

Abstract
This retrospective study was performed to determine the ranges of the sodium gradient (SG) between the dialysate sodium concentration (DNa) and serum sodium concentration (SNa) in hemodialysis (HD) patients and to examine the relationships between HD parameters over a 1 year period. Fifty-five clinically stable HD patients, who had been on HD >2 years were enrolled. Monthly HD [ultrafiltration (UF) amount, systolic blood pressure (SBP), frequency of intradialytic hypotension (IDH)] and laboratory data were collected and 12-month means were subjected to analysis. The SG was calculated by subtracting SNa from prescribed DNa. Mean SG values were 1.5±3.3 (range -5.6~9.1). SG was positively related to DNa and the frequency of IDH. A higher SG was associated with larger UF amounts and SBP reduction during HD. The percentages of patients with a SG ≥3mEq/L increased as DNa increased. On the other hand, SG was not found to be associated with SNa or pre-HD SBP. DNa appears to cause a significant increase in SG, and this seems to be related to HD parameters, such as, UF amount and IDH.
Keywords: Renal dialysis, Dialysis solutions, Sodium
Introduction
In chronic HD patients, sodium(Na+) balance largely depends on interdialytic dietary salt intake and intradialytic Na+ removal1). To preserve a neutral Na+ balance, interdialytic Na+ gain should be removed during HD.
From the 1980s, dialysis units have adopted high sodium bicarbonate dialysate because a higher dialysate sodium concentration (DNa) reduces the level of dialysis discomfort and the incidence of symptomatic hypotension and disequilibrium2). However, there is concern that a DNa higher than the serum sodium concentration (SNa) will result in a diffusive Na+ flux from dialysate to the patient, which can lead to a positive Na+ balance during HD and cause fluid overload and hypertension2). Indeed, higher sodium gradients (SGs) are associated with increased thirst3) and interdialytic weight gain3,4).
Furthermore, dialysis patients appear to have a unique set point for SNa5), which is stable over long-term observations6) and is actively defended7). Therefore, the use of a fixed DNa for all HD patients can cause a positive Na+ balance in some patients, which strengthen the importance of DNa individualization to achieve neutral Na+ balance8).
The aim of this retrospective study was to document sodium gradient (SG) ranges using SNa and SNa corrected for the Gibbs-Donnan effect, the void volume, and even for hyperglycemia in HD patients, and to examine relationships between SG, ultrafiltration (UF) amount, and blood pressure (BP).
Materials and Methods
1. Subjects
This retrospective, observational, clinical study was performed on end stage renal disease (ESRD) patients who were followed up at a HD center in Inha University Hospital (Incheon, Republic of Korea) from February 2013 to January 2014. In this HD center, DNa had been previously fixed to 138mEq/L for all patients. However, in view of associated problems, such as, volume overload and hypertension, DNa was individualized to BP from January 2010. In patients whose BP was well controlled, DNa was maintained at 138mEq/L, but in others, DNa was reduced to 135 or 136mEq/L. On the other hand, in patients who exhibited dialysis hypotension infrequently, DNa was increased to 140 or 142mEq/L. In patients who exhibited dialysis hypotension frequently, a sodium profiling or combined sodium/ultrafiltration profiling method was applied.
HD patients that had been clinically stable for more than 2 years were enrolled in this study. The exclusion criteria were congestive heart failure, liver cirrhosis, malignancy, acute myocardial infarction, any hemodynamically unstable condition, the requirement for a sodium profiling method during HD, hospital admittance for infection, cardiovascular disease, malignancy, transfer to another hospital, or kidney transplantation during the study period. Of the 102 patients initially considered, 55 were considered eligible and these patients constituted the study cohort.
