

Abstract
Papillary thyroid carcinoma is well known for its low malignant potential and good prognosis. The outcome can be fatal in patients with low compliance and delayed treatment. Recent advances in ultrasonographic screening and US guided fine needle aspiration biopsy has facilitated early diagnosis of papillary thyroid carcinomas. This epithelial thyroid tumour accounts for more than 80 % of all thyroid tumours. An occult primary carcinoma of thyroid presenting as lymphangioma has been reported rarely. We present a case of a 40-year-old female patient with huge cystic midline swelling on the right side of the neck mimicking lymphangioma on USG. MRI neck showed a cystic mass causing displacement of the trachea and arising from Rt lobe of thyroid gland. Hemithyroidectomy was carried out and histopathology revealed papillary carcinoma. In patients with neck swellings presenting as huge cystic mass the differential diagnosis of Intra cystic variant of papillary carcinoma thyroid and metastatic thyroid papillary carcinoma must always be considered prior to planning surgery.
Keywords: Occult, Papillary thyroid carcinoma, Lymphangioma
Introduction
The most common thyroid malignancy is papillary thyroid carcinoma (80 % of all types of thyroid cancers) [1]. It usually presents as a solitary thyroid nodule. A malignant thyroid cyst is rare (<2 %) [2].
Cystic neck masses appearing in the anterior or posterior triangles of the neck are usually benign. But they can sometimes be malignant and so should be kept in the differential diagnosis and appropriately investigated [3]. Papillary thyroid carcinoma, uncommonly, presents as a solitary cervical cystic mass.
We report a case of papillary thyroid carcinoma with an unusual presentation as a loculated true cystic swelling in neck extending till the mastoid. The case was diagnosed after surgery by histopathological examination.
Case Report
A 40-year-old female patient presented with swelling in the midline of the neck (Fig. 1) since 1 year. Initially it was of the size of about a peanut, and gradually increased to the size of a lemon in 6 months and then rapidly increased to the present size (10 × 12 cm). It was going to right side and the back of the neck.
Fig. 1.

Pre Operative Clinical Photograph showing trilobed swelling extending from midine to posterior triangle on the right side of the neck
On examination there was a trilobed swelling with well defined margins extending from midline to posterior triangle on the right side of the neck. The skin over the swelling was normal and not adherent to the swelling with no dilatation of the veins. The swelling was moving on deglutition, fluctuant and cystic on palpation and was showing trans-illumination.
Cervical lymph nodes were not enlarged. On indirect laryngoscopy, no abnormality was detected. Thyroid profile was within normal limits. Fine needle aspiration cytology (FNAC) of the swelling showed features, suggestive of lymphangioma. Ultrasound of the neck showed left lobe of thyroid, measuring 1.2 × 3.9 × 1.3 cm with small hypoechoic nodule of the size 2 mm. Right lobe of thyroid appears compressed by large cystic lesion with a solid component of approximately 2.9 × 2.2 cm within it. Lesion could not be visualized separately from the thyroid gland or could be a arising from the gland or a lymphangioma, requiring further investigation.
MRI study revealed a huge well capsulated, macro lobulated homogenous cystic signal intensity mass lesion of the size 11.3 × 10.2 × 7.6 cm (AP × T × CC) in the right side of neck, bulging into subcutaneous plane and medially extending up to right paratracheal region. Polypoidal soft tissue component was noted along the medial wall of cyst which seemed to be arising to be arising from right lobe of thyroid gland. Mass effect was noted in the form of tracheal deviation and mild posterior displacement of carotid vessels and no obvious direct infiltration into adjacent structures (Fig. 2).
Fig. 2.

MRI neck showing lobulated homogenous cystic mass arising from right lobe of Thyroid with deviation of Trachea to the left
Right hemi-thyroidectomy along with excision of cystic mass was done (Fig. 3) under general anaesthesia, with preservation of right recurrent laryngeal nerve (Fig. 4). Postoperative period was uneventful. On histopathological examination of specimen papillary carcinoma of thyroid was found with cystic degeneration.
Fig. 3.

Intraoperative picture showing huge cystic lesion in the right side of the neck
Fig. 4.
