

Abstract
Context:
Athletic trainers have traditionally conceptualized rehabilitation programs in terms of 3 distinct physiologic phases; however, these phases appear to neglect athletes' psychosocial responses to their injuries.
Objective:
To document injured athletes' psychosocial responses during the different phases of injury rehabilitation.
Design:
Qualitative study.
Setting:
National Collegiate Athletic Association Division II university in the mid-Atlantic region of the United States.
Patients or Other Participants:
A total of 8 previously injured athletes (4 men and 4 women) participated in the study.
Data Collection and Analysis:
We collected participant data by using semistructured interviews, transcribed verbatim and analyzed by directed content analysis. Established themes were triangulated to determine trustworthiness.
Results:
Initially, athletes' cognitive appraisals were predominately negative in nature, leading to negative emotions. These appraisals changed after diagnosis and when moving to the reaction-to-rehabilitation phase and the reaction-to-sport phase. During the reaction-to-rehabilitation phase, athletes reported mixed cognitive appraisals and identified frustration as the main emotional response. When returning to sport, athletes reflected on the lessons learned, yet they expressed some doubts related to their ability to return to play. These cognitive appraisals served as a precursor to the resulting emotional responses of nervousness and reinjury anxiety, as well as excitement. Throughout the various phases of rehabilitation, athletes reported seeking out social support: initially from significant others and then from their athletic trainers during the reaction-to-rehabilitation phase.
Conclusions:
The results appear to support the use of the integrated model of psychological response to sport injury and the rehabilitation process and the 3 phases of rehabilitation as a framework for understanding how physical and psychosocial factors may interact during sport-injury rehabilitation. Understanding this interaction may help athletic trainers provide better care to their injured athletes.
Key Words: cognitive appraisals, emotional and behavioral responses, integrated model, sport psychology, rehabilitation stages
Key Points
Injured athletes' cognitive appraisals and emotional and behavioral responses varied during the different phases of the injury-rehabilitation process.
Understanding how athletes' psychosocial responses interact during the different phases of rehabilitation can help athletic trainers better understand how an athlete might react during the injury-rehabilitation process.
Athletic trainers (ATs) have traditionally conceptualized rehabilitation programs in terms of 3 distinct physiologic phases: acute injury phase, repair phase, and remodeling phase.1 According to Prentice and Arnheim,1 these phases, which are based on the 3 stages of the healing process, provide ATs with a potential blueprint for guiding treatment, using modalities, and implementing rehabilitation exercises. Although the use of these 3 stages has proven to be effective in facilitating injured athletes' physical return to the field of play, athletes' psychosocial responses to their injuries have not been considered. Indeed, evidence collected from ATs indicates that they appear to recognize the prevalence of psychosocial responses to athletic injuries, but their lack of education on how to appropriately deal with these responses limits their ability to properly incorporate athletes' reactions into their treatment plans and thereby provide holistic care.2
Recently Kamphoff et al3 suggested a variation of the phase-like approach to rehabilitation by integrating psychosocial components with physical characteristics of the healing process: reaction to injury, reaction to rehabilitation, and reaction to return to sport.3 The development of these phases, guided by the physical healing process, has the potential to increase ATs' ability to provide holistic care to injured athletes. According to Kamphoff et al,3 use of this phased approach could help ATs develop and implement psychosocial strategies to address some of the psychosocial challenges athletes may encounter during the recovery process.
Typically, injured athletes experience a range of psychosocial challenges, which may vary during the course of the recovery process. For example, Johnston and Carroll4 found that during the early stages of rehabilitation, athletes often exhibited frustration and depression due to their sudden lack of sport involvement. As they moved into the middle stages of their rehabilitation programs, some athletes experienced apathy and poor adherence (ie, doing too much or too little), which could be a result of lack of motivation to complete the required rehabilitation exercises or a sign of impatience and eagerness to return to sport. Tracey5 reported that injured athletes also experienced a variety of psychosocial challenges throughout the recovery process, including but not limited to decreased self-esteem, frustration, anger, and fear of injury. Kamphoff et al,3 in developing the phased approach, indicated that each of the stages in their phase-like approach is associated with specific psychosocial challenges. More specifically, during the reaction-to-injury phase, athletes often experience anxiety and negative cognitive appraisals. In the reaction-to-rehabilitation phase, injured athletes may be faced with motivational challenges. Finally, in the reaction-to-return-to-play phase, athletes may encounter self-confidence concerns and fears or anxiety about the possibility of reinjury. Sport-injury rehabilitation is clearly a dynamic and evolving process during which athletes' psychosocial responses vary.
Although Kamphoff et al3 suggested a shift toward approaching rehabilitation from both the physical and psychosocial perspectives, research in this area is still limited. However, the integrated model of response to the sport injury and rehabilitation process6 provides theoretical support to the phased approach, thus validating the importance of addressing athletes' psychosocial responses for successful recovery. According to the integrated model,6 athletes can respond to their injuries in a variety of ways, and a number of preinjury factors (eg, personality, coping resources, and previous history of stressors) can influence not only injury occurrence but also subsequent reactions to injury. In short, the integrated model6 suggests that once injured, the athlete will often experience a range of thoughts, emotions, and feelings, which may have an effect on the athlete's behavior and vice versa (eg, behaviors can affect emotions, and emotions can affect cognitions). Moreover, these responses are all influenced by a range of personal (eg, individual differences) and situational (eg, sports medicine team influences) factors.6
The integrated model6 highlights the importance of being knowledgeable about injured athletes' psychosocial responses to injury, yet this concept has been limited in application to the different phases of injury rehabilitation. Wiese-Bjornstal et al6 postulated that with the application of the integrated model across different phases of rehabilitation (as outlined by Kamphoff et al3), ATs could potentially be more cognizant of athletes' psychosocial responses (ie, cognitive appraisals, emotional and behavioral responses) at each of these phases and be able to take the necessary steps to ensure successful recovery. Furthermore, understanding the theory underpinning psychosocial responses to injury may help ATs promote a more holistic approach in choosing appropriate psychosocial strategies to help athletes proceed through each phase and successfully back to the field of play. As a result, the aim of our study was to explore injured athletes' psychosocial responses (cognitive appraisals, emotional and behavioral responses) to sport injury at the different phases of rehabilitation: reaction to injury, reaction to rehabilitation, and reaction to return to sport.3
METHODS
Research Design
Because our goal was to explore the experiences of injured athletes and more specifically their psychosocial responses as they relate to sport-injury rehabilitation, we adopted a qualitative research design. Using this approach, we were able to focus on the participants' subjective experiences and interpretations of their injury experiences, and as such, to understand the injury experience from an athlete's personal perspective rather than our own. We collected the participants' data using semistructured interviews and analyzed the data using directed content analysis.7
Participants
A convenience sample of 8 (4 male, 4 female) National Collegiate Athletic Association Division II athletes, aged 18 to 22 years, participated in interviews for this study. Each athlete was enrolled at a Division II university in the mid-Atlantic region of the United States and was a current member of a varsity athletic team at that institution (acrobatics and tumbling: n = 4; football, n = 3; baseball, n = 1). Participants reported their class year as freshman (n = 2), junior (n = 4), or senior (n = 2). All of the athletes had suffered an injury that restricted their sport participation for a minimum of 6 weeks in the past year and had since successfully returned to sport within the expected time period required for their injury recovery. The encountered injuries included anterior cruciate ligament reconstruction (n = 3), fractures (n = 3), rotator cuff repair (n = 1), and chondrocyte removal from the elbow (n = 1).