HD was performed for 4 hours per session, three times per week, using a polysulfone dialyzer (F6HPS, Fresenius Medical Care, Bad Homburg, Germany) and a Fresenius Medical Care 5008 machine. Dialyzers were not reused. Hemotrate®-B No. 1 and No. 2 (JW Pharmaceutical, Republic of Korea) were used as dialysate concentrates for non-diabetics, and Hemo B dex® 0.15% No. 1 and No. 2 (JW Pharmaceutical, Republic of Korea) were used for diabetics. Blood flow rates were between 250 and 300mL/min, depending on the arteriovenous fistula status. The dialysate flow rate was 500mL/min. BP was measured hourly using an automated BP measuring device attached to the dialysis machine. Kt/Vurea values were calculated using the Daugirdas second generation equation10).
The study protocol was approved by the Institutional Review Board of Inha University Hospital and complied with the Declaration of Helsinki. The requirement for written consent was waived because of the retrospective nature of the study. All data used was obtained routinely for the purpose of patient management.
2. Correction of serum sodium(SNa)
Serum sodium concentrations (SNa) were measured using an indirect potentiometry method (Hitachi 7600, Toshiba, Tokyo). All SNa values were corrected for void volume and the Gibbs-Donnan effect using the following formula:
| csNa=SNa×[1.007-(0.009×TP)]/[0.989-(0.0047×TP)], |
where TP is serum total protein (g/dL) and csNa is corrected SNa9).
When serum glucose exceeded 100mg/dL, SNa was further corrected for glucose, using the following formula:
| csNag=csNa+0.0016×[serum glucose-100], |
where csNag means csNa corrected for serum glucose concentration11).
3. Calibration of dialysate sodium concentration
The quality of DNa delivery was assured by taking monthly DNa measurements and by machine calibration.
4. Calculation of sodium gradient
The sodium gradient between dialysate and blood was calculated using the following equations:
| SGna=DNa - SNa, |
| SGcna=DNa - csNa, |
| SGcnag=DNa - csNag, |
where SGna is the sodium gradient calculated using SNa, SGcna the sodium gradient calculated using csNa, SGcnag the sodium gradient using csNag, and DNa is the prescribed DNa.
5. HD and laboratory data
UF amount, DNa, pre- and post-HD SBP, and dry weight data were determined at monthly blood examinations, and biochemical data, that is, pre-HD SNa, glucose, total protein (TP), albumin, BUN, creatinine, hemoglobin, and post-HD BUN were obtained from the medical records from February 2013 to January 2014. Serum osmolality was calculated using the following equation:
| sOsm(mOsm/kg)=2×SNa+BUN/2.8+glucose/18, |
where sOsm is the calculated serum osmolality12). ΔSBP was calculated as follows:
| ΔSBP=(pre-HD - post-HD) SBP. |
The 12-month means of the variables for each patient were analyzed. The number of intradialytic hypotension (IDH) episodes was also investigated. The definition of IDH used was a modification of that used by Chesterton et al., that is an SBP of <100mmHg with or without symptoms13).
6. Statistical analysis
Results are presented as means±SDs or as medians, modes and ranges. The coefficient of variation (CV) of SNa was calculated using the following equation:
| CV=SD×100/mean |
Differences between SNa and csNa or csNag were evaluated using a paired t-test. The unpaired Student's t-test was used to determine the significance of differences between group mean values. Group categorical data were compared using the chi-square test, and the Pearson's correlation coefficients were used to determine the natures of relationships between two variables. P-values of <0.05 were considered significant.
Results
1. Patient characteristics
Of 55 patients, 26 (47.3%) were male and 24 (43.6%) were diabetics (Table 1). Mean overall patient age was 59±11 years, mean patient dry weight was 67±10 kg, and mean HD duration was 8.5±4.4 years. The mean number of anti-hypertensive drugs being taken was 1.6±1.2. At study commencement, mean pre-HD BUN, creatinine, hemoglobin, total protein, albumin, glucose concentrations, and Kt/Vurea were 79.3±18.7mg/dL, 11.4±2.8mg/dL, 10.3±1.1 g/dL, 6.9±0.4 g/dL, 4.0±0.3 g/dL, 144±67mg/dL, and 1.4±0.2, respectively.
