

Abstract
A young house wife presented with low grade fever, cough, haemoptysis and SOB of unknown aetiology for 40 days duration. Respiratory system examination revealed diffuse crepts and rhonchi. Other organ system examination did not reveal any abnormality. X-ray chest PA view and CT thorax showed diffuse bilateral necrotising nodular lesions of various sizes with small pleural effusion. She also had low resting oxygen saturation with falling haematocrit. Her Serum was week positive for p-ANCA and negative for MPO-ANCA. Bronchoscopy revealed continuous bloody aspirates. We could not isolate any organisms in any of the specimens from her and she was unresponsive to any of the antibiotics either. Based on the clinical, laboratory data, radiological features and positive outcome to pulse therapy of methylprednisolone and cyclophosphamide, she was diagnosed as a case of IPIPC.
Keywords: Isolated pauci-immune pulmonary capillaritis, hemoptysis, vasculitis
INTRODUCTION
Isolated pauci-immune pulmonary capillaritis (IPIPC) is a rare disorder of unknown etiology. It is characterized by small vessel vasculitis confined to lungs, and systemic manifestations are typically absent. It is considered as a subset of microscopic polyangiitis (MPA) but is mostly sero-negative for anti-neutrophilic cytoplasmic antibodies (ANCA).[1] First described by Nierman et al.[2] in the year 1995, the disorder was fully characterized by Jenning et al.[3] Since then only sporadic case reports of the disorder are available in the English literature.[4] We are reporting such a case which, to the best of our knowledge and belief, is the first case report of the disorder in Indian medical literature.
CASE REPORT
RD, a 28-year-old housewife from Narnaul, Haryana, was referred to the outpatient Department of Respiratory Medicine on 23.08.2013 with low grade fever, cough, hemoptysis and shortness of breath (SOB) for about 40 days duration. Other than this, she did not have any systemic symptoms. She had never smoked or consumed alcohol. Her bladder and bowel habits were regular and she had a normal appetite. She did not reveal any significant illness in the past. She was a multi-para with normal vaginal deliveries, last being 11 years back.
Prior to this, she reported to a private practitioner with sudden onset of intermittent fever, cough and SOB for which she was put on oral amoxiclav along with symptomatic treatment but after a bout of severe hemoptysis, she was rushed to a general hospital on 18.07.2013 where she was investigated. Her laboratory reports are shown in Table 1. Her X-rays [Figure 1a and b], contrast enhanced computerized tomography (CECT) and high-resolution computerized tomography (HRCT) thorax [Figure 2a and b] revealed diffuse bilateral cavitating nodular lesions and consolidation in right lower lobe along with small pleural effusion but without any remarkable changes in the mediastinal lymph nodes or the vasculature. Echocardiography revealed trivial tricuspid regurgitation without any clot or vegetation, normal pericardium and an ejection fraction of 60%. She was kept on intravenous (IV) meropenem and levofloxacin along with other symptomatic treatment but the patient continued to deteriorate and she was referred to this hospital.
Table 1.
Laboratory investigations before admission
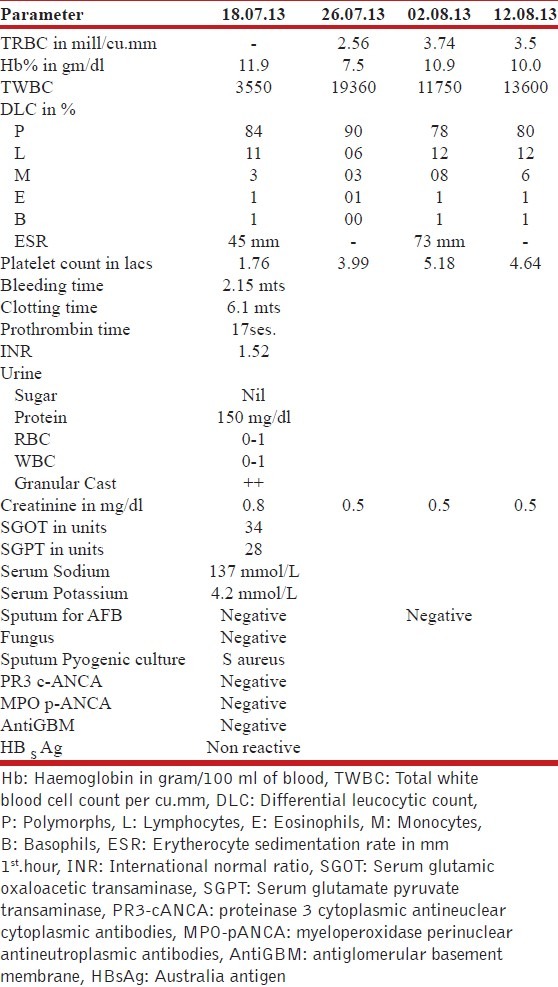
Figure 1.