Interview Guide
The framework for the interview guide used in this study was adopted from the integrated model.6 As shown in the Table, the first section contained general questions about the athlete and his or her background. As such, questions like “Could you tell me about yourself?” were used to act as an icebreaker. The following 3 sections were concerned with athletes' cognitive appraisals (ie, how the athlete viewed the situation), emotional responses (ie, how he or she felt about the injury), and behavioral responses to the injury (ie, how he or she acted and reacted to the injury situation) at different phases of rehabilitation (initial reactions, reactions during rehabilitation, and reactions related to return to sport).
Table.
Interview Questions
| Section A: Background |
| 1. Could you tell me about yourself? |
| 2. Could you tell me about your life before or around the time of your injury? |
| 3. Could you tell me about the time when you got injured? |
| Section B: Cognitive and emotional responses |
| 4. Describe your initial thoughts and emotions after sustaining your injury. |
| 5. How did these thoughts and emotions change once you knew about the seriousness and impact of the injury? |
| 6. Could you explain how your injury has affected you? |
| 7. How do you feel you have coped with your injury? |
| 8. How do you feel about your injury now? |
| 9. In your own words, what has been the most challenging aspect of being injured? |
| 10. Could you tell me how you did or how you are coping with that? |
| Section C: Behavioral responses |
| 11. Can you tell me about specific methods or techniques you have used to cope with your injury? |
| 12. When you got injured, who did you turn to for support? |
| 13. Could you tell me about your experiences with that support? |
| 14. Could you tell me about your rehab experience? |
| 15. How did it progress? |
| 16. What was the environment like? |
| 17. Can you tell me anything specific that you feel has helped your recovery? |
| 18. In a similar manner, can you tell me anything specific that you feel has hindered your recovery? |
| Section D: Readiness for return to play |
| 19. Tell me about your goals (life and sport) since sustaining your injury. |
| 20. What are your goals when you return to play? |
| 21. How motivated are you to return to play? |
| 22. What do you miss about participating in your sport? |
| 23. What were/are your thoughts and feelings concerning return to play? |
| 24. How can you use this experience in life and on the playing field? |
Procedure
Before participant recruitment or data collection, we obtained institutional review board approval from West Virginia University. For the study, convenience sampling was used to recruit previously injured athletes who had since recovered from their injuries. Once potential participants were identified, they were approached by 1 of the researchers and given a cover letter explaining the nature of the study and requirements for participation. Those who expressed an interest in taking part were then scheduled for an interview at a convenient time and location for both the researcher and the participant. Interviews took place one on one in a private, quiet room within the athletic facilities of the university and averaged about 55 minutes. Once on location, the researcher explained the nature of the study. The researcher also informed participants about their right not to answer any questions they felt uncomfortable with, that they could deviate from the interview questions when necessary, and of their right to withdraw from the research at any point they chose. They also were informed that to ensure their confidentiality, pseudonyms would be used. Once participants understood the study, and any possible questions had been answered, they were asked to complete, sign, and return the consent form to the researcher. All participants also gave consent for the use of a voice-recording device.
Pilot Interview
We pilot tested the interview guide on club-sport athletes (N = 2) who had since recovered from their injuries. The pilot interviews were conducted to determine if the questions on the interview guide were neutral (ie, not worded to influence answers) and clear (devoid of any scientific or sport psychology terminology) and if the order of the questions flowed well. Furthermore, pilot interviews allowed the interviewer to practice developing follow-up questions and to increase the interviewer's confidence in conducting interviews. Based on the feedback obtained from the pilot interviews, we revised some of the questions, and as a result, slightly modified the order of some questions. Upon the completion of pilot interviews, the interviewer participated in a bracketing interview with a researcher who had qualitative experience. The purpose of this bracketing interview was to allow the interviewer to gain additional insight into her own experiences relative to sport and injuries and to heighten the interviewer's awareness relative to personal biases that might influence the interview process.8,9 Once this bracketing interview was completed, the interviewer reported being prepared to conduct the interviews knowing that her own experiences would not influence the process.
Data Analysis
After the interviews, the recordings were transcribed verbatim by the researcher and stored in a Word (version 97–2003; Microsoft Inc, Redmond, WA) document on a password-protected computer in a locked office. The research team (which consisted of 3 researchers, all of whom were involved in coding and data analysis) randomly selected 1 of the participants, Harry, to initiate the analysis process. What follows is a description of the data-analysis process, which was replicated with all participants until we felt that saturation had been reached.
Initially the data analysis was guided by the integrated model.6 This allowed us to identify any possible cognitive appraisals and emotional and behavioral responses that might have emerged as a result of the injury and during the injury-rehabilitation process, as well as if any personal or situational factors influenced such processes. The analysis was not, however, restricted to the individual factors and responses listed in the integrated model6 but rather open to alternative cognitive appraisals and emotional and behavioral responses that might emerge from the data. After this analysis, we identified such responses to each of the 3 stages of rehabilitation as identified by Kamphoff et al.3 As noted earlier, the phases of rehabilitation acted as a framework to which we added as items emerged from the data.
