

Abstract
The porpose of this study was to determine the optimal length of power arms for achieving controlled anterior tooth movement in segmented arch mechanics combined with power arm. A three-dimensional finite element method was applied for the simulation of en masse anterior tooth retraction in segmented power arm mechanics. The type of tooth movement, namely, the location of center of rotation of the maxillary central incisor in association with power arm length, was calculated after the retraction force was applied. When a 0.017 × 0.022-in archwire was inserted into the 0.018-in slot bracket, bodily movement was obtained at 9.1 mm length of power arm, namely, at the level of 1.8 mm above the center of resistance. In case a 0.018 × 0.025-in full-size archwire was used, bodily movement of the tooth was produced at the power arm length of 7.0 mm, namely, at the level of 0.3 mm below the center of resistance. Segmented arch mechanics required shorter length of power arms for achieving any type of controlled anterior tooth movement as compared to sliding mechanics. Therefore, this space closing mechanics could be widely applied even for the patients whose gingivobuccal fold is shallow. The segmented arch mechanics combined with power arm could provide higher amount of moment-to-force ratio sufficient for controlled anterior tooth movement without generating friction, and vertical forces when applying retraction force parallel to the occlusal plane. It is, therefore, considered that the segmented power arm mechanics has a simple appliance design and allows more efficient and controllable tooth movement.
Keywords: Segmented arch, finite element method, power arm
Introduction
Two types of mechanics have been commonly used for space closure in extraction cases during orthodontic treatment. One is the non-friction technique, so-called loop mechanics wherein space closure is achieved by activation of closing loops incorporated into an archwire.1,2 The other is the friction technique, so-called sliding mechanics wherein a straight archwire slides through the brackets and tubes.3–7 Both techniques have several advantages and disadvantages. When loop mechanics is employed, 100% of force magnitude is delivered to the anterior teeth because of non-friction system. However, the anterior teeth tend to be tipped into the extraction site since the retraction force is passing at the level of brackets which are located incisal to the center of resistance (CR) of the anterior segment. Another disadvantage is that an excessive vertical force could be generated if a gable bend is given to a closing loop to obtain a higher moment-to-force ratio (M/F).8 In sliding mechanics, the anterior tooth movement can be controlled by using power arms attached onto an archwire. However, the friction, which is generated at the bracket–wire interface, may reduce the velocity of tooth movement and consequently prolong the treatment time.
To overcome the shortcomings of those conventional techniques for space closure, segmented arch technique has been developed.9 In this technique, friction is not produced since an archwire is divided into three pieces, namely, one for the anterior segment and the other two for both the right and left posterior segments. In addition, movements of both the anterior and posterior segments can be controlled by varying the angulation of the arms and position of retraction T loops, which are placed between anterior and posterior segmented arches, and delivering differential M/F. However, this technique has not been widely popularized due to the complexity of technique and appliance design. In addition, vertical forces are exerted on both segments as side effects since the loop is mostly placed at a closer position to the canine (off-center position) to deliver higher M/F to the anterior segment in this technique.
It is suggested that a combination of segmented arch mechanics and power arms would produce higher M/F without generating friction and vertical forces,9–12 thereby allowing efficient and controllable tooth movement.
The purpose of this study was to determine the optimal height of power arm for attaining controlled movement of the anterior teeth in segmented power arm mechanics by means of three-dimensional (3D) finite element method (FEM).
