

Abstract
Background:
Shivering associated with spinal anesthesia is a common complication. It also causes more usage of oxygen, increased production of carbon dioxide (CO2), and lactic acidosis with movement of clots and bleeding after surgery. This study was performed to compare the different dosages of intrathecal meperidine and their effects on shivering during and after surgery and to compare these to the control group.
Materials and Methods:
This study is a clinical trial. Target population consisted of the patients who were candidates for lower limb orthopedic surgery under spinal anesthesia. About 120 patients were chosen and randomly divided into four groups. In group 1, spinal anesthesia was performed with 3 ml marcaine 0.5% and 0.1 mg/kg meperidine. In group 2, 3 ml marcaine 0.5% and 0.2 mg/kg meperidine was given. In group 3, 3 ml marcaine 0.5% and 0.3 mg/kg meperidine, and in the fourth group, 3 ml marcaine 0.5% and normal saline in the same volume were injected. During surgery and recovery, hemodynamic index and shivering were recorded.
Results:
Based on the analyzed data, in the fourth group 23 patients (76.7%) had shivering. While the prevalence of shivering in the first, second, and third groups was 15 patients (50%), 11 patients (36.7%), and 3 patients (10%), respectively. Chi-square test showed significant difference in the four groups (P < 0.001).
Conclusions:
Using higher dosage of intrathecal meperidine (0.3 mg/kg) was more effective than using lower dosage of meperidine (0.1 mg/kg and 0.2 mg/kg) in reducing the incidence and severity of shivering during spinal anesthesia in lower extremity orthopedic surgeries.
Keywords: Meperidine, orthopedic surgery, shivering, spinal anesthesia
INTRODUCTION
Shivering after spinal anesthesia is a common complication encountered in more than 56.7% of patients.[1] This is unpleasant for the patients and may interrupt monitoring of ECG, blood pressure, and pulse oximetry. Also, it may cause more oxygen usage, more CO2 production, and lactic acidosis,[2,3,4] which is dangerous for patients with limited cardiopulmonary capacity.[3] Other than these, shivering may cause surgical problems such as clot movement and bleeding. So, control of shiver after spinal anesthesia is important.[5] The mechanism of shivering after spinal anesthesia is unknown, but there are different theories to explain it.[6,7,8] After general anesthesia, heat is distributed from the central parts to the peripheral parts. Lack of thermoregulatory mechanism, below the blocked level, causes more loss of heat. This thermoregulatory mechanism causes decrease in vasoconstriction (0.5°C) and increased threshold of sweating. As a treatment of this shiver, intravenous injection of drugs such as meperidine, clonidine, ketanserin, magnesium sulfate, and physostigmine is suggested. Meperidine is the only opioid and agonist of μ and K receptors which is suggested to treat and prevent shivering.[4,9,10] Meperidine (in a dosage of 0.5–1.8 mg/kg) alone is used in spinal anesthesia.[8,9] In this dosage, complications like nausea, vomiting, itching, decrease of blood pressure, bronchospasm, bradycardia, and respiratory depression are reported,[11,12,13,14] corresponding to the dosage.[15] Anti-shiver effect of meperidine may be because of systemic absorption. Intravenous meperidine is more effective in comparison to other μ agonists like fentanyl, alfentanil, sufentanil, and morphine in the same dosage.[9,16,17] There are evidences indicating that the anti-shivering effect of meperidine is primarily due to the other receptors,[16,17] and it seems that the most active receptor is the k receptor which is activated by meperidine. So, many researchers believe that the anti-shivering effect of meperidine is mediated by the agonist activation of k receptors.[16,18,19] But there is not enough evidence about the prophylactic effect of different dosages of meperidine on shivering. So, we performed this study to compare the efficacy of different dosages of meperidine (0.1 mg/kg, 0.2 mg/kg, and 0.3 mg/kg) on the incidence and severity of shivering during and after spinal anesthesia in lower extremity orthopedic surgeries.