During the analysis, each researcher identified a number of cognitive appraisals and emotional and behavioral responses to injuries in the participant's responses, which were then placed into the different phases of rehabilitation. After this process, we collated the emergent themes into a master list of themes and quotations from the transcript. This process allowed us to organize consistently across all analyses and to identify commonly occurring themes. These themes were reevaluated for any possible discrepancies and revised when necessary. Once the themes were established, we immersed ourselves in the remaining transcripts and allowed further themes to emerge inductively from the data.
During the analysis, it was evident that participants presented themselves with different cognitive appraisals and emotional and behavioral responses to injuries that were influenced by a range of personal and situational factors. It also became evident that the athletes' reactions to their injuries (phase 1) manifested in 2 distinct phases (initial reaction and reaction after diagnosis), which are not explicitly stated in the 3-stage model. Given the purpose and aim of this study, the emergence of such themes confirmed that we had reached the saturation point, and as such, we were confident that the sample size was sufficient for this study.
The trustworthiness of the data was established by triangulation, peer review, and participant checking.8,10 Triangulation occurred when all members of the research team reviewed the transcripts and coding of emerging themes and supporting quotations to assure interrater reliability and consistency of analysis. An academician with qualitative research experience peer reviewed the themes to ensure they were consistent with the transcripts. Lastly, the findings and themes were explained and discussed with 2 participants to determine if they felt these were representative of their experiences. The participants agreed with the emergent themes and found them to be consistent with their experiences.
RESULTS
With the directed content analysis, we found commonalities in athletes' psychosocial responses to injuries across the 3 phases of rehabilitation. Overall, it appeared that athletes' cognitive appraisals of their injuries and subsequent emotional and behavioral responses varied across the rehabilitation process and were typically influenced by 4 distinct events (ie, initial reaction to injury, reactions to injury after diagnosis, reactions to rehabilitation, and reactions to return to sport). It was also evident that these reactions were influenced by reactions displayed during the earlier phases and by several prominent personal (ie, injury severity, recovery status, perceived length of time to return to sport) and situational (ie, teammate, coach, family, sport medicine professional influences) factors.
Phase 1: Reaction to Injury
Overall, athletes' initial cognitive appraisals of the injury were predominately negative. These had an effect on the subsequent emotional responses, which also were generally negative. Initially, the most common behavioral response was to seek social support from family and significant others. However, once the injury was formally diagnosed, athletes reported changes in their cognitive appraisals and emotional responses. However, seeking social support from family and significant others continued to be the most prominent behavioral response.
More specifically, athletes' initial cognitive appraisals were strongly influenced by the perceived severity of their injuries. In other words, initial cognitive appraisals were influenced by a common theme of perceived injury severity influencing appraisal, in that the more athletes perceived their injury to be severe or expected to be away from their sport for a significant period of time (or both), the more negative their cognitive appraisals were and vice versa. The athletes who initially perceived their injuries as severe typically appraised the injury as negative. For example, Harry reported, “I never really thought that I'd be able to come back out and throw again.” Similarly, Gabby stated, “As soon as it happened, I knew something was definitely wrong, like it was a serious injury. It wasn't a pain I'd ever felt before.” Furthermore, Faith commented, “I knew I was at least done for the year and I didn't really know if I would ever be able to come back.”
Other athletes appeared to hope their injuries were not serious, and as a result appraised the injury more positively. Eric noted, “My initial thoughts, I didn't think it was anything. I just thought I came down on it wrong. I thought it was just sore from the way I landed. I didn't think anything was wrong with it, so I just continued what I was doing.” Anthony explained, “I was just hoping that I could get back so we could have a better chance of winning.”
Athletes' emotional responses were underpinned by a common theme of negative thoughts leading to negative emotions. That is, athletes' initial emotional responses to their injuries also appeared to be negative to varying degrees. In essence, if the athlete had appraised the injury as really serious and devastating, his or her emotional response was also highly negative. For example, both Faith and Gabby, whose initial appraisals of their injuries were very negative, also described very negative emotions. Faith indicated she was hysterical: “I was just a little bit hysterical because I knew I was at least done for the year.” Gabby experienced anger: “Um, afterwards I was angry.” In a similar way, David reported being in shock: “I dropped to the floor in shock just processing”; and Candace, whose initial appraisal was negative, but not catastrophic, explained how she felt: “I was injured and I was just really, really upset.”
The theme that emerged as the most common behavioral response during this phase was seeking social support, particularly from significant others. Some emphasized the importance of the support received from family members. For example, David said, “I first turned to my family and asked them for advice.” Similarly, Candace indicated, “My mom and the rest of my family provided me with support.” Other athletes sought support from their teammates. For example, Beverly stated, “Umm I turned to my teammates,” and Harry explained, “I would probably say I turned to my teammates.” Some even reported receiving social support from their coaches, as Anthony remarked: “My coaches, they would call me and asked where I was at or ask me how the treatment was.” Similarly, Gabby noted, “I had a lot of support from my coach.” At the initial reaction-to-injury stage, only Beverly (“The [athletic] trainers, um, helped me to kinda get through everything”) and David (“With the support of the [athletic] trainers, they helped comfort me”) listed receiving and seeking social support from their ATs. The key responses to injuries immediately after injury are displayed in Figure 1.
Figure 1.
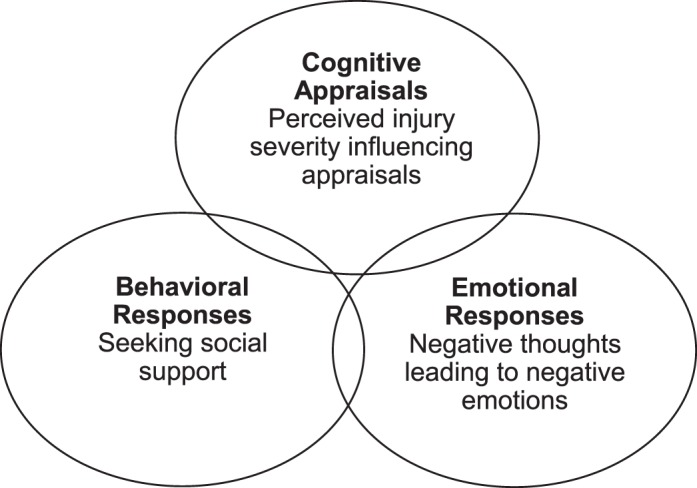
Initial psychosocial responses to injury immediately after injury.
