parham Vetter P, Obagi S. Subcision and 1320-nm ND:YAG nonablative laser resurfacing for the treatment of acne scars: a simultaneous split-face single patient trial. Dermatol Surg. 2004;30:1356–1360. doi: 10.1111/j.1524-4725.2004.30411.x. [DOI] [PubMed] [Google Scholar]
- 14.Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast Surg. 1997;21:48–51. doi: 10.1007/s002669900081. [DOI] [PubMed] [Google Scholar]
- 15.Fabbrocini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scarring treatment using skin needling. Clin Exp Dermatol. 2009;34:874–879. doi: 10.1111/j.1365-2230.2009.03291.x. [DOI] [PubMed] [Google Scholar]
- 16.Johnson WC. Treatment of pitted scars; punch transplant technique. J Dermatol Surg Oncol. 1986;12:260–265. doi: 10.1111/j.1524-4725.1986.tb01462.x. [DOI] [PubMed] [Google Scholar]
- 17.Solotoff S. Treatment for pitted acne scarring-postauricular punch grafts followed by dermabrasion. Dermatol Surg Oncol. 1986;12:1021–1027. doi: 10.1111/j.1524-4725.1986.tb02086.x. [DOI] [PubMed] [Google Scholar]
- 18.Grevelink JM, White V. Concurrent use of laser skin resurfacing and punch excision in the treatment of facial acne scarring. Dermatol. Surg. 1998;24:527–530. doi: 10.1111/j.1524-4725.1998.tb04201.x. [DOI] [PubMed] [Google Scholar]
- 19.Dreno B, Fischer TC, Perosino E, et al. Expert opinion: efficacy of superficial chemical peels in active acne management--what can we learn from the literature today? Evidence-based recommendations. J Eur Acad Dermatol Venereol. 2011;25:695–704. doi: 10.1111/j.1468-3083.2010.03852.x. [DOI] [PubMed] [Google Scholar]
- 20.Al-Waiz M, Al-Sharqi A. Medium-depth chemical peels in the treatment of acne scars in dark-skinned individuals. Dermatol Surg. 2002;28:383–387. doi: 10.1046/j.1524-4725.2002.01081.x. [DOI] [PubMed] [Google Scholar]
- 21.Park JH, Choi YD, Kim SW, Kim YC, Park SW. Effectiveness of modified phenol peel (Exoderm) on facial wrinkles, acne scars and other skin problems of Asian patients. J Dermatol. 2007;34:17–24. doi: 10.1111/j.1346-8138.2007.00210.x. [DOI] [PubMed] [Google Scholar]
- 22.Lee JB, Chung WG, Kwahck H, Lee KH. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg. 2002;28:1017–1021. doi: 10.1046/j.1524-4725.2002.02095.x. [DOI] [PubMed] [Google Scholar]
- 23.Kitano Y, Uchidda H. Analysis of focal high concentration TCA treatment for atrophic acne scarring. Jap J Plast ReconstrSurg. 2006;49:573–653. [Google Scholar]
- 24.Yug A, Lane JE, Howard MS, Kent DE. Histological study of depressed acne scars treated with serial high concentration (95%) trichloroacetic acid. Dermatol Surg. 2006;32:985–990. doi: 10.1111/j.1524-4725.2006.32220.x. [DOI] [PubMed] [Google Scholar]
- 25.Leheta T, Tawdy A, Hay R, Farid S. Percutaneous collagen induction versus full-concentration trichloroacetic Acid in the treatment of atrophic acne scars. Dermatol Surg. 2011;37:207–216. doi: 10.1111/j.1524-4725.2010.01854.x. [DOI] [PubMed] [Google Scholar]
- 26.Wang F, Garza LA, Kang S, et al. In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;43:155–163. doi: 10.1001/archderm.143.2.155. [DOI] [PubMed] [Google Scholar]
- 27.Richards KN, Rashid RM. Twenty-four month persistence of hyaluronic acid filler for an atrophic scar. J Gosmet Dermatol. 2011;10:311–312. doi: 10.1111/j.1473-2165.2011.00589.x. [DOI] [PubMed] [Google Scholar]
- 28.Richards KN, Rashid RM. Twenty-four month persistence of hyaluronic acid filler for an atrophic scar. J Gosmet Dermatol. Dermatology Online Journal. 2011;1018:311–312. 15. doi: 10.1111/j.1473-2165.2011.00589.x. [DOI] [PubMed] [Google Scholar]
- 29.Halachmi S, Ben Amitai D, Lapidoth M. Treatment of acne scars with hyaluronic acid: an improved approach. J Drugs Dermatol. 2013;12:el21–el23. [PubMed] [Google Scholar]
- 30.Beer K. A single-center, open-label study on the use of injectable poly-L-lactic acid for the treatment of moderate to severe scarring from acne or varicella. Dermatol Surg. 2007;33(Suppl 2):S159–S167. doi: 10.1111/j.1524-4725.2007.33356.x. [DOI] [PubMed] [Google Scholar]
- 31.Goldberg DJ, Amin S, Hussain M. Acne scar correction using calcium hydroxyapatite in a carrier-based gel. J Gosmet Laser Ther. 2006;8:134–136. doi: 10.1080/14764170600891632. [DOI] [PubMed] [Google Scholar]
- 32.Epstein R, Spencer J. Correction of atrophic scars with Artefill: an open-label pilot study. J Drugs Dermatol. 2010;9:1062–1064. [PubMed] [Google Scholar]
- 33.Goodman G. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857–871. doi: 10.1046/j.1524-4725.2000.99232.x. [DOI] [PubMed] [Google Scholar]
- 34.Azzam OA, Atta AT, Sobhi RM, Mostafa PI. Fractional CO (2) laser treatment vs autologous fat transfer in the treatment of acne scars: a comparative study. J Drugs Dermatol. 2013;12:e7–el3. [PubMed] [Google Scholar]
