

Abstract
Rationale: Marked socioeconomic health-care disparities are recognized in India, but lung health inequalities between urban and rural children have not been studied.
Objectives: We investigated whether differences exist in spirometric pulmonary function in healthy children across the Indian urban–rural continuum and compared results with those from Indian children living in the UK.
Methods: Indian children aged 5 to 12 years were recruited from Indian urban, semiurban, and rural schools, and as part of the Size and Lung Function in Children study, London. Anthropometric and spirometric assessments were undertaken.
Measurements and Main Results: Acceptable spirometric data were obtained from 728 (58% boys) children in India and 311 (50% boys) UK-Indian children. As an entire group, the India-resident children had significantly lower z FEV1 and z FVC than UK-Indian children (P < 0.0005), when expressed using Global Lung Function Initiative–2012 equations. However, when India-resident children were categorized according to residence, there were no differences in z FEV1 and z FVC between Indian-urban and UK-Indian children. There were, however, significant reductions of ∼0.5 z scores and 0.9 z scores in both FEV1 and FVC (with no difference in FEV1/FVC) in Indian-semiurban and Indian-rural children, respectively, when compared with Indian-urban children (P < 0.0005). z Body mass index, socioeconomic circumstances, tobacco, and biomass exposure were individually significantly associated with z FEV1 and z FVC (P < 0.0005).
Conclusions: The presence of an urban–rural continuum of lung function within a specific ethnic group emphasizes the impact of environmental factors on lung growth in emerging nations such as India, which must be taken into account when developing ethnic-specific reference values or designing studies to optimize lung health.
Keywords: children, urban, rural, socioeconomic circumstances, ethnic differences in lung function
At a Glance Commentary
Scientific Knowledge on the Subject
Although it is well established that ethnic differences exist in lung size, the underlying causes for this remain controversial, at least partly due to failure to take potential confounders into account.
What This Study Adds to the Field
After adjusting for known confounders, average FEV1 and FVC in Indian urban children are similar to those in Indian children living in the UK, both being approximately 11% lower than that predicted for white European children. Values were, however, significantly lower in Indian semiurban and rural children (by ∼6 and 11%, respectively) when compared with their Indian urban counterparts, emphasizing the need to take nutritional status and environmental exposures into account when establishing ethnic-specific reference data or investigating risk factors associated with lifelong lung health.
Disease burden from chronic respiratory disease is increasing globally, with chronic obstructive pulmonary disease (COPD) predicted to become the third leading cause of mortality by 2030 (1). Although the main risk factors for the development of COPD are genetic, tobacco, and biomass smoke exposure, failure to attain optimal lung and airway growth during childhood constitutes a significant risk (2). Normal lung growth and development during the intrauterine period and early childhood are important for attaining maximal adult lung function. A number of early life factors, including maternal smoking, low birth weight, prematurity, indoor air pollution, and childhood infections, all of which may reflect poor early life socioeconomic circumstances (SEC), are associated with reduced lung function in childhood and early adulthood (3–7). The extent to which such factors contribute to chronic lung disease in resource-poor countries is, however, often confounded by ethnic differences in lung function.
Ethnic differences in lung function were first reported more than 150 years ago (8) and have been variously ascribed to differences in body physique, SEC, environmental exposures, and/or genetic ancestry (9–14). Interpretation of these studies is complicated not only by differences in methodology, study population, and sample size but also by the heterogeneity of regional populations in developing countries, making it challenging to assess the extent to which ethnic differences reflect those factors primarily determined by genetics (12, 15). Several studies have reported higher lung function in specific nonnative ethnic groups born and living in developed countries as opposed to first-generation immigrants or those residing in their native country (16, 17). Gaps in health-related outcomes between the rich and poor are large, with widening urban–rural disparities in life expectancy (18), particularly in developing countries such as India (19). Few studies have investigated disparities in lung health in healthy children across the urban–rural continuum with different socioeconomic and environmental exposures that could affect lung development (20, 21).
We hypothesized that lung function in healthy Indian children residing in India will be lower than that in healthy Indian children residing in the UK and that, within India, lung function will be adversely affected in children living in rural or semiurban regions when compared with those residing in the more affluent urban areas.
Some of the results of this study have been previously reported in the form of an abstract (22).
Methods
This prospective cross-sectional study was conducted in India and the UK using identical equipment, techniques, and quality control criteria to compare spirometric lung function. The M.S. Ramaiah Medical College and Teaching Hospitals Ethics Board, Bengaluru, Karnataka, India, approved the study undertaken in India. Assessments undertaken as part of the London Size and Lung Function in Children (SLIC) study were granted ethical approval by the Research Ethics Committee (London-Hampstead: REC 10/H0720/53) (23). Parental written consent and verbal assent from each child were obtained before assessments.
Subjects
All healthy school children between 5 and 12 years old with parental consent were eligible. Children were only excluded from assessments if they had overt signs of illness on the test day. For final analysis, data were excluded from children with: current or chronic respiratory disease (e.g., current asthma, prior bronchopulmonary dysplasia, pulmonary tuberculosis) or significant congenital abnormalities likely to influence lung function (23).
