

Abstract
Context:
Trauma in South Asia is an increasingly significant problem, particularly in light of increasing motorization. Societal changes are resulting in alterations in the epidemiology of trauma.
Aims:
To assess various epidemiological parameters that influence causation of injury in the patients admitted in a major trauma center in Northern India.
Settings and Design:
Prospective, cross-sectional, Hospital based study from August 2008 to July 2009.
Materials and Methods:
A prospective study of 748 patients chosen by random assortment was carried out over a period of 1 year (August 2008 to July 2009) and following parameters were noted: Age group, sex, mode of trauma, type of injury, place where the trauma occurred and factors leading to injury. The length of stay of patients, Kampala trauma score (KTS) and mortality depending on the arrival time in emergency department was also noted.
Statistical Analysis:
Data analysis was performed using SPSS Version 16.
Results:
Overall trauma was most common in the age group 15-30 years (Mean age: 29.43 ± 16.87 years), with male constituting 85.29% of the total patients. It was observed that road side injuries were the most frequent (66.71%) site of injuries, whereas household injuries (23.66%), farm site (6.28%), work place (1.60) were the next most common modes of trauma. Mean time of presentation of injured patient was 2.53 ± 4.92 days. About 48.13% patients were admitted after more than 24 h after the injury. Two wheelers (32.09) were found to be the most common mode of injury. Maximum injuries (65.31%) occurred in the rural setting. The overall length of hospital stay ranged from 2 days to 178 days (median15.6 days). Mortality is more in patients who arrive in night (between 9 pm and 5 pm).
Conclusions:
We conclude that the majority of injuries are preventable and the epidemiological trends differ from that of developed countries. Therefore, preventive strategies should be made on the basis of these epidemiological trends.
Keywords: Epidemiology, fall, injury, road traffic accidents, trauma
INTRODUCTION
South East Asia region is passing through a major epidemiological transition and technological revolution during the past two decades. Countries are passing through significant urbanization, motorization, industrialization and changes in the socio-economic values of societies. While this ongoing epidemiological, demographic, and socio-economic transition has seen a decline of some communicable diseases, it has also seen the emergence of injuries as a leading health-problem.[1] Injuries on roads, at home and in the work place have increased due to lack of safety related policies and programs. India is no exception to this change. In India, systematic and scientific efforts in injury prevention and control are yet to begin.[2]
India leads world in road deaths. ThirteenIndians die every hour due to an accident. 1,14,590 people died in road traffic accidents in India (2007), highest in the world. Fatalities due to road traffic injuries in India are projected to increase by 150% by the year 2020.[3] The nature of injuries sustained due to trauma is well understood, however, the causality of injury is less well understood. There are few studies from developing countries discussing the epidemiology of trauma.[2] Our study aims to assess the various epidemiological parameters that influence the cause of injury in the patients admitted in a major trauma center in Northern India.
MATERIALS AND METHODS
This was a prospective study conducted at the trauma centre attached to a King George Medical University in Northern India over a 12 month period. A total of 748 patients with trauma admitted between August 2008 to July 2009 were chosen by random assortment. Intentional injuries were excluded from our study.
A detailed history taking and examination were done and all patients were assessed with regards to their age, sex, mode of trauma/injury, type of injury, site of trauma and place of trauma. Mode of trauma was divided into blunt and penetrating. Factors causing the injury such as weather conditions, road character, area type, use of seat belt and helmet etc., were also noted. The types of injury were divided into subgroups: Head injuries, upper limb fracture, chest fracture, pelvis fracture, hip fracture, lower limb fracture, injury involving the half body, injury involving whole body and abdominal injuries.
Ethical clearance was obtained from the Institutional Ethical Committee for conducting the study and consent of each patient was obtained for inclusion in the study.
Statistical analysis
Data was analyzed using SPSS version 16. Data was analyzed in terms of descriptive tables.
