

Abstract
This survey aimed to assess the conceptualization of and utilization of blood stasis syndrome within traditional East Asian medicine among Doctors of Korean Medicine (DKMs). A survey was conducted with 22 questions classified into four categories (the present status, problems and requirements of a BSS diagnosis; the concept, diseases and prescriptions regarding BSS; the present status and problems with the Korean standard classification of diseases (KCD) relevant to BSS and the demographic characteristics of the survey respondents). A total of 17,550 DKMs affiliated with the association of Korean medicine were sent surveys via e-mail. Of the 678 respondents, more than half (53%) had difficulties with the diagnosis of BSS because objective measurement methods were not readily available. Most respondents (88%) thought that the development of an objective diagnostic method for BSS was necessary. Regarding the concept of blood stasis, “an abnormal mass in organ and tissue” considered the most significant indicator, followed by extravasated blood, the blood circulating sluggishly and a disorder of the blood cells. According to 606 DKMs, a traumatic injury was the most frequent reason for BSS in the clinic. And the Dangkwisoo-san was most frequently mentioned prescription for BSS in the clinic. The majority of respondents (76%) reported that it was necessary for an additional code of BSS in KCD. Our data suggest the need to develop more objective diagnostic tools for BSS diagnosis. Future research into BSS should consider DKMs’ perceptions of BSS, diseases relevant to BSS and KCD codes. However, we cannot completely discount the possibility that the low response rate could indicate a biased selection of respondents and limit the interpretations of our study results.
Keywords: Blood stasis, traditional Korean medicine, traditional East Asian medicine, survey
Introduction
In traditional East Asia medicine (TEAM), blood is one of the basic elements that determine the body’s diverse physiologic functions. If pathogenic factors, e.g., – internal causes, external causes and causes that are neither internal nor external, – cause disharmony, a blood circulation disorder can occur. Blood stasis is one of the pathogenic products caused by disorder of the blood circulation and blood stasis syndrome (BSS), it is a pathological condition of stagnant blood within the body and collaterals (jing luo) [1,2]. This phenomenon is called ‘Eo Hyeol’ in Korean, ‘Yu Xue’ in Chinese and ‘Oketsu’ in Japanese. The concept of blood stasis has been interpreted, changed and developed systematically since ancient times [3].
BSS manifests with a dark-purple face or tongue, pain in a fixed position, bleeding, blood spots under the skin and an astringent pulse among other features [4]. BSS is mainly diagnosed by considering the BSS–related symptoms and signs gathered by the four examinations – inspection, listening and smelling, verbal inquiry and palpation. Since the 1980s, experts have established some diagnostic criteria and questionnaires for BSS diagnosis, e.g., the Oketsu checklist, the Quantified Diagnostic Criteria of BSS (QDCB) and the Blood stasis questionnaire [3,5,6]. These criteria and questionnaires mainly consist of signs and symptoms. The QDCB also includes measurement of complete blood viscosity, blood plasma viscosity, thrombus weight, platelet aggregation, microcirculation, hemodynamic and fibrinolytic activity markers. Recently, many researchers have reported the correlation of physiopathology with BSS, e.g. thrombus, atherosclerosis, proinflammatory cytokines and signaling pathway [7-12].
Because blood stasis connotes a disorder of blood circulation, the extravasated blood and the blood that is congested in a viscus, many diseases could be related to BSS. Cardiovascular disease, cerebral vascular disease, diabetes mellitus, chronic gastritis, chronic renal failure and chronic hepatitis are commonly thought to be BSS–related diseases [13-19].
Considering the importance of BSS in TEAM, there was not much information about the conceptualization of and utilization of blood stasis syndrome among doctors of Korean medicine (DKMs). This survey aimed to assess the conceptualization of and utilization of BSS among DKMs and provide an academic basis for future BSS research.
Materials and methods
Study design
This study was an e-mail survey of DKMs regarding their conceptualization of and utilization of BSS in TEAM.
Participants and recruitment
This survey was conducted between February 10 and March 4, 2014. We contacted the Association of Korean Medicine (AKOM) and received permission to use their member database. A total of 17,550 DKMs who were members of the AKOM were invited to participate in this survey via three e-mails, two were reminders. We surveyed licensed DKMs of the AKOM regardless of gender, age, and residence.