For the Indian study, healthy children were recruited from schools in Bengaluru city (one school), Yelahanka (semiurban; one school), and Kaiwara (rural; two schools), Karnataka, India between January 2013 and August 2013. Indian children residing in India were further categorized according to the area of residence to urban, semiurban, and rural (henceforth referred to as Indian urban, Indian semiurban, and Indian rural). Anthropometric and spirometric measurements were performed at schools. For the SLIC study, measurements were undertaken in London within a mobile laboratory parked in the school grounds or in classrooms between December 2010 and July 2013 (23). Identical methods, equipment, and quality control were used for both studies.
Assessments.
The child’s respiratory history, family SEC, and tobacco and biomass smoke exposures were obtained via a questionnaire administered to the child by the researcher. SEC were considered at the individual level using the Family Affluence Scale (FAS) based on collated score for number of computers, vehicle ownership, and whether the child had their own bedroom (23, 24). Weight, standing and sitting height, and other anthropometric measurements were undertaken using established protocols (25). Height, weight, and body mass index (BMI) were expressed as sex-specific standard deviation (SD) scores (z scores) based on Indian growth charts (25).
Spirometry assessments were performed according to American Thoracic Society/European Respiratory Society standards adapted for children (25, 28) using the portable Easy-on-PC spirometer (ndd, Zurich, Switzerland). All assessments were undertaken with the child seated and nose clip in situ. Successful spirometry was defined as those with at least two technically acceptable forced expiratory maneuvers according to American Thoracic Society/European Respiratory Society acceptability and repeatability criteria adapted for children (26). All spirometry data were subjected to independent quality control using the same overread method (26). Outcome measures were FVC, FEV1, and FEV1/FVC. All data were adjusted for age, sex, and height and expressed using recently derived Global Lung Function Initiative (GLI)-2012 Indian spirometry coefficients (27, 28).
Statistical Analysis
Power of study.
Comparison of data from ∼300 Indian children living in India with those from a similar number of Indian subjects residing in London from the SLIC study (henceforth referred to as UK-Indian) would provide 90% power at the 5% significance level to detect differences in either anthropometry or spirometry equivalent to ∼0.25 z scores. When determining differences between children living in India according to residence, technically satisfactory data from 160 children in each group would be required to give similar power and significance to detect differences of ∼0.4 z scores between urban and either the semiurban or rural children, while adjusting for the two comparisons.
Data from the Indian urban children were compared with those from UK Indian children (23), using independent-samples t tests. For the Indian arm of the study, a one-way between-subjects analysis of variance and Chi-square tests were conducted as appropriate to compare demographic differences and lung function results between urban, semiurban, and rural children. Anthropometric and demographic variables tested were current weight, BMI, chest dimensions, FAS, and biomass and tobacco smoke exposure. For the numeric variables, Tukey honest significant difference post hoc comparisons were used to further examine the pattern of differences. Univariable and multivariable linear regression were performed to further quantify spirometric outcomes according to area of residence.
All analyses were performed using SPSS software for Windows, version 22 (SPSS Inc, Chicago, IL). Graphs were created using GraphPad Prism, version 5 (GraphPad Software; San Diego, CA).
Results
Data were available for 311 Indian subjects from the SLIC study, UK (Table 1). Of these, 241 were born in the UK. The characteristics and spirometry results of UK-born Indian children and Indian children residing in the UK but born elsewhere were virtually identical (see Table E1 in the online supplement). Thus, for the purposes of this manuscript, all the UK Indian children are included when comparing with results from those residing in India. Nine hundred fourteen children were recruited to the Indian arm of the study. After excluding three children with current asthma from the urban cohort and technically unacceptable spirometric data (183 children [i.e., 20% failure rate]), results were available from 728 children (58% boys) (Figure 1 and Table 1). The results presented include 10% of the children with mild upper respiratory symptoms during assessments, as this had no significant impact on results (Table E2). When considered as a total group, Indian children residing in India were significantly shorter and lighter after adjustment for age and sex, with significantly lower z FEV1 and z FVC than their UK Indian counterparts, but with no differences in FEV1/FVC (Table 1 and Figure 2).
Table 1.
Comparison of Characteristics and Lung Function between UK Indian and All Indian (Urban, Semiurban, and Rural) Children
| UK-Indian | All Indian | Mean Difference (UK − India) (95% CI) | P Value | |
|---|---|---|---|---|
| Subjects, N (% boys) | 311 (50) | 728 (51) | ||
| Age, yr | 8.1 (1.6) | 9.6 (2.0) | −1.55 (−1.78 to −1.31) | <0.0005 |
| z Height* | 0.34 (1.0) | −0.54 (1.1) | 0.88 (0.74 to 1.02) | <0.0005 |
| z Weight* | 0.13 (1.0) | −0.57 (1.2) | 0.70 (0.56 to 0.84) | <0.0005 |
| z BMI* | −0.04 (1.0) | −0.41 (1.0) | 0.37 (0.24 to 0.50) | <0.0005 |
| FAS | 3.5 (1.4) | 1.7 (1.7) | 1.8 (1.5 to 1.9)† | <0.0005 |
| Household tobacco smoking, n (%) | 42 (14) | 169 (23) | −9 (−14 to −5) | 0.027 |
| z FEV1 | 0.04 (0.94) | −0.32 (1.0) | 0.36 (0.23 to 0.49) | <0.0005 |
| z FVC | 0.01 (0.96) | −0.34 (1.1) | 0.35 (0.22 to 0.48) | <0.0005 |
| z FEV1/FVC | 0.16 (1.03) | 0.14 (1.0) | 0.02 (−0.12 to 0.16) | 0.770 |
Definition of abbreviations: BMI = body mass index; FAS = family affluence score.