MATERIALS AND METHODS
After obtaining institutional approval from the Ethic Committee of the university and taking written informed consent from the patients, this randomized double-blinded clinical trial was performed in 2012 in Kashani Medical Center. The statistical community consisted of patients who were candidates for lower limb orthopedic surgery with spinal anesthesia in this hospital in the year 2012. The inclusion criteria were: patients of age 18–65 years with ASA I and II and willingness of the patients who were candidates for lower limb orthopedic surgery to participate in the study. The exclusion criteria were: lack of patient's cooperation for spinal anesthesia, bleeding during surgery if transfusion was needed, and any kind of change in anesthesia method. Randomization was performed by using random allocation software. The drugs of study were prepared by a physician who was not informed about the group allocation, and data collection was performed by another physician who was not aware of the study drugs. To increase reliability, we enrolled 30 patients in each group. In these groups with level of assurance 95% and poverty of test 80%, the prevalence of shivering during surgery was 56.7%.[1] After getting permission from the research committee of the university and acceptance of the patients, the patients were divided into four groups randomly. In the first group, spinal anesthesia was administered with 3 ml marcaine 0.5% and 0.1 mg/kg meperidine. The second and third group of patients were injected with 3 ml marcaine 0.5% added to 0.2 mg/kg and 0.3 mg/kg meperidine, respectively, and in the fourth group, normal saline and 3 ml marcaine 0.5% were injected in the same volume. Drugs were prepared in the same volume and syringes by the anesthesiologist. After the patients entered the operation room, monitoring of ECG, noninvasive blood pressure, heart rate, and pulse oximetry was done. Before administering anesthesia, 15 ml/kg Ringer's lactate was injected to all patients. All the liquids were warmed up to 37°C. In all groups, spinal anesthesia was administered in a sitting position at L3-L4 joint space with 25 G needle in the midline. After anesthesia, the maximum level of block was measured every minute for 10 min by pinprick sense evaluation. Room temperature was kept between 21 and 23°C. To evaluate the severity of shivering, we used Crossley and Mahajan score and measured it every 15 min until the end of surgery. The scoring was as follows: 0: without shivering; 1: piloerection or peripheral vasoconstriction without visible shivering; 2: muscular activation only in one group of muscles; 3: muscular activation in more than one group of muscles without generalized shivering; 4: generalized shivering. Mean arterial blood pressure, heart rate, and SPO2 were measured and recorded every 15 minutes during surgery. Central temperature was measured by tympanic thermoscan every 15 min from the beginning of spinal block till the end of the surgery and recorded. Peripheral temperature of the patients was measured by axillary thermoscan every 15 min from the beginning of spinal anesthesia and recorded. Drug reactions such as urinary retention, itching, and respiratory depression were also measured in the four groups. Hypotension was defined as systolic blood pressure lower than 20% of baseline. Bradycardia was defined as pulse rate lower than 20% of baseline during surgery. If there was decrease of blood pressure, 5-10 ml ephedrine was injected intravenously. When there was decrease in heart rate, 0.5 mg atropine was injected intravenously. For pain reduction during surgery, 25-50 μg fentanyl was injected if the Visual Analog Scale (VAS) was over 4 cm. In the recovery room, severity of shivering was recorded every 15 min until the patient was shifted from there. When shivering reached above level 2, at any time, 25 mg meperidine was injected intravenously. If the patient had nausea and vomiting, 0.1 mg/kg metoclopramide was injected intravenously. Duration of stay at the recovery room was noted as return of sensory block to two segments and recorded. Data were entered and analyzed by SPSS 20 software, and t-test, q-square, one-way analysis of variance, variance analysis with repeated measure, and Mann-Whitney test were used for analysis.
RESULTS
In this study, 120 patients who were candidates for orthopedic surgery on the lower limbs participated and were randomly divided into four groups. Table 1 shows their demographic features. Q-square and Fisher tests and one-way analysis of variance showed no significant differences between these groups (P > 0.5).