Survey development and variables
The questionnaire was developed by the research team and included the following key subjects (Appendix 1).
- Present status, problems and requirements with BSS diagnosis.
- Concept, diseases and prescriptions associated with BSS.
- Present status, problem and requirements of the Korean Standard Classification of Diseases (KCD) relevant to BSS; and.
- Demographic characteristics of the respondents.
Data sources/measurement
We surveyed licensed DKMs of the AKOM via e-mail.
Bias
Most of the participants possessed sufficient knowledge about BSS due to education and training. Therefore, there is unlikely to be a selection bias in this study. However a low response rate among surveyed participants could indicate selection bias.
Study size
There are approximately 21,000 DKMs in Korea. We contacted an AKOM administrator about the survey and obtain permission to use their address list of members for the survey. The total number of AKOM members was 17,550.
Statistical analysis
Descriptive statistics are presented with the frequency and percentage distributions for the categorical data. The analysis of the survey results were performed using Excel statistical analysis program (Microsoft, Excel 2010).
Ethical considerations
The ethical review committee of the Korea Institute of Oriental Medicine waived the need for formal ethical approval and for informed consent to be obtained from participants due to the nature of the study. The survey was conducted on a voluntary basis, and the participants agreed to the use of the collected data for scientific purposes.
Results
General characteristics
Of the initial 17,550 DKMs surveyed, only 678 responded (3.9%). Descriptive statistics for selected participant characteristics are given in Table 1. The respondents comprised 571 (84.2%) males and 107 (15.8%) females. Among the respondents, there were 323 (47.6%) physicians with under 10 years of experience, 223 (32.9%) with 10-20 years of experience and 132 (19.5%) with over 20 years of experience. A total of 506 (74.6%) worked in Korean medicine clinics, 77 (11.4%) worked in Korean medicine hospitals, and the others were in private practice at health centres or Korean medicine universities.
Table 1.
Demographic characteristics of respondents (n = 678)
| Classification | Total (n = 678) | |
|---|---|---|
|
| ||
| N | % | |
| Sex | ||
| Female | 107 | 15.8 |
| Male | 571 | 84.2 |
| Age (years) | ||
| 20-29 | 45 | 6.6 |
| 30-39 | 254 | 37.5 |
| 40-49 | 246 | 36.3 |
| 50-59 | 110 | 16.2 |
| > 60 | 23 | 3.4 |
| Residence | ||
| Seoul | 176 | 25.9 |
| Metropolis (7 region) | 175 | 25.7 |
| Other | 327 | 48.4 |
| Clinical experience (years) | ||
| 0-10 | 323 | 47.6 |
| 10-20 | 223 | 32.9 |
| Over 20 | 132 | 19.5 |
| Education | ||
| Bachelor | 329 | 48.5 |
| Master | 107 | 15.8 |
| Doctor | 242 | 35.7 |
| Place of work | ||
| KM hospital | 77 | 11.4 |
| KM clinic | 506 | 74.6 |
| Other (university, etc) | 95 | 14.0 |
| KM specialist | ||
| Yes | 149 | 22.0 |
| No | 529 | 78.0 |
All data are expressed as N (%).
Present status, problems and requirements with BSS diagnosis
Regarding the question how often they diagnosed BSS in all their patients, the most frequent answer was 10 to 30 % (n = 307, 45.3%), followed by below 10% (n = 158, 23.3%), 30 to 50% (n = 139, 20.5%), 50 to 70% (n = 46, 6.8%) and over 70% (n = 28, 4.1%) (Table 2). The most common difficulties in diagnosing BSS encountered by DKMs were “the lack of an objective measurement method” (n = 356, 52.5%), “an ambiguous definition of BSS” (n = 108, 15.9%), “absence of diagnostic equipment” (n = 106, 15.6%) and “absence of an appropriate diagnostic code for BSS” (n = 99, 14.6%). More than half (n = 599, 88.9%) thought that the development of an objective diagnostic method for BSS was necessary. The most important need for BSS research was “a clear definition of BSS” (n = 369, 54.4%), followed by diagnostic equipment (n = 347), “clinical practice guidelines for BSS” (n = 294, 43.4%), “a KCD code covered by insurance” (n = 239, 35.3%) and “an objective questionnaire” (n = 161, 23.7%).
Table 2.