Table 1.
Patient characteristics
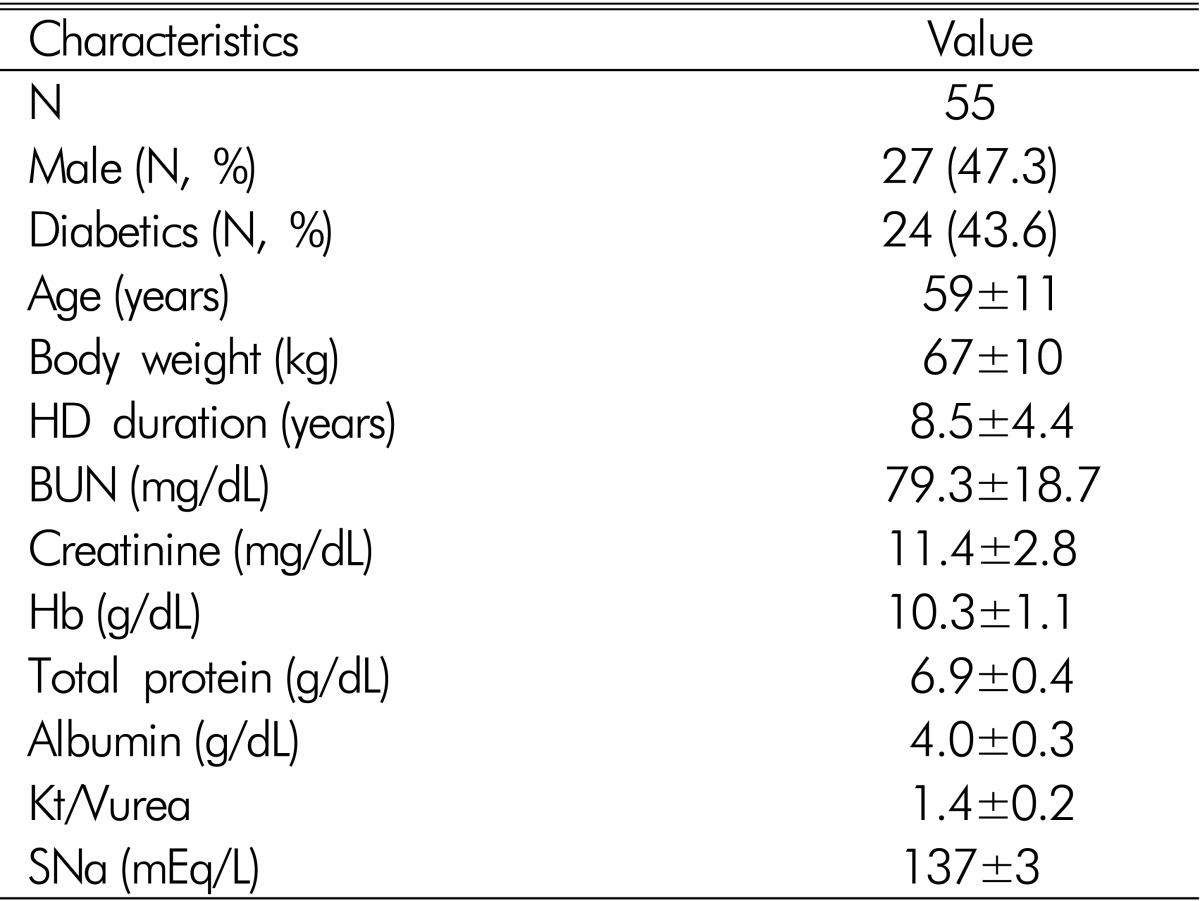
HD: hemodialysis, BUN: blood urea nitrogen, Hb: hemoglobin, SNa: serum sodium concentration
2. Analysis of sodium gradient-related data
In the 55 patients, SNa values ranged from 130 to 142 mEq/L and the mean CV of SNa was 1.5±0.5%. The numbers of patients with a SNa between l30 and 137 mEq/L, 138 and 139mEq/L, and 140 and 144mEq/L were 29 (52.7%), 19 (34.5%), and 7 (12.7%), respectively, and mean SNa, csNa and csNag were 137±3, 136±3, and 137±2mEq/L, respectively (Fig. 1A, 1B, 1C). Mean SNa was significantly higher than the mean csNa and csNag (p<0.01). On Bland-Altman plots, csNa was ~1.6 mEq/L lower than SNa (Figs. 2A and 2B), and csNag was 0.8mEq/L lower than SNa but had a wider distribu- tion than csNa.