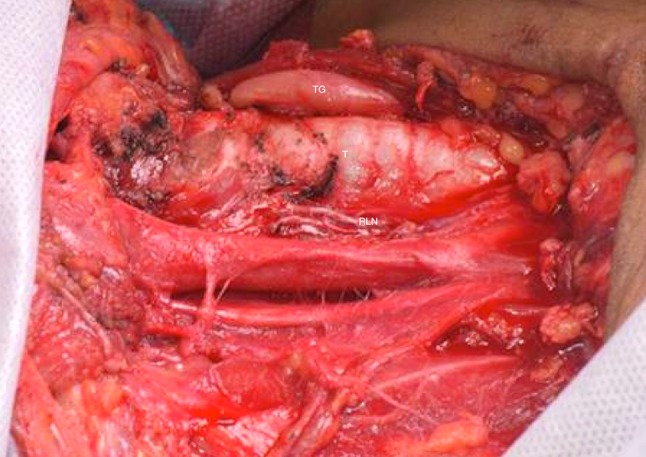
Intraoperative Picture after Excision of cystic mass and Hemithyroidectomy showing Trachea (T), Recurrent Laryngeal Nerve (RLN), left Thyroid Gland (TG)
Discussion
The various common cysts in the neck include the epidermoid, branchial and dermoid cysts, teratomas, lymphangiomas, and cystic hygromas. Cystic masses of the neck can also be lymph node metastases from and head and neck tumors [4]. Thyroid cysts are common but thyroid cancers presenting itself as a cystic mass may be due to metastasis to the cervical lymph nodes or as a primary true cystic mass without palpable lesion in the thyroid gland [5].
Papillary thyroid carcinoma is a slowly growing tumour and so easily misdiagnosed as benign cysts specially in young patients [7]. Papillary thyroid carcinoma can have local spread to recurrent laryngeal nerve, larynx, trachea, and esophagus in 4–16 % of cases responsible for the disease recurrence and death [8].
Ultrasonography is commonly used to diagnose the thyroid swellings. A solid, hypoechogenicity, absence of a hypoechoic halo, presence of microcalcifications, irregular margins, and intranodular vascularity are features of a malignant nodule in thyroid [9]. According to a study by Jun et al. [10], only 5 % of all papillary thyroid carcinomas were purely cystic, 69 % had marked intrinsic hypervascularity and 22 % had perinodal vascularity. Chan et al. [11] reported that all predominantly cystic papillary thyroid carcinomas in their study showed blood flow in the central part of the tumor that was greater than that of the surrounding parenchyma.
Initial presentation of papillary thyroid carcinoma, in approximately 50 % of patients, is with cervical lymph node metastases [12]. Although in our case there were no palpable lymph nodes. In up to 20 % of all patients, lymph node metastases may even be the sole or initial manifestation of disease (occult primary tumor) [13]. Approximately 40 % (reported range, 21–50 %) of all lymph node metastases from papillary thyroid carcinomas have the tendency to completely cavitate a lymph node by cystic degeneration and thus may mimic an apparently benign cervical cyst [14]. In case of doubt an MRI should be done to assist in the diagnosis [15].
Universally all thyroid nodules detected on USG are further investigated by FNAC [9]. Thyroid cysts without microcalcifications suggest a lower likelihood of malignancy. FNAC is less sensitive in the diagnosis of cystic neck masses compared with solid masses having a false negative rate ranging from 50 to 67 % [16]. In a study by Muller et al. [17], FNAC had false negative rate of 45 % in diagnosing cystic papillary thyroid carcinoma. This high level of false negativity is due to sampling error and not cytological misdiagnosis. Ultrasound guided FNAC that can obtain material from the wall and solid part of the cyst increases the accuracy of FNAC [18].
Excisional biopsy is essential to detect papillary thyroid carcinoma in patients with negative FNAC. If clinical or radiological suspicion of malignancy is present, frozen section analysis of the specimen may help to proceed for a total thyroidectomy with modified radical neck dissection at the same setting. Histologically, the microscopic examination shows a fibrous cyst wall with papillary structures on inner surface, composed of a fibrovascular core line by overcrowded cell. Cells shows orphan eye looking nuclei. There is presence of psammoma bodies with scanty colloid [15].
To reduce the recurrences it is advocated to give post-operative radio-iodine with suppressive thyroxine dose and estimate the serum thyroglobulin for early detection of recurrence or metastasis. Papillary thyroid carcinoma carries an excellent prognosis >90 % survival with a poorer 30–60 % 20 year survival in presence of extra-thyroid extension [8].
Conclusion
Papillary thyroid carcinoma is the commonest of thyroid malignancies presenting with solitary thyroid nodule or as lymph node mass, although unusual presentation like solitary cystic nodal mass or multiple cystic mass in neck must be considered. Ultrasonography and MRI can help in diagnosing the origin of the cystic lesion of neck. FNAC is not very accurate in diagnosis of cystic lesions originating from the thyroid. Total thyroidectomy with cyst excision and radical neck node dissection provides good prognosis.
Conflict of interest
None.
Financial support
None.
