

Abstract
AIM: To determine the accuracy of endoscopic polyp size measurements using disposable graduated biopsy forceps (DGBF).
METHODS: Gradations accurate to 1 mm were assessed with the wire of disposable graduated biopsy forceps. When a polyp was noted, endoscopists determined the width of the polyp; then, the graduated biopsy forceps was inserted and the largest diameter of the tumor was measured. After excision, during surgery or endoscopy, the polyp was measured using the vernier caliper.
RESULTS: One hundred and thirty-three colorectal polyps from 119 patients were studied. The mean diameter, by post-polypectomy measurement, was 0.92 ± 0.69 cm; 83 were < 1 cm, 36 were between 1 and 2 cm, and 14 were > 2 cm. The mean diameter, by visual estimation, was 1.15 ± 0.88 cm; compared to the actual size measured using vernier calipers, the difference was statistically significant. The mean diameter measured using the DGBF was 0.93 ± 0.68 cm; compared to the actual size measured using vernier calipers, this difference was not statistically significant. The ratio between the mean size estimated by visual estimation and the actual size was significantly different from that between the mean size estimated using the DGBF and the actual size (1.26 ± 0.30 vs 1.02 ± 0.11).
CONCLUSION: The accuracy of polyp size estimation was low by visual assessment; however, it improved when the DGBF was used.
Keywords: Disposable graduated biopsy forceps, Polyp size measurement, Colonoscopy, Accuracy
Core tip: In this study, we designed a disposable graduated biopsy forceps and used the forceps as “scale plate” to measure the polyp size. We enrolled 133 polyps from 119 patients and found that the accuracy of the visual estimation for a polyp size was low but could be improved if the disposable graduated biopsy forceps were used as a scale. Though some slight deviation still existed for estimation of polyps over 2 cm, the difference was not significant and did not affect treatment.
INTRODUCTION
The size of a tumor, detected at colonoscopy, is associated with the subsequent management of patients. If the size of a colon polyp is less than 3 cm, endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) could achieve complete resection with few complications[1,2]. If a colon polyp is greater than 3 cm, the bowel would need to be resected by endoscopic resection; these cases have been associated with a high risk of complications. However, for colon polyps less than 3 cm, the methods used and risks associated with endoscopic resection are different; that is, for polyps 2-3, 1-2 cm and those less than 1 cm[3,4]. Several clinical guidelines include the size and extent of the tumor as an important factor for deciding on the use of endoscopy for resection of colon polyps. Therefore, accurate measurement of colon polyps, during colonoscopy, is crucial for the appropriate management of patients with colon polyps[5-7]. However, there are no standard criteria for measuring the size of a colon polyp during colonoscopy.
Many endoscopists evaluate the size of a polyp based on their personal experience, which may be inconsistent with the actual size of the colon tumor. Eichenseer et al[8] compared the estimated size of 10 to 25-mm polyps, as determined during endoscopy, with the size determined by post-fixation histopathology of the polyps by 15 different endoscopists; they found that the mean size variation between the polyp size estimation at endoscopy and the size determined by histopathology of the polyps was 73.6% (range of mean size variation, 13%-127%). In addition, 62.6% (range, 0%-91%) included polyps that were clinically sized incorrectly; overestimation of the polyp size, during endoscopy, was more common than underestimation. Furthermore, some endoscopists inaccurately estimated the size of adenomas, and this led to inappropriate surveillance recommendations. In order to evaluate the differences between the size estimated by endoscopists and the actual size, as determined by histopathology, we developed a system using disposable graduated biopsy forceps to evaluate the size of colon polyps and compared this to both the estimation reported by endoscopists and the final size determined by histopathology.
MATERIALS AND METHODS
Ethics
The study was approved by the Ethics Committee of the Third Affiliated Hospital of Nanjing University of Traditional Chinese Medicine. All patients signed an informed consent form.
Study subjects
The graduated biopsy forceps was developed based on the traditional disposable biopsy forceps. At the beginning of the steel wire of the traditional disposable biopsy forceps, gradations were drawn every 1 mm along a 3-cm total length, using medical pigment. This was used as a scale plate for estimating the size of the tumors. From April to September 2013, patients with polyps were enrolled from the National Center of Colorectal Surgery, Nanjing University of Traditional Chinese Medicine. First, when the endoscopists discovered a polyp or tumor, they assessed the largest diameter of the tumor; then, they inserted a graduated biopsy forceps and measured the largest diameter of the tumor from the vertical view; lastly, the “gold standard” for the largest diameter of the tumor was accurately measured using a vernier caliper, after excising the tumor by surgery or endoscopy (Figure 1). A correct measurement was defined as a variation of less than 10% between the size evaluated and the actual size as measured using a vernier caliper. The accuracy rate was defined as the number of polyps accurately evaluated divided by the total number of polyps. Five endoscopists who had an experience of over 2000 cases of colonoscopy were involved in the study.