Materials and methods
3D finite element model
Using a multi-image cone beam computed tomography (CT) scanner (3DX; J. Morita, Kyoto, Japan), images of the 14 maxillary teeth were taken. These CT images were saved as digital imaging and communication in medicine (DICOM) data and exported to 3D image processing and editing software (Mimics 10.02; Materialize Software, Leuven, Belgium). The 3D solid model was created and converted to 3D finite element (FE) model by using FE analysis pre- and post-processor software (Patran 2008r1; MSC Software Corp, Los Angeles, CA, USA). Each 3D FE model for periodontal ligament (PDL), alveolar bone, bracket, archwire, and power arm was separately constructed using the same software. Thickness of the PDL was determined to be a uniform 0.2 mm.8–10 All the brackets were with 0.018 × 0.025-in slot, and 0.017 × 0.022-in and 0.018 × 0.025-in stainless steel archwires were modeled. All brackets were sited on the facial-axis points.13 Based on these 3D solid models, an FE mesh was created to make a node-to-node connection between tooth, PDL, and alveolar bone. An FE mesh of the archwire was created separately from the bracket. In this model, the perpendicular distance from bracket slot to the CR of the maxillary central incisor is 7.3 mm. The 3D FE model consisted of 399,000 10-noded isoparametric tetrahedral solid elements and 77,600 nodes (Figure 1).
Figure 1.
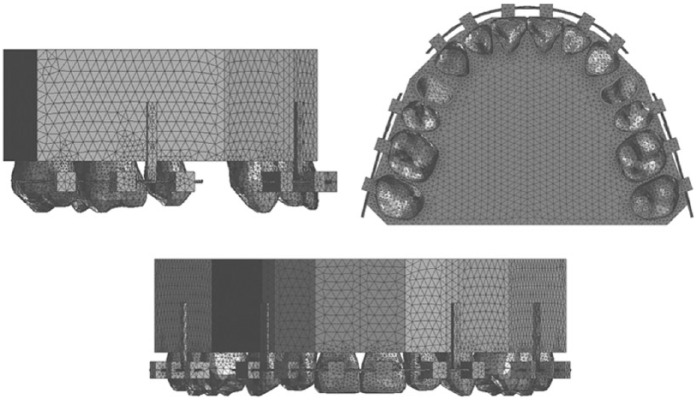
3D finite element model of maxillary dentition, including PDL, alveolar bone, brackets, and archwire.
Material parameters
The material parameters used in this study are represented in Table 1.14–16 In order to simplify the model and to reduce the time for analysis, the same properties were given to the archwire, power arm, and brackets. The structures of tooth, alveolar bone, and PDL were modeled as being homogeneous and isotropic for the same reason.
Table 1.
Material parameters of tooth, PDL, alveolar bone, archwire, power arm, and bracket.
| Material | Young’s modulus (MPa) | Poisson’s ratio |
|---|---|---|
| Tooth | 20,000 | 0.30 |
| PDL | 0.05 | 0.30 |
| Alveolar bone | 2000 | 0.30 |
| Archwire/power arm/bracket | 200,000 | 0.30 |
PDL: periodontal ligament.
FE loads and boundary conditions
The model was a bilaterally first premolar extraction case on the assumption of a maxillary protrusion case. Segmented power arm mechanics consisted of three segmented archwires for anterior and posterior segments (Figure 2). Four power arms were employed in this mechanics. Two of them were attached onto the anterior segmented wire at the sites between lateral incisor and canine bilaterally and perpendicular to the archwire. Other two power arms were attached onto the posterior segmented wires at the sites between second premolar and first molar. In order to focus on the anterior tooth movement, it was assumed that the posterior teeth were connected with the implant anchorage so that they could not move.
Figure 2.
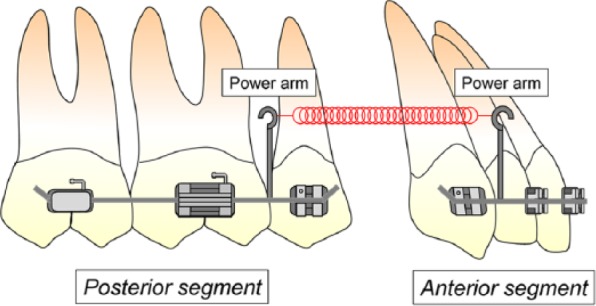
Illustration of the segmented power arm mechanics.