Subsequent to initial reactions to injuries, a theme that emerged from the data was cognitive reappraisals after diagnosis. It appeared that after the initial reactions to the injury, the first major point of change in the initial appraisals was after diagnosis. That is, once athletes were fully aware of the injury severity (a personal factor), their initial response to injury changed depending on the diagnosis. In some cases, the news of the diagnosis fostered a positive outlook on the situation. Eric, for example, who had initially perceived the injury as minor, indicated, “I was glad it was the end of the season because I knew something was going to have to happen medical-wise, so I was just glad that it was the end of the season so I could focus on my shoulder.” Others expressed similar thoughts, such as Gabby, who stated, “I knew it was going to be a long recovery and I didn't want to waste that time not cheering.” After her diagnosis, Beverly reported, “I knew I could get back for my senior season.” Not all athletes reappraised their injury situation as positive. Anthony expressed negative thoughts: “I felt that I was letting everybody down.” David viewed his situation as a challenge: “I knew that it was a test that I had to pass. Everyone goes through tests and I felt that this was one of them.”
The knowledge of the diagnosis also affected athletes' resultant emotional responses: a common theme of knowing the severity changed emotions was evident in all of the participants' transcripts. Anthony commented that knowing the severity of the injury “made me real upset because I felt like I was letting my team down.” Harry stated it “kinda made, like, my emotions worse.” In a similar manner, Beverly indicated that she went through a “week of depression,” and “for a full solid week, I probably cried nonstop.” Candace reported, “I think I became, like, just really down about myself and about the sport that I was doing.” For some athletes, knowledge of the injury severity brought about different emotions. For example, Faith noted, “I thought everything was going to be torn, and then it was just my ACL [anterior cruciate ligament], and I felt a little bit better about it.” Eric, on the other hand, reported, “It didn't affect me emotionally that much.”
It also appeared that after diagnosis, the theme of seeking social support from a range of sources, particularly significant others, remained the most dominant behavioral response. Eric, who appeared to appraise his injury in a positive manner, said that his mother was the greatest source of support: “My mom is always there when I need support for anything…She would come out to the doctors' appointments and stuff to see how serious it was…It was mainly her; after surgery, I stayed with her. She took care of me.” The key responses to injuries after injury diagnosis are illustrated in Figure 2.
Figure 2.
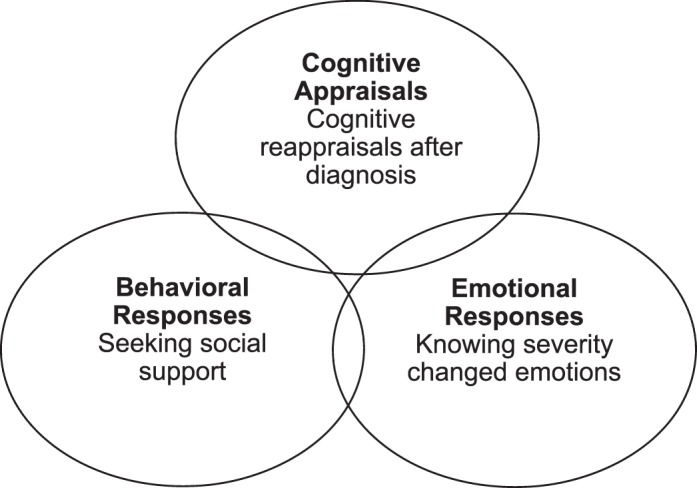
Psychosocial responses to injury postdiagnosis.
Phase 2: Reaction to Rehabilitation
Moving from the reaction to injury to the reaction-to-rehabilitation phase, overall, athletes described varying cognitive appraisals that were mainly concerned with thoughts questioning the rehabilitation process. The most common emotional response to rehabilitation was frustration. Athletes also indicated being cautious about the rehabilitation and continued to seek social support from family and significant others. However, during rehabilitation, they also sought social support from the ATs.
More specifically, during the reaction-to-rehabilitation phase, the emergent theme in athletes' cognitive appraisals was characterized by thoughts that question the rehabilitation process. At the start of rehabilitation, it appeared that athletes' cognitive appraisals of their rehabilitation were mixed and underpinned with thoughts about the perceived value of their rehabilitation programs, their willingness to get on with the process, and the perceived difficulty of these programs. Anthony stated, “I mean it's good…[to] see their aspects on what they think is wrong with me, and it's just cool seeing how there's so many different things that can affect your body. They know exactly what to do to get you better.” Beverly's and Candace's cognitive appraisals of their rehabilitation were influenced by their willingness to get on with the process. Beverly indicated, “I loved to look forward to come to rehab. It gives me something to look forward to each day.” Similarly, Candace reported, “I'm just gonna push through it, and something bigger and better is gonna come along.” Other athletes' cognitive appraisals were influenced by the perceived difficulty of the rehabilitation programs. For example, David stated, “I didn't think I was going to make it.” Faith expressed similar thoughts: “After surgery, the rehab part was hard.”
Such mixed thoughts on the rehabilitation process resulted in changes in emotional responses. In the reaction-to-rehabilitation phase, the emergent theme among the athletes was feeling frustrated. Most notably, Gabby explained, “I definitely got frustrated, frustrated when I first started to walk again. I was frustrated that my weight was down.” Harry also reported feelings of frustration: “I said starting out, you know, because all you're doing is 2-pound weights, or just arm exercises where it's no weights or just bands or something, so it's frustrating because you can't lift any weights. You know your arm feels so weak.” Other athletes also expressed similar feelings. Beverly said, “Not being able to do what you were doing right before you tore it and kind of having, like, people having to pick up your leg for you isn't really the best feeling.” Faith indicated feeling frustrated, as evidenced by her comment that “it was just a sad thing when you couldn't even bend your leg, when it was something that you never really thought about before.”
These feelings of frustration could have influenced the ways in which the athletes reacted behaviorally to the rehabilitation. The first emergent theme in the reaction-to-rehabilitation phase was being cautious. For example, Anthony reported, “I mean at first it started off slow.” Beverly shared Anthony's approach: “I started off slow and then within a couple weeks, I began progressing more and more.” Eric indicated he “just took it day by day,” and Gabby stated, “You just have to take baby steps, a little at a time really.” Candace's approach to her rehabilitation was comparable: “At first I was hesitant.”