Table 1.
Demographic variables of the patients in the four groups
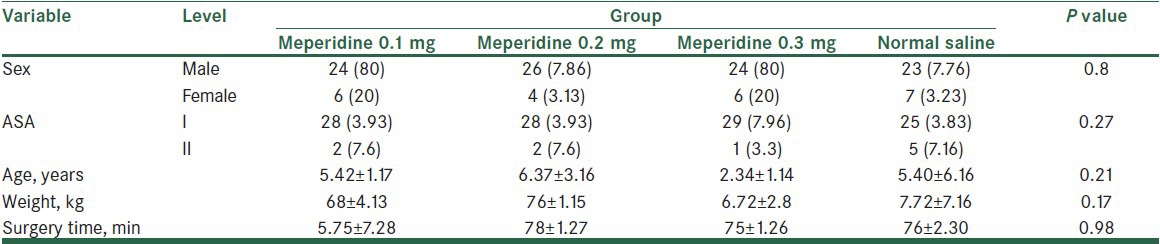
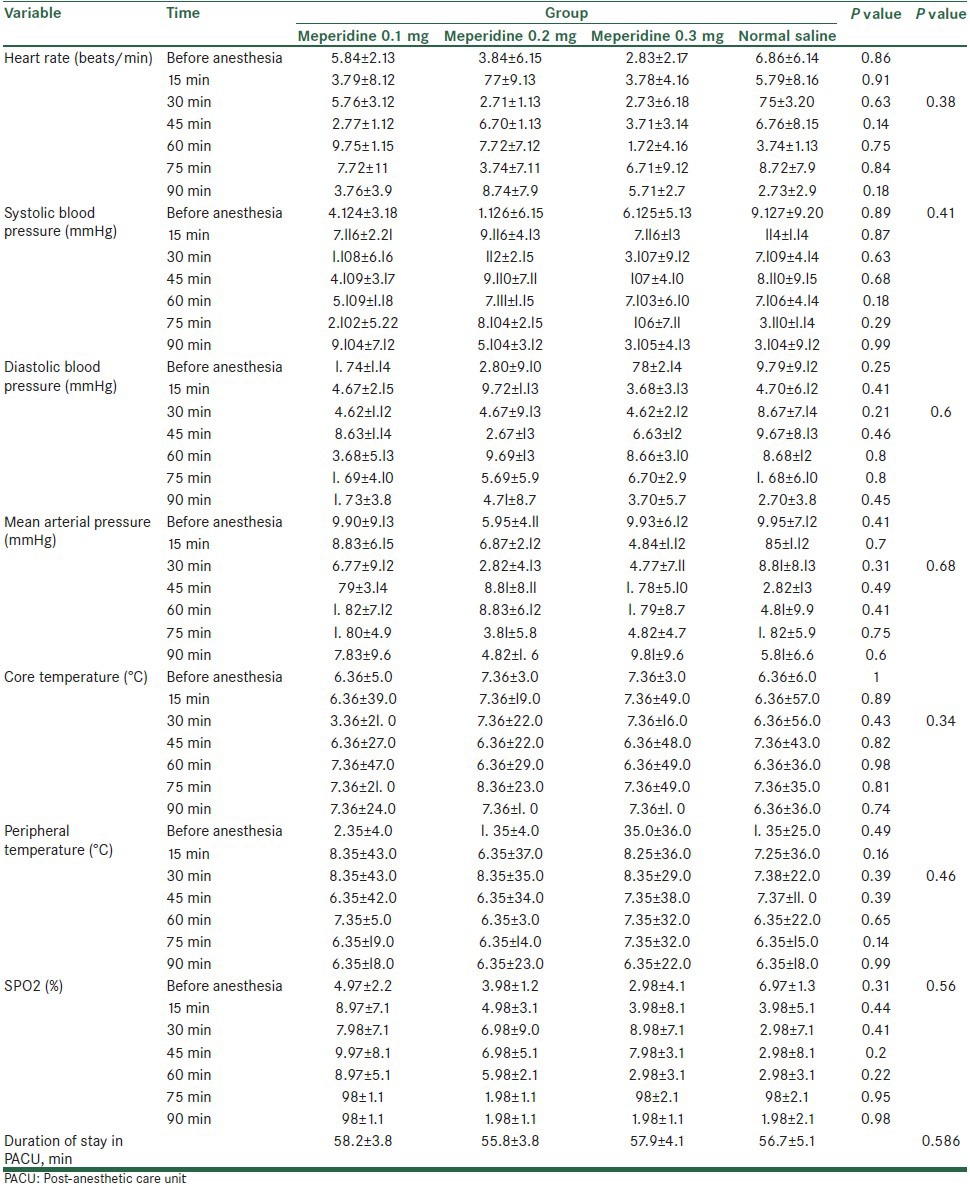
Table 2 shows the hemodynamic parameters in the four groups. The tests used showed no significant difference at different time periods in the four groups (P > 0.05). Also, repeated measures variance analysis of hemodynamic data showed no significant difference from the time before anesthesia till 90 min in the four groups (P > 0.05). The prevalence of pressure loss in the four groups was: 7 (23.3%), 8 (26.7%), 7 (23.3%), and 7 (23.3%). q-square test did not show significant differences between the groups (P = 0.99).
Table 2.
Mean and standard deviation of hemodynamic indices from 0 to 90 min in the four groups
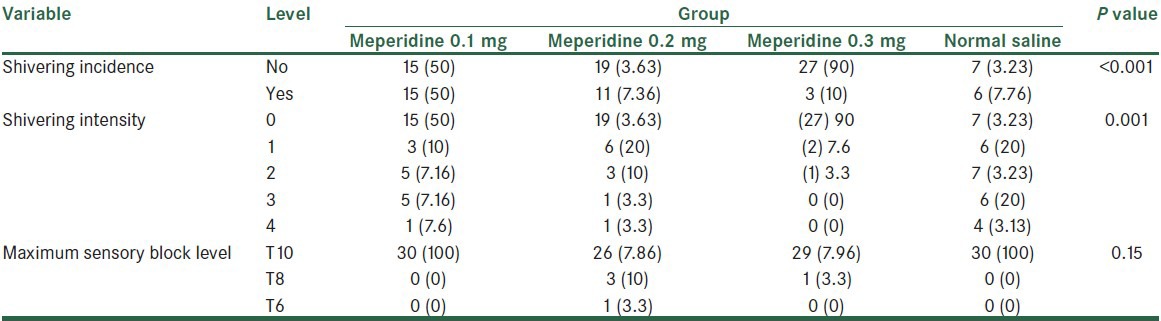
In Table 3, the prevalence of shivering during the study in the four groups is shown. Data show that in the fourth group, 23 patients (76.7%) had shiver, while the prevalence of shiver in three first groups was 15 patients (50%), 11 patients (36.7%), and 3 patients (10%), respectively. Q-square test showed significant difference between the groups (P < 0.001). Mann-Whitney test showed significant difference between the fourth and third groups (P < 0.001). But there was no significant difference between the first and fourth groups (P = 0.08). On the other hand, the tests showed significant difference between the second and third groups in the severity of shivering (P = 0.014). Also, the difference between the first and third groups was significant (P < 0.001). But there was no significant difference in the severity of shivering between the first and second groups (P = 0.13). Table 3 shows the prevalence of severity of shivering in the four groups. Wilkinson test showed significant difference between the four groups. Also, the maximum block sensory level is shown in this table. Fisher test showed that the differences between the groups were not significant (P = 0.15). The average time of stay at the recovery room in the four groups were 30.5 ± 8.7, 28.5 ± 7.3, 29.7 ± 6.7, and 28.8 ± 5.4, respectively. One-way variance analysis showed the differences between the four groups were not significant (P = 0.7).