(a) X-ray chest PA view dated 18.07.2013 showing diffuse bilateral necrotizing nodular lesions, more on right than left and heterogeneous opacity in right lower lobe (b) X-ray chest PA view dated 24.07.2013 showing appearance of new nodular shadows in right upper and mid zones and in left lower zone
Figure 2.

(a) CT thorax dated 24.07.2013 showing diffuse necrotizing nodular lesions (b) Topogram dated 24.07.2013 showing bilateral diffuse thick-walled necrotizing nodular lesions with consolidation and small right sided pleural effusion
She was an average built, poorly nourished female having pale and toxic look. Her body temperature was 98°F, pulse; 160/minute, blood pressure; 90/60 mm of Hg and respiratory rate; 30/minute. Respiratory system examination revealed decreased breath sounds in the right mid and lower chest along with diffuse crepitations and occasional rhonchi. Ear, nose, throat and eye checkup did not reveal any abnormality as was the examination of other organ systems. A repeat X-ray chest PA view and CT thorax on admission were remarkably similar to her earlier X-rays and CT thorax [Figures 1a and b and 2a and b]. Total leucocyte count (TLC) was 11,370/mm3 with polymorphs; 90%, Lymphocytes; 7%, Eosinophils; 1%, Monocytes; 1% and Basophils; 1%. Platelet count was 2.48 lacs/cmm but hemoglobin (Hb) was low i.e. 9.1 gm%. Her sputum samples were negative for pyogenic organisms, acid fast bacilli or fungi. Considering necrotizing pneumonia, she was continued on antibiotics and symptomatic treatment. The patient was also given 2 units of fresh blood during the hospital stay and oxygen by face mask, but she continued to have cough, hemoptysis and weight loss. Repeat hemogram was unremarkable except that hemoglobin (Hb) was further lowered to 7.1 gm%. Blood culture was sterile. Mantoux skin test was non-reactive. Ultrasound abdomen revealed nothing abnormal. A repeat serology was negative for angiotensin-converting enzyme (ACE), anti-nuclear antibodies (ANA), rheumatoid factor (RF), cytoplasmic antineutrophilic cytoplasmic antibodies (C-ANCA), antiglomerular basement membrane (Anti-GBM) antibodies and anti-aspergillous antibodies but positive for C-reactive proteins (CRP) and weekly positive for perinuclear antineutrophilic cytoplasmic antibodies (P-ANCA) by indirect immune-fluorescence assay (IIFA). Bronchoscopy revealed normal architecture of the airways on either side, but active bleeding was seen from the right lower lobe bronchus. An attempt was made to stop bleeding by instilling frequent aliquots of adrenaline mixed with cold saline but hemostasis could not be achieved so the plan for obtaining lung tissue by transbronchial route was shelved.
A provisional diagnosis of IPIPC was made on the basis of the overall clinical, radiological and laboratory findings. The patient was started on pulse therapy with methylprednisolone (1 g IV for 3 days) along with cyclophosphamide (15 mg per kg body weight IV on day 1). On this, the patient improved and was discharged on iron therapy with the advice to report for repeat pulse therapies every fortnightly. In due course, cough and SOB declined, hemoptysis stopped, Hb levels increased to 11.5 g% and X-ray chest PA view showed remarkable clearance [Figure 3]. Patient is still under follow up and is asymptomatic by the end of the 6th cycle.
Figure 3.

X-ray chest PA view dated 28.10.13 showing resolution of lesions as compared to Figure 1b
DISCUSSION
Brow[1] suggested that falling hematocrit with or without hemoptysis, unexplained bilateral diffuse alveolar infiltrates in X-ray chest and persistently bloody return in serially aspirated bronchoalveolar lavage (BAL) favored the diagnosis of DAH. Later, Cordier et al.[5] opined that infections, hematological disorders, hemolysis or hemorrhage elsewhere should be ruled out prior to make the diagnosis of DAH.
Based on the presence or absence of systemic symptoms, DAH has been classified into two broad groups, one with systemic manifestations of vasculitis and the other without it. The latter is further classified as (a) Anti-GBM disease in limited pulmonary form (positive anti-GBM antibody with linear deposits in the lung tissue), (b) pulmonary-limited MPA (positive for p-ANCA and MPO-ANCA), (c) isolated pauci-immune pulmonary capillaritis (ANCA negative neutrophilic pulmonary capillaritis) and (d) idiopathic pulmonary hemosiderosis (Acute, sub-acute or chronic bland DAH in the absence vasculitis in young smokers).[6]
Only few case reports of IPIPC with varied presentations are available in the medical literature. Nierman et al.[2] described IPIPC in a 49-year-old female patient for the first time. She presented with acute fever, type 1 respiratory failure and bilateral pulmonary infiltrates. Her thoracoscopic lung biopsy showed capillary destruction and neutrophilic infiltration of the lung interstitium/air spaces but direct evidence for DAH was lacking in this case. She was ANCA negative but circulating primed neutrophils were seen in her blood. Jennings et al.[3] in the year 1997, reviewed 29 patients with DAH and biopsy-proven pulmonary capillaritis. Eight (28%) of them were diagnosed as IPIPC. The median age was 30 years. All had symptoms related to of lower respiratory tract, six of them also having acute respiratory failure and 4 of them needed mechanical ventilation. Associated upper respiratory tract involvement was seen in 7. All were ANCA negative but direct immune-fluorescence assay (IFA) of lung tissue was positive in 3. Monteiro et al.[4] reported a case of IPIPC in a 27-year-old female. This patient used to consume cocaine and presented with hemoptysis and progressive dyspnea of short duration. Serum tests for infectious diseases, collagen disorders and vasculitis were negative and urine examination was normal. Diffuse alveolar infiltrate were seen in her CT thorax. A thoracoscopic lung biopsy showed capillaritis and diffuse intra-alveolar hemorrhage.