Results are expressed as mean (SD) unless otherwise specified. FAS based on collated score for numbers of computers, vehicle ownership (car, motorcycle, bicycle), and whether the child had own bedroom (score 0–6).
z Height, z weight, and z BMI are based on Indian growth charts (25).
P < 0.0005. Spirometry results are adjusted for age, height, and sex based on recently derived Global Lung Function Initiative–2012 coefficients for Indian children (28).
Figure 1.
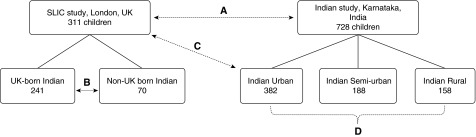
Subjects with acceptable spirometry data in the two arms of the study and comparisons between different groups. (A) Comparison of lung function between UK-Indian and all India resident children (Table 1, Figure 2). (B) Comparison of lung function between UK-born and non-UK born Indian children resident in the UK (Table E1). (C) Comparison of lung function between UK-Indian and Indian urban children (Table E3). (D) Comparison of lung function between Indian urban, semiurban, and rural children (Table E4, Figure 3). SLIC = Size and Lung Function in Children.
Figure 2.

Spirometry data from UK Indian and all Indian children according to Global Lung Function Initiative–2012 Indian equations. Solid black lines indicate mean and SD. Dashed lines depict ±2 z scores, within which 95% of well-nourished Indian children would fall (27, 28).
Association between Place of Residence and Lung Function
When data were analyzed according to place of residence, significant differences were seen between the four groups (UK Indian, Indian urban, Indian semiurban, and Indian rural) with respect to both demographic and spirometric outcomes (Table 2, Figure 3). Indian urban children were significantly older than the UK Indian children by, on average, 1 year. However, after expressing results as z scores, which adjust for height, age, and sex, spirometric outcomes between UK Indian children and Indian urban children were virtually identical (Table E3), with mean (SD) z scores based on the Indian GLI-based coefficient (28) approaching zero (1) as expected for a “normal” population.
Table 2.
Population Characteristics and Lung Function According to Place of Residence
| UK Indian | Indian Urban | Indian Semiurban | Indian Rural | |
|---|---|---|---|---|
| Subjects, n (% boys) | 311 (50) | 382 (68)* | 188 (43) | 158 (51) |
| Age, yr | 8.1 (1.6) | 9.0 (1.9) | 10.8 (1.8) | 9.8 (1.9) |
| z Height† | 0.34 (1.0) | 0.07 (0.9) | −1.19 (1.0) | −1.24 (0.9) |
| z Weight† | 0.13 (1.0) | 0.13 (0.9) | −1.31 (0.9) | −1.38 (0.9) |
| z BMI† | −0.04 (1.0) | 0.12 (0.9) | −0.98 (0.8) | −1.02 (0.8) |
| FAS | ||||
| High FAS (5–6), n (%) | 77 (25) | 42 (11) | 0 | 0 |
| Medium FAS (2–4), n (%) | 206 (67) | 308 (81) | 45 (24) | 0 |
| Low FAS (0–1), n (%) | 24 (8) | 32 (8) | 143 (76) | 158 (100) |
| Exposure to household tobacco smoking, n (%) | 42 (14) | 34 (9) | 78 (42) | 57 (36) |
| Exposure to indoor biomass smoke, n (%)‡ | 0 (0) | 0 (0) | NA | 142 (90) |
| z FEV1 | 0.04 (0.94) | 0.02 (0.95) | −0.52 (0.85) | −0.88 (0.99) |
| z FVC | 0.01 (0.96) | −0.00 (0.99) | −0.56 (0.89) | −0.91 (1.22) |
| z FEV1/FVC | 0.16 (1.03) | 0.11 (0.93) | 0.11 (0.89) | 0.26 (1.28) |
| Respiratory symptoms§ | 18 (6) | 52 (14) | 49 (26) | 30 (19) |
| Prior asthma | 0 | 14 (4) | 2 (1) | 1 (1) |
Definition of abbreviations: BMI = body mass index; FAS = family affluence score; NA = not available.
Results are expressed as mean (SD), unless otherwise specified; P values were derived from analysis of variance or Chi-square test as appropriate. FAS was grouped in three categories due to the large variation in scores according to area of residence (data were missing in four UK-Indian children).
Data from three children with current asthma were excluded.
z Height, z weight, and z BMI are based on Indian growth charts (25).
