

Abstract
Background:
Fall from height is a common cause of morbidity and mortality in suburban population in India. These cases are either domestic or workplace injuries with different causative factors. We analyzed different aspects of these falls to identify their risk factors.
Materials and Methods:
We conducted prospective and retrospective epidemiological study to identify various causative, contributory factors, and resultant injuries in cases of fall from height. The study group comprised of semiurban population and involved both domestic and workplace injuries presenting to a tertiary care hospital.
Results:
There were 208 cases of workplace (112) and domestic (96) fall from height. In domestic cases absence of parapet on roof was the commonest cause, most of falls occurred during summer and rainy season. Alcohol consumption prior to fall was commonest associated factor in adult males. Children mostly fell while playing on roof and climbing trees. Among workplace cases, civil construction site injuries were commonest and absence of any protective gear and long working and evening hours were commonest associated factors. Mean injury severity score was 10.86 in domestic cases and 14.87 in workplace cases. There were 17 mortalities with head injury being commonest associated cause. Only difference in incidence of alcohol consumption and permanent disability was statistically significant between workplace and domestic falls.
Conclusion:
Different factors are responsible for domestic and workplace cases of fall from height. Most of these cases are potentially preventable.
Keywords: Fall, free fall, injuries, ladder injuries, unintentional fall
INTRODUCTION
Unintentional fall from height resulting in various orthopedic, neurosurgical, and surgical injuries is a common presentation in India. Most of such cases are accidental and preventable. Understanding various factors responsible for such fall from height and subsequent preventive measures can help in reducing associated morbidity, mortality, and resultant burden on scarce healthcare facilities. Factors responsible for such falls differ from urban to rural areas and in developed and developing world due to different socioeconomic conditions. There are few reported studies on different factors responsible for such falls, but most of them have come from developed countries or urban centers.[1,2,3,4,5,6,7] We conducted a retrospective and prospective epidemiological study analyzing the causative, contributory factors and injuries sustained in such cases presenting to a tertiary care hospital catering to suburban and rural population.
MATERIALS AND METHODS
We collected and analyzed data of patients presenting to emergency of a tertiary care center situated in a semiurban area, with primary history of accidental domestic and work site fall from height requiring hospitalization between January 2008 and December 2010. Ethical clearance from hospital review board was taken for the study. Medical records of patients prior to March 2009, when the study was commenced were accessed from medical records department and cases in which circumstances of fall and height of fall were not recorded, were excluded from the study. Any case of non-accidental fall was excluded. There were 208 such cases and we analyzed different causative, contributory factors and injuries sustained due to such falls.
The cases were divided into domestic and work site accidents. Age, gender, injuries sustained, and duration of hospital stay of each patient was documented and injury severity score (ISS) calculated. Any resultant permanent disability was subsequently recorded.
Different causative and contributory factors recorded included height of fall, cause of fall, time of day, season, history of alcohol intake/any other intoxicating substance consumption, or any other significant associated factor. In case of work place falls, number of working hours put in before fall and worksite safety measures being used at time of fall were also recorded.
Statistical analysis
Chi-square test and Student's t-test were used for statistical analysis. P < 0.05 was taken as statistically significant.
RESULTS
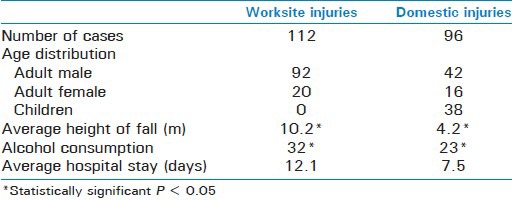
Out of 208 such patients admitted in Neurosurgery, Surgery, or Orthopedic Department; there were 126 males and 44 females including 38 children. There were 112 cases of workplace and 96 cases of domestic fall [Table 1].
Table 1.
Population characteristics associated with workplace and domestic fall
One hundred and fourteen (54.8%) cases had head injury, 87 (41.8%) cases had fracture of extremity, and 73 (35%) cases had chest/abdominal trauma. One hundred and forty-six (70.1%) cases required combined care of more than one department. Eighty-seven (41.8%) cases required surgical intervention for management of injuries. Fifty-four (25.9%) cases required intensive care treatment for an average of 7 days. In all there were 17 mortalities and 35 (16.8%) cases had permanent disability.