Conceptualization and utilization of blood stasis syndrome by doctors of Korean medicine
| Questions | N | % |
|---|---|---|
| 1. Of all patients, how many did you diagnose as BSS? | ||
| 0-10%. | 158 | 23.3 |
| 10-30%. | 307 | 45.3 |
| 30-50%. | 139 | 20.5 |
| 50-70%. | 46 | 6.8 |
| Over 70%. | 28 | 4.1 |
| 2. The most difficult problem regarding diagnosis of BSS. | ||
| An ambiguous definition of BSS. | 108 | 15.9 |
| The lack of an objective measurement method. | 356 | 52.5 |
| Absence of diagnostic equipment. | 106 | 15.6 |
| Absence of an appropriate diagnostic code for BSS. | 99 | 14.6 |
| Other. | 9 | 1.3 |
| 3. Necessary of developing an objective BSS diagnosis method. | ||
| Absolutely essential. | 308 | 45.4 |
| Necessary. | 291 | 42.9 |
| Moderate. | 55 | 8.1 |
| Not necessary. | 8 | 1.2 |
| Completely unnecessary. | 6 | 0.9 |
| I don’t know. | 10 | 1.5 |
| 4. The most important thing for the study of BSS diagnosis (multiple answers permitted). | ||
| A clear definition of BSS. | 369 | 54.4 |
| An objective questionnaire. | 161 | 23.7 |
| Development of diagnostic equipment. | 347 | 51.2 |
| Clinical practice guidelines for BSS. | 294 | 43.4 |
| KCD code relevant to BSS that is covered by insurance. | 239 | 35.3 |
| Other. | 7 | 1.0 |
| 5. The concept of blood stasis (multiple answers permitted). | ||
| An abnormal mass in organ and tissue. | 529 | 78.0 |
| A disorder of blood composition. | 262 | 38.6 |
| Extravasated blood. | 311 | 45.9 |
| Sluggishly circulating blood. | 342 | 50.4 |
| Other. | 11 | 1.6 |
| 6. The most relevant pathological mechanism for BSS (multiple answers permitted). | ||
| Tissue damage and inflammation caused by internal or external factors. | 543 | 80.1 |
| Abnormality in the component of blood caused by infection or genetic factor. | 259 | 38.2 |
| Thrombus or abnormality of hemorheology. | 489 | 72.1 |
| Neoplasm. | 323 | 47.6 |
| Other. | 16 | 2.4 |
| 7. Of all patients, how many did you diagnose using the U-code? | ||
| 0-10%. | 449 | 66.2 |
| 10-30%. | 159 | 23.5 |
| 30-50%. | 39 | 5.8 |
| 50-70%. | 15 | 2.2 |
| Over 70%. | 16 | 2.4 |
| 8. Of all BSS patients, how many did you diagnose using the U-code? | ||
| 0-10%. | 562 | 82.9 |
| 10-30%. | 73 | 10.8 |
| 30-50%. | 24 | 3.5 |
| 50-70%. | 9 | 1.3 |
| Over 70%. | 10 | 1.5 |
| 9. Why did you not use the U-code to diagnose BSS? (multiple answers permitted) | ||
| I did not know the U-code. | 258 | 38.1 |
| If I diagnose a BSS patient using the U-code, the patient is not covered by insurance. | 392 | 47.8 |
| I could diagnose the BSS patient using another KCD code(s). | 289 | 42.6 |
| The patients did not understand the U-code. | 62 | 9.1 |
| I did use the U-code. | 52 | 7.7 |
| 10. Do you think that the registration of a new KCD code for BSS is necessary? | ||
| It is necessary. | 515 | 76.0 |
| It is not necessary. | 77 | 11.4 |
| I don’t know. | 86 | 12.7 |
| 11. How should a new KCD code for BSS be registered? | ||
| Register a new BSS code outside the U or R-codes. | 147 | 28.8 |
| Register a new BSS code below the existing codes. | 140 | 27.5 |
| If the new BSS code is covered by insurance, it does not matter which form. | 222 | 43.5 |
| Other. | 1 | 0.2 |
| 12. What is(are) the most frequent prescription(s) you use in the clinic? (multiple answers permitted) | ||
| Dangkwisoo-san. | 639 | 94.2 |
| Gyezibokryeong-whan. | 502 | 74.0 |
| Onkyung-tang. | 385 | 56.8 |
| Doinseunggi-tang. | 368 | 54.3 |
| Hyeolbuchukeo-tang. | 317 | 46.8 |
All data are expressed as N (%).