Data on biomass smoke exposure were not available for the semiurban group. Spirometry results are adjusted for age, height, and sex based on recently derived Global Lung Function Initiative–2012 coefficients for Indian children (28); at this age 1 z score for FEV1 and FVC equates to a difference of ∼11% (28).
Respiratory symptoms included runny nose, mild cough, and upper respiratory tract infections on the day of testing. Inclusion of data from these children did not impact overall lung function results as summarized in Table E2.
Figure 3.
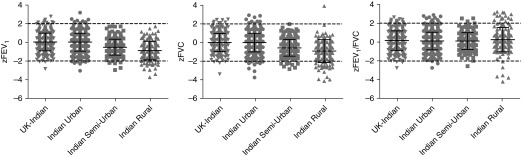
Spirometry data from UK Indian and India resident children according to place of residence using Global Lung Function Initiative–2012 Indian equations. Solid black lines indicate mean and SD. Dashed lines depict ±2 z scores, within which 95% of well-nourished Indian children would fall (27, 28).
Height, weight, and BMI z scores were significantly lower in the rural and semiurban children when compared with urban children, but there was no significant difference between rural and semiurban children (Table 2, Table E4). FAS was significantly lower in rural than in both urban and semiurban children (P < 0.0005) (Table 2). Both tobacco and biomass smoke exposure were significantly higher in the rural children (P < 0.0005), whereas tobacco smoke exposure was highest among the semiurban children (Table 2).
Both FEV1 and FVC were significantly reduced by, on average, 0.5 z scores in the Indian semiurban and 0.9 z scores in Indian rural children when compared with Indian urban children (Table 2, Figure 3, Table E4). The proportional reductions in FEV1 and FVC meant, however, that FEV1/FVC was not significantly different between groups (Table 2, Figure 3, Table E4).
On univariable regression analysis, z height, z weight, z BMI (as surrogates for nutritional status), FAS, and environmental exposure to tobacco smoke and biomass fuel were significantly associated with z FEV1 and z FVC. However, many of these variables were highly correlated with place of residence (especially in children from rural schools), such that the degree of multicollinearity precluded attempts to attribute the specific contribution from any one of these factors independently using multivariable linear regression analysis.
After adjustment for potential confounders, namely z weight, z BMI, tobacco and biomass smoke exposures, and FAS in a multivariable regression model, a significant mean reduction of 0.75 (95% confidence interval, −1.27 to −0.22) in z FEV1 and 0.77 (95% confidence interval, −1.33 to −0.20) in z FVC remained between Indian rural and urban children.
Discussion
After adjusting for age, height, and sex, we found that, as an entire group, Indian children residing in India had significantly lower FEV1 and FVC when compared with Indian children residing in the UK. However, when Indian children residing in India were categorized according to place of residence, there was no difference in lung function between the UK Indian and Indian urban children, but there was a gradient average reduction of ∼0.5 z scores and 0.9 z scores in both FEV1 and FVC in semiurban and rural children, respectively, when compared with their urban counterparts.
The relationship between residence location and health status is a complex interaction between a number of contributing factors, including SEC, environmental exposures, and nutrition (19, 20, 29, 30). However, the lower lung function in the Indian rural children was only partly explained by the multiple potential confounders that were included in the regression analyses. This suggests that there are other adverse factors, such as exposures to intrauterine and early childhood insults to the developing lung (2, 6), that could not be assessed in this study but may be responsible for the variability in lung function between the two groups.
Comparison of Lung Function in Indian Children Living in the UK and India
Although there is evidence that first-generation adult and adolescent immigrants may have lower anthropometry and pulmonary function for age and height compared with second-generation immigrants (10, 16, 17, 31–33), this was not true for the well-nourished UK-Indian children in this study, who, after adjustment for height, sex, and age, had very similar spirometric lung function to their urban counterparts in India. This may reflect the nature of immigration, lifestyle patterns, and the age of our cohort. Similarly, it has been suggested that within any specific ethnic group, higher lung function is attained in those born and living in developed countries as opposed to those residing in their native country (16, 17), which was not the case in our study. This may reflect the fact that not only were both groups of urban children well-nourished and attending schools with similar socioeconomic conditions but also identical methods and standards of quality control were applied during data collection across the entire study. It is important to note that had we simply compared results from all the children living in India with those living in the UK, without considering place of residence and associated socioeconomic and nutritional status, we would have falsely concluded that within a specific ethnic group, lung function was increased in those who had emigrated to countries such as the UK.
Strengths and Limitations
A major strength of the current study is that equipment, techniques, and quality control were based on those developed for the SLIC study (23) and were identical across all sites, such that any differences in lung function cannot be attributed to methodological discrepancies. In contrast to some field-based studies in which relatively simple spirometric equipment has precluded strict quality control during field studies (12), we used a modern ultrasonic device that stores all data and allowed immediate inspection of flow–volume loops and volume–time curves at time of data collection as well as during subsequent overread, an essential feature when assessing children. All staff were highly trained and given frequent feedback, with rate of exclusions for technically unacceptable data (∼20%) being similar to that reported in other recent studies of naive young children (34, 35).