Work place cases
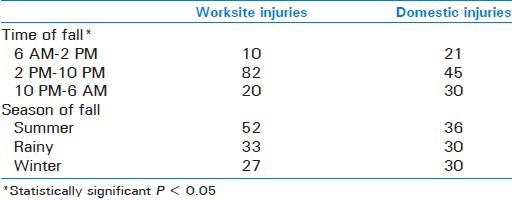
One hundred and two cases (91%) occurred from 2 PM to 6 AM after an average of 7.2 h of work (range 1-11 h). Average height of fall was 10.2 m (range 3-30 m). Seventy-eight (69.6%) cases had fall at construction site, while other causes included fall from electricity pole (n = 16, 14.2%) and ladders (n = 12, 10.7%). Majority of such patients (62%) were not using proper protective measures at time of fall [Figures 1 and 2]. Most of such falls occurred in summer (46.4%) and least in winter season (24.1%) [Table 2].
Figure 1.
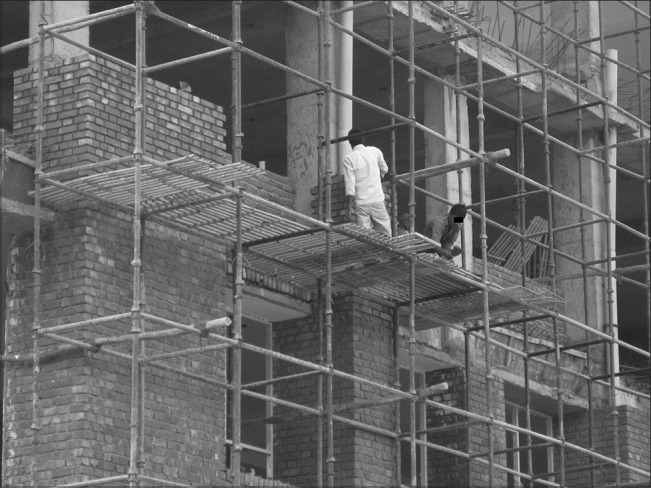
Construction site workers without protective gear or nets
Figure 2.

Construction site workers without protective gear or nets
Table 2.
Diurnal and seasonal variation in incidence of fall from height
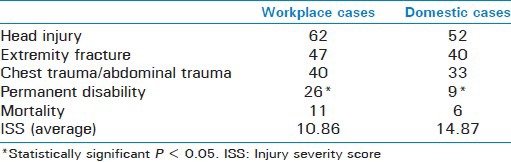
Twenty-six patients had permanent disability; in 20 patients it was secondary to spinal fracture, while in six cases it was secondary to head injury. There were 11 mortalities. Mortality was secondary to head injury in all cases, while three cases also had associated pelvic fracture. Average ISS score was 10.86 ± 16.98 [Table 3].
Table 3.
Distribution of injuries sustained
Domestic cases
Most common cause was absence of parapet on roof of houses (n = 69, 71.8%). Average height of fall was 4.2 m (range 3.6-11 m). Sixty-six cases (68.7%) occurred during summer and rainy season. 51.7% (n = 30) cases of fall involving adult population occurred in night, while in case of children all cases occurred during daytime [Table 2].
All the cases involving children were domestic injuries and most common cause was fall from roof without a parapet (n = 21, 55.2%) while playing besides fall from tree [Figure 3].
Figure 3.
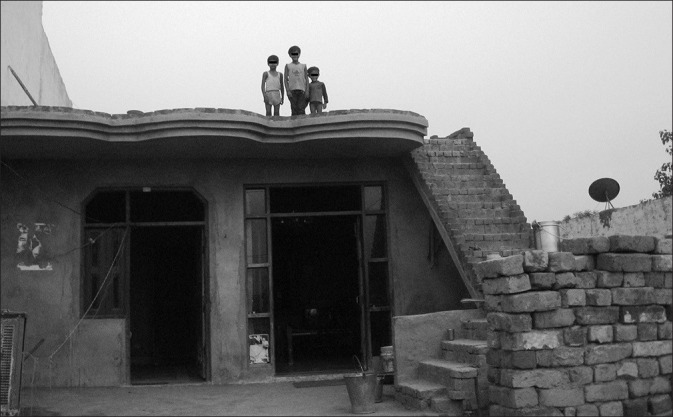
House without a parapet
Twelve male patients (28.5%) had fall while trying to hook an electrical wire to overhead high voltage wires to draw electricity illegally. All such cases also had electrical burns [Figure 4].
Figure 4.