Concept, diseases and prescriptions regarding BSS
“An abnormal mass in organ and tissue” was the most common conception of blood stasis (multiple answers permitted) (n = 529, 78.0%), followed by “extravasated blood” (n = 342, 50.4%), “sluggishly circulating blood” (n = 311, 45.9%) and “a disorder of blood cells” (n = 262, 38.6%) (Table 2). In addition, 543 DKMs reported that the pathological mechanism of blood stasis was tissue damage and inflammation caused by internal or external factors. In relation to questions 7 and 8, regarding the connection between BSS and disease, 639 DKMs (94.2%) thought that traumatic injury was the most relevant and related condition followed by menstruation-related conditions (n = 579), cerebrovascular disease (n = 488) and cardiovascular disease (n = 380). Additionally, 606 DKMs reported that traumatic injury was the most frequent reason for diagnosis of BSS in the clinic, other frequently reported aliments included menstruation-related conditions (n = 509), cerebrovascular disease (n = 295) and cardiovascular disease (n = 126) (Figure 1). The most frequent prescription (multiple answers permitted, n = 639, 94.2%) for BSS patients in the clinic was the Dangkwisoo-san.
Figure 1.
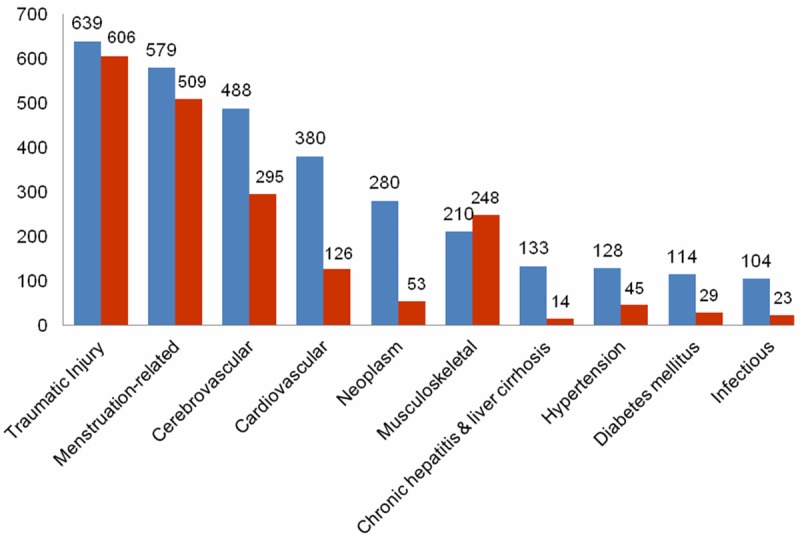
The connection between diseases (conditions) and blood stasis syndrome (BSS) according to the doctors of Korean medicine. (multiple answers permitted). Blue: The relevant diseases (conditions) considered relating to BSS by doctors of Korean medicine; Red: The frequent diseases (conditions) relating to BSS in a clinic; Number: The number of doctor of Korean medicine.
Present status, problems and requirements with Korean Standard Classification of Diseases relevant to BSS.
Most participants (n = 449, 66.2%) reported that diagnosis using U-code was below 10 % and that a BSS diagnosis using a U-code was also below 10%, either (n = 562, 82.9%) (Table 2). The most frequent reason why they didn’t use U-code was that the patient wouldn’t be covered by insurance (n = 392). Most responders (n = 515, 76%) thought that registration of a new KCD code relevant to BSS was necessary and 222 DKMs thought that if a new BSS code were covered by insurance, then the code format did not matter.
Discussion
This study was conducted to report on the conceptualization and utilization of the blood stasis syndrome by DKMs in South Korea. Of the 678 respondents, more than half encountered difficulties in diagnosing BSS because of the lack of an objective measurement method. We suggested it was because the important symptoms for BSS diagnosis, such as dark-purple face or tongue, infraorbital darkness, an astringent pulse and so on, didn’t have clearly quantitative standard because these symptoms are subjective or difficult to measure objectively. It was a problem not only for BSS, but pattern identification [20]. An objective measurement method has been one of the major issues and challenges in TEAM. It could be one of solutions that finding new biomarkers and establishing a standard diagnostic for BSS with those.