Anthropometric data from this study were expressed as z scores based on the Khadilkar Indian growth charts, which were derived from 18,666 children attending 10 affluent schools from five major geographical regions of India (25). Data from the UK Indian and Indian urban children were comparable, with mean (SD) values ∼0 (1), suggesting that the sociodemographics of both these groups were representative of well-nourished children throughout India. For pragmatic reasons, the schools and locations within India were chosen to represent a wide spectrum of living conditions within a day’s travel of Bangalore city. Although the urban–rural socioeconomic divide is worse in certain parts of India compared with the population studied (36), which could potentially exacerbate the differences in lung function observed, urban–rural demographics throughout India are largely similar, such that the findings from this study are likely to be generalizable. All anthropometric and spirometric data were expressed as z scores, which adjusted for age, height, and sex, thereby overcoming any bias due to the slight differences in mean age between the different groups, which simply reflected local variations in policy within selected schools.
Limitations of the study include the fact that, due to lack of any systematic record-keeping in most parts of India, it was impossible to obtain any reliable data on birth weight, prematurity, childhood infections, or detailed SEC from the Indian children, all of which may contribute to the observed variability in lung function.
Ethnic Differences in Lung Function between Indian and White Children
Although there was no difference in lung function between Indian urban children and UK Indian children, both groups had significantly lower values than those predicted for white children (27) and those recently observed in the white children recruited to the SLIC study (34). This is in agreement with previous studies (9–11, 33) and presumably reflects biological variability in spirometric lung function between Indian and white subjects associated with differences in body proportions, which persist even when socioeconomic conditions and other exposures are well matched. Although being adjusted for age, standing height, and sex, current lung function reference equations, including the GLI-2012, do not take the biological differences in body frame that may exist between different populations (such as differences in sitting/standing height ratio [Cormic index] and/or chest dimensions) into account. Thus, lower lung volumes for the same stature do not necessarily indicate “worse” lung function but simply a bias in the predicted values due to their dependence on stature. It is important to note that, in this study, whether comparing results from the relatively affluent Indian urban children with those predicted for white children, or those from rural communities with their urban peers, reductions in FEV1 and FVC were proportional, such that no difference in mean FEV1/FVC was observed. This suggests that overall, despite marked differences between the degree of exposure to tobacco smoke and biomass in the various groups, there were no differences in relative airway narrowing at this age but simply a reduction in lung size (37). Although there is considerable evidence that a reduced FEV1 associated with obstructive airway disease in childhood is significantly associated with increased risk of COPD in adulthood (38), we are not aware of any data showing an increased risk in the presence of a normal FEV1/FVC.
The greater mean reduction in FEV1 of ∼30% reported among South Asian adults in the recent Prospective Urban and Rural Epidemiological Study (12) when compared with that in those of European descent may reflect the different age range, the heterogeneous nature of their population (many of whom were recruited from rural areas), and methodological limitations relating to the spirometric device used, which precluded the type of quality control undertaken for the current study. Interestingly, ethnic differences in FEV1 and FVC also tended to be proportional in the PURE study, suggesting reduced lung size when compared with North American subjects, without specific evidence of airway obstruction.
Clinical Significance of Findings
An understanding of factors determining the growth, development, and loss of lung function is important for formulation of strategies to prevent respiratory disease. There is evidence that individuals with lower SEC during childhood subsequently have lower levels of adult pulmonary function than those with a more privileged background (37, 39). Individuals with lower lung function in childhood may attain lower maximal lung function in early adulthood relative to those who attain higher peak values (40–42). Reduced peak pulmonary function and accelerated rate of subsequent pulmonary function decline are risk factors for developing undesirable health conditions, including COPD, cardiovascular disease, and early mortality (43).
In contrast to the stability noted among those of white European descent (44), secular changes in both anthropometry and lung function are likely to be observed in emerging countries/resource-poor areas such as India, which will complicate attempts to separate effects of pre- and postnatal exposures on subsequent lung health, unless results can be related to contemporaneous healthy subjects with the same ethnic ancestry who have had adequate pre- and postnatal nutrition and minimal exposure to environmental pollution (45). Although we were unable to attribute the precise contribution of individual factors to the observed deficit, adjusting for differences in biomass exposure and SEC only partly explained the observed differences in lung function between urban and rural children, suggesting that other factors, such as poor pre- and postnatal nutrition and early life events, may play a significant role. Our findings have important public health implications, and a longitudinal study, ideally commencing antenatally, will be required to disentangle these relationships to inform health policies on modifiable risk factors.