- 35.Eremia S, Newman N. Long-term follow-up after autologous fat grafting: analysis of results from 116 patients followed at least 12 months after receiving the last of a minimum of two treatments. Dermatol Surg. 26:1150–1158. [PubMed] [Google Scholar]
- 36.Weiss RA, Weiss MA, Beasley KL, Munavalli G. Autologous cultured fibroblast injection for facial contour deformities: a prospective, placebo-controlled, phase III clinical trial. Dermatol Surg. 2007;33:263–268. doi: 10.1111/j.1524-4725.2007.33060.x. [DOI] [PubMed] [Google Scholar]
- 37.Weiss R, Weiss MA, Beasley KL, Munavalli G. Autologous cultured fibroblast injection for facial contour deformities: a prospective, placebo-controlled, phase III clinical trial. Dermatol Surg. 2007;33:263–268. doi: 10.1111/j.1524-4725.2007.33060.x. [DOI] [PubMed] [Google Scholar]
- 38.Munavalli GS, Smith S, Maslowski JM, Weiss R. Successful treatment of depressed, distensible acne scars using autologous fibroblasts: a multi-site, prospective, double blind, placebo-controlled clinical trial. Dermatol Surg. 2013;39:1226–1236. doi: 10.1111/dsu.12204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tierney MD. Treatment of acne scarring using a dual-spot-size ablative fractionated carbon dioxide laser: review of the literature. Dermatol Surg. 2011;37:945–961. doi: 10.1111/j.1524-4725.2011.02036.x. [DOI] [PubMed] [Google Scholar]
- 40.Alster TS, West TB. Resurfacing of atrophic facial acne scars with a high-energy, pulsed carbon dioxide laser. Dermatol Surg. 1996;22:151–154. doi: 10.1111/j.1524-4725.1996.tb00497.x. [DOI] [PubMed] [Google Scholar]
- 41.Alster TS. Cutaneous resurfacing with CO2 and erbium: preoperative, intraoperative, and postoperative considerations. Plast Reconstr Surg. 1999;103:619–632. doi: 10.1097/00006534-199902000-00040. [DOI] [PubMed] [Google Scholar]
- 42.Jeong JT, Kye YC. Resurfacing of pitted facial acne scars with a long-pulsed Er:YAG laser. Dermatol Surg. 2001;27:107–110. doi: 10.1046/j.1524-4725.2001.00201.x. [DOI] [PubMed] [Google Scholar]
- 43.Bellew SG, Le C, Weiss MA, et al. Improvement of atrophic acne scars with a 1320 NdYAG laser: a retrospective study. Dermatol Surg. 2005;31:1218–1222. doi: 10.1111/j.1524-4725.2005.31929. [DOI] [PubMed] [Google Scholar]
- 44.Chua SH, Ang P, Khoo LSW, et al. Nonablative 1450-nm diode laser in the treatment of facial atrophic scars in skin type IV and V Asian skin: a prospective clinical study. Dermatol Surg. 2004;30:1287–1291. doi: 10.1111/j.1524-4725.2004.30402.x. [DOI] [PubMed] [Google Scholar]
- 45.Bhatia AC, Dover JS, Arndt KA, et al. Patient satisfaction and reported long-term therapeutic efficacy associated with 1320 nm NDYAG laser treatment of acne scarring and photoaging. Dermatol Surg. 2006;32:346–352. doi: 10.1111/j.1524-4725.2006.32071.x. [DOI] [PubMed] [Google Scholar]
- 46.Tanzi EL, Alster TS. Comparison of a 1450-nm diode laser and a 1320-nm NdYAG laser in the treatment of atrophic acne scars: a prospective clinical and histologic study. Dermatol Surg. 2004;30:152–157. doi: 10.1111/j.1524-4725.2004.30078.x. [DOI] [PubMed] [Google Scholar]
- 47.Manstein D, Herron GS, Sink RK, et al. Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34:426–438. doi: 10.1002/lsm.20048. [DOI] [PubMed] [Google Scholar]
- 48.Geronemus R. Fractional photothermolysis: current and future applications. Lasers Surg Med. 2006;38:169–176. doi: 10.1002/lsm.20310. [DOI] [PubMed] [Google Scholar]
- 49.Alster TS, Tanzi EL, Lazarus M. The use of fractional laser photothermolysis for the treatment of atrophic scars. Dermatol Surg. 2007;33:295–299. doi: 10.1111/j.1524-4725.2007.33059.x. [DOI] [PubMed] [Google Scholar]
- 50.Weiss R, Weiss M, Beasley K. Long-term experience with fixed array 1540 fractional erbium laser for acne scars. Abstract Am Soc Laser Med Surg Conf, Kissimmee, April 2008. [Google Scholar]
- 51.Mahmoud BH, Srivastava D, Janiga JJ, et al. Safety and efficacy of erbium-doped yttrium aluminum garnet fractionated laser for treatment of acne scars in type IV to VI skin. Dermatol Surg. 2010;36:602–609. doi: 10.1111/j.1524-4725.2010.01513.x. [DOI] [PubMed] [Google Scholar]
- 52.Chapas AM, Brightman L, Sukal S, et al. Successful treatment of acneiform scarring with CO2 ablative fractional resurfacing. Lasers Surg Med. 2008;40:381–386. doi: 10.1002/lsm.20659. [DOI] [PubMed] [Google Scholar]
- 53.Ortiz A, Elkeeb L, Truitt A, et al. Evaluation of a novel fractional resurfacing device for the treatment of acne scarring. Abstract presented at American Society for Laser Medicine and Surgery Conference, April 2008, Kissimee, Florida.