RESULTS
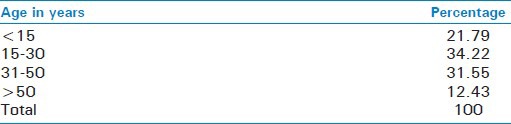
The mean age of presentation was 29.43 ± 16.87 years. Maximum numbers of patient admitted were among the age group of 15-30 years (34.22%) [Table 1].
Table 1.
Distribution of cases by age (n=748)
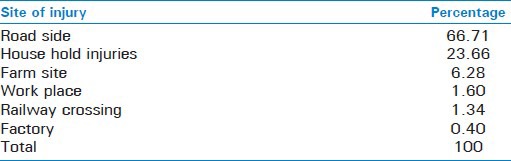
85.29% of the patients were male, as compared to 14.7% of females. The mean time of presentation of the injured patient reporting to the trauma centre was 2.53 ± 4.92 days. Among the injured patients about 50% were admitted to the hospital after 24 h of injury [Table 2]. Roadside injuries (66.71%) were found to be the leading cause of admissions in our study followed by household injuries (23.66%) [Table 3].
Table 2.
Time elapsed between admission and injury (in h)
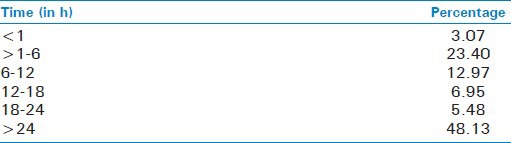
Table 3.
Distribution of cases by the site of injury (n=748)
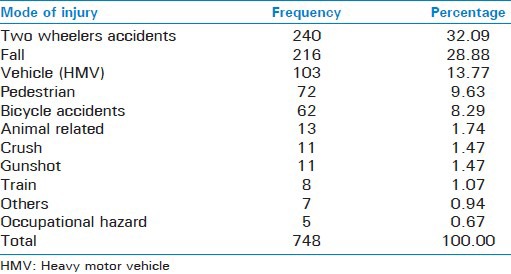
Two wheelers were the most common mode of injury contributing to a total of 32.09% injuries which together with a fall from height contributed to more than 50% of all admissions in the trauma centre [Table 4].
Table 4.
Percentage distribution according to mode of injury
Blunt injuries (94.92% were much more common than penetrating injuries (5.08%). The admissions due to accident in rural areas (65.31%) were almost twice in relation to those in urban areas (34.69%).
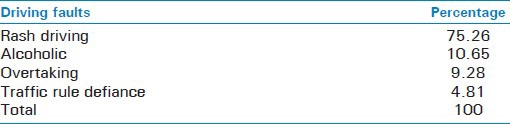
Poor visibility of vehicle or roads contributed to the injuries in 29.94% of cases in which pedestrians were most commonly involved. Rash driving was the most common nature of driving fault accounting for 75% of cases in this group. Driving under the influence of alcohol, over speeding and overtaking was the major behavioral factors. 10.65% were driving under the influence of alcohol [Table 5].
Table 5.
Nature of driving faults
Driving a two wheeler without a helmet was a major contributor to injuries (71.77%). Among the motor vehicle injuries it was observed that 79% of the drivers were not wearing seat belts at the time of accident and only 20.24% cases wearing seat belts were injured. Approximately 1/3rd of the drivers of different vehicle were driving without a driving license (33.47%).
Among the poly trauma patients admitted in our series torso injuries (80.49%) i.e. (spinal cord injury combined with chest, abdominal and pelvic injury were the maximum followed by limb injury and head injury. Head injury was the most common single injury amongst all patients admitted in our series (57.27%).