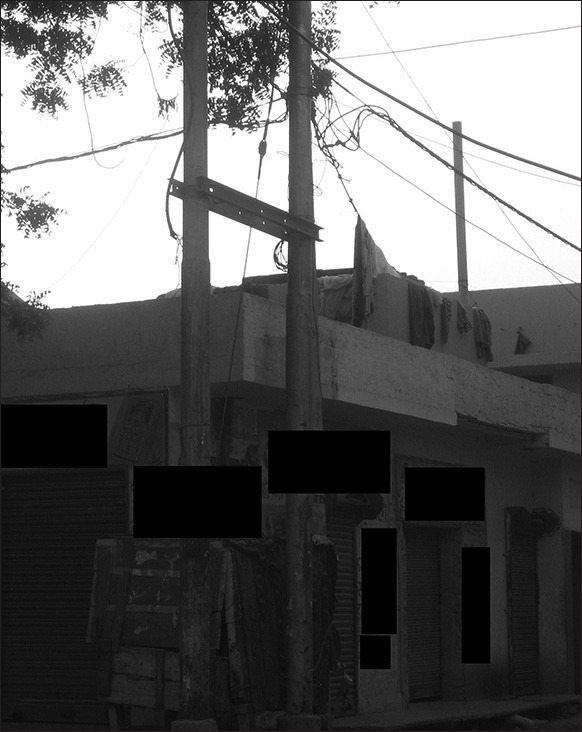
House without parapet with cloths hanging on illegal electric connection wire
There were six mortalities; in four cases it was secondary to head injury, while in two cases it was secondary to pelvic fracture. Out of six mortalities four were adults less than 60 years, while two were more than 60 years of age. Nine patients had permanent disability all due to spinal injuries. Average ISS score was 14.87 ± 20.48 [Table 3].
There was history of alcohol consumption in 55 (41%) adult males (32 workplace and 23 domestic cases) within 6 h prior to fall, the difference being statistically significant. There was no history of consumption of any other intoxicating material.
Also, the difference in incidence of permanent disability and time of fall was statistically significant between the two groups.
DISCUSSION
National Crime Records Bureau, Ministry of Home Affairs, Government of India in a published report in 2010 has mentioned that fall from height contributed 2.6% of all fatalities due to natural and unnatural causes.[8] Fall from height is a common cause of polytrauma in urban population.[6,7] But in suburban population, the factors responsible for such fall and resultant injuries are different. Most of such falls are easily preventable with simple measures. Study of such falls can help in determination of various factors responsible for them and help in formulation of specific corrective measures.
This study was conducted at a tertiary care medical college located in a suburban area catering to both urban and rural population. 64.4% of all cases were adult males with 73% belonging to 18-60 age groups, which represent the active productive population.
We divided these fall from height into workplace and domestic cases because of difference in causative factors, height of fall and extent of injuries sustained in both cases.
In our study, maximum number of cases belonged to workplace injuries (n = 112, 54%), which is contrary to similar study by Gulati et al.,[6] where 90% cases were domestic injuries and Kent and Pearce[9] who reported 57.4% cases of domestic fall. It was so because their study was done in predominantly urban population. But, our study group belonged to suburban population which is witnessing rapid urbanization and construction of high-rise commercial and residential complexes without proper deployment of safety measures. Most of these complexes have come up on land in and around villages. Such villages though surrounded by these high-rise buildings still lag behind in urbanization and have rural infrastructure with poor socioeconomic conditions.
On analysis of domestic cases, we observed certain age-specific variations. Children, in 55.2% cases fell from rooftops while flying kites, which is a common sport in southeast Asian and Middle East countries. An important contributory factor was absence of parapet on roof tops in rural areas. Another cause was fall from trees while trying to pluck fruits. Both of these and other outdoor activities are common in summer and rainy season which explains majority of falls during these seasons. Similar observations have been reported in other studies also.[1,2,3,5]
In adults, most falls (51.7%) occurred in night especially in summers as people sleep on roof tops to avoid hot interiors.[3,5,6] 52.3% of domestic cases involving adult males had history of alcohol consumption within 6 h prior to fall. Alcohol causes impairment of judgment and also produces an urge to urinate. In elderly male, urge to urinate in night when they are not fully awake, led to such falls. Absence of parapet was a major contributory factor in such falls.[3,5]
A peculiar cause of fall, seen in 12 male patients was electrocution while trying to hook electricity wire from their roof tops to overhead high voltage electricity transmission lines, in order to draw power illegally. This is a practice in rural and suburban areas to avoid paying electricity charges. Usually when electrocuted, these patients were thrown off by high voltage current leading to fall from roof.