Fig. 1.

Distribution of the mean (A) SNa, (B) csNa, and (C) csNag values of the study subjects.
SNa: serum sodium concentration, csNa: SNa corrected for void volume and the Gibbs-Donnan effect, csNag: csNa corrected for glucose concentration.
Fig. 2.

Bland-Altman plot between (A) SNa and csNa, and between (B) SNa and csNag. SNa: serum sodium concentration, csNa: SNa corrected for void volume and the Gibbs-Donnan effect, csNag: csNa corrected for glucose concentration.
The mean DNa values of 28 (50.9%), 13 (23.6%), 7 (12.7%), 6 (10.9%), and 1 (1.8%) patient were 138, 142, 136, 140, and 135mEq/L respectively, and mean SGna, SGcna, and SGcnag values were 1.5±3.3 (range -5.6~9.1, median 0.8, mode -0.3), 3.0±3.3 (range -4.0~10.4, median 2.5, mode -4.0), and 2.2±3.1 (range -4.4~10.4, median 2.0, mode -4.4)mEq/L, respectively.
Significant positive correlations were observed between DNa and SGna (r=0.60, p<0.01), SGcna (r=0.59, p<0.01), or SGcnag (r=0.58, p<0.01). In addition, significant positive correlations were noted between mean UF amounts and SGna (r=0.40, p=0.002, Fig. 3), SGcna (r=0.40, p=0.003), or SGcnag (r=0.44, p=0.001), and between mean ΔSBP and SGna (r=0.34, p=0.012, Fig. 4), SGcna (r=0.35, p=0.009), or SGcnag (r=0.31, p=0.02). On the other hand, no relationship was observed between pre-HD mean serum osmolality and SGna, SGcna or SGcnag, or between pre-HD SBP and SGna, SGcna or SGcnag. In addition, no correlation was found between DNa and mean SNa, csNa, or csNag values.
Fig. 3.

Correlation between mean SGna and mean ultrafiltration (UF) amount (r=0.40, p=0.002).
Fig. 4.

Correlation between mean SGna and mean (pre - post) SBP (r=0.34, p=0.012). ΔSBP: (pre - post) SBP.
The patients were allocated to group 1 (SGna, SGcna or SGcnag <3mEq/L) and group 2 (SGna, SGcna or SGcnag ≥3mEq/L). Using SGna or SGcnag, the number of group 2 was zero when DNa was 135 or 136mEq/L. On the other hand, group 2 patients showed from DNa 138mEq/L and percentages increased when DNa was increased to 140 and 142mEq/L (10.7, 50.0, and 69.2% in SGna, 17.9, 66.7, and 69.2% in SGcnag) (Fig. 5). Group 2 patients even showed from DNa 136mEq/L when SGcna (28.6% in 136mEq/L, 17.9% in 138mEq/L, 66.7% in 140mEq/L, and 76.9% in 142mEq/L) was used. Group 2 had significantly lower pre-HD SNa, csNa, csNag, serum osmolality levels and higher mean UF amount than group 1 for all 3 SG values (Table 2). Group 2 also contained more diabetics than group 1.
Fig. 5.

Number of patients (filled squares) of (A) SGna, (B) SGcna, and (C) SGcnag ≥3 mEq/L) among total patients (white squares) according to DNa concentration.