A retraction force of 300 g was applied bilaterally to the power arms parallel to the archwire. The height levels of the power arms were 0, 2, 4, 6, 8, 10, and 12 mm from the bracket slot to clarify the relationship between the height of horizontal force and degree of labiolingual tipping of the maxillary central incisor. Additionally, more detailed analysis was made by changing the level of power arm at an interval of 0.1 mm to obtain the required height for achieving controlled lingual root tipping, bodily movement, and controlled lingual crown tipping. The model was restrained in 6 degrees of freedom at the bottom of the alveolar bone to avoid sliding movement of the entire model. Coefficient of friction between bracket slots and archwire was assumed to be 0.2.7,17,18 Under these conditions, 3D FE analysis was performed by using a 3D FE program (Marc; MSC Software Corp). We investigated how the maxillary central incisor moved after orthodontic force application, and the comparison of the results obtained with 0.017 × 0.022-in and 0.018 × 0.025-in stainless steel archwires was performed. Clinical application of this mechanics with respect to sliding mechanics will also be discussed.
Results
Figure 3 shows the controlled anterior tooth movements such as controlled lingual root tipping, bodily movement, and controlled lingual crown tipping. The controlled lingual root tipping is the type of tooth movement in which the tooth tips around its incisal edge as the center of rotation (CRo). On the other hand, controlled lingual crown tipping indicates the movement in which the tooth tips with its root apex as the CRo.
Figure 3.
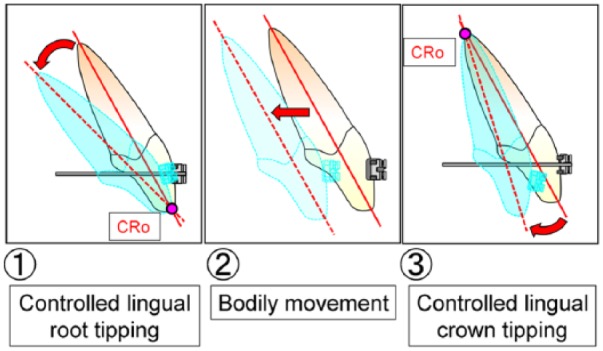
The type of controlled anterior tooth movement.
The relationship between the degree of labiolingual tipping of the maxillary central incisor and height of the retraction force on the power arm is shown in Figure 4. In case the 0.017 × 0.022-in stainless steel archwire was used, that is, a play existed between brackets and archwire, the controlled lingual crown tipping of the maxillary central incisor was observed when the retraction force was set at 8.1 mm (Figure 5). The direction of tooth rotation changed from lingual crown tipping to lingual root tipping as the height level of the retraction force on the power arm was moved apically from the level of the bracket slot. At the height level of 9.1 mm, no rotation was produced and bodily movement occurred. Controlled lingual root tipping of the incisor was observed when the retraction force was set at 9.7 mm height of power arm.
Figure 4.

The relationship between the degree of labiolingual tipping of the maxillary central incisor and the height of retraction force on the power arm.
Figure 5.
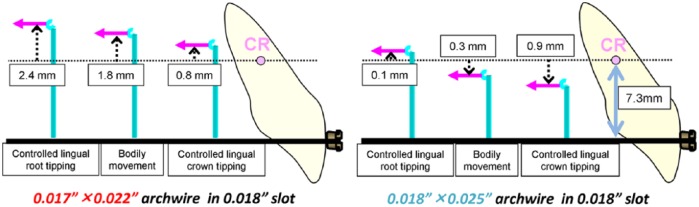
Loading conditions when controlled anterior tooth movements are performed.
When the 0.018 × 0.025-in stainless steel archwire was used, the rotational tendency was the same as in the case previously mentioned. Bodily movement of the incisor was achieved at the height level of the retraction force of 7.0 mm. The controlled lingual crown tipping was obtained at 6.4 mm, and the controlled lingual root tipping occurred at 7.4 mm height of power arm.