Table 3.
Frequency distribution of shivering incidence and intensity in the four groups
The average dosages of metoclopramide, meperidine, and ephedrine used are shown in Table 4. One-way variance analysis showed the average dosages of meperidine and metoclopramide used in the four groups had significant difference, but the average dosage of ephedrine used was almost the same. Atropine was used in a dosage of 0.5 mg Table 4, but Fisher test showed no significant difference in the groups using this drug.
Table 4.
Mean and standard deviation of meperidine, metoclopramide, and ephedrine dosages used in the four groups

DISCUSSION
Meperidine is the only opioid drug and agonist of μ and K receptors that is suggested to treat and prevent shivering. IV meperidine is much more effective in treating shivering than equianalgesic doses of other opioid agonists such as fentanyl, alfentanil, sufentanil, or morphine. The efficacy of meperidine in shivering is largely preserved during the administration of a standard dose of naloxone (0.5 μg/kg/min), but is virtually obliterated by a 10-fold increase in the dose (5.0 μg/kg/min).[20] There are evidences of anti-shivering effect of meperidine which is catalyzed by other receptors, and it seems that the most active receptor is the k receptor which is activated by meperidine. So, many researchers believe that the anti-shivering effect of meperidine is mediated by the agonist activation of k receptors. Also, meperidine decreases the shivering threshold almost twice as much as the vasconstriction threshold, and this reduction in the shivering threshold appears to underlie the anti-shivering effect of meperidine. But there is not enough evidence about the prophylactic effect of different dosages of meperidine on shivering. The goal of this study was to compare the effects of different dosages of intrathecal meperidine on shivering during and after surgery with a control group.
The obtained data show that all the four groups were almost matched with respect to the demographic variables such as sex, age, weight, duration of surgery, and ASA. The results of our study showed no hemodynamic changes in the four groups during surgery. So, meperidine can be considered a safe drug in lower limb orthopedic surgery. Data show that the prevalence of shivering in the fourth group was 76.7%, while that in the first three groups was 50%, 36.7%, and 10%, respectively. So, the prevalence of shivering in the fourth group was significantly higher. On the other hand, data showed that the dosage of meperidine is also important in controlling shivering. The prevalence of shivering showed significant difference between the fourth group and the second and third groups, whereas the first and fourth groups had no significant difference. Also, the prevalence of shivering had no significant difference between the first and second groups. These results agree to those of Chen et al.'s study. Chen et al. mentioned that low dosage of intrathecal meperidine, at all instances except midwifery, can cause decrease in outbreak of shiver.[1] Roy et al.'s study also showed that 0.2 mg/kg of intrathecal meperidine can cause less shivering during cesarean section.[21] In Davoudi et al.'s study, the efficiency and assurance of low dosage of intrathecal meperidine during spinal anesthesia is shown.[22] Anaraki and Mirzaei's study showed that high dose of intrathecal meperidine (0.4 mg/kg) is effective in reducing the incidence and intensity of shivering associated with spinal anesthesia for cesarean delivery, but the high incidence of nausea and vomiting is unpleasant for the patient.[23] Chun et al. also showed the addition of meperidine 0.2 mg/kg to intrathecal bupivacaine lowers the incidence and severity of shivering during transurethral prostatectomy in elderly patients.[24] Based on these results, intrathecal meperidine in a dosage of 0.3 mg/kg is also effective in controlling post-surgical complications such as nausea and vomiting. The average dosage of metoclopramide used in the third group was 5.42 ± 1.44 mg, but in the other three groups it was 10 mg. The dosage of other drugs which were used, such as ephedrine and atropine, had no significant difference in the four groups. The study had some limitations. Cases of this study were just the patients undergoing spinal anesthesia, and also, they were only the candidates for lower limb orthopedic surgery, which implies the need for further studies on patients undergoing general anesthesia, or performing similar studies on patients undergoing other surgical procedures.