Head injury, extremity fracture, and spinal trauma with or without neurological deficit, chest trauma were most common injuries; while abdominal trauma was relatively less common in domestic injuries.[1,3,9]
From analysis of these cases we concluded that construction of a parapet alone can significantly prevent such domestic cases in both adult and pediatric population.
While analyzing data of worksite injuries, we found that 70% such cases were due to fall at civil construction sites. Due to rapid growth of population there is a strong demand for new housing units leading to extensive construction in suburban areas.
Majority of these cases had fall from more than three floors. Agalar et al.,[10] and Auñón-Martín et al.,[11] concluded that height of fall and age was significant factors in determining the severity of trauma. However, Goodacre et al.[12] opined that height of fall is a poor predictor of major injury. Lapostolle et al.,[13] reported a correlation between the height of fall and mortality. Chen-Chi et al.,[14] and Auñón-Martín et al.,[11] reported no statistically significant correlation between these variables. In our study also there was significant difference in height of fall between the two groups, but there was no significant difference in ISS, injuries sustained, and mortality; but workplace injuries had significantly higher incidence of permanent disability.
Most of these patients were not trained in work site safety guidelines. Lack of protective gear, working in evening and night hours especially during summers in artificial lighting, and unregulated long working hours were major contributory factors leading to such falls [Figure 5]. Due to hot and humid conditions during day throughout the year except in winters and restriction on trucks carrying construction material during day to prevent congestion on roads, most of construction work is undertaken in evening and night.
Figure 5.
Construction site workers without protective gear working in night
Fourteen percent cases of worksite injury had fall from electricity poles while working on them, while 11% had fall from ladder. Different studies have identified fall from ladder as major cause of injury with ladder instability as major cause of fall. Injuries are usually less severe involving mainly the extremities.[15,16]
Head injury, extremity fractures, chest, abdominal trauma, and spinal trauma were common presentations. Different studies have found that impacting body part as an independent prognostic factor in fall from height,[11,12] but we found that it was not possible to reliably obtain information regarding the same from either the patient or informants in most of the cases.
Comparing the data between the two groups we found that incidence of fall after alcohol consumption and permanent disability was significantly more in workplace cases. Also, there was statistically significant difference in timing of fall and height of fall between the two groups.
Sensitizing the workforce and contractors regarding various safety measures may be able to decrease the number of accidents and their severity at construction sites. Also, local administration should be proactive in enforcement of safety guidelines, which is easier as most of construction sites are situated in clusters in suburban areas.
This study reflects the majority of factors responsible for fall from height in both domestic and workplace cases that can be easily prevented. Efforts made for prevention of such cases may be able to significantly impact the number of such cases.
Examples of such preventive initiatives include the Swiss Advisory Board for Accident Prevention which provides information about accident prevention and protection measures to architects, property managements, communities, and individuals[1] and Health and Safety Executive in United Kingdom which also educates and publishes literature in form of booklets and leaflets for various safety measures and prevention techniques to prevent fall-related injuries at workplace.
The New York City Department of Health started a program “Children Can’t Fly” in the early 1970s. In this program, all hospital emergency rooms and police reported all fall-related childhood deaths and injuries to a central unit and was followed by a nurse visit to home to examine and document other characteristics. Awareness among parents was increased by individual counseling, radio talks, television, and other channels. A community education program followed soon. Windows guard was provided free of cost to families with young children living in high risk areas.[4] Suitable legislation followed thereafter to ensure all high raise apartments installed window guards.
Community education programs aimed at preventive measures for falls like making of parapet, prevention of illegal drawing of power from overhead wires, enforcement of building rules, educating workers about safe construction practices, distributing leaflets describing various safe practices and use of protective gear, and strict no alcohol policy at work, may prevent such injuries.
This study had certain limitations as approximate height of fall and other contributory factors were subjectively assessed based on facts as told by patient's attendants. Also, only cases which required hospitalization were recorded and there may have been mortalities which were not brought to the hospital. Further study is required to determine whether the preventive measures based on observations of this study will lead to decrease in incidence of such falls or not.
In conclusion, there are different factors responsible for domestic and workplace falls in suburban and rural population. Construction of parapet on roof tops at homes and good safety measures at workplace can potentially lead to decrease in incidence of such cases.