Figure 1.
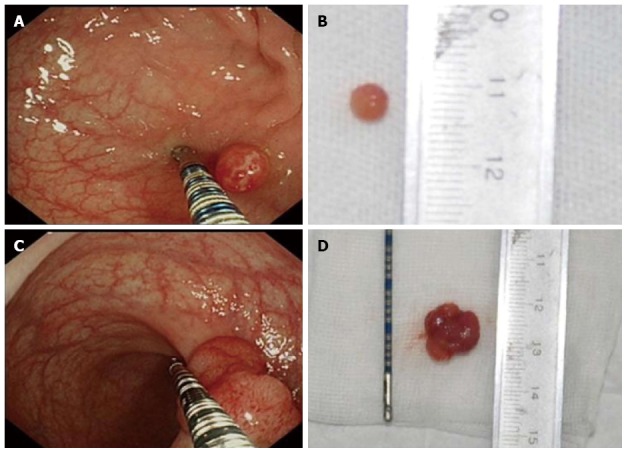
Comparison of measurements using the graduated biopsy forceps and the vernier caliper. A: 0.6 cm, measured using the graduated biopsy forceps; B: 0.6 cm, measured using the vernier caliper; C: 1.4 cm, measured using the graduated biopsy forceps; D: 1.4 cm, measured using the vernier caliper.
Statistical analysis
Data were analyzed using SPSS 17.0 software for Windows. The paired Student’s t-test was used to compare the ratio of the estimated size, by the endoscopists, to the actual size measured using the vernier caliper, with the ratio of the size measured using the graduated biopsy forceps to the actual size measured using the vernier caliper. Analysis of variance was used to compare the differences among the three groups. A P-value < 0.05 was considered statistically significant.
RESULTS
Basic clinical characteristics of the polyps
One hundred and thirty-three colon polyps from 119 patients (76 males and 43 females; average age, 58.29 ± 11.45 years; range, 28-82 years) were included. Among the polyps, 40 were rectal polyps, 43 sigmoid colon polyps, seven descending colon polyps, 12 transverse colon polyps, and 31 cecum or ascending colon polyps. Among the patients, two underwent laparoscopic colectomy, and all others had endoscopic mucosal resection. One hundred and seven were adenomas, while four were villous adenomas (of which, one was mucosal cancer, two were tubulovillous adenomas and one was a neuroendocrine tumor, a carcinoid tumor).
Influence of different tumor sizes on tumor size evaluation
The mean largest diameter of the resected polyps, measured using a vernier caliper, was 0.92 ± 0.69 cm (range, 0.1-4.0 cm); among the polyps, 83 were < 1 cm, 36 were between 1 and 2 cm and 14 were > 2 cm (Figure 2).
Figure 2.
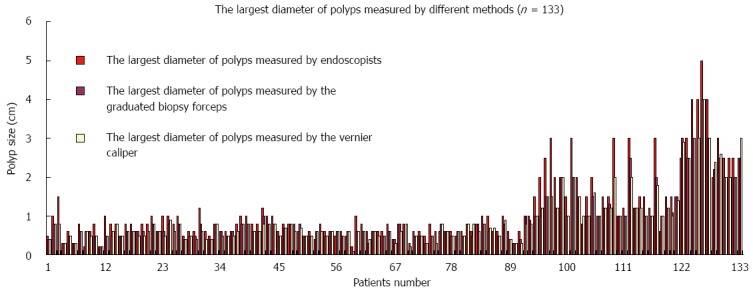
Comparison of the largest diameter measured using the three different methods.
For those polyps < 1 cm, the mean largest diameter evaluated by the endoscopists was 0.70 ± 0.23 cm (range, 0.2-1.5 cm); this was significantly different from the actual size measured using the vernier caliper (0.57 ± 0.17 cm) (P = 0.000). The mean largest diameter measured using the graduated biopsy forceps was 0.58 ± 0.17 cm; this was not significantly different from the actual size as measured using the vernier caliper (P = 0.096).
For polyps 1 to 2 cm, the mean largest diameter measured using the vernier caliper was 1.31 ± 0.34 cm, while the mean largest diameter by the endoscopists was 1.77 ± 0.71 cm (range, 0.6-3.0 cm); the difference was statistically significant (P = 0.000). The mean largest diameter measured using the graduated biopsy forceps was 1.323 ± 0.43 cm (range, 0.9-2.1 cm); this was not significantly different from the mean largest diameter measured using the vernier caliper (P = 0.688).
