

Abstract
Background and Aim:
Pain on intravenous (IV) cannulation continues to cause considerable anxiety among the patients visiting the hospital for elective surgery. Often, it is the only unpleasant experience, especially in ambulatory surgical settings. Although, anecdotal evidence suggests that antecubital fossa (ACF) might be less painful site for venous cannulation, no scientific study exists to validate the same.
Methods:
In this prospective randomised study, effect of site selection on pain of venous cannulation was studied. Fifty-five consecutive adults, scheduled to undergo elective surgery, were randomly allocated to get IV cannulation first on ACF (28 patients) or on dorsum of hand (DOH) (27 patients) followed by cannulation on the contralateral arm on the alternative site (DOH or ACF). Five patients were excluded due to multiple cannulation attempts. Pain scores on cannulation related to both sites were recorded and compared.
Results:
Non-parametric data and frequency data analysis, using the Wilcoxon signed rank test or the Chi-square test as appropriate, showed that ACF approach was significantly less painful in comparison to the DOH when using a 20-gauge cannula for venous cannulation (P < 0.05).
Conclusion:
We recommend that in the absence of any contraindications, ACF should be the cannulation site of choice. However, considerations like increased chance of kinking and obstruction might preclude such practice.
Keywords: Pain on cannulation, sites of venous cannulation, venous cannulation
INTRODUCTION
Venous cannulation is one of the most commonly performed invasive procedures in clinical practice. During the perioperative period, the anticipated pain prior to cannulation along with the resulting pain significantly elevates a patient's anxiety levels. Anaesthesia providers in the past have used a wide variety of measures such as the Valsalva manoeuvre,[1] local anaesthetic or ethyl chloride spray,[2] and application of eutectic mixtures of local anaesthetics[3] in an effort to obtund this pain/discomfort, but the degree of success remains limited.[4] The antecubital fossa (ACF) and the dorsum of the hand (DOH) are the commonly preferred sites for routine venous cannulation. The sensory innervation density of the skin varies depending upon the site; thus, the associated pain at various sites is likely to be different. The current study was conducted to evaluate site-specific pain thresholds (ACF vs. DOH) to venous cannulation in patients presenting for surgery.
METHODS
After Institutional Review Board clearance, informed/written pre-operative consent was obtained from the patients. The study was conducted in a 500 bedded district general hospital of about 500 beds. On literature search, no previous study comparing planned sites of cannulation could be found; thus for the study a longitudinal sampling strategy for a period of maximum 9 months was adopted with a planned interim analysis at the end of 3 months evaluating for any achieved significant difference in pain scores. A maximum of 3 such interim analyses was planned and further recruitment was to be terminated if a statistically significant result was found in an interim analysis or the recruitment period of 9 months was crossed (whichever occurred earlier). This allowed initial phase to act as a pilot study phase. Fifty-five consecutive adult patients of American Society of Anaesthesiologists physical status grades I/II, aged between 18 and 70 years undergoing general anaesthesia for elective surgery were eventually included in the study by the end of 6 months (2nd interim analysis). In each patient, two intravenous (IV) cannulae (20-gauge each) were inserted where one was used post-operatively to connect to a ‘patient controlled analgesia’ pump while the other was used to maintain fluid infusion and administer anaesthetic/medications. In order to eliminate any bias in reporting pain due to 2nd cannulation (series of painful stimulus may alter degree of pain felt) patients were divided into two random groups (by computer generated number sequence), DOH first group (27 patients) and ACF first group (28 patients). [Figure 1] Patients were premedicated with oral midazolam or diazepam as per individual anaesthesiologists’ preferences prior to shifting to the operating room. Prior to IV cannulation, the anaesthesiologist involved was given a questionnaire to evaluate his/her personal preference based on experience for the lowest possible pain when comparing the ACF or DOH site. Eventually, in each patient, either the DOH or the ACF site of one arm was cannulated first (on the basis of above-randomised allocation) for insertion of a 20-gauge Adsyte® cannula. Depending upon the site selected for insertion of the first cannula (ACF or DOH), the contralateral arm was used for venous cannulation on the second site using a 20-gauge Adsyte® cannula by an experienced anaesthesiologist. Patients requiring more than one attempt for venous cannulation at any of the above sites were excluded from the study analysis (observed in five patients). Rest of the fifty patients were then asked to rank their pain of each procedure on a pain scale of 1–10 (1: No pain; 10: Worst pain imaginable). A blinded observer (unaware of groups as to which site was cannulated first), collected data from the patient, whether they found the ACF or the DOH site to be the less painful site for cannula insertion.
Figure 1.