Footnotes
Source of Support: Nil
Conflict of Interest: No.
REFERENCES
- 1.Mayer L, Meuli M, Lips U, Frey B. The silent epidemic of falls from buildings: Analysis of risk factors. Pediatr Surg Int. 2006;22:743–8. doi: 10.1007/s00383-006-1731-7. [DOI] [PubMed] [Google Scholar]
- 2.Lallier M, Bouchard S, St-Vil D, Dupont J, Tucci M. Falls from height among children: A retrospective review. J Paediatr Surg. 1999;34:1060–3. doi: 10.1016/s0022-3468(99)90564-x. [DOI] [PubMed] [Google Scholar]
- 3.Yagmur Y, Guloglu C, Aldemir M, Orak M. Falls from flat – roofed houses: A surgical experinace of 1643 patients. Injury. 2004;35:425–8. doi: 10.1016/S0020-1383(03)00198-0. [DOI] [PubMed] [Google Scholar]
- 4.Spiegel CN, Lindaman FC. Children can’ t fly: A programme to prevent childhood morbidity and mortality from window falls. American Journal of Public Health. 1977;67:1143–7. doi: 10.2105/ajph.67.12.1143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Goren S, Subasi M, Týrasci Y, Gurkan F. Fatal falls from heights in and around Diyarbakir, Turkey. Forensic Sci Int. 2003;137:37–40. doi: 10.1016/s0379-0738(03)00285-8. [DOI] [PubMed] [Google Scholar]
- 6.Gulati D, Aggarwal AN, Kumar S, Agarwal A. Skeletal injuries following unintentional fall from height. Ulus Travma Acil Cerrahi Derg. 2012;18:141–6. doi: 10.5505/tjtes.2012.12058. [DOI] [PubMed] [Google Scholar]
- 7.Kohli A, Banerjee KK. Pattern of injuries in fatal falls from buildings. Med Sci Law. 2006;46:335–41. doi: 10.1258/rsmmsl.46.4.335. [DOI] [PubMed] [Google Scholar]
- 8.Accidental deaths and suicide in India. National Crime record Bureau, Ministry of Home Affairs. 2010 [Google Scholar]
- 9.Kent A, Pearce A. Review of morbidity and mortality associated with falls from heights among patients presenting to a major trauma centre. Emerg Med Australas. 2006;18:23–30. doi: 10.1111/j.1742-6723.2006.00800.x. [DOI] [PubMed] [Google Scholar]
- 10.Agalar F, Cakmakci M, Sayek I. Factors effecting mortality in urban vertical free falls: Evaluation of 180 cases. Int Surg. 1999;84:271–4. [PubMed] [Google Scholar]
- 11.Auñón-Martín I, Doussoux PC, Baltasar JL, Polentinos-Castro E, Mazzini JP, Erasun CR. Correlation between pattern and mechanism of injury of free fall. Strategies Trauma Limb Reconstr. 2012;7:141–5. doi: 10.1007/s11751-012-0142-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Goodacre S, Than M, Goyder EC, Joseph AP. Can the distance fallen predict serious injury after a fall from a height? J Trauma. 1999;46:1055–8. doi: 10.1097/00005373-199906000-00014. [DOI] [PubMed] [Google Scholar]
- 13.Lapostolle F, Gere C, Borron SW, Pétrovic T, Dallemagne F, Beruben A, et al. Prognostic factors in victims of falls from height. Crit Care Med. 2005;33:1239–42. doi: 10.1097/01.ccm.0000164564.11989.c3. [DOI] [PubMed] [Google Scholar]
- 14.Liu CC, Wang CY, Shih HC, Wen YS, Wu JJ, Huang CI, et al. Prognostic factors for mortality following falls from a height. Injury. 2009;40:595–7. doi: 10.1016/j.injury.2008.11.014. [DOI] [PubMed] [Google Scholar]
- 15.Partridge RA, Virk AS, Antosia RE. Causes and patterns of injury from ladder falls. Acad Emerg Med. 1998;5:31–4. doi: 10.1111/j.1553-2712.1998.tb02571.x. [DOI] [PubMed] [Google Scholar]
- 16.Tsipouras S, Hendrie JM, Silvapulle MJ. Ladders: Accidents waiting to happen. Med J Aust. 2001;174:516–9. doi: 10.5694/j.1326-5377.2001.tb143403.x. [DOI] [PubMed] [Google Scholar]