Very similar to the aforementioned phases, during the reaction-to-rehabilitation phase, the theme seeking and receiving social support was evident. All the athletes reported receiving good social support during rehabilitation. For Candice and Beverly, their family and friends continued to be the main source of support. Candace recalled,
I'd go home every weekend, and they'd (mainly, my parents, my family) comfort me and I'd tell them about everything throughout the process of being injured like the treatment, everything I would explain it all to them [and] they could comfort me.
However, it appeared that during the reaction-to-rehabilitation phase, the role of sports medicine professionals as a source of social support became amplified. Of the athletes in this study, all but Candace indicated that the social support they received from their sports medicine professional was vital for their rehabilitation and recovery. Anthony commented that his sport medicine professionals “helped me to stay positive; they pushed me to work hard and helped me to see the bigger picture.” Moreover, during the rehabilitation stage, social support from coaches and teammates was imperative to some athletes, as “they know what you are going through” and they are “always there for you” (Harry). Harry also noted, “They (the coaches) would talk to me every day after practice…and ask how my rehab was going.…They had faith in me to rehab and come back strong…and that gave me faith in myself.” The key responses to injuries during rehabilitation are shown in Figure 3.
Figure 3.
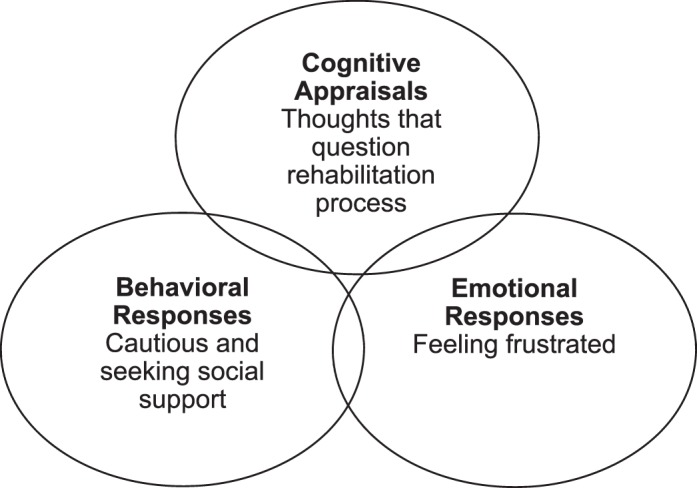
Psychosocial responses to rehabilitation.
Phase 3: Reaction to Return to Sport
During the reaction-to-return-to-sport phase, athletes reported both positive and negative cognitive appraisals. These cognitive appraisals served as precursors to their emotional responses because the athletes described feelings of nervousness and reinjury anxiety, as well as positive excitement. Such feelings were also reflected in their behavioral responses, as the athletes described cautiousness in their actions as they returned to play.
In particular, during the return-to-sport phase, it appeared that all of the athletes in this study had gained perspective as a result of the injury and rehabilitation process. This seemed to manifest itself as an overall theme of lessons learned, which was characterized by personal reflections on having learned a lesson during the process of dealing with their injuries and the rehabilitation process. For example, Harry stated that the injury had made him “love the game more because I realize, you know, at any moment, it can be taken away.” Anthony reported that being injured “kinda made me stronger in a sense because I had to battle through that adversity.” David believed that after injury, he gained “an appreciation for the simplicity of just having all of your body parts.” Gabby observed that as a result of her injury, “It makes me work harder. It makes me stay stronger because I know how easily things like that happen.”
Although lessons learned appeared to be a general theme in athletes' cognitive appraisals regarding their return to play, negative appraisals were also present. Beverly said, “I wasn't sure of how my knee could hold up since I do, do a really contact sport. I do a lot on my knee, um, I wasn't sure how it could hold up.” Faith also expressed a similar sentiment: “It made me more cautious about what I do, and I see things now like this, this, and this can happen, whereas before I could have cared less before I did that.”
Subsequent to the above cognitive appraisals, feelings of excitement and reinjury anxiety was a common theme among the emotional responses during the return-to-sport phase. Some athletes were very excited about returning to sport, whereas others felt insecure about their abilities to return to sport and the possibility of reinjuring themselves. Gabby commented, “I was just anxious to be back, excited.” David was really “excited to see what we can do as a team,” and Eric felt that “it was real exciting to get back. I just wanted to have fun and do what I could do.” Conversely, Beverly was “a little nervous to just, um, jump back into it.” Candace had a similar feeling, being afraid that doing the same buildup that hurt her in the first place was going to injure her again.
These cognitive appraisals and emotional responses acted as a foundation for athletes' behavioral responses, in that they predominately reported being “cautious in their return to play.” For example, Anthony indicated, “It just caused me to be more cautious and look at the little things more than the big things.” Beverly planned a similar approach, as she said, “I know I'll take it slow, and I know that my coach will let me take it slow at first.” Candace reported, “I had to be really careful 'cause I didn't want to be out any longer.” Similarly, Faith said, “I knew that I was going to be able to pace myself. I wasn't going to be pushed to do something that I wasn't ready to do.” The key responses to injuries during return to sport are displayed in Figure 4.
Figure 4.
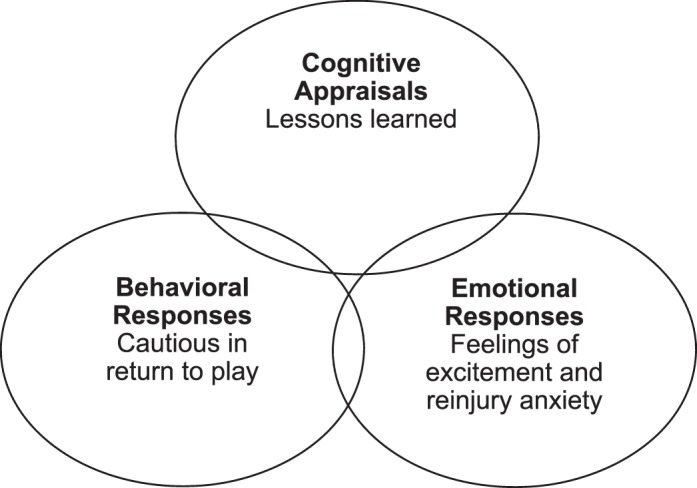
Psychosocial responses to return to sport.