The similarity between groups with respect to mean FEV1/FVC in this study would suggest that differences in lung function were primarily due to smaller lungs rather than reflecting airway obstruction or lung disease among the less advantaged groups. Within any particular group, the relationship between z FEV1 and z FVC remained constant across the age range studied, with both sexes displaying similar patterns. There was, however, a marked increase in between-subject variability for FEV1/FVC among the rural Indian children (the SD for which was 28% higher than expected for a normal population; Table 2), with an increased proportion of such children having either elevated or diminished values, which fell outside the 95% range of normality (as depicted by ± 2 z scores, Figure 3). It has been reported that Indian children with the lowest SEC, in whom short stature and low BMI provides evidence of stunted growth, produce the highest FEV1/FVC ratios (46). Both pre- and postnatal nutrition will impact both somatic and lung growth. Although interpretation of results in this study is limited due to the lack of any reliable data on either birth weight or subsequent growth patterns, findings of an elevated FEV1/FVC in at least some of the rural children suggests that shorter stature, whether due to stunted growth or developmental differences, may affect vital capacity disproportionately. This in turn could potentially confound attempts to identify the impact of biomass exposure in such children, in whom a much more marked relative fall in FEV1 would be needed before the reduction in FEV1/FVC became indicative of any degree of airway obstruction. These factors, including the impact of increased heterogeneity on power of study, need to be borne in mind when designing intervention trials aimed at improving either nutrition or biomass exposure in such populations.
In conclusion, marked differences in SEC and nutritional status within an ethnically similar population are associated with significant differences in lung function during childhood. Although the precise causes and potential long-term implications have yet to be established, the average reductions in lung function in rural Indian children, which are additional to the ethnic differences observed among healthy well-nourished children, must be taken into account when assessing “ethnic differences” in lung function, establishing ethnic-specific reference data, or undertaking epidemiological studies to investigate risk factors associated with lifelong lung health.
Footnotes
Funded by Wellcome Trust grant WT094129MA (S.S., S.L., A.W., and J.S.) and Asthma UK grant 10/013 (S.S., S.L., and J.S.).
Author Contributions: S.S. conceived the study, performed data collection, performed analysis and interpretation of data, and wrote the manuscript; S.L. and J.S. interpreted data and contributed to the manuscript; J.K., R.B., V.S., P.T.L., B.R., and S.C.N. performed data collection; A.W. interpreted the statistical analysis and contributed to the manuscript. All authors approved the final draft of the manuscript.
This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org
Originally Published in Press as DOI: 10.1164/rccm.201406-1049OC on November 20, 2014
Author disclosures are available with the text of this article at www.atsjournals.org.
References
- 1.World Health OrganizationWorld Health Statistics 2008. World Health Organization2008[accessed 2014 May 22]. Available from: http://www.who.int/gho/publications/world_health_statistics/EN_WHS08_Full.pdf [Google Scholar]
- 2.Stocks J, Hislop A, Sonnappa S. Early lung development: lifelong effect on respiratory health and disease. Lancet Respir Med. 2013;1:728–742. doi: 10.1016/S2213-2600(13)70118-8. [DOI] [PubMed] [Google Scholar]
- 3.Barker DJ, Godfrey KM, Fall C, Osmond C, Winter PD, Shaheen SO. Relation of birth weight and childhood respiratory infection to adult lung function and death from chronic obstructive airways disease. BMJ. 1991;303:671–675. doi: 10.1136/bmj.303.6804.671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Edwards CA, Osman LM, Godden DJ, Campbell DM, Douglas JG. Relationship between birth weight and adult lung function: controlling for maternal factors. Thorax. 2003;58:1061–1065. doi: 10.1136/thorax.58.12.1061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lawlor DA, Ebrahim S, Davey SG. Association between self-reported childhood socioeconomic position and adult lung function: findings from the British Women’s Heart and Health Study. Thorax. 2004;59:199–203. doi: 10.1136/thorax.2003.008482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Stein CE, Kumaran K, Fall CH, Shaheen SO, Osmond C, Barker DJ. Relation of fetal growth to adult lung function in south India. Thorax. 1997;52:895–899. doi: 10.1136/thx.52.10.895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lawlor DA, Ebrahim S, Davey SG. Association of birth weight with adult lung function: findings from the British Women’s Heart and Health Study and a meta-analysis. Thorax. 2005;60:851–858. doi: 10.1136/thx.2005.042408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Quanjer PH. Lung function, race and ethnicity: a conundrum. Eur Respir J. 2013;41:1249–1251. doi: 10.1183/09031936.00053913. [DOI] [PubMed] [Google Scholar]