The majority (n = 599, 88.9%) thought that the development of an objective diagnostic method for BSS was essential for clinical diagnosis. We supposed that DKMs were not satisfied with current questionnaires for BSS, and that they want more or other objective methods to measure signs of BSS and more relevant diagnostic equipment.
Furthermore, many DKMs wanted a clear definition of blood stasis. It seems to be because the concept of blood stasis has changed and developed since ancient times. Actually, the classic definition of blood stasis was comparatively clear, which was a pathogenic product of stagnant blood within the body. However, regarding its pathological mechanism and utilization of BSS in a clinical field, it seemed to be more complicated. So, we assumed that many DKMs really wanted a clear correlation between the classical blood stasis with pathological mechanism and diseases, based on scientific evidence. And we suggested that such ‘modern correlation’ could further help the communications among DKMs and western medical doctors.
Regarding the concept and definition of blood stasis, most DKMs generally agreed that BSS is “an abnormal mass in organ and tissue” (n = 529, 78.0%), but only half agreed with the concept of blood stasis as sluggishly circulating blood. This finding demonstrates that differences of opinion exist over the main concept of blood stasis in China [3]. In addition, we found considerable disagreement between the DKMs’ concept of blood stasis and the clinical situation in Korea. Most DKMs generally agreed that blood stasis is an abnormal mass in organ and tissue and an abnormal mass in organ and tissue is closely related with tumor or hematoma [4]. But, most DKMs (n = 639, 94.2%) thought that traumatic injury was the most frequently relevant condition and 606 DKMs (89.4%) reported that traumatic injury was the most frequent disease in a clinic setting, which suggests that the most common theoretical definition of BSS may not reflect actual clinical practice and observation well.
Dangkwisoo-san, which was composed of Angelicae Gigantis Radix, PaeoniaeRadix Rubra, Linderae Radix, Cyperi Rhizoma, Sappan Lignum, Carthami Flos, Persicae Semen, Cinnamomum cassia, Glycyrrhizae Radix was the most frequently prescribed herbal formula for BSS patients in the clinic. Generally, Dangkwisoo-san has been usually prescribed in traumatic injury [21]. This indicates further that the clinical coverage of BSS in Korea give priority to traumatic injuries compared with the popularity of its concepts.
Most of participants didn’t use the U-code for BSS diagnosis. We suspect that the reasons for this limited coverage were the lack of KCD codes for BSS and the current U-codes relevant to BSS are not reimbursed by private insurance. A total of 515 DKMs (76%) also thought that registration of a new KCD code relevant to BSS was necessary. And a further 222 DKMs said that if the new BSS code were covered by insurance, then the code form did not matter.
There are some limitations to the current study. We surveyed DKM practitioners, thus giving us a snapshot of the concept of blood stasis and its use among DKM practitioners, but we do not know the extent to which this reflects how BSS is understood and used in China, Japan or Western countries. Consequently our results are limited to Korea and cannot be generalized to other countries. A second limitation is that while the survey was sent to 17,550 DKM practitioners, only 678 responded to the survey, which is only 3.9% of those surveyed and only approximate 3.2% of the estimated total number of DKM practitioners. This low response rate could indicate bias and weaken generalizability of results. However, despite these limitations we feel that the survey has added important information very useful to future studies of BSS. We propose that a survey of TEAM practitioners in other countries can help address the issue of generalizability of findings and further that additional strategies should be used to increase the response rate among surveyed practitioners.
In conclusion, our data suggest the need to develop more objective tools and expand the tools to capture a wider range of understanding and utilization for diagnosis of BSS. We should proceed with further research into BSS to investigate the conceptualization and utilization of BSS both among DKMs’ in Korea and among other TEAM practitioner groups outside Korea and to further develop the concept of BSS, the disease and conditions relevant to BSS and potential KCD and International Classification of Diseases (ICD) codes.
Acknowledgements
This research was supported by the Korea Institute of Oriental Medicine (K14281).
Appendix 1
Questionnaire: Perception on Blood Stasis Syndrome in Korean Medicine
A. These are general questions about the present status, problems and requirements with BSS diagnosis.
1) In what percentage of your patients did you diagnose BSS?
a) Below 10%.
b) 10 to 30%.
c) 30 to 50%.
d) 50 to 70%.
e) Over 70%.