- 54.Kim S. Clinical trial of a pinpoint irradiation technique with the CO2 laser for the treatment of atrophic acne scars. J Gosm Laser Ther. 2008;29:1–4. doi: 10.1080/14764170801930080. [DOI] [PubMed] [Google Scholar]
- 55.Cho SB, Lee SJ, Kang JM, et al. The efficacy and safety of 10,600-nm carbon dioxide fractional laser for acne scars in Asian patients. Dermatol Surg. 2009;8:481–485. doi: 10.1111/j.1524-4725.2009.01316.x. [DOI] [PubMed] [Google Scholar]
- 56.Kim S, Cho KH. Clincal trial of dual treatment with an ablative frational laser and a nonablative laser for the treatment of acne scars in Asian patients. Dermatol Surg. 2009;35:1089–1098. doi: 10.1111/j.1524-4725.2009.01193.x. [DOI] [PubMed] [Google Scholar]
- 57.Cho SB, Lee SJ, Oh SH, et al. Non-ablative 1550nm erbium-glass and ablative 10,600nm carbon dioxide fractional lasers for acne scar: a randomized split-face study with blinded response evaluation. JEADV. 2010;24:921–925. doi: 10.1111/j.1468-3083.2009.03551.x. [DOI] [PubMed] [Google Scholar]
- 58.Rubenstein R, Roenigk HH, Stegman SJ. Atypical keloids after dermabrasion of patients taking isotretinoin. J Am Acad Dermatol. 1986;15:280–285. doi: 10.1016/s0190-9622(86)70167-9. [DOI] [PubMed] [Google Scholar]
- 59.Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118:704–706. doi: 10.1111/j.1365-2133.1988.tb02574.x. [DOI] [PubMed] [Google Scholar]
- 60.Bernestein LJ, Geronemus RG. Keloid formation with the 585-nm pulsed dye laser during isotretinoin treatment. Arch Dermatol. 1997;133:111–112. doi: 10.1001/archderm.1997.03890370123029. [DOI] [PubMed] [Google Scholar]
- 61.Katz BE, McFarlane DF. Atypical facial scarring after isotretinoin therapy in a patient with previous dermabrasion. J Am Acad Dermatol. 1994;30:852–853. doi: 10.1016/s0190-9622(94)70096-6. [DOI] [PubMed] [Google Scholar]
- 62.Goihman-Yahr M. Correspondence. Int J Dermatol. 1999;38:228–229. [Google Scholar]
- 63.Manzano R, Herranz P, Borbujo J, et al. Keloid appearance during isotretinoin therapy for acne. Adas Dermo-SifiUogrdficas. 1995;86:123–126. [Google Scholar]
- 64.Rivera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol. 2008;59:659–676. doi: 10.1016/j.jaad.2008.05.029. [DOI] [PubMed] [Google Scholar]
- 65.Bagatin E, Ramos dos Santos Guadanhim L, Yarak S, Kamamoto C, Augusto de Almeida F. Dermabrasion for acne scars during treatment with oral isotretinoin. Dermatol Surg. 2010;36:483–489. doi: 10.1111/j.1524-4725.2010.01474.x. [DOI] [PubMed] [Google Scholar]
- 66.Picosse FR, Yarak S, Cabral NC, Bagatin E. Early chemabrasion for acne scars after treatment with oral isotretinoin. Dermatol Surg. 2012;38:1521–1526. doi: 10.1111/j.1524-4725.2012.02460.x. [DOI] [PubMed] [Google Scholar]
- 67.Yoon JH, Park EJ, Kwon IH, et al. Concomitant use of an infrared fractional laser with low-dose isotretinoin for the treatment of acne and acne scars. J Dermatolog Treat. doi: 10.3109/09546634.2013.768758. 2013 May 6. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]