- 9.Strippoli MP, Kuehni CE, Dogaru CM, Spycher BD, McNally T, Silverman M, Beardsmore CS. Etiology of ethnic differences in childhood spirometry. Pediatrics. 2013;131:e1842–e1849. doi: 10.1542/peds.2012-3003. [DOI] [PubMed] [Google Scholar]
- 10.Whitrow MJ, Harding S. Ethnic differences in adolescent lung function: anthropometric, socioeconomic, and psychosocial factors. Am J Respir Crit Care Med. 2008;177:1262–1267. doi: 10.1164/rccm.200706-867OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Harik-Khan RI, Muller DC, Wise RA. Racial difference in lung function in African-American and White children: effect of anthropometric, socioeconomic, nutritional, and environmental factors. Am J Epidemiol. 2004;160:893–900. doi: 10.1093/aje/kwh297. [DOI] [PubMed] [Google Scholar]
- 12.Duong M, Islam S, Rangarajan S, Teo K, O’Byrne PM, Schunemann HJ, Igumbor E, Chifamba J, Liu L, Li W, et al. Global differences in lung function by region (PURE): an international, community-based prospective study. Lancet Respir Med. 2013;1:599–609. doi: 10.1016/S2213-2600(13)70164-4. [DOI] [PubMed] [Google Scholar]
- 13.Brehm JM, Acosta-Perez E, Klei L, Roeder K, Barmada MM, Boutaoui N, Forno E, Cloutier MM, Datta S, Kelly R, et al. African ancestry and lung function in Puerto Rican children. J Allergy Clin Immunol. 2012;129:1484–1490. doi: 10.1016/j.jaci.2012.03.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kumar R, Seibold MA, Aldrich MC, Williams LK, Reiner AP, Colangelo L, Galanter J, Gignoux C, Hu D, Sen S, et al. Genetic ancestry in lung-function predictions. N Engl J Med. 2010;363:321–330. doi: 10.1056/NEJMoa0907897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Donnelly PM, Yang TS, Peat JK, Woolcock AJ. What factors explain racial differences in lung volumes? Eur Respir J. 1991;4:829–838. [PubMed] [Google Scholar]
- 16.Massey DG, Fournier-Massey G. Japanese-American pulmonary reference values: influence of environment on anthropology and physiology. Environ Res. 1986;39:418–433. doi: 10.1016/s0013-9351(86)80066-4. [DOI] [PubMed] [Google Scholar]
- 17.Fulambarker A, Copur AS, Cohen ME, Patel M, Gill S, Schultz ST, Quanjer PH. Comparison of pulmonary function in immigrant vs US-born Asian Indians. Chest. 2010;137:1398–1404. doi: 10.1378/chest.09-1911. [DOI] [PubMed] [Google Scholar]
- 18.Singh GK, Siahpush M. Widening rural-urban disparities in life expectancy, US, 1969–2009. Am J Prev Med. 2014;46:e19–e29. doi: 10.1016/j.amepre.2013.10.017. [DOI] [PubMed] [Google Scholar]
- 19.Pradhan J, Arokiasamy P. Socio-economic inequalities in child survival in India: a decomposition analysis. Health Policy. 2010;98:114–120. doi: 10.1016/j.healthpol.2010.05.010. [DOI] [PubMed] [Google Scholar]
- 20.Budhiraja S, Singh D, Pooni PA, Dhooria GS. Pulmonary functions in normal school children in the age group of 6–15 years in north India. Iran J Pediatr. 2010;20:82–90. [PMC free article] [PubMed] [Google Scholar]
- 21.Glew RH, Kassam H, Vander VJ, Agaba PA, Harkins M, VanderJagt DJ. Comparison of pulmonary function between children living in rural and urban areas in northern Nigeria. J Trop Pediatr. 2004;50:209–216. doi: 10.1093/tropej/50.4.209. [DOI] [PubMed] [Google Scholar]
- 22.Sonnappa S, Lum S, Wade A, Subramanya V, Lakshman PT, Rajan B, Nooyi SC, Stocks J. Disparate lung function in healthy children across the Indian urban–rural continuum [abstract] Am J Respir Crit Care Med. 2014;189:A3228. doi: 10.1164/rccm.201406-1049OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lum S, Sonnappa S, Wade A, Harding S, Wells J, Trelevan P, Cole TJ, Griffiths C, Kelly F, Bonner R, et al. London, UK: UCL Institute of Child Health; 2014. Exploring ethnic differences in lung function: the Size and Lung function In Children (SLIC) study protocol and feasibility. [Google Scholar]
- 24.Currie CE, Elton RA, Todd J, Platt S. Indicators of socioeconomic status for adolescents: the WHO Health Behaviour in School-aged Children Survey. Health Educ Res. 1997;12:385–397. doi: 10.1093/her/12.3.385. [DOI] [PubMed] [Google Scholar]
- 25.Khadilkar VV, Khadilkar AV, Cole TJ, Sayyad MG. Crosssectional growth curves for height, weight and body mass index for affluent Indian children, 2007. Indian Pediatr. 2009;46:477–489. [PubMed] [Google Scholar]
- 26.Kirkby J, Welsh L, Lum S, Fawke J, Rowell V, Thomas S, Marlow N, Stocks J. The EPICure study: comparison of pediatric spirometry in community and laboratory settings. Pediatr Pulmonol. 2008;43:1233–1241. doi: 10.1002/ppul.20950. [DOI] [PubMed] [Google Scholar]