2) What do you think is the most difficult problem regarding diagnosis of BSS?
a) An ambiguous definition of BSS.
b) The lack of an objective measurement method.
c) The absence of diagnostic equipment.
d) The absence of an appropriate diagnostic code for BSS.
e) Other (please explain):
3) Do you think that the development of objective BSS diagnosis method is necessary?
a) It is absolutely essential.
b) I agree that it is necessary in some ways.
c) Its necessity is moderate.
d) It is not necessary.
e) It is completely unnecessary.
f) I don’t know.
4) Which of the following do you think is the most important for the study of BSS diagnosis?
a) A clear definition of BSS.
b) An objective questionnaire.
c) Development of diagnostic equipment.
d) Clinical practice guideline for BSS.
e) KCD code relevant to BSS that is, covered by insurance.
f) Other (please explain):
B. These are questions regarding the concept, diseases and prescriptions for BSS.
5) What do you think about blood stasis? (multiple answers permitted).
Blood stasis occurs when abnormal blood stagnates within the body, including, which is a pathological product and pathogenic factor.
a) An abnormal mass in organ and tissue.
b) A disorder of blood compositions.
c) Extravasated blood.
d) Sluggishly circulating blood.
e) Other (please explain):
6) Which of the following do you think are the most relevant pathological mechanism for BSS? (multiple answers permitted).
a) Tissue damage and inflammation caused by internal or external factors.
b) Abnormality in the components of blood caused by infection or a genetic factor.
c) Thrombus or abnormality of hemorheology.
d) Neoplasm.
e) Other (please explain):
7) Which of the following do you think are the most relevant diseases or conditions for BSS? (multiple answers permitted).
a) Ischemic heart disease.
b) Cerebrovascular disease.
c) Traumatic injury.
d) Musculoskeletal disease (exclude traumatic injury).
e) Menstruation-related disease.
f) Chronic hepatitis or liver cirrhosis.
g) Chronic renal failure.
h) Infectious disease.
i) Hypertension.
j) Diabetes mellitus.
k) Neoplasm.
l) Other (please explain):
8) Which of the following do you think are the most frequent diseases relevant to BSS? Please choose 3 diseases from the above examples.
9) The following prescriptions are remedies for blood stasis. Please choose the most frequent prescriptions you use in the clinic. (multiple answers permitted)
a) Dangkwisoo-san.
b) Gyezibokryeong-whan.
c) Dansam-eum.
d) Hyunhosaek-san.
e) Onkyung-tang.
f) Doinseunggi-tang.
g) Silso-san.
h) Tongyu-tang.
i) Hyeolbuchukeo-tang.
j) Modified Sujeom-San.
k) Modified Doinseunggi-tang.
l) Soeo-eum.
m) Sobokchukeo-Tang.
n) Daehwangmaengchung.
o) Sihosamultang.
p) Jisilhaebaekgyeji-tang.
q) Tonggyuhwalhyeol-tang.
r) Cheongonpaedok-eum.
s) Dodamhwalhyeol-tang.
t) Sambu-tang.
u) Boyanghwano-tang.
v) Bokbangdaeseunggi-tang.
w) Insamyangyoung-tang and Doinseunggi-tang.
x) Mokyakjetong-tang.
y) Sintongchukeo-tang.
z) Sengchinsan.
Aa) Sunbangwhalmyung-Eum.
Ab) Chili-san.
Ac) Cheonggangeonbi-Tang.
Ad) Geupguhoeyang tang.
Ae) Seogagjihwang-tang.
Af) Other (please explain):
C. Present status, problems and requirements of the Korean Standard Classification of Diseases relevant to BSS.
10) What proportion of all patients did you diagnose using the U-code?
a) Below 10%.
b) 10 to 30%.
c) 30 to 50%.
d) 50 to 70%.
e) Over 70%.
11) What proportion of BSS patients did you diagnose using the U-code?
a) Below 10%.
b) 10 to 30%.
c) 30 to 50%.
d) 50 to 70%.
e) Over 70%.