For polyps that were > 2 cm, the mean largest diameter measured using the vernier caliper was 2.70 ± 0.58 cm, while the mean largest diameter evaluated by the endoscopists was 3.12 ± 0.91 cm (range, 2.0-5.0 cm); this difference was statistically significant (P = 0.006), which implied that the endoscopists tend to overestimate the polyp size. The mean largest diameter measured using the graduated biopsy forceps was 2.64 ± 0.59 cm; this was not significantly different from the mean largest diameter measured using the vernier caliper (P = 0.223).
Influence of different tumor sizes on the accuracy of tumor size estimation
For 83 polyps less than 1 cm, only 22.2% (8/36) could be accurately estimated by the endoscopists, while 86.7% (72/83) could be accurately measured using the graduated biopsy forceps; this difference was statistically significant (P = 0.000).
For 36 polyps between 1 and 2 cm, only 11.1% (4/36) could be accurately estimated by the endoscopists, while 66.7% (24/36) were accurately measured using the graduated biopsy forceps; this difference was statistically significant (P = 0.009).
For polyps over 2 cm, none were accurately estimated by endoscopist assessment, while 57.1% were accurately measured using the graduated biopsy forceps.
DISCUSSION
The size of a colon polyp, assessed at colonoscopy, is crucial for determining patient management. Many clinical guidelines use the size and extent of the tumor as an important factor for determining whether to resect colon polyps using endoscopy[5-7]. However, accurate estimation of the size of a polyp, during colonoscopy, is not guaranteed. Currently, the size of a polyp is evaluated by endoscopists based on their personal experience; however, there is great variation among endoscopists with regard to the evaluated size and actual size of a colon polyp. In some studies, the oncological potential of a colon polyp has been related to its size and shape, indicating that the measurement of the colon polyp size was an important factor for determination of the risk associated with the colon polyp[9,10]. In this study, the difference between the actual size of the colon polyp and the size assessed by the endoscopists was significant. The actual size measured using the vernier caliper varied from the size estimated by the endoscopists, and this difference was statistically significant, especially for polyps greater than 1 cm. The reason for the variation in size estimation via endoscopy was the absence of a “scale plate”. All size estimations were done based on the endoscopists’ experience. Those endoscopists who were more experienced could accurately evaluate the size of the colon polyps; however, the size estimated by those endoscopists who were less experienced varied from the actual size. The accuracy of size estimation was improved by using the graduated biopsy forceps during endoscopy[11]. Morales et al[12] used an open biopsy forceps as a guide to measuring the colon polyp size during colonoscopy; however, there were significant differences between the endoscopic estimates and the post-polypectomy measurements for three-quarters of the polyps. Gopalswamy et al[13] compared the accuracy of a linear probe, visual estimation and forceps for estimating polyp size during colonoscopy; they found that the measurement of the polyp size using a linear probe had the best agreement with the actual polyp size, followed closely by visual estimation. The open biopsy forceps method was the least accurate. However, the linear probe requires special software to estimate size, which adds to the examination time and cost of the procedure. In recent years, the computed tomography (CT) colonoscopy has been used to estimate the size of colon polyps with a high degree of accuracy. However, the patients required bowel preparation before a CT colonoscopy and the procedure was very costly[14-16].
To estimate the size of colon polyps, we developed a graduated biopsy forceps based on the traditional disposable biopsy forceps. Gradations were drawn every 1 mm along the 3-cm total length using medical pigment. The accuracy of estimating the size of the colon polyps increased when using the graduated biopsy forceps. In this study, the mean estimated size, by the endoscopists, was 1.15 cm; this was different from the actual size measured using the vernier caliper (0.92 cm) and the difference was statistically significant. However, the mean size measured using the graduated biopsy forceps was 1.02 cm, which was statistically similar to the actual size measured using the vernier caliper (0.93 cm). Therefore, the size measured using the graduated biopsy forceps was consistent with the actual size as measured using the vernier caliper. The ratio of the size estimated by the endoscopists to the actual size measured using the vernier caliper was 1.26, while the ratio of the size measured using the graduated biopsy forceps to the actual size measured using the vernier caliper was 1.02; the difference between these two ratios was statistically significant (P = 0.000). These findings show that the graduated biopsy forceps could improve the accuracy of size estimation of colon polyps.