Discussion
It was clarified that a close relationship existed between the type of anterior tooth movement and the length of power arm employed in segmented power arm mechanics. When a play at the bracket–wire interface existed, namely, a 0.017 × 0.022-in archwire was engaged in 0.018-in slot brackets, controlled lingual crown tipping of the incisor was observed in case the retraction force passes at the level of 0.8 mm apical to the CR of the tooth. Bodily movement was achieved at 1.8 mm above the CR. Controlled lingual root tipping occurred at the height of 2.4 mm above the CR. In case of a single tooth movement, the force passing through the CR translates a tooth.19 However, this concept does not work with the segmented power arm mechanics as well as with sliding mechanics.20 It may be due to the existence of a play between bracket and archwire, which could cause the anterior teeth to be freely tipped until the binding of the archwire in the bracket slots is generated in the early stage of space closure. Thus, the length of power arm longer than the perpendicular distance from bracket slot to the CR is required to achieve bodily movement under the condition that a play between bracket and archwire exists.20
On the other hand, when a 0.018 × 0.025-in full-size archwire was used, controlled lingual crown tipping, bodily movement, or controlled lingual root tipping of the central incisor was achieved when applying a retraction force at the level of 0.9 mm, 0.3 mm below, or 0.1 mm above the CR, respectively. In other words, bodily movement can be produced by applying the force approximately at the level of the CR according to biomechanical principles. It contributes to more predictable anterior tooth movement. Thus, it is considered that a usage of a full-size archwire is recommendable for achieving controlled anterior tooth movement within the range of shorter lengths of power arms, which could reduce the risk of causing irritation on the buccal mucosa.
Especially in extraction cases, the control of the anterior tooth movement is quite important since the total amount of movement of the anterior teeth tends to be relatively large. The relocation of the anterior teeth to their final target destinations along the shortest paths possibly results in more efficient tooth movement and faster treatment. An elimination of excess movement also reduces the risk of root resorption.
In such background, several techniques have been used to achieve controlled anterior tooth movement. Nevertheless, conventional techniques for space closure have some disadvantages. In sliding mechanics, although the anterior tooth movement can be controlled by changing the length of power arms attached onto an archwire, extremely long power arms are required since an undersized archwire is employed in order to reduce friction. In other words, as mentioned above, a longer power arm is required for controlled anterior tooth movement when there is a play between brackets and archwire as compared with when a full-size archwire is used.20 Then, an impingement of long power arms on the gingival mucosa is likely to be produced in case the mucobuccal fold is shallow. For this reason, torque control of anterior teeth is still difficult for some patients even with utilization of power arms combined with sliding mechanics. Contrary to this, in segmented power arm mechanics, bodily movement can be achieved by power arm whose height is almost at the same level as the CR.
In loop mechanics, although it is non-friction system, the stiffness of an archwire is reduced in the region where loops are incorporated. This causes a substantial amount of deformation of an archwire, and consequently uncontrolled tipping of the anterior teeth is expected to be produced in this technique. Another disadvantage is that the higher degree of gable bend is placed in a loop for obtaining a higher M/F, and the more substantial magnitude of vertical force could be generated.8 On the contrary, in segmented power arm mechanics, higher M/F can be easily produced by attaching power arms onto an archwire, which enables orthodontists to attain any type of anterior tooth movement within the applicable range of power arm length in daily orthodontic practice. In addition to it, this mechanics produces no friction, which contributes to speedy and efficient tooth movements.
The use of Burstone’s segmented arch technique allows controlled movement of both anterior and posterior segments. However, it has some disadvantages. That is, this technique and its appliance design are complicated and vertical forces are generated as undesirable side effects since the loop is placed at off-center position between anterior and posterior segments. On the other hand, the segmented power arm mechanics can provide sufficient amount of M/F for controlled tooth movement without generating vertical forces in a simple design when the retraction force is set to be parallel to the occlusal plane. It is, therefore, suggested that the segmented power arm mechanics is an effective method which has advantages of both sliding and loop mechanics and can allow accurate and controllable anterior tooth movement during space closure.