DISCUSSION
Overall, it appeared that injured athletes' cognitive appraisals and emotional and behavioral responses varied during the different phases of the injury-rehabilitation process. These cognitive appraisals and emotional and behavioral responses seemed to evolve in a cyclical manner and were distinct at each of the phases of rehabilitation and recovery. In other words, athletes' psychosocial responses during the different phases of rehabilitation, as identified by Kamphoff et al,3 were influenced by earlier responses.
Athletes' psychosocial responses to injury, rehabilitation, and return to sport appeared to follow clear themes throughout the rehabilitation process. More specifically, athletes' initial cognitive appraisals of their injuries were predominately negative in nature and primarily influenced by perceived severity and ability to return to sport. Such thoughts seemed to influence the resulting emotional responses, which also were generally negative, including being upset, angry, in shock, and hysterical. The most common behavioral response athletes exhibited in this early stage of the injury process was to seek social support from their significant others. Significant others in this instance varied from family members to teammates, coaches, and to a lesser extent, ATs. Such findings are not surprising. Existing literature indicates that injured athletes typically report negative thoughts at injury onset5,11 and that these negative thoughts can often lead to negative emotions.4,12–14 Moreover, the resulting behavioral responses were also consistent with previous research findings, which typically indicated that injured athletes often gravitated toward their significant others for social support.11,14 However, more recently, Yang et al15 found that athletes, once injured, tended to seek social support from their ATs and physicians, as opposed to significant others such as family members and teammates. This finding might have been influenced by the different settings in which the studies were conducted. Yang et al15 collected their data at a Division I university, whereas we collected our data at a Division II university. The differences in access to and structure of sport medical services between Division I and II universities may have accounted for the fact that athletes in the study by Yang et al15 sought social support primarily from their ATs and physicians instead of from family and significant others. Typically, Division I universities have large sports medicine staffs, whereas smaller Division II universities may lack such services. Therefore, athletes in our study may have gravitated toward their family and significant others for social support because of AT and physician staff shortages and the increased demands on those who were available.
After initial reactions to injury, the next significant stage when psychosocial responses were easily identifiable and likely to change from initial responses was after diagnosis. In this study, the athletes reported changes in their cognitive appraisals and heightened emotional responses as a result of their diagnoses. That is, some athletes indicated that knowing the severity of their injuries fostered a positive outlook on the situation, whereas others expressed negative thoughts or viewed the situation as a challenge they needed to overcome. Furthermore, knowledge of their diagnoses amplified some of the previously reported negative emotions (ie, being upset, angry, in shock). Athletes also still sought social support, with the primary source continuing to be their significant others.
These findings appear to be consistent with previous literature, as Leddy et al12 affirmed that the greatest fluctuations in mood as a result of injury occurred in the initial stages of the injury-recovery process. Udry16 further commented that mood fluctuations were often more pronounced in the earlier stages of the injury process than in the later stages. The importance of the diagnosis as a point at which initial responses to injuries are reevaluated and changed has also been supported by Johnston and Carroll.4 They found that injured athletes who initially presented with a positive cognitive appraisal often reported feelings of belief and encouragement after diagnosis; however, those with negative appraisals as a result of their diagnoses reported negative emotions such as shock, disbelief, anger, and confusion.
After the initial reaction-to-injury phase, we found that once athletes transitioned into injury rehabilitation, their cognitive appraisals varied and often contained both positive and negative thoughts. These thoughts were primarily influenced by the perceived value of the rehabilitation programs, their personal willingness to get on with the process, and the perceived difficulty of these programs. The most common emotional reaction to rehabilitation appeared to be frustration. Consistent with the earlier phases of the rehabilitation process, athletes continued to report seeking social support as their main behavioral response. However, unlike during the earlier phases, they now appeared to seek social support from their ATs, as opposed to their significant others alone. Another dominant behavioral response reported by athletes in this phase was the tendency to adopt a hesitant and cautious approach to their rehabilitation programs.
In support, Johnston and Carroll4 agreed that cognitive appraisals during the actual rehabilitation process could be a mixture of positive or negative appraisals and that these appraisals can play a significant role in the resulting emotions and behavioral responses. Johnston and Carroll4 found that those athletes who had a positive appraisal of their injury rehabilitation reported being happy and relieved, and these emotions fostered increased adherence. However, as revealed in our study, those who had negative appraisals reported frustration, which may have led to hesitancy and cautiousness toward their rehabilitation programs. Moreover, this hesitancy and cautiousness could have also been directly related to the subsequent negative cognitive appraisals and their resulting emotions.
Previous research14 also supports the transition to seek social support from ATs in place of significant others. Carson and Polman14 identified “a change in the importance of social support, moving away from the family and becoming more focused on the staff in charge of rehabilitation.” Yang et al15 reported that injured athletes often perceived that ATs and physicians could better help them deal with the stress associated with injury and provide them with the necessary guidance regarding their rehabilitation when compared with significant others. Moreover, their unique understanding and ability to relate to injured athletes, coupled with their capacity to provide emotional and informational support, could also have been responsible for the shift.
Similar to earlier phases, in the return-to-sport phase of the injury process, athletes continued to report both positive and negative cognitive appraisals. Many athletes reflected on the lessons learned as a result of the injury process and were grateful for the opportunity to be able to play their sport again. At the same time, they expressed some doubts related to their return to play. For some, these thoughts were more unidirectional—they were either appreciative of the ability to play again or they felt doubtful about their readiness to return to play. These cognitive appraisals served as precursors to their emotional responses, and as such, athletes described feelings of nervousness, reinjury anxiety, and positive excitement. Finally, similar to the behaviors during the rehabilitation phase, the athletes expressed being cautious in their return to play.
The notion that athletes reflected on their injury as a lesson learned appears to be supported in the literature.5,17–19 For example, Tracey5 stated that when injured, athletes often reflected on their injuries, and that doing so enabled them to learn about “oneself, inner strength and commitment, and learning not to take being healthy for granted.” Although the participants' experiences of lessons learned have been supported in the literature, so has their tendency to report doubts about their ability to return to play.20–22 Additionally, previous research17–21 provides more support for the emotional response of fear of reinjury when compared with the emotion of excitement, as noted by some athletes in the current sample. The resulting behavioral response, cautiousness in their return to play, appears to be directly related to athletes' fear of reinjury.4 Johnston and Carroll4 observed that athletes' fear of reinjury often resulted in a number of behavioral responses, including but not limited to “being hesitant, holding back, not giving 100% effort, and being wary of injury-provoking situations.”