Different polyp sizes affected the accuracy of size estimation. The bigger the tumor size was, the less accurately the tumor was estimated. From our study, the polyp size by endoscopist tends to be overestimated, and the polyp size tends to be more accurately estimated when we used the graduated biopsy forceps. For polyps less than 1 cm, 86.7% could be accurately measured. For polyps between 1 and 2 cm, only 11.1% could be accurately estimated by the endoscopists, while 66.7% were accurately measured using the graduated biopsy forceps. These findings indicate that using the graduated biopsy forceps improved the accuracy of size estimation and decreased the variation of measurements.
However, this type of graduated biopsy forceps could only measure polyps along the longitudinal axis of the bowel; polyps that surrounded the enteric cavity could not be directly measured with the graduated biopsy forceps. In such cases, estimations by the endoscopists were needed; they identified polyps that surrounded the enteric cavity. In this study, for 14 polyps that were > 2 cm, variation existed in 42.9% (6/14) of the polyps, especially for the lateral spread of the polyps. The size measurement could not be determined in one view, and in such cases the assessment might be different from the actual size.
In conclusion, the estimation of colon polyp size during endoscopy based on endoscopists’ experience had lower accuracy; use of the graduated biopsy forceps during endoscopy improved the accuracy of size estimation. Although there were variations in laterally spreading colon polyps that were > 2 cm, the variations were significantly decreased and they did not affect treatment and follow-up.
ACKNOWLEDGMENTS
Many thanks to Mrs. Ping Liu, Mrs. Xiu Zhang, and Mrs. Hui-Ping Lin for their assistance with the acquisition of data, and Dr. Hang Yao, Dr. Kunlan Wu, and Dr. Jin-Hao Zhang for their assistance with data analysis and interpretation.
COMMENTS
Background
The size of a tumor, detected at colonoscopy, is associated with the subsequent management of patients. However, there are no standard criteria for measuring the size of a colon polyp during colonoscopy. Several studies showed that some endoscopists inaccurately estimated the size of adenomas, and this led to inappropriate surveillance recommendations. Therefore, in order to evaluate the differences between the size estimated by endoscopists and the actual size, as determined by histopathology, the authors developed a system using disposable graduated biopsy forceps (DGBF) to evaluate the size of colon polyps and compared this to both the estimation reported by endoscopists and the final size determined by histopathology.
Research frontiers
In order to evaluate the differences between the size estimated by endoscopists and the actual size, as determined by histopathology, authors developed a system using disposable graduated biopsy forceps to evaluate the size of colon polyps and compared this to both the estimation reported by endoscopists and the final size determined by histopathology.
Innovations and breakthroughs
This paper showed an easy method to measure the size of colon polyps. The study showed that the accuracy of polyp size estimation was low by visual assessment; however, it improved when the DGBF was used. Although some slight deviations still existed for estimations of polyps over 2 cm, the difference was not significant.
Applications
The DGBF is a very easy method to accurately measure the size of polyps during endoscopy. It is a very useful method and does not increase the medical cost.
Peer review
The manuscript is novel and potentially helpful to the practicing gastroenterologist. It is a very interesting paper and presents an original view of the problem.
Footnotes
Supported by National Nature Science Foundation of China, No. 3097383 and No. 81273944; and grants from The Nanjing Medical Technology Development Project, No. NJYX201203.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: May 26, 2014
First decision: June 18, 2014
Article in press: July 25, 2014
P- Reviewer: Figueiredo PN, Nowicki MJ S- Editor: Gou SX L- Editor: Wang TQ E- Editor: Ma S
References
- 1.Saito Y, Fujii T, Kondo H, Mukai H, Yokota T, Kozu T, Saito D. Endoscopic treatment for laterally spreading tumors in the colon. Endoscopy. 2001;33:682–686. doi: 10.1055/s-2001-16213. [DOI] [PubMed] [Google Scholar]