Table 2.
Comparison between group 1 (SG <3mEq/L) and 2 (SG ≥3mEq/L)
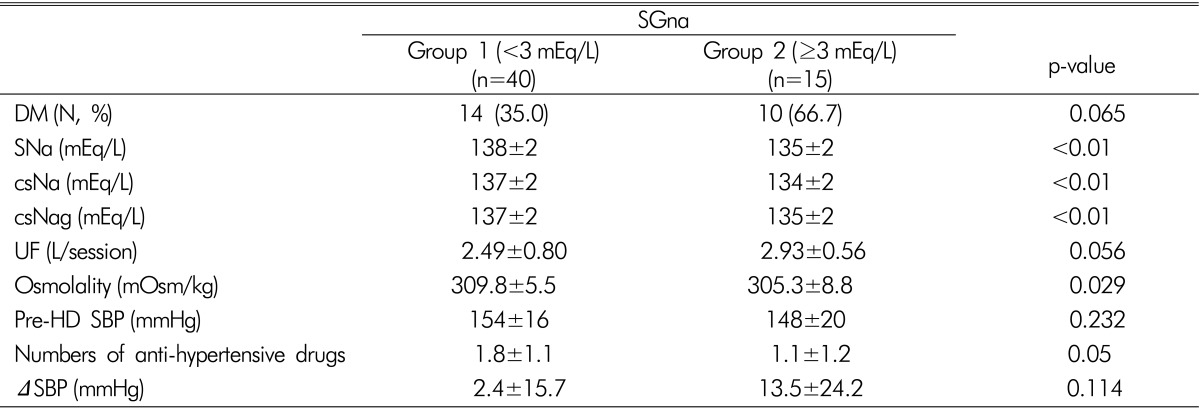
All values are 1-year means, SNa=serum Na, csNa=SNa, corrected for void volume and Gibbs-Donnan efficient, csNag=corrected for hyperglycemia, ΔSBP=(pre - post) HD SBP
3. Relationship between sodium gradient and intradialytic hypotension
During the yearlong study period, 17 patients experienced IDH; 1 episode in 7 patients, 2 in 4 patients, 3 in 4 patients, 8 in one patient, and 9 in one patient. 38 patients (69.1%) did not experience IDH. Significant correlations were found between the frequency of IDH and DNa (r=0.358, p=0.007) (Fig. 6), mean SNa (r=-0.34, p=0.011), and SGna (r=-0.34, p=0.011). Frequency of IDH increased as SG increased, regardless of SGna, SGcna, or SGcnag. Furthermore, IDH occurred even when the SG was zero.
Fig. 6.

Correlation between the frequency of intradialytic hypotension (IDH) and mean SGna (r=0.358, p=0.007).
Discussion
This study confirms the presence of a patient specific distribution of pre-HD SNa among study subjects. In addition, csNa and csNag were significantly lower than SNa, and SG was found to be positively related to DNa and the frequency of IDH. Moreover, a higher SG was associated with a larger amount of UF and a reduction in SBP during HD. In particular, patients with a SGna of more than 3mEq/L tended to have a DNa of ≥138 mEq/L and the percentages of these patients were increased as DNa was increased. On the other hand, SG did not appear to be associated with SNa or pre-HD SBP.
Several DNa have been used for HD, but the optimal concentration remains controversial. Dialysis units generally used a high DNa, because it reduces dialysis discomfort and the incidences of symptomatic hypotension and disequilibrium2). However, when a high DNa is used, the increased SG produced could result in a cumulative total body Na+ expansion, excessive thirst, increased interdialytic weight gain, and the recrudescence of hypertension in sensitive individuals5). Indeed, a high DNa has been associated with increased thirst3) and interdialytic weight gain3,4). Accordingly, our results are in line with those of previous reports. In addition, we observed positive correlations between DNa and SG, and between SG and UF amount (which reflects interdialytic weight gain). On the other hand, the correlation between SG and Pre-HD SBP was not consistent. Several studies have concluded SG and high DNa are not associated with pre-HD hypertension3,14). Similarly, in the present study, no correlation was observed between SG and pre-HD SBP. Interestingly, numbers of anti-hypertensive drugs tended to be less in patients with a SGna of >3, which might have been due in part to the adjustment of DNa according to BP status.