The process of psychosocial responses seemed to be cyclical in nature (ie, cognitions influencing emotions and behaviors and vice versa) and influenced by distinct personal (ie, severity of injury diagnosis) and situational (ie, source of social support and timing of injury) factors. This is consistent with the integrated model,6 which assumes that a number of situational and personal factors will influence the athletes' cognitive appraisal and emotional and behavioral responses (also known as the “dynamic core”) to the injury. When proposing the model, Wiese-Bjornstal et al6 posited that these interactions are bidirectional but that they would be more dominant in the clockwise direction (ie, cognitive appraisals affect emotions, emotions affect behavior, behaviors affect cognitive appraisals), which was the case among the participants in this study.
Consistent with the original model of Wiese-Bjornstal et al,6 these interactions among the different components of the dynamic core also appeared to be 3-dimensional and spiral-like in nature. That is, the psychosocial recovery for the athletes in this study had an “upward spiral,” meaning that as the rehabilitation advanced, their overall thoughts, emotions, and behaviors became more positive as they progressed toward successful recovery from their injuries. Also, the most notable points of change in athletes' cognitive appraisal, as well as emotional-response inclines and declines in athletes' recovery spirals, were identifiable at the different phases of recovery: initial reactions to injury (including after diagnosis), reactions to rehabilitation, and reactions to return to sport.
However, throughout the process of recovery, one factor that remained consistent was the athletes' need for social support. Injured athletes in this study sought and received social support throughout the different phases of recovery and this appeared to have a huge effect on these individuals during the course of their rehabilitation. This finding is also consistent with the model of Wiese-Bjornstal et al,6 as the integrated model posits that social support (ie, use or disuse of social support), a situational factor, and a behavioral response are vital parts of successful recovery. Seeking and receiving support from different people (eg, parents, siblings, coach, and AT) was also evident in this study, and as such, highlighted the importance of identifying a range of sources that may be useful for injured athletes during recovery.
Application of Findings
Based on our results, we believe that in order to best assist injured athletes in their rehabilitation process, ATs should be equipped to understand and use psycho-education in their work with injured athletes. Understanding how athletes' cognitive appraisals and emotional and behavioral responses interlink during the different phases of rehabilitation can better equip ATs to understand and relate to athletes and their resulting psychosocial responses during injury rehabilitation. More importantly, ATs will then be able to use this information to better help their athletes navigate the injury-recovery process from a psychosocial standpoint. Among the areas in which we feel that ATs could be further educated is their ability to understand how individual psychosocial responses to injuries vary from 1 person to another. For example, personal factors, such as a history of stressors, self-motivation, athletic identity, and self-perceptions, and situational factors, such as teammate influences, coach influences, sport ethic, and the rehabilitation environment, can all potentially influence how 2 athletes with seemingly similar injuries may react completely differently throughout the course of their injury rehabilitation. We believe that an increased understanding of how these 2 concepts interact during the entire injury-recovery process can potentially help ATs tailor their approach to working with each athlete based on his or her psychosocial responses, which reflect different personal and situational factors.
In addition to educating athletes about the injury process from a psychosocial standpoint, athletes should also be educated about how their thoughts, emotions, and behaviors are likely to evolve in a cyclical manner throughout the entire process. More specifically, athletes should be educated that as they move through the different phases of rehabilitation, they may be faced with new challenges that could potentially require them to engage in new behaviors and will affect their thinking and emotions. Above all, we believe that it is imperative to let athletes know that as they progress through the injury-recovery process, it is normal to experience fluctuations in thoughts, emotions, and behaviors, which, on occasion, can also be negative in nature.
Finally, as social support was seen as the most constant behavioral response by the athletes in this study (they sought social support throughout the process), we believe that ATs could benefit from being further educated about social support. Understanding the mechanisms of social support and who is best suited to provide different types of social support, as well as the significance of their own role as a potential source of social support, can help ATs to work more effectively with their athletes.23 Specifically, ATs, in conjunction with other allied health professionals, such as a sport psychologist, could educate the athletes about the importance of social support in the rehabilitation process, the different types of social support available,23,24 the differences between perceived and received social support,23,25 and from whom they should seek the different types of social support throughout the injury-recovery process.23,26 We believe that increased education in these areas could increase injured athletes' ability to make use of the variety of social-support sources they have at their disposal. Moreover, with increased education, the effectiveness of the social support sought could also potentially increase.
Limitations and Future Directions
Although our results provided meaningful findings with regard to athletes' psychosocial responses during the various phases of injury rehabilitation, the study is not without limitations. First, the participants were a convenience sample of Division II athletes who were not representative of athletes who compete at varying levels of competition. Given the sample size, unique characteristics, and the different situational and personal factors (as stipulated by Wiese-Bjornstal et al6) associated with Division II athletes, these results cannot be generalized to all settings. Additionally, participants were interviewed retrospectively; this may have resulted in poor recall of their emotions during the different phases of rehabilitation. Finally, the responses reported in this study represent only athletes with more severe injuries, and as such, cannot be generalized to athletes who sustain less severe injuries.
Nevertheless, future researchers in this area should investigate the psychosocial responses of injured athletes who compete at a variety of levels, including but not limited to high school, Divisions I and III, professional, Olympic, and senior. Additionally, it may be useful to ascertain athletes' psychosocial states before injury and possibly at a 6-month follow-up after return to play. Finally, it may also be worthwhile to use a mixed-methods approach involving the use of instruments such as the Emotional Responses of Athletes to Injury Questionnaire27 and the Profile of Mood States.28,29
In summary, injured athletes' cognitive appraisals and emotional and behavioral responses varied during the different phases of the injury-rehabilitation process. Our findings provide support for both the integrated model6 and the different phases of rehabilitation,3 as well as understanding how these 2 interlink. Recognizing how athletes' cognitive appraisal and emotional and behavioral responses interact during the different phases of rehabilitation can help ATs better comprehend athletes' reactions during the process and thus help them provide better care to their patients. Moreover, understanding how individual psychosocial responses to injuries are often affected by injury diagnosis warrants increased awareness from those treating injured athletes.