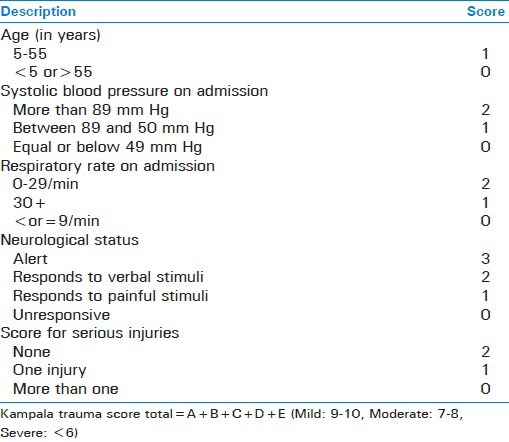
As per the Kampala Trauma Score II (KTS II) [Table 6], the majority of patients sustained moderate injuries (KTS II = 7-8) in 582 (77.8%). Severe injuries (KTS II ≤ 6) and mild injuries (KTS II = 9-10) were recorded in 104 (13.9%) and 72 (9.62%) patients respectively. The mortality rates in patients with mild, moderate and severe injuries were 8.3%(6 deaths). 3.7% (22 deaths) and 30.7% (32 deaths). According to multivariate logistic regression analysis, these differences were statistically significant (P < 0.001).
Table 6.
Kampala trauma score II description
The overall length of hospital stay ranged from 2 to 178 days with the mean of 16.5 ± 10.5 days. The median was 15.6 days According to multivariate logistic regression analysis mortality is more in patients who arrive at night (between 9 pm and 5 pm) [Table 7].
Table 7.
Mortality depending on the arrival time of the patient

DISCUSSION
In our study the maximum numbers of patients admitted were between the age group of 15-30 years (31.55%) with a mean age of 29.43 ± 16.87 years. This probably was due to the inexperienced youth and their temperamental qualities. The present study also shows that the incidence of accidents was lower in people below the age of 15 years due to the fact that the children were taken care by elders and there was less use of vehicles in the adolescent age group. There was also low incidence of accidental injuries in people above 50 years of age; the reason probably could be due to less mobility of such population. This is consistent with other studies, which also show that injuries occur in more productive age group and they are more vulnerable to injury.[4,5,6,7,8,9,10]
Sex distribution was found to be heavily skewed towards males. This is probably because men are more active and thus exposed to risk-factors.[9] The delay in presentation of injured patient may be attributed to the fact that our center is a referral center, so patients usually come aftertaking initial treatment from local hospitals, nursing homes, etc.
Our study found that 66.71% of injury cases admitted to hospital was road side injuries, but according to National institute of Mental Health and Neurosciences NIMHANS study Road side injury RSI was the leading cause of injury in 46% of patients.[4] Two wheeler accidents was the most common mode of injury contributing to a total of 32.09% injuries, which along with a fall from height contributed to more than 50% of all admissions in a trauma center. In Indian set ups, houses are usually of poor design and they lack wall surrounding the roof, due to which persons sleeping on the roof are liable to fall during the night.[11] Studies have also suggested that environmental factors such as building structure and socio-economic factors such as the availability of electric lighting may contribute to falls to a greater extent in low- and middle-income countries.[12]
Among the injured patients of road traffic accidents, two wheeler vehicle collisions (12.30%) constitute the maximum percentage. Pedestrians represented the majority of victims sustaining injury as a result of being knocked by a vehicle, motorbike or cycle. This shows the erratic behavior and reckless driving on the road. Our findings are consistent with the study done by Mishra et al.[13] The higher percentage in our study may be attributed to the failure in proper traffic management and also due to the large number of pedestrians on the road.
The mean time of presentation of the injured patient reporting to the trauma centre was 2.53 ± 4.92 days. Reason can be attributed to the fact that our centre is a referral centre, so patients usually come after taking initial treatment from local hospitals, nursing homes, etc., Road side injuries (66.71%) were found to be the leading cause of admissions in our study followed by household injuries (23.66%). The findings are consistent with the findings of Gururaj.[14]
In the present study, the severity of injury was determined using the KTS II whose validity and reliability for use in both adults and children was described elsewhere [Table 6].[15] This scoring system compares favorably with other trauma scoring systems such as the revised trauma score and injury severity score. The majority of patients in this study suffered moderate injury according to KTS II score.