12) Why did you not use the U-code to diagnose BSS, if applicable?
a) I did not know the U-code.
b) If I diagnose a BSS patient using the U-code, the patient is not covered by insurance.
c) I did not use the U- code, because I could diagnose the BSS patient using another KCD codes.
d) The patients did not understand the U-code.
e) I did use the U-code.
f) Other (please explain):
13) Do you think that the registration of a new KCD code for BSS is necessary?
a) It is necessary.
b) It is not necessary.
c) I don’t know.
14) If you answered “a” to Question 13, how should a new KCD code be registered?
a) Registering a new BSS code separate from the U or R-code.
b) Registering a new BSS code below the existing codes.
c) If the new BSS code was covered by insurance, it does not matter what the code form is.
d) Other (please explain):
D. These are questions about you.
15) Where is your place of work?
a) Seoul metropolitan city.
b) Other (please specify the city/town and province).
16) How old are you?
a) I’m in my 20-s.
b) I’m in my 30-s.
c) I’m in my 40-s.
d) I’m in my 50-s.
e) I’m 60 years or older.
17) What is your gender?
a) Male.
b) Female.
18) How long have you worked as a Korean medical doctor?
a) Fewer than five years.
b) Between five and 10 years.
c) Between 10 and 20 years.
d) More than 20 years.
19) What are your qualifications?
a) I completed a bachelor’s degree in Korean medicine.
b) I completed a master’s degree in Korean medicine.
c) I completed a doctorate in Korean medicine.
20) What University did you graduate from?
a) Gachon (Kyung Won) Univ. KM.
b) Kyung Hee Univ. KM.
c) Daegu Haany Univ.
d) Dae Jeon Univ. KM.
e) Dong Guk Univ. KM.
f) Dong Sin Univ. KM.
g) Dong Eui Univ. KM.
h) Sang Ji Univ. KM.
i) Se Myeong Univ. KM.
j) Won Kwang Univ. KM.
k) Woo Suk Univ. KM.
l) Pusan national Univ. KM.
21) Do you have a specialist qualification?
a) I am a specialist of Korean medicine.
b) I am not a specialist of Korean medicine.
22) Where do you work?
a) I work in a KM hospital.
b) I work in a KM clinic.
c) Other (please explain):
Disclosure of conflict of interest
None to declare.
References
- 1.Matsumoto C, Kojima T, Ogawa K, Kamegai S, Oyama T, Shibagaki Y, Kawasaki T, Fujinaga H, Takahashi K, Hikiami H, Goto H, Kiga C, Koizumi K, Sakurai H, Muramoto H, Shimada Y, Yamamoto M, Terasawa K, Takeda S, Saiki I. A Proteomic Approach for the Diagnosis of ‘Oketsu’ (blood stasis), a Pathophysiologic Concept of Japanese Traditional (Kampo) Medicine. Evid Based Complement Alternat Med. 2008;5:463–474. doi: 10.1093/ecam/nem049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen KJ. Blood stasis syndrome and its treatment with activating blood circulation to remove blood stasis therapy. Chin J Integr Med. 2012;18:891–896. doi: 10.1007/s11655-012-1291-5. [DOI] [PubMed] [Google Scholar]
- 3.Wu D, Chen J, Zhu H, Xiong XG, Liang QH, Zhang Y, Zhang Y, Wang Y, Yang B, Huang X. UPLC-PDA determination of paeoniflorin in rat plasma following the oral administration of Radix Paeoniae Alba and its effects on rats with collagen-induced arthritis. Exp Ther Med. 2014;7:209–217. doi: 10.3892/etm.2013.1358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yang DH, Park YJ, Park YB. A Fundamental Study for Making a Questionaire of Blood Stasis. The Journal of The Korean Institute of Oriental Medicine Diagnosis. 2005;9:84–97. [Google Scholar]
- 5.Terasawa K. The presentation of diagnostic criteria for “Yu-xie” (stagnated blood) conformation. Int J Oriental Medicine. 1989;14:194–213. [Google Scholar]
- 6.Park YJ, Yang DH, Lee JM, Park YB. Development of a valid and reliable blood stasis questionnaire and its relationship to heart rate variability. Complement Ther Med. 2013;21:633–640. doi: 10.1016/j.ctim.2013.08.019. [DOI] [PubMed] [Google Scholar]