- 2.Wang HM, Huang CM, Zheng CH, Li P, Xie JW, Wang JB, Lin JX, Lu J. Tumor size as a prognostic factor in patients with advanced gastric cancer in the lower third of the stomach. World J Gastroenterol. 2012;18:5470–5475. doi: 10.3748/wjg.v18.i38.5470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tseng MY, Lin JC, Huang TY, Shih YL, Chu HC, Chang WK, Hsieh TY, Chen PJ. Endoscopic submucosal dissection for early colorectal neoplasms: clinical experience in a tertiary medical center in taiwan. Gastroenterol Res Pract. 2013;2013:891565. doi: 10.1155/2013/891565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Toyonaga T, Man-i M, Chinzei R, Takada N, Iwata Y, Morita Y, Sanuki T, Yoshida M, Fujita T, Kutsumi H, et al. Endoscopic treatment for early stage colorectal tumors: the comparison between EMR with small incision, simplified ESD, and ESD using the standard flush knife and the ball tipped flush knife. Acta Chir Iugosl. 2010;57:41–46. doi: 10.2298/aci1003041t. [DOI] [PubMed] [Google Scholar]
- 5.Horiuchi Y, Chino A, Matsuo Y, Kishihara T, Uragami N, Fujimoto Y, Ueno M, Tamegai Y, Hoshino E, Igarashi M. Diagnosis of laterally spreading tumors (LST) in the rectum and selection of treatment: characteristics of each of the subclassifications of LST in the rectum. Dig Endosc. 2013;25:608–614. doi: 10.1111/den.12040. [DOI] [PubMed] [Google Scholar]
- 6.Tanaka S, Terasaki M, Hayashi N, Oka S, Chayama K. Warning for unprincipled colorectal endoscopic submucosal dissection: accurate diagnosis and reasonable treatment strategy. Dig Endosc. 2013;25:107–116. doi: 10.1111/den.12016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Winawer SJ, Zauber AG, Fletcher RH, Stillman JS, O’brien MJ, Levin B, Smith RA, Lieberman DA, Burt RW, Levin TR, et al. Guidelines for colonoscopy surveillance after polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. CA Cancer J Clin. 2006;56:143–59; quiz 184-5. doi: 10.3322/canjclin.56.3.143. [DOI] [PubMed] [Google Scholar]
- 8.Eichenseer PJ, Dhanekula R, Jakate S, Mobarhan S, Melson JE. Endoscopic mis-sizing of polyps changes colorectal cancer surveillance recommendations. Dis Colon Rectum. 2013;56:315–321. doi: 10.1097/DCR.0b013e31826dd138. [DOI] [PubMed] [Google Scholar]
- 9.Reinhart K, Bannert C, Dunkler D, Salzl P, Trauner M, Renner F, Knoflach P, Ferlitsch A, Weiss W, Ferlitsch M. Prevalence of flat lesions in a large screening population and their role in colonoscopy quality improvement. Endoscopy. 2013;45:350–356. doi: 10.1055/s-0032-1326348. [DOI] [PubMed] [Google Scholar]
- 10.Einspahr JG, Alberts DS, Gapstur SM, Bostick RM, Emerson SS, Gerner EW. Surrogate end-point biomarkers as measures of colon cancer risk and their use in cancer chemoprevention trials. Cancer Epidemiol Biomarkers Prev. 1997;6:37–48. [PubMed] [Google Scholar]
- 11.Turner JK, Wright M, Morgan M, Williams GT, Dolwani S. A prospective study of the accuracy and concordance between in-situ and postfixation measurements of colorectal polyp size and their potential impact upon surveillance. Eur J Gastroenterol Hepatol. 2013;25:562–567. doi: 10.1097/MEG.0b013e32835d1f2d. [DOI] [PubMed] [Google Scholar]
- 12.Morales TG, Sampliner RE, Garewal HS, Fennerty MB, Aickin M. The difference in colon polyp size before and after removal. Gastrointest Endosc. 1996;43:25–28. doi: 10.1016/s0016-5107(96)70255-9. [DOI] [PubMed] [Google Scholar]
- 13.Gopalswamy N, Shenoy VN, Choudhry U, Markert RJ, Peace N, Bhutani MS, Barde CJ. Is in vivo measurement of size of polyps during colonoscopy accurate? Gastrointest Endosc. 1997;46:497–502. doi: 10.1016/s0016-5107(97)70003-8. [DOI] [PubMed] [Google Scholar]
- 14.Barancin C, Pickhardt PJ, Kim DH, Spier B, Lindstrom M, Reichelderfer M, Gopal D, Pfau P. Prospective blinded comparison of polyp size on computed tomography colonography and endoscopic colonoscopy. Clin Gastroenterol Hepatol. 2011;9:443–445. doi: 10.1016/j.cgh.2011.01.020. [DOI] [PubMed] [Google Scholar]
- 15.Summers RM. Polyp size measurement at CT colonography: what do we know and what do we need to know? Radiology. 2010;255:707–720. doi: 10.1148/radiol.10090877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yeshwant SC, Summers RM, Yao J, Brickman DS, Choi JR, Pickhardt PJ. Polyps: linear and volumetric measurement at CT colonography. Radiology. 2006;241:802–811. doi: 10.1148/radiol.2413051534. [DOI] [PubMed] [Google Scholar]