References
- 1.Scott A, Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A national cancer data base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995. Cancer. 1998;83(12):2638–22948. doi: 10.1002/(SICI)1097-0142(19981215)83:12<2638::AID-CNCR31>3.0.CO;2-1. [DOI] [PubMed] [Google Scholar]
- 2.Benito HI, Sánchez RA, Rodríguez PM, et al. Simple thyroid cyst. Rev Esp Med Nucl. 2001;20(1):32–35. [PubMed] [Google Scholar]
- 3.Seven H, Gurkan A, Cinar U, Vural C, Turgut S. Incidence of occult thyroid carcinoma metastases in lateral cervical cysts. Am J Otolaryngol. 2004;25(1):11–17. doi: 10.1016/j.amjoto.2003.10.002. [DOI] [PubMed] [Google Scholar]
- 4.Nakagawa T, Takashima T, Tomiyama K. Differential diagnosis of a lateral cervical cyst and solitary cystic lymph node metastasis of occult thyroid papillary carcinoma. J Laryngol Otol. 2001;115(3):240–242. doi: 10.1258/0022215011907109. [DOI] [PubMed] [Google Scholar]
- 5.Attie JN, Setzin M, Klein I. Thyroid carcinoma presenting as an enlarged cervical lymph node. Am J Surg. 1993;166(4):428–430. doi: 10.1016/S0002-9610(05)80348-4. [DOI] [PubMed] [Google Scholar]
- 6.Loughran CF. Case report: cystic lymph node metastasis from occult thyroid carcinoma: a sonographic mimic of a branchial cleft cyst. Clin Radiol. 1991;43(3):213–214. doi: 10.1016/S0009-9260(05)80483-0. [DOI] [PubMed] [Google Scholar]
- 7.Monchik JM, De Petris G, De Crea C. Occult papillary carcinoma of the thyroid presenting as a cervical cyst. Surgery. 2001;129(4):429–432. doi: 10.1067/msy.2001.112965. [DOI] [PubMed] [Google Scholar]
- 8.Andersen PE, Kinsella J, Loree TR, Shaha AR, Shah JP. Differentiated carcinoma of the thyroid with extrathyroidal extension. Am J Surg. 1995;170(5):467–470. doi: 10.1016/S0002-9610(99)80331-6. [DOI] [PubMed] [Google Scholar]
- 9.Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: society of radiologists in ultrasound consensus conference statement. Ultrasound Q. 2006;22(4):231–238. doi: 10.1097/01.ruq.0000226877.19937.a1. [DOI] [PubMed] [Google Scholar]
- 10.Jun P, Chow LC, Jeffrey RB. The sonographic features of papillary thyroid carcinomas: pictorial essay. Ultrasound Q. 2005;21(1):39–45. [PubMed] [Google Scholar]
- 11.Chan BK, Desser TS, McDougall IR, Weigel RJ, Jeffrey RB., Jr Common and uncommon sonographic features of papillary thyroid carcinoma. J Ultrasound Med. 2003;22(10):1083–1090. doi: 10.7863/jum.2003.22.10.1083. [DOI] [PubMed] [Google Scholar]
- 12.Hoang JK, Lee WK, Lee M, Johnson D, Farrell S. US features of thyroid malignancy: pearls and pitfalls. Radiographics. 2007;27(3):847–860. doi: 10.1148/rg.273065038. [DOI] [PubMed] [Google Scholar]
- 13.Al-Brahim N, Asa SL. Papillary thyroid carcinoma: an overview. Arch Pathol Lab Med. 2006;130(7):1057–1062. doi: 10.5858/2006-130-1057-PTCAO. [DOI] [PubMed] [Google Scholar]
- 14.Tae HJ, Lim DJ, Baek KH, et al. Diagnostic value of ultrasonography to distinguish between benign and malignant lesions in the management of thyroid nodules. Thyroid. 2007;17(5):461–466. doi: 10.1089/thy.2006.0337. [DOI] [PubMed] [Google Scholar]
- 15.Beahrs O, Kiernan P, Hubert JJ. Cancer of the thyroid gland. In: Suen J, Myers E, editors. Cancer of the head and neck. New York: Churchill Livingstone; 1981. pp. 599–632. [Google Scholar]
- 16.Chi HS, Wang LF, Chiang FY, Kuo WR, Lee KW. Branchial cleft cyst as the initial impression of a metastatic thyroid papillary carcinoma: two case reports. Kaohsiung J Med Sci. 2007;23(12):634–638. doi: 10.1016/S1607-551X(08)70063-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Muller N, Cooperberg PL, Suen KCH, Thorson SC. Needle aspiration biopsy in cystic papillary carcinoma of the thyroid. Am J Roentgenol. 1985;144(2):251–253. doi: 10.2214/ajr.144.2.251. [DOI] [PubMed] [Google Scholar]
- 18.Cooper DS, Doherty GM, Haugen BR, et al. Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–1214. doi: 10.1089/thy.2009.0110. [DOI] [PubMed] [Google Scholar]