Dialysis patients appear to have a unique set point for SNa5), that remains stable over long-term observations6), and which is actively controlled7), and our results concur with this observation. We found SNa varied with a mean CV of 1.5±0.5% over the one year study period.
Therefore, the optimal of DNa appears to be patient and SG dependent15). Several studies have focused on sodium alignment, which effectively reduces interdialytic weight gain, anti-hypertensive drug requirements, and intradialytic morbidity9,16,17). However, the application of Na+ alignment presents several problems, such as, the feasibility of measuring SNa prior to each HD session, the need to correct for the Gibbs-Donnan effect, void volume, and hyperglycemia, the methods used to measure SNa, and the accuracy of the DNa delivered by the dialysis machine on a prescribed DNa setting9). Raimann et al. presented a straightforward means of correcting for the Gibbs-Donnan effect and void volume9), and there is a well known means of correcting SNa for hyperglycemia11,18). When we compared SNa with csNa and csNag, we found it was significantly higher than both. On the other hand, the difference between SNa and csNag was less than that of SNa and csNa. Considering that many patients visit dialysis centers after they eat a meal, it appears to be reasonable to correct SNa for void volume, the Gibbs-Donnan effect, and hyperglycemia for all patients. Therefore, csNag can be estimated by subtracting the mean difference between SNa and csNag from SNa. However, our results should be interpreted carefully and further confirmatory studies are needed.
A positive SG of ≥3mEq/L has been reported to be associated with increased hospitalization and mortality19), and thus, this value was used as a cut-off value for SG. Patients with a SGna or SGcnag of ≥3mEq/L showed from a DNa of 138mEq/L. When SGcna was used, patients with a SGna or SGcnag of ≥3mEq/L showed even from a DNa of 136mEq/L. Furthermore, IDH occurred at a SG of zero, regardless of SGna, SGcna, or SGcnag. This result was surprising because, in most patients, a DNa between 138 and 142mEq/L is considered to be the standard in current clinical practice20).
These results raise the question 'If an individualized DNa prescription cannot be fulfilled in a facility, should the fixed DNa be lowered to below 138mEq/L?' This is a hot topic in the hemodialysis field. Some specialists have recommended the use of a fixed DNa of ~137 mEq/L21), whereas others have suggested it is reasonable to prescribe a DNa between 138 and 142mEq/L in most patients20). However, they also recommended that it is important to consider whether a given patient is within a specific clinical subset, in which there is clear evidence that a positive Na balance may benefit from the manipulation of DNa20). Another group even recommended reducing the DNa to 134-138mEq/L22). Kim et al. reported that when DNa was lower than the pre-HD SNa, pre-HD SBP and interdialytic weight gain were reduced23). On the other hand, recent studies failed to show a decrease in mortality risk in those exposed to a lower DNa at any SNa level24). An association between a low DNa and increased mortality has also been reported25,26). However, due to the retrospective, observational nature of our study, it is not possible to suggest an optimal DNa.
This study had several limitations. First, active Na+ concentration was not measured by direct potentiometry. On the other hand, SNa is usually measured by indirect potentiometry in clinical practice. Second, the simple equation proposed by Gotch et al.27) was used to correct for void volume and the Gibbs-Donnan effect, but this equation does not consider the lipid concentrations as part of the void volume. Third, this retrospective study was conducted on a small number of subjects at a single HD center. Fourth, we used prescribed DNa and DNa values were not measured directly, although we should add that HD machines were calibrated monthly.