REFERENCES
- 1.Prentice WE, Arnheim DD. Arnheim's Principles of Athletic Training: A Competency-Based Approach. 14th ed. New York, NY: McGraw-Hill Higher Education;; 2011. [Google Scholar]
- 2.Clement D, Granquist MD, Arvinen-Barrow MM. Psychosocial aspects of athletic injuries as perceived by athletic trainers. J Athl Train. 2013;48(4):512–521. doi: 10.4085/1062-6050-48.3.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kamphoff C, Thomae J, Hamson-Utley JJ. Integrating the psychological and physiological aspects of sport injury rehabilitation: rehabilitation profiling and phases of rehabilitation. In: Arvinen-Barrow MM, Walker N, editors. The Psychology of Sport Injury and Rehabilitation. New York, NY: Routledge;; 2013. pp. 134–155. [Google Scholar]
- 4.Johnston LH, Carroll D. The context of emotional responses to athletic injury: a qualitative analysis. J Sport Rehabil. 1998;7(3):206–220. [Google Scholar]
- 5.Tracey J. The emotional response to the injury and rehabilitation process. J Appl Sport Psychol. 2003;15(4):279–293. [Google Scholar]
- 6.Wiese-Bjornstal DM, Smith AM, Shaffer SM, Morrey MA. An integrated model of response to sport injury: psychological and sociological dynamics. J Appl Sport Psychol. 1998;10(1):46–69. [Google Scholar]
- 7.Zhang Y, Wildemuth BM. Qualitative analysis of content. In: Wildemuth BM, editor. Applications of Social Research Methods to Questions in Information and Library Science. Westport, CT: Libraries Unlimited;; 2009. pp. 308–319. [Google Scholar]
- 8.Patton MQ. Qualitative Research and Evaluation Methods. 3rd ed. Thousand Oaks, CA: Sage Publications;; 2002. [Google Scholar]
- 9.Fischer CT. Bracketing in qualitative research: conceptual and practical matters. Psychother Res. 2009;19(4–5):583–590. doi: 10.1080/10503300902798375. [DOI] [PubMed] [Google Scholar]
- 10.Pitney WA, Parker J. Qualitative Research in Physical Activity and the Health Professions. Champaign, IL: Human Kinetics;; 2009. [Google Scholar]
- 11.Gould D, Bridges D, Udry E, Beck L. Stress sources encountered when rehabilitating from season-ending ski injuries. Sport Psychol. 1997;11(4):361–378. [Google Scholar]
- 12.Leddy MH, Lambert MJ, Ogles BM. Psychological consequences of athletic injury among high-level competitors. Res Q Exerc Sport. 1994;65(4):347–354. doi: 10.1080/02701367.1994.10607639. [DOI] [PubMed] [Google Scholar]
- 13.McDonald SA, Hardy CJ. Affective response patterns of the injured athlete: an exploratory analysis. Sport Psychol. 1990;4(3):261–274. [Google Scholar]
- 14.Carson F, Polman CJ. ACL injury rehabilitation: a psychological case study of a professional rugby union player. J Clin Sport Psychol. 2008;2(1):71–90. [Google Scholar]
- 15.Yang J, Peek-Asa C, Lowe JB, Heiden E, Foster DT. Social support patterns of collegiate athletes before and after injury. J Athl Train. 2010;45(4):372–379. doi: 10.4085/1062-6050-45.4.372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Udry E. Coping and social support among injured athletes following surgery. J Sport Exerc Psychol. 1997;19(1):71–90. [Google Scholar]
- 17.Ievleva L, Orlick T. Mental links to enhanced healing: an exploratory study. Sport Psychol. 1991;5(1):25–40. [Google Scholar]
- 18.Rose J, Jevne RF. Psychosocial process associated with athletic injuries. Sport Psychol. 1993;7(3):309–328. [Google Scholar]
- 19.Podlog L, Eklund RC. Return to sport after serious injury: a retrospective examination of motivation and psychological outcomes. J Sport Rehabil. 2005;14(1):20–34. [Google Scholar]
- 20.Podlog L, Eklund RC. A longitudinal investigation of competitive athletes' return to sport following serious injury. J Appl Sport Psychol. 2006;18(1):44–68. [Google Scholar]
- 21.Bianco T, Malo S, Orlick T. Sport injury and illness: elite skiers describe their experiences. Res Q Exerc Sport. 1999;70(2):157–169. doi: 10.1080/02701367.1999.10608033. [DOI] [PubMed] [Google Scholar]
- 22.Crossman J. Psychological rehabilitation from sports injuries. Sports Med. 1997;23(5):333–339. doi: 10.2165/00007256-199723050-00005. [DOI] [PubMed] [Google Scholar]
- 23.Arvinen-Barrow M, Pack SM. Social support in sport injury rehabilitation. In: Arvinen-Barrow M, Walker N, editors. The Psychology of Sport Injury and Rehabilitation. New York, NY: Routledge;; 2013. pp. 117–132. [Google Scholar]
- 24.Hardy CJ, Crace RK, Burke KL. Social support and injury: a framework for social support-based interventions with injured athletes. In: Pargman D, editor. Psychological Bases of Sport Injuries. 3rd ed. Morgantown, WV: Fitness Information Technology;; 2007. pp. 175–198. [Google Scholar]
- 25.Norris FH, Kaniasty K. Received and perceived social support in times of stress: a test of the social support deterioration deterrence model. J Pers Soc Psychol. 1996;71(3):498–511. doi: 10.1037//0022-3514.71.3.498. [DOI] [PubMed] [Google Scholar]
- 26.Heil J. Psychology of Sport Injury. Champaign, IL: Human Kinetics;; 1993. [Google Scholar]
- 27.Smith AM, Scott SG, O'Fallon WM, Young ML. Emotional responses of athletes to injury. Mayo Clin Proc. 1990;65(1):38–50. doi: 10.1016/s0025-6196(12)62108-9. [DOI] [PubMed] [Google Scholar]
- 28.McNair DM, Lorr M, Droppleman LF. Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service;; 1971. [Google Scholar]
- 29.Terry PC, Lane AM, Fogarty GJ. Construct validity of the profile of mood states—adolescents for use with adults. Psychol Sport Exerc. 2003;4(2):125–139. [Google Scholar]