The FE analysis performed in this study was based on a linear analysis and was limited to a calculation of initial tooth displacements. Further study will be required to construct a FE model whose material parameters are approximate to the living body and to develop the system which can simulate a long-term orthodontic tooth movement including bone remodeling process.
Clinical application
The segmented power arm mechanics has another advantage from clinical aspect. That is, the anterior tooth movement can be monitored in the course of space closure. If lingual root tipping of the incisor occurs, there will be a vertical step between the height level of distal end of the anterior segment and the mesial end of posterior segment of an archwire (Figure 6(a)).
Figure 6.
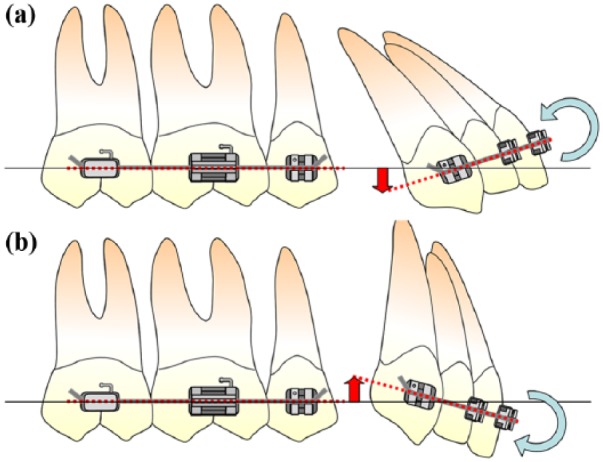
Relationship between the tendency of the anterior tooth movement and the position of the wire end of each segment: (a) if controlled lingual root tipping of the central incisor was achieved and (b) if controlled lingual crown tipping of the central incisor was achieved.
If lingual crown tipping of the incisor is produced, height level of distal end of the anterior segment of an archwire is higher than the mesial end of posterior segment (Figure 6(b)). When the levels of both ends of segmented arches are the same, bodily movement is performed when the retraction force parallel to the occlusal plane is applied. In other words, several months after this mechanics was employed, the tendency of the central incisor movement can be easily estimated by comparing the height of the distal end of the archwire on the anterior segment and the mesial end of the posterior segment wire. In this manner, we can evaluate how the anterior teeth move by observing the vertical step of the wire ends. If the type of tooth movement deviates from one at the time of the diagnosis, the power arm length should be adjusted so as to redirect the anterior tooth movement to its final destination.
Conclusion
In the segmented arch mechanics, required height level of power arms for achieving controlled anterior tooth movement was determined to be within 1 mm of the level of the CR of the anterior teeth, which is much shorter as compared with when sliding mechanics is used in combination with power arms. By reducing the required length of power arm, patients’ comfort would be improved, and space closing mechanics could be widely applied even for the patients whose mucobuccal fold is shallow.
The segmented arch mechanics combined with power arm could provide higher amount of M/F sufficient for controlled anterior tooth movement without generating friction and vertical forces when applying retraction force parallel to the occlusal plane. It is, therefore, considered that the segmented power arm mechanics has a simple appliance design and allows more efficient and controllable tooth movement.