CONCLUSION
Using higher dosage of intrathecal meperidine (0.3 mg/kg) was more effective than using lower dosage of meperidine (0.1 mg/kg and 0.2 mg/kg) in reducing the incidence and severity of shivering during spinal anesthesia in lower extremity orthopedic surgeries. There was no significant hemodynamic change on using higher dosage of intrathecal meperidine.
ACKNOWLEDGMENTS
The authors wish to sincerely thank all the colleagues in Kashani Hospital Medical Center affiliated to Isfahan University of Medical Sciences in Isfahan, Iran for their support. Furthermore, our special thanks go to the patients, who wholeheartedly and actively assisted us to carry out this research. No conflict of interest existed. This prospective randomized observational study was approved by the Ethics Committee of our university (Anesthesiology and Critical Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran) and all patients gave written, informed consent.
Footnotes
Source of Support: Anesthesiology and Critical Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Chen JC, Hsu SW, Hu LH, Hong YJ, Tsai PS, Lin TC, et al. Intrathecal meperidine attenuates shivering induced by spinal anesthesia. Ma Zui Xue Za Zhi. 1993;31:19–24. [PubMed] [Google Scholar]
- 2.Macintyre PE, Pavlin EG, Dwersteg JF. Effect of meperidine on oxygen consumption, carbon dioxide production, and respiratory gas exchange in postanesthesia shivering. Anesth Analg. 1987;66:751–5. [PubMed] [Google Scholar]
- 3.Piper SN, Fent MT, Röhm KD, Maleck WH, Suttner SW, Boldt J. Urapidil does not prevent postanesthetic shivering: A dose-ranging study. Can J Anaesth. 2001;48:742–7. doi: 10.1007/BF03016688. [DOI] [PubMed] [Google Scholar]
- 4.Tsai YC, Chu KS. A comparison of tramadol, amitriptyline, and meperidine for postepidural anesthetic shivering in parturients. Anesth Analg. 2001;93:1288–92. doi: 10.1097/00000539-200111000-00052. [DOI] [PubMed] [Google Scholar]
- 5.Morgan GE, Mikhail MS, Murray MJ. Anesthesia for genitourinary surgery. In: Murray MJ, Morgan GE, Mikhail MS, editors. Clinical anesthesiology. 3rd ed. New York: McGraw-Hill; 2002. pp. 695–6. [Google Scholar]
- 6.Matsukawa T, Sessler DI, Christensen R, Ozaki M, Schroeder M. Heat flow and distribution during epidural anesthesia. Anesthesiology. 1995;83:961–7. doi: 10.1097/00000542-199511000-00008. [DOI] [PubMed] [Google Scholar]
- 7.Kurz A, Sessler DI, Schroeder M, Kurz M. Thermoregulatory response thresholds during spinal anesthesia. Anesth Analg. 1993;77:721–6. doi: 10.1213/00000539-199310000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Ozaki M, Kurz A, Sessler DI, Lenhardt R, Schroeder M, Moayeri A, et al. Thermoregulatory thresholds during epidural and spinal anesthesia. Anesthesiology. 1994;81:282–8. doi: 10.1097/00000542-199408000-00004. [DOI] [PubMed] [Google Scholar]
- 9.Alfonsi P, Sessler DI, Du Manoir B, Levron JC, Le Moing JP, Chauvin M. The effects of meperidine and sufentanil on the shivering threshold in postoperative patients. Anesthesiology. 1998;89:43–8. doi: 10.1097/00000542-199807000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Monso A, Riudeubas J, Barbal F, Laporte JR, Arnau JM. A randomized, double-blind, placebo-controlled trial comparing pethidine to metamizol for treatment of post-anaesthetic shivering. Br J Clin Pharmacol. 1996;42:307–11. doi: 10.1046/j.1365-2125.1996.04124.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Patel D, Janardhan Y, Merai B, Robalino J, Shevde K. Comparison of intrathecal meperidine and lidocaine in endoscopic urological procedures. Can J Anaesth. 1990;37:567–70. doi: 10.1007/BF03006327. [DOI] [PubMed] [Google Scholar]