The admissions due to accident in rural areas were almost twice in relation to those inurban areas. Among the admitted injured patients, majority were from accidents in rural area favoring the fact that in an urban area overcrowding on roads results in low velocity injuries causing minimal damage to the patient for which admission is not required. Poor visibility of vehicle or road contributed to the injuries in 29.94% of cases in which pedestrians were most commonly involved. Poor visibility of vehicle or roads was responsible for 1/3rd of the total injuries. This is similar to findings of NIMHANS study.[4]
Rash and careless driving were the most common nature of driving fault accounting for 75% of cases in this group. Driving under the influence of alcohol, over speeding and overtaking were the major behavioral factors. 10.65% of the drivers were driving under the influence of alcohol. Drivers and occupants of motorized two wheeled vehicles, and pedestrians were involved in crashes to a greater extent among alcohol users.[16] With the emergence of injuries and alcohol as twin major public health problems, immediate efforts are required to reduce the burden in developing societies. Legislation and enforcement strategies along with education developed on epidemiological, clinical, and public-health research need to be coordinated, target oriented, visible and with stiffer penalties for achieving desired results.[16,17,18]
Driving a two wheeler without a helmet was a major contributor to injuries (71.77%). This justifies the use of helmet as an important preventive measure against head and oral maxillofacial injuries. This is more than the findings of study done by NIMHANS.[4] Among the motor vehicle injuries, it was observed that 79% of the drivers were not wearing seat belts at the time of accident and only 20.24% cases wearing seat belts were injured. This percentage is also higher as compared to other studies.[19] Approximately, 1/3rd of the drivers of different vehicle were driving without a driving license (33.47%). The reason may be the easy availability of the vehicle and the casual attitude of drivers towards obtaining a driving license.
Among the polytrauma patients admitted in our series torso injuries (80.49%) i.e., spinal cord injury combined with chest, abdominal and pelvic injury were the maximum followed by limb injury and head injury amongst all patients admitted in our series (52.27%). The high mortality rate in the present study was found in the night and early morning. It may be because of the lack of street and road lights that accidents were more severe at this time.
CONCLUSION
This study has demonstrated that the majority of injuries in developing countries are preventable. A greater level of awareness of safety on the roads, home, workplace is required at all levels with the development and implementation of safety policies and programs. This can be done by educating the public through the media and initiating road safety training campaigns in schools and colleges. The use of properly designed helmets should be made compulsory especially, among riders of motorized twowheelers. This might be effective in reducing incidence of head injury. Reducing driving under the influence of alcohol can be decreased by strict enforcement of law. Other preventive measures are use of speed control mechanisms and improving visibility of vehicles and roads by better lightening of roads. Methods should be devised to ensure early transportation of the patient to hospital. Strengthening training of doctors and allied personals in early recognition and management of the brain injured patient will go a long way in decreasing morbidity and mortality of head injured patients.
Undoubtedly, this man made tragedy can be effectively controlled and needs a vision and mission to act.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gururaj G. Injuries in India: A national perspective. NCMHbackground papers: Burden of disease in India,??? [Last accessed on 2009 Dec 09, Jan 2009]. Available from: http://www.whoindia.org/LinkFiles/Commision_on_Macroeconomic_and_Health_Bg_P2_Injury_in_India.pdf .