- 7.Wang J, Yu G. A Systems Biology Approach to Characterize Biomarkers for Blood Stasis Syndrome of Unstable Angina Patients by Integrating MicroRNA and Messenger RNA Expression Profiling. Evid Based Complement Alternat Med. 2013;2013:510208. doi: 10.1155/2013/510208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Guo S, Chen J, Chuo W, Liu L, Feng X, Lian H, Zheng L, Wang Y, Xie H, Luo L, Zheng C, Fu B, Wang W. A New Biomarkers Feature Pattern Consisting of TNF-alpha, IL-10, and IL-8 for Blood Stasis Syndrome with Myocardial Ischemia. Evid Based Complement Alternat Med. 2013;2013:130702. doi: 10.1155/2013/130702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Huang Y, Wang JS, Yin HJ, Chen KJ. The Expression of CD14(+)CD16(+) Monocyte Subpopulation in Coronary Heart Disease Patients with Blood Stasis Syndrome. Evid Based Complement Alternat Med. 2013;2013:416932. doi: 10.1155/2013/416932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yuan ZK, Wang LP, Huang XP. The screening and the functional pathway analysis of differential genes correlated with coronary heart disease of blood stasis syndrome. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2012;32:1313–1318. [PubMed] [Google Scholar]
- 11.Wang J, Yu G. Biomedical mechanisms of blood stasis syndrome of coronary heart disease by systems biology approaches. Chin J Integr Med. 2014;20:163–169. doi: 10.1007/s11655-013-1461-3. [DOI] [PubMed] [Google Scholar]
- 12.Hao EW, Deng JG, Du ZC, Bao CH, Lu XY, Deng XQ, Tang ZL. Study on the regulation role of semen persicae to cAMP-PKA signal pathway in the rats with cold and heat blood stasis syndrome. Zhong Yao Cai. 2013;36:780–783. [PubMed] [Google Scholar]
- 13.Du JP, Shi DZ, Li TC, Xu H, Chen H. Correlation between blood stasis syndrome and pathological characteristics of coronary artery in patients with coronary heart disease. Zhong Xi Yi Jie He Xue Bao. 2010;8:848–852. doi: 10.3736/jcim20100908. [DOI] [PubMed] [Google Scholar]
- 14.Tang H, Gu BL, Zhou XM. Study on the scores of blood stasis syndrome of acute ischemic stroke and its correlation with TOAST subtypes. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2012;32:1500–1502. [PubMed] [Google Scholar]
- 15.Wei J, Wu R, Zhao D. Analysis on traditional Chinese medicine syndrome elements and relevant factors for senile diabetes. J Tradit Chin Med. 2013;33:473–478. doi: 10.1016/s0254-6272(13)60151-x. [DOI] [PubMed] [Google Scholar]
- 16.Luo JW, Chen H, Wu XY. Relationship between gene polymorphism and haplotype of SLC6A2 promoter and blood-stasis pattern in patients with essential hypertension. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2010;30:458–462. [PubMed] [Google Scholar]
- 17.Liu M, Liu Z. Overview of clinical study on traditional Chinese medicine invigorating spleen and stomach, promoting blood circulation and remove blood stasis in treatment of chronic atrophic gastritis. Zhongguo Zhong Yao Za Zhi. 2012;37:3361–3364. [PubMed] [Google Scholar]
- 18.Qu K, Wang TF, Zhao Y, Xue XL, Wu XY, Deng HL, Yang L, Yu LL, Yue H, Wang QG. Common syndrome factors of traditional Chinese medicine in chronic renal failure based on the questionnaire investigation among experts. Zhong Xi Yi Jie He Xue Bao. 2010;8:1147–1152. doi: 10.3736/jcim20101206. [DOI] [PubMed] [Google Scholar]
- 19.Liu SY, Zhang YQ, Liu YL, Guo P, Zhou CM. Intervention of chronic hepatitis B liver fibrosis patients in different stages by syndrome typing and different activating blood removing stasis methods: a clinical study. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2013;33:1457–1461. [PubMed] [Google Scholar]
- 20.O’Brien KA, Birch S. A review of the reliability of traditional East Asian medicine diagnoses. J Altern Complement Med. 2009;15:353–366. doi: 10.1089/acm.2008.0455. [DOI] [PubMed] [Google Scholar]
- 21.Wei C. Clincial observation of Dangguixu Powder in treating 40 cases of acute pulmonary contusion. Journal of Modern Medicine & Health. 2013;29:1768–1769. [Google Scholar]