- 12.Hansen D, Hansen S. The effects of three graded doses of meperidine for spinal anesthesia in African men. Anesth Analg. 1999;88:827–30. doi: 10.1097/00000539-199904000-00027. [DOI] [PubMed] [Google Scholar]
- 13.Norris MC, Honet JE, Leighton BL, Arkoosh VA. A comparison of meperidine and lidocaine for spinal anesthesia for postpartum tubal ligation. Reg Anesth. 1996;21:84–8. [PubMed] [Google Scholar]
- 14.Sangarlangkarn S, Klaewtanong V, Jonglerttrakool P, Khankaew V. Meperidine as a spinal anesthetic agent: A comparison with lidocaine-glucose. Anesth Analg. 1987;66:235–40. [PubMed] [Google Scholar]
- 15.Tauzin-Fin P, Maurette P, Vincon G, Hecquet D, Houdek MC, Bonnet F. Clinical and pharmacokinetic aspects of the combination of meperidine and prilocaine for spinal anaesthesia. Can J Anaesth. 1992;39:655–60. doi: 10.1007/BF03008225. [DOI] [PubMed] [Google Scholar]
- 16.Pauca AL, Savage RT, Simpson S, Roy RC. Effect of pethidine, fentanyl and morphine on post-operative shivering in man. Acta Anaesthesiol Scand. 1984;28:138–43. doi: 10.1111/j.1399-6576.1984.tb02029.x. [DOI] [PubMed] [Google Scholar]
- 17.Guffin A, Girard D, Kaplan JA. Shivering following cardiac surgery: Hemodynamic changes and reversal. J Cardiothorac Anesth. 1987;1:24–8. doi: 10.1016/s0888-6296(87)92593-2. [DOI] [PubMed] [Google Scholar]
- 18.Kurz M, Belani KG, Sessler DI, Kurz A, Larson MD, Schroeder M, et al. Naloxone, meperidine, and shivering. Anesthesiology. 1993;79:1193–201. doi: 10.1097/00000542-199312000-00009. [DOI] [PubMed] [Google Scholar]
- 19.Wang JJ, Ho ST, Lee SC, Liu YC. A comparison among nalbuphine, meperidine, and placebo for treating postanesthetic shivering. Anesth Analg. 1999;88:686–9. doi: 10.1097/00000539-199903000-00041. [DOI] [PubMed] [Google Scholar]
- 20.De Witte J, Sessler DI. Perioperative shivering: Physiology and pharmacology. Anesthesiology. 2002;96:467–84. doi: 10.1097/00000542-200202000-00036. [DOI] [PubMed] [Google Scholar]
- 21.Roy JD, Girard M, Drolet P. Intrathecal meperidine decreases shivering during cesarean delivery under spinal anesthesia. Anesth Analg. 2004;98:230–4. doi: 10.1213/01.ANE.0000093251.42341.74. [DOI] [PubMed] [Google Scholar]
- 22.Davoudi M, Mousavi-Bahar H, Farhanchi A. Intrathecal meperidine for prevention of shivering during transurethral resection of prostate. Urol J. 2007;4:212–6. [PubMed] [Google Scholar]
- 23.Anaraki AN, Mirzaei K. The effect of different intrathecal doses of meperidine on shiverering during delivery under spinal anesthesia. Int J Prev Med. 2012;3:706–12. [PMC free article] [PubMed] [Google Scholar]
- 24.Chun DH, Kil HK, Kim HJ, Park C, Chung KH. Intrathecal meperidine reduces intraoperative shivering during transurethral prostatectomy in elderly patients. Korean J Anesthesiol. 2010;59:389–93. doi: 10.4097/kjae.2010.59.6.389. [DOI] [PMC free article] [PubMed] [Google Scholar]