In summary, a high SG appeared to be developed by a considerable number of patients. This appears to be because HD patients show various distributions of pre-HD SNa and SG seems to be positively related to prescribed DNa. Furthermore, SG appears to be related to UF amount, ΔSBP, and frequency of IDH. However, additional studies are needed to confirm these relations.
Footnotes
The authors have no potential conflicts of interests to declare.
This study was the subject of an oral presentation at the 34th Annual Spring meeting of Korean Society of Nephrology.
References
- 1.Santos SFF, Peixoto AJ. Sodium balance in maintenance hemodialysis. Semin Dial. 2010;23:549–555. doi: 10.1111/j.1525-139X.2010.00794.x. [DOI] [PubMed] [Google Scholar]
- 2.Flanigan MJ. Sodium Flux and Dialysate Sodium in Hemodialysis. Semin Dial. 2007;11:298–304. [Google Scholar]
- 3.Munoz Mendoza J, Sun S, Chertow GM, Moran J, Doss S, Schiller B. Dialysate sodium and sodium gradient in maintenance hemodialysis: a neglected sodium restriction approach? Nephrol Dial Transplant. 2011;26:1281–1287. doi: 10.1093/ndt/gfq807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hecking M, Kainz A, Hörl WH, Herkner H, Sunder-Plassmann G. Sodium setpoint and sodium gradient: influence on plasma sodium change and weight gain. Am J Nephrol. 2011;33:39–48. doi: 10.1159/000322572. [DOI] [PubMed] [Google Scholar]
- 5.Petitclerc T, Jacobs C. Dialysis sodium concentration: what is optimal and can it be individualized? Nephrol Dial Transplant. 1995;10:596–599. [PubMed] [Google Scholar]
- 6.Keen ML, Gotch FA. The association of the sodium "setpoint" to interdialytic weight gain and blood pressure in hemodialysis patients. Int J Artif Organs. 2007;30:971–979. doi: 10.1177/039139880703001105. [DOI] [PubMed] [Google Scholar]
- 7.Peixoto AJ, Gowda N, Parikh CR, Santos SFF. Long-term stability of serum sodium inhemodialysis patients. Blood Purif. 2010;29:264–267. doi: 10.1159/000274460. [DOI] [PubMed] [Google Scholar]
- 8.Lomonte C, Basile C. Do not forget to individualize dialysate sodium prescription. Nephrol Dial Transplant. 2011;26:1126–1128. doi: 10.1093/ndt/gfr073. [DOI] [PubMed] [Google Scholar]
- 9.Raimann JG, Thijssen S, Usvyat LA, Levin NW, Kotanko P. Sodium alignment in clinical practice-implementation and implications. Semin Dial. 2001;24:587–592. doi: 10.1111/j.1525-139X.2011.00973.x. [DOI] [PubMed] [Google Scholar]
- 10.Daugirdas JT. Second generation logarithmic estimates of single-pool variable volume Kt/V: an analysis of error. J Am Soc Nephrol. 1993;4:1205–1213. doi: 10.1681/ASN.V451205. [DOI] [PubMed] [Google Scholar]
- 11.Katz MA. Hyperglycemia-induced hyponatremia-calculation of expected serum sodium depression. N Engl J Med. 1973;289:843–844. doi: 10.1056/NEJM197310182891607. [DOI] [PubMed] [Google Scholar]
- 12.Rasouli M, Kalantari KR. Comparison of methods for calculating serum osmolality: multivariate linear regression analysis. Clin Chem Lab Med. 2005;43:635–640. doi: 10.1515/CCLM.2005.109. [DOI] [PubMed] [Google Scholar]
- 13.Chesterton LJ, Selby NM, Burton JO, Fialova J, Chan C, McIntyre CW. Categorization of the hemodynamic response to hemodialysis: the importance of baroreflex sensitivity. HemodialInt. 2010;14:18–28. doi: 10.1111/j.1542-4758.2009.00403.x. [DOI] [PubMed] [Google Scholar]