Our patient presented with hemoptysis, cough, shortness of breath and low grade fever for about 40 days duration. Other than this, she was devoid of any systemic illness. She never smoked or consumed alcohol and did not have a significant illness in the past. She was not exposed to any occupational hazard or drugs in her lifetime. She had a pale and toxic look. Respiratory system examination on auscultation revealed diffuse crepitations and occasional rhonchi but other system examination revealed nothing abnormal. Her serial complete blood tests revealed persistent leukocytosis and falling hematocrit. Urine examination revealed nothing abnormal. Her X-ray chest PA view and HRCT thorax showed diffuse bilateral cavitating nodular lesions of varying sizes and patchy consolidation. Her ultrasound abdomen and echocardiography were unremarkable. Sputum examination was negative for infections. Meanwhile, she was continued on antibiotics but she did not respond and showed clinical and radiological deterioration. Bronchoscopy showed active bleeding but was normal otherwise. Transbronchial lung biopsy could not be undertaken due to continued bleeding in spite of repeated installation of adrenaline mixed saline. Her serology was negative for ANA, RF, c-ANCA, Anti GBM, MPO-ANCA and anti-aspergillous antibodies but was positive for C-reactive proteins and weekly positive for P-ANCA. Thus necrotizing pneumonia and other infections (tuberculosis, fungal infections etc.), systemic vasculitis disorders (collagen vascular disorders, WG, MPA and CSS) and vasculitis without systemic manifestations (pulmonary renal syndromes and pulmonary limited MPA) as the cause of DAH were ruled out in our case. Absence of smoking history, presence of frank hemoptysis (rather than blend hemorrhage), persistent bloody aspirates in BAL and the presence of necrotizing lesions in her X-ray chest did not favor the diagnosis of idiopathic pulmonary hemosiderosis either. Thus we were left with IPIPC as the only feasible diagnosis in our case. Successful response to pulse therapy with methylprednisolone and cyclophosphamide strongly supported the diagnosis of IPIPC in our patient. Park et al.[6] were also of the opinion that although biopsy remained the key to diagnosis of IPIPC yet a confident diagnosis may occasionally be made without tissue biopsy on the basis of clinic-radiological features.
It is suggested that IPIPC, though a rare disease, should be kept in mind and considered in differential diagnosis of DAH in an ANCA-negative young patient in the absence of systemic manifestations, more so when infections, hematological disorders, hemolysis or hemorrhage and collagen vascular diseases have been ruled out.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Brown KK. Pulmonary vasculitis. Proc Am Thorac Soc. 2006;3:48–57. doi: 10.1513/pats.200511-120JH. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nierman DM, Kalb TH, Ornstein MH, Gil J. A patient with antineutrophil cytoplasmic antibody-negative pulmonary capillaritis and circulating primed neutrophils. Arthritis Rheum. 1995;38:1855–8. doi: 10.1002/art.1780381221. [DOI] [PubMed] [Google Scholar]
- 3.Jennings CA, King TE, Jr, Tuder R, Cherniack RM, Schwarz MI. Diffuse alveolar hemorrhage with underlying isolated, pauciimmune pulmonary capillaritis. Am J Respir Crit Care Med. 1997;155:1101–9. doi: 10.1164/ajrccm.155.3.9116994. [DOI] [PubMed] [Google Scholar]
- 4.Monteiro AS, Addor G, Nigri DH, Torres W, Franco CA. Diffuse alveolar hemorrhage resulting from Pauci-immune pulmonary capillaritis. J Pneumologia. 2003;29:217–220. [Google Scholar]
- 5.Cordier JF, Cottin V. Alveolar hemorrhage in vasculitis: Primary and secondary. Semin Respir Crit Care Med. 2011;32:310–21. doi: 10.1055/s-0031-1279827. [DOI] [PubMed] [Google Scholar]
- 6.Park MS. Diffuse alveolar hemorrhage. Tuberc Respir Dis (Seoul) 2013;74:151–62. doi: 10.4046/trd.2013.74.4.151. [DOI] [PMC free article] [PubMed] [Google Scholar]