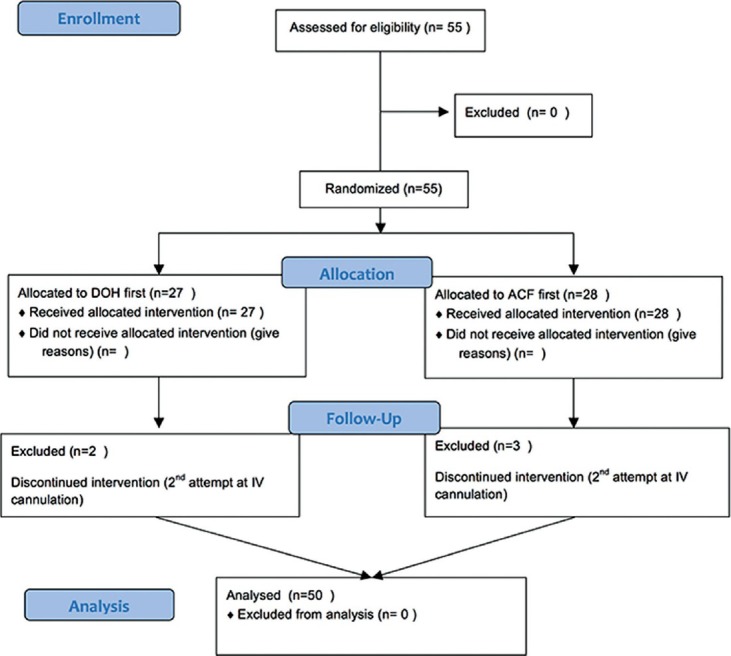
Consort diagram showing study plan
RESULTS
Statistical analysis was done using SPSS Software (IBM Inc., Chicago, IL, USA) for Macintosh. Descriptive statistics was used for demographic data. Non-parametric data and frequency data were analysed using the Wilcoxon signed rank test or the Chi-square test as appropriate. During comparisons, an alpha error of <5% (or P < 0.05) was chosen to be statistically significant, assuming a difference of 30% in pain scores between two sites.
Evaluating anaesthesiologists’ responses to questionnaires prior to cannulation, it was determined that 93.7% of patients considered the ACF to be a less painful site for cannula insertion than the DOH. As many as 22.9% said that they had, on occasion, used this site in preference to the DOH for the purpose of minimizing pain of insertion, with 10.4% doing so on regular basis. However, selection of this site is not without drawbacks as the IV infusions may not run as freely with the elbow flexed, and access to port of injection could be difficult.
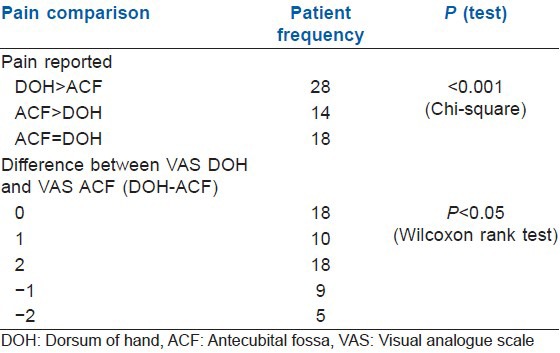
Fifty patients completed the trial: Sixteen were males, and 34 were females. Mean age of patients was 35.8 years, (range 19–56) [Table 1]. Twenty-eight of the 50 patients found the DOH to be a more painful cannulation site than that of the ACF site. Fourteen of the 50 patients found the ACF site to be a more painful cannulation site. Eight patients found no difference in terms of pain between the two cannulation sites. The data was analysed using a Chi-square test and showed that the selection of the DOH as the site of cannulation was significantly more painful than at the ACF site (P < 0.01). The difference between pain scores for the two sites of cannula insertion was analysed using the Wilcoxon signed rank test. This again showed a significant difference in venous cannulation pain between the DOH site and the ACF site (P < 0.05). Further analysis showed that of the patients who found the ACF to be a more painful site for cannula insertion, there was a difference of only one point in the pain scores of 35.71% of this group, whereas in the patients who found the DOH to be more painful site for cannula insertion, 17.85% of patients had a difference of one point in their pain scores. The remaining 82.15% of the patients had pain scores higher by two or more units [Table 2].
Table 1.
Patient parameters
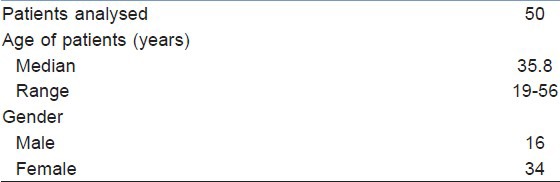
Table 2.