- 14.Hecking M, Karaboyas A, Rayner H, et al. Dialysate Sodium Prescription and Blood Pressure in Hemodialysis Patients. Am J Hypertens. 2014;27:1160–1169. doi: 10.1093/ajh/hpu040. [DOI] [PubMed] [Google Scholar]
- 15.Levin NW, Zhu F, Keen M. Interdialytic weight gain and dry weight. Blood Purif. 2001;19:217–221. doi: 10.1159/000046944. [DOI] [PubMed] [Google Scholar]
- 16.Murisasco A, France G, Leblond G, et al. Sequential sodium therapy allows correction of sodium-volume balance and reduces morbidity. Clin Nephrol. 1985;24:201–208. [PubMed] [Google Scholar]
- 17.De Paula FM, Peixoto AJ, Pinto LV, Dorigo D, Patricio PJM, Santos SFF. Clinical consequences of an individualized dialysate sodium prescription in hemodialysis patients. Kidney Int. 2004;66:1232–1238. doi: 10.1111/j.1523-1755.2004.00876.x. [DOI] [PubMed] [Google Scholar]
- 18.Penne EL, Thijssen S, Raimann JG, Levin NW, Kotanko P. Correction of serum sodium for glucose concentration in hemodialysis patients with poor glucose control. Diabetes Care. 2010;33:e91. doi: 10.2337/dc10-0557. [DOI] [PubMed] [Google Scholar]
- 19.Penne EL, Sergeyeva O. Sodium Gradient: A Tool to Individualize Dialysate Sodium Prescription in Chronic Hemodialysis Patients? Blood Purif. 2011;31:86–91. doi: 10.1159/000321851. [DOI] [PubMed] [Google Scholar]
- 20.Marshall MR, Dunlop JL. Are dialysate sodium levels too high? Semin Dial. 2012;25:277–283. doi: 10.1111/j.1525-139X.2012.01072.x. [DOI] [PubMed] [Google Scholar]
- 21.Gembala M, Kumar S. In: Sodium and Hemodialysis. In: Progress in Hemodialysis - From Emer- gent Biotechnology to Clinical Practice [Internet] Carpi A, editor. InTech; 2011. [cited 2014 Jun 8]. Available from: http://www.intechopen.com/books/progress-in-hemodialysis-from-emergent-biotechnology-to-clinical-practice/sodium-and-hemodialysis. [Google Scholar]
- 22.Parker T., 3rd Creating an open dialogue on improving dialysis care. Nephrol News Issues. 2013;27:14–16. [PubMed] [Google Scholar]
- 23.Kim SM, Kim JG, Shin JH, et al. The effects of low sodium dialysate in hemodialysis patients. Korean J Nephrol. 2011;30:53–60. [Google Scholar]
- 24.Hecking M, Karaboyas A, Saran R, et al. Predialysis serum sodium level, dialysate sodium, and mortality in maintenance hemodialysis patients: the Dialysis Outcomes and Practice Patterns Study (DOPPS) Am J Kidney Dis. 2012;59:238–248. doi: 10.1053/j.ajkd.2011.07.013. [DOI] [PubMed] [Google Scholar]
- 25.Hecking M, Karaboyas A, Saran R, et al. Dialysate sodium concentration and the association with interdialytic weight gain, hospitalization, and mortality. Clin J Am SocNephrol. 2012;7:92–100. doi: 10.2215/CJN.05440611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mc Causland FR, Brunelli SM, Waikar SS. Dialysate sodium, serum sodium and mortality in maintenance hemodialysis. Nephrol Dial Transplant. 2012;27:1613–1618. doi: 10.1093/ndt/gfr497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gotch FA, Lam MA, Prowitt M, Keen M. Preliminary clinical results with sodium-volume modeling of hemodialysis therapy. Proc Clin Dial Transplant Forum. 1980;10:12–17. [PubMed] [Google Scholar]