- 2.Uthkarsh PS, Suryanarayana SP, Gautham MS, Shivraj NS, Murthy NS, Pruthvish S. Profile of injury cases admitted to a tertiary level hospital in south India. Int J Inj Contr Saf Promot. 2012;19:47–51. doi: 10.1080/17457300.2011.603149. [DOI] [PubMed] [Google Scholar]
- 3.Kopits E, Cropper M The World Bank. Washington DC: World Bank Policy Research Working Paper No 3035; 2003. [Last accessed on 7th nov 2009]. Traffic Fatalities and Economic Growth. http://www.ntl.bts.gov/lib/24000/24400/24490/25935_wps3035.pdf . [Google Scholar]
- 4.Bengaluru Injury Surveillance Collaborators Group. Bangalore Publication; 2008. Road traffic surveillanceprogramme: A feasibility study: National Institute of Mental Health and Neurosciences; pp. 45–70. [Google Scholar]
- 5.Jadaan KS. The epidemiology of road traffic accidents in Jordan. J R Soc Health. 1989;109:141–4. doi: 10.1177/146642408910900411. [DOI] [PubMed] [Google Scholar]
- 6.Verma PK, Tewari KN. Regional Health Forum WHO South-East Asia Region. World Health Organisation; 2004. Epidemiology of road traffic injuries in Delhi: Results of survey; p. 8. [Google Scholar]
- 7.Manciaux M, Romer CJ. Geneva: WHO; 1991. Accidents in childhood and adolescence-The role of research; pp. 3–5. [Google Scholar]
- 8.Sahdev P, Lacqua MJ, Singh B, Dogra TD. Road traffic fatalities in Delhi: Causes, injury patterns, and incidence of preventable deaths. Accid Anal Prev. 1994;26:377–84. doi: 10.1016/0001-4575(94)90011-6. [DOI] [PubMed] [Google Scholar]
- 9.Mohan D. Transportation Research and Injury Prevention Programme. Delhi: Indian Institute of Technology; 2004. The road ahead: Traffic injuries and fatalities in India; pp. 1–30. [Google Scholar]
- 10.Jagnoor Road traffic injury prevention: A public health challenge. Indian J community Med. 2006;31:129–31. [Google Scholar]
- 11.Jagnoor J, Suraweera W, Keay L, Ivers RQ, Thakur JS, Gururaj G, et al. Childhood and adult mortality from unintentional falls in India. Bull World Health Organ. 2011;89:733–40. doi: 10.2471/BLT.11.086306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jitapunkul S, Yuktananandana P, Parkpian V. Risk factors of hip fracture among Thai female patients. J Med Assoc Thai. 2001;84:1576–81. [PubMed] [Google Scholar]
- 13.Mishra B, Sinha Mishra ND, Sukhla S, Sinha A. Epidemiological study of road traffic accident cases from Western Nepal. Indian J Community Med. 2010;35:115–21. doi: 10.4103/0970-0218.62568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gururaj G. Alcohol and road traffic injuries in South Asia: Challenges for prevention. J Coll Physicians Surg Pak. 2004;14:713–8. [PubMed] [Google Scholar]
- 15.Mutooro SM, Mutakooha E, Kyamanywa P. A comparison of Kampala trauma score II with the new injury severity score in Mbarara university teaching hospital in Uganda. East Cent Afr J Surg. 2010;15:62–70. [Google Scholar]
- 16.Gururaj G. The effect of alcohol on incidence, pattern, severity and outcome from traumatic brain injury. J Indian Med Assoc. 2004;102:157–60. [PubMed] [Google Scholar]
- 17.Kobusingye OC. Road safety threats and opportunities for poor countries. Afr Health Sci. 2004;4:199–201. [PMC free article] [PubMed] [Google Scholar]
- 18.Chagas Silva M, Gaunekar G, Patel V, Kukalekar DS, Fernandes J. The prevalence and correlates of hazardous drinking in industrial workers: A study from Goa, India. Alcohol Alcohol. 2003;38:79–83. doi: 10.1093/alcalc/agg016. [DOI] [PubMed] [Google Scholar]
- 19.Peden M, Scurfield R, Sleet D, editors. Geneva: World Health Organization; 2004. [Last accessed dec 8 2009]. World Report on Road Traffic Injury Prevention. http://www.who.int/world.health.day/2004/infomaterials/world_report/en/summary_en_rev.pdf . [Google Scholar]