Footnotes
Declaration of conflicting interest: The authors declare that there is no conflict of interest.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- 1. Burstone CJ, Koenig HA. Optimizing anterior and canine retraction. Am J Orthod 1976; 70(1): 1–19. [DOI] [PubMed] [Google Scholar]
- 2. Burstone CJ. The segmented arch approach to space closure. Am J Orthod 1982; 82(5): 361–378. [DOI] [PubMed] [Google Scholar]
- 3. Bennett JC, McLaughlin RP. Controlled space closure with a preadjusted appliance system. J Clin Orthod 1990; 24(4): 251–260. [PubMed] [Google Scholar]
- 4. Bennett JC, McLaughlin RP. Management of deep overbite with a preadjusted appliance system. J Clin Orthod 1990; 24(11): 684–696. [PubMed] [Google Scholar]
- 5. McLaughlin RP, Bennett JC. The transition from standard edgewise to preadjusted appliance systems. J Clin Orthod 1989; 23(3): 142–153. [PubMed] [Google Scholar]
- 6. McLaughlin RP, Bennett JC. Finishing and detailing with a preadjusted appliance system. J Clin Orthod 1991; 25(4): 251–264. [PubMed] [Google Scholar]
- 7. Kusy RP, Whitley JQ, Prewitt MJ. Comparison of the frictional coefficients for selected archwire-bracket slot combinations in the dry and wet states. Angle Orthod 1991; 61(4): 293–302. [DOI] [PubMed] [Google Scholar]
- 8. Yoshida N, Jost-Brinkmann PG, Koga Y, et al. Moment/Kraft-Verhältnisse von Kontraktionsbögen während Deaktivierung. Kieferorthop 2004; 18: 175–182. [Google Scholar]
- 9. Choy K, Pae EK, Kim KH, et al. Controlled space closure with a statically determinate retraction system. Angle Orthod 2002; 72(3): 191–198. [DOI] [PubMed] [Google Scholar]
- 10. El-Bialy T. Segmented and sectional orthodontic technique: review and case report. J Health Spec 2013; 1(2): 90–96. [Google Scholar]
- 11. Sia SS, Koga Y, Yoshida N. Determining the center of resistance of maxillary anterior teeth subjected to retraction forces in sliding mechanics. Angle Orthod 2007; 77(6): 999–1003. [DOI] [PubMed] [Google Scholar]
- 12. Park YC, Choy K, Lee JS, et al. Lever-arm mechanics in lingual orthodontics. J Clin Orthod 2000; 34(10): 601–605. [PubMed] [Google Scholar]
- 13. Andrews LF. The six keys to optimal occlusion. In: Andrews LF. (ed.) Straight wire: the concept and appliance. San Diego, CA: LA Wells, 1989, pp. 13–24. [Google Scholar]
- 14. Collidge ED. The thickness of the human periodontal membrane. J Am Dent Assoc Dent Cosmos 1937; 24: 1260–1270. [Google Scholar]
- 15. Vollmer D, Bourauel C, Maier K, et al. Determination of the centre of resistance in an upper human canine and idealized tooth model. Eur J Orthod 1999; 21: 633–648. [DOI] [PubMed] [Google Scholar]
- 16. Reimann S, Keilig L, Jager A, et al. Biomechanical finite-element investigation of the position of the centre of resistance of the upper incisors. Eur J Orthod 2007; 29: 219–224. [DOI] [PubMed] [Google Scholar]
- 17. Kusy RP. Effect of salivary viscosity on frictional coefficients of orthodontic archwire/bracket couples. J Mater Sci Mater Med 1995; 6: 390–395. [Google Scholar]
- 18. Kusy RP, Whitley JQ. Friction between different wire-bracket configurations and materials. Semin Orthod 1997; 3: 166–177. [DOI] [PubMed] [Google Scholar]
- 19. Nanda R, Ghosh J. Biomechanical considerations in sliding mechanics. In: Nanda R. (ed.) Biomechanics in clinical orthodontics. Philadelphia, PA: W.B. Saunders Co, 1997, pp. 188–217. [Google Scholar]
- 20. Tominaga JY, Chiang PC, Ozaki H, et al. Effect of play between bracket and archwire on anterior tooth movement in sliding mechanics: a three-dimensional finite element study. J Dent Biomech. Epub ahead of print 17 October 2012. DOI: 10.1177/1758736012461269. [DOI] [PMC free article] [PubMed] [Google Scholar]