Pain comparison between the groups
DISCUSSION
Venous cannulation is usually the first procedure that anaesthesiologists perform on patients presenting for procedures that require sedation/anaesthesia, and is probably the one that patients will remember the most. Work to date has concentrated on assessing methods of providing local anaesthesia to the venepuncture site. While 22.9% of anaesthesiologists in our questionnaire stated that based on their experience of possible lower pain, they selected the ACF in preference to the DOH for the purpose of reducing pain on cannula insertion, there have been no investigations demonstrating a difference between these two commonly selected sites of cannula insertion. The results of our work demonstrate quite clearly that patients felt the ACF to be a significantly less painful site for cannula insertion than the DOH. Further support for this is seen in the assessment of pain scores. Not only did patients find that cannula insertion in the ACF to be more painful than in the DOH, but often, the difference was by more than two points. Furthermore, examination of the pain scores of the 14 people who felt the DOH to be less painful site for cannula insertion revealed that in 35.71%, there was a difference of no more than one point. Assessment of the pain scores of the 28 patients who found the ACF to be a less painful site for cannula insertion showed that there was a difference of no more than one point in 17.85% of cases, which would suggest that not only did patients find cannulation in the dorsum painful more frequently, but also that it produced a greater difference. Reasons for the difference between the two sites are uncertain but may include tougher skin and greater density of nociceptors[5,6] on the DOH. While the results of this study validate the clinical practice of selection of the ACF in an effort to minimise pain of cannula insertion, it remains to be seen whether it should be chosen as the optimal site for venous cannulation in view of the aforementioned drawbacks. Additionally, Yamada et al. showed that in around 30% patients, the ACF vein may overlie the median cutaneous nerve of forearm and thus can be injured.[7]
Work by Sado and Deakin has shown conclusively that local anaesthetic infiltration preceding cannula insertion to be significantly less painful than insertion of even a 22-gauge cannula.[8] Our study was performed without using a local anaesthetic prior to cannulation, and it is uncertain whether the difference between the two sites would still apply in situations where a local anaesthetic is used.
The importance of our findings can also be extrapolated for practical use in the paediatric population. Conduction of such pain assessment studies in children is difficult due to the limitations of child cooperation and grading the pain by the child. However, pain on IV cannulation in children draws more attention pre-operatively. Choosing less painful sites will help to gain confidence and cooperation of the child. Presently literature on paediatric site-specific pain is limited to make any direct conclusions. Thus, further research is needed to validate the finding from studies done in the adult population.
CONCLUSION
Pain thresholds vary on the basis of cannulation sites and IV cannulation in ACF is significantly less painful in comparison to the DOH. Thus, proper choice of sites like ACF (or other sites with evidence of lower pain potential) can be simple and effective methods of pain reduction during IV cannulation.
ACKNOWLEDGMENTS
The authors would like to thank Amit K. Manjunath (premed student, research assistant), Hospital of the University of Pennsylvania, Philadelphia, PA 19104, USA.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Agarwal A, Sinha PK, Tandon M, Dhiraaj S, Singh U. Evaluating the efficacy of the valsalva maneuver on venous cannulation pain: A prospective, randomized study. Anesth Analg. 2005;101:1230–2. doi: 10.1213/01.ane.0000167270.15047.49. [DOI] [PubMed] [Google Scholar]
- 2.Costello M, Ramundo M, Christopher NC, Powell KR. Ethyl vinyl chloride vapocoolant spray fails to decrease pain associated with intravenous cannulation in children. Clin Pediatr (Phila) 2006;45:628–32. doi: 10.1177/0009922806291013. [DOI] [PubMed] [Google Scholar]
- 3.Zempsky WT. Pharmacologic approaches for reducing venous access pain in children. Pediatrics. 2008;122(Suppl 3):S140–53. doi: 10.1542/peds.2008-1055g. [DOI] [PubMed] [Google Scholar]
- 4.Moore A, Straube S, McQuay H. Minimising pain during intravenous cannulation. BMJ. 2009;338:a2993. doi: 10.1136/bmj.a2993. [DOI] [PubMed] [Google Scholar]
- 5.Dauch JR, Lindblad CN, Hayes JM, Lentz SI, Cheng HT. Three-dimensional imaging of nociceptive intraepidermal nerve fibers in human skin biopsies. J Vis Exp. 2013:e50331. doi: 10.3791/50331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Frahm KS, Mørch CD, Grill WM, Lubock NB, Hennings K, Andersen OK. Activation of peripheral nerve fibers by electrical stimulation in the sole of the foot. BMC Neurosci. 2013;14:116. doi: 10.1186/1471-2202-14-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yamada K, Yamada K, Katsuda I, Hida T. Cubital fossa venipuncture sites based on anatomical variations and relationships of cutaneous veins and nerves. Clin Anat. 2008;21:307–13. doi: 10.1002/ca.20622. [DOI] [PubMed] [Google Scholar]
- 8.Sado DM, Deakin CD. Local anaesthesia for venous cannulation and arterial blood gas sampling: Are doctors using it? J R Soc Med. 2005;98:158–60. doi: 10.1258/jrsm.98.4.158. [DOI] [PMC free article] [PubMed] [Google Scholar]