

Triphasic CT scan of abdomen showed diffuse, large heterogeneous area involving left lobe and anterior segments of right lobe of liver with multiple similar character lesions in posterior segment with centripetal filling suggestive of liver hemangiomatosis (Figure 1A, B and C). The giant hemangioma was seen causing mass effect in form of compression of right hepatic vein and non-visualization of middle and left hepatic veins with chinking of intrahepatic inferior vena cava consistent with Budd-Chiari syndrome (Figure 1B). The diagnosis was confirmed with magnetic resonance imaging and venography (2D). Free fluid was also present in the abdomen. Patient improved on conservative measures (salt restriction and diuretics) and after 6 months had total disappearance of ascites.
Figure 1.
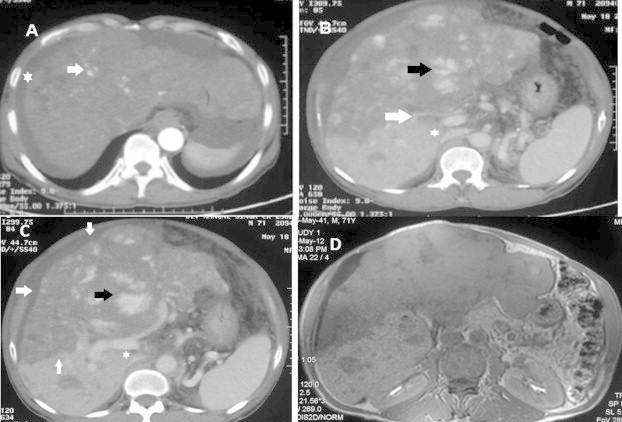
Nodular peripheral enhancement of the lesions in arterial phase (A) with centripetal filling in the venous phase (B) which are isodense in delayed phase with one lesion showing centripetal enhancement in delayed phase (C) (arrows). There is chinking of IVC in venous phase with non-visualisation of hepatic veins (B). MRI image confirming the findings (D).
Liver hemangiomas are common incidental finding reflecting a high overall prevalence in the population. Approximately 80% of hemangiomas are of the cavernous type. These can, occasionally, grow to reach large size and may become symptomatic.1 Giant hemangiomas are defined as those measuring 5 cm or more in diameter. These may cause symptoms, including abdominal pain and right upper quadrant fullness. Acute pain may also occur if thrombosis or hemorrhage occurs within the hemangioma. The majority of hepatic hemangiomas remain stable over time though few studies have described significant growth, with occurrence of symptoms requiring surgical resection of lesions.1 Weimann et al reported size increase in 11 (10.6%) of 103 patients with liver hemangiomas over a median follow up of 32 months.2 Hemangiomatosis of the liver, with multiple hemangiomas scattered in the hepatic parenchyma, is uncommon in adulthood and has been reported only occasionally.3
Secondary Budd-Chiari syndrome is an uncommon clinical disorder characterized by hepatic venous outflow obstruction due to compression or invasion by a lesion originating outside the hepatic veins. There are only two previous reports of hepatic hemangioma causing Budd-Chiari syndrome. In one of the earlier reports, a 52-year old male was incidentally found to have hepatic hemangioma with cystic degeneration, causing symptoms of Budd-Chiari syndrome, which improved with cyst excision.4 In another report, a 45-year old woman symptomatic with pain in right hypochondrium had a giant hepatic hemangioma compressing the retrohepatic vena cava which improved with hepatic segmentectomy.5 Our patient had a giant hemangioma completely replacing the left lobe of liver and parts of right lobe with multiple other small hemangiomas consistent with hepatic hemangiomatosis causing compression of hepatic veins and the intrahepatic inferior vena cava resulting in Budd-Chiari syndrome. Although the therapeutic strategy for hemangiomas is usually non-operative, symptomatic lesions need operative intervention in form of hepatic resection or enucleation of hemangiomas. Surgical intervention was not considered in our patient because of the diffuse involvement of liver with multiple lesions. Our patient improved with conservative measures and remains asymptomatic on follow-up.
Conflicts of interest
All authors have none to declare.
References
- 1.Gedaly R., Pomposelli J.J., Pomfret E.A., Lewis W.D., Jenkins R.L. Cavernous hemangioma of the liver: anatomic resection vs. enucleation. Arch Surg. 1999;134:407–411. doi: 10.1001/archsurg.134.4.407. [DOI] [PubMed] [Google Scholar]
- 2.Weimann A., Ringe B., Klempnauer J. Benign liver tumors: differential diagnosis and indications for surgery. World J Surg. 1997;21:983–990. doi: 10.1007/s002689900337. [DOI] [PubMed] [Google Scholar]
- 3.Moon W.S., Yu H.C., Lee J.M., Kang M.J. Diffuse hepatic hemangiomatosis in an adult. J Korean Med Sci. 2000;15:471–474. doi: 10.3346/jkms.2000.15.4.471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hanazaki K., Koide N., Kajikawa S. Cavernous hemangioma of the liver with giant cyst formation: degeneration by apoptosis? J Gastroenterol Hepatol. 2001;16:352–355. doi: 10.1046/j.1440-1746.2001.02344.x. [DOI] [PubMed] [Google Scholar]
- 5.Kim D.Y., Pantelic M.V., Yoshida A., Jerius J., Abouljoud M.S. Cavernous hemangioma presenting as Budd-Chiari Syndrome. J Am Coll Surg. 2005;3:470–471. doi: 10.1016/j.jamcollsurg.2004.07.037. [DOI] [PubMed] [Google Scholar]