- 27.Quanjer PH, Stanojevic S, Cole TJ, Baur X, H/all GL, Culver B, Enright PL, Hankinson JL, Ip MS, Zheng J, et al. Multi-ethnic reference values for spirometry for the 3–95 year age range: the global lung function 2012 equations. Eur Respir J. 2012;40:1324–1343. doi: 10.1183/09031936.00080312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kirkby JC, Lum S, Stocks J, Bonner R, Sonnappa S. Adaptation of the GLI- 2012 spirometry reference equations for use in Indian children [abstract] Eur Respir J. 2014;43:191. [Google Scholar]
- 29.Chalasani S. Understanding wealth-based inequalities in child health in India: a decomposition approach. Soc Sci Med. 2012;75:2160–2169. doi: 10.1016/j.socscimed.2012.08.012. [DOI] [PubMed] [Google Scholar]
- 30.Jackson BE, Coultas DB, Suzuki S, Singh KP, Bae S. Rural-urban disparities in quality of life among patients with COPD. J Rural Health. 2013;29:s62–s69. doi: 10.1111/jrh.12005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Demissie K, Ernst P, Hanley JA, Locher U, Menzies D, Becklake MR. Socioeconomic status and lung function among primary school children in Canada. Am J Respir Crit Care Med. 1996;153:719–723. doi: 10.1164/ajrccm.153.2.8564123. [DOI] [PubMed] [Google Scholar]
- 32.Raven PB, Taguchi S, Drinkwater BL, Kaneko M, Horvath SM, Matsui H. Anthropometric, spirometric, and physiologic comparisons of migrant Japanese. Hum Biol. 1974;46:483–494. [PubMed] [Google Scholar]
- 33.Korotzer B, Ong S, Hansen JE. Ethnic differences in pulmonary function in healthy nonsmoking Asian-Americans and European-Americans. Am J Respir Crit Care Med. 2000;161:1101–1108. doi: 10.1164/ajrccm.161.4.9902063. [DOI] [PubMed] [Google Scholar]
- 34.Bonner R, Lum S, Stocks J, Kirkby J, Wade A, Sonnappa S. Applicability of the global lung function spirometry equations in contemporary multiethnic children. Am J Respir Crit Care Med. 2013;188:515–516. doi: 10.1164/rccm.201212-2208LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Loeb JS, Blower WC, Feldstein JF, Koch BA, Munlin AL, Hardie WD. Acceptability and repeatability of spirometry in children using updated ATS/ERS criteria. Pediatr Pulmonol. 2008;43:1020–1024. doi: 10.1002/ppul.20908. [DOI] [PubMed] [Google Scholar]
- 36.Panagariya A, Mukim M. A comprehensive analysis of poverty in India. Asian Dev Rev. 2014;31:1–52. [Google Scholar]
- 37.Raju PS, Prasad KV, Ramana YV, Balakrishna N, Murthy KJ. Influence of socioeconomic status on lung function and prediction equations in Indian children. Pediatr Pulmonol. 2005;39:528–536. doi: 10.1002/ppul.20206. [DOI] [PubMed] [Google Scholar]
- 38.Tai A, Tran H, Roberts M, Clark N, Wilson J, Robertson CF. The association between childhood asthma and adult chronic obstructive pulmonary disease. Thorax. 2014;69:805–810. doi: 10.1136/thoraxjnl-2013-204815. [DOI] [PubMed] [Google Scholar]
- 39.Jackson B, Kubzansky LD, Cohen S, Weiss S, Wright RJ. A matter of life and breath: childhood socioeconomic status is related to young adult pulmonary function in the CARDIA study. Int J Epidemiol. 2004;33:271–278. doi: 10.1093/ije/dyh003. [DOI] [PubMed] [Google Scholar]
- 40.Stern DA, Morgan WJ, Wright AL, Guerra S, Martinez FD. Poor airway function in early infancy and lung function by age 22 years: a non-selective longitudinal cohort study. Lancet. 2007;370:758–764. doi: 10.1016/S0140-6736(07)61379-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sears MR, Greene JM, Willan AR, Wiecek EM, Taylor DR, Flannery EM, Cowan JO, Herbison GP, Silva PA, Poulton R. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003;349:1414–1422. doi: 10.1056/NEJMoa022363. [DOI] [PubMed] [Google Scholar]
- 42.Phelan PD, Robertson CF, Olinsky A. The Melbourne Asthma Study: 1964–1999. J Allergy Clin Immunol. 2002;109:189–194. doi: 10.1067/mai.2002.120951. [DOI] [PubMed] [Google Scholar]
- 43.Griffith KA, Sherrill DL, Siegel EM, Manolio TA, Bonekat HW, Enright PL. Predictors of loss of lung function in the elderly: the Cardiovascular Health Study. Am J Respir Crit Care Med. 2001;163:61–68. doi: 10.1164/ajrccm.163.1.9906089. [DOI] [PubMed] [Google Scholar]
- 44.Quanjer PH, Stocks J, Cole TJ, Hall GL, Stanojevic S. Influence of secular trends and sample size on reference equations for lung function tests. Eur Respir J. 2011;37:658–664. doi: 10.1183/09031936.00110010. [DOI] [PubMed] [Google Scholar]
- 45.Mukhopadhvay S, Macleod KA, Ong TJ, Ogston SA. “Ethnic” variation in childhood lung function may relate to preventable nutritional deficiency. Acta Paediatr. 2001;90:1299–1303. doi: 10.1080/080352501317130362. [DOI] [PubMed] [Google Scholar]
- 46.Quanjer PH, Stanojevic S, Stocks J, Hall GL, Prasad KV, Cole TJ, Rosenthal M, Perez-Padilla R, Hankinson JL, Falaschetti E, et al. Changes in the FEV/FVC ratio during childhood and adolescence: an intercontinental study. Eur Respir J. 2010;36:1391–1399. doi: 10.1183/09031936.00164109. [DOI] [PubMed] [Google Scholar]