

Abstract
Background: Hypertension is an important public-health challenge worldwide. The prevalence of hypertension greatly varies across countries. The aim of this study was to estimate the prevalence of self-reported hypertension and to determine related factors in a large random sample of Tehran population in 2011.
Methods: In this cross sectional study, 69173 individuals aged 25–64 years were selected using multistage cluster random sampling method. All participants were interviewed by trained personnel using standard questionnaires. Weighted prevalence and incidence rates were calculated and principle component analysis (PCA) was used to construct wealth index. Chi-square and odds ratio were used to assess associations in univariate analysis. Logistic Regression model was used in multivariate analysis.
Results: The prevalence of self-reported hypertension was 5.27% in total, 3.83% in men and 6.64% in women (p< 0.001). The annual incidence rate of self-reported hypertension was 6.87 per 1000; 5.26 in men and 8.43 in women (p< 0.001), obviously varied across various districts. In multivariate analysis, age, sex (woman), marital status (single), obesity and smoking were positively associated with prevalence of self-reported hypertension. Education level was negatively associated to hypertension. On the other hand, wealth status was not associated to self-reported hypertension.
Conclusion: Our study findings highlighted low awareness rates of hypertension among Tehran adults especially in men and younger people. Hence, we recommend public health strategies to improve health education programs. Moreover, programs to develop the surveillance system and screening programs to early detection of undiagnosed cases are urgently needed particularly in high risk population subgroups.
Keywords: Hypertension, Self-reporting, Prevalence, Tehran
Introduction
Hypertension (HTN), known as a global public-health challenge, is a condition in which blood vessels have persistently raised pressure. It may lead to heart attacks, stroke, kidney failure, blindness, rupture of blood vessels and cognitive impairment (1-5). In 2008, the condition has affected approximately one billion individuals, 40% of adults aged 25 and above across the world (1, 3). The highest prevalence of raised blood pressure was reported in the WHO African region with 46% for males and females combined, while the lowest reported in the WHO region of the America with 35% for both males and females. However, the prevalence of hypertension shows a significant variation across countries (6). Awareness of hypertension also varies from 25.2% to 75% [4]. Hypertension accounts for 57 million disability adjusted life years (DALYS) or 3.7% of total DALYS (7). According to the WHO, complications of hypertension account for 9.4 million deaths worldwide every year (8). In Iran, according to a systematic review of 29 studies, the estimated overall prevalence of hypertension in 30 – 55 and >55-year-old population was around 23% and 50%, respectively. This prevalence in men was 1.3% less than that in women and by each year increase in the mean age of subjects, the prevalence increased about 0.5% (8). Other studies on hypertension in Iran have reported the prevalence rates in adults ranged from 21.2% to 41.8%, mostly with higher rates in females, higher age groups, illiterates, poor people and urban residents (9-14).
At the early stages, hypertension is a silent and invisible condition with rare symptoms. Thus, enhancing public awareness and early detection is important to avoid its further stages’ complications. Recently, researchers and health specialists increasingly face to obtain information about chronic illnesses conditions and risk factors from self-reports of target populations (15-20), because prevalence rates based on clinically measured blood pressure are often higher than the self-reports’ rates (21). While self-reported data is often more economically feasible and readily available compared to clinically measured hypertension, these reports may underestimate clinical prevalence and also may vary in different socio-cultural positions (22) .
The aim of this study was to estimate the prevalence of self-reported hypertension and to assess its associated factors in a representative sample of Tehran adults.
Methods
The second Urban HEART project was a cross-sectional study conducted in Tehran, Iran, in fall 2011. Participants were visited at their house by interviewers who were trained during a two-day workshop prior to data gathering (23).
There were 3 types of questionnaires consisting of 20 parts. The first 14 parts were completed for all selected households, but 3 of these, including demographic, socioeconomic and hypertension data were used for current analysis. All the gathered data were based on the participants’ self-reports. Any participant, who was diagnosed as hypertensive patient by a physician or used anti hypertensive drug at the time of the survey, was considered as a hypertension case. The patients whose time of onset of condition was one year or less were considered as new cases and calculated at the annual incidence rates. Body mass index (BMI) was calculated using the formula weight (kg)/height (m2). Wealth index was calculated using principle component analysis (PCA) on 14 assets and some other household data including: owning a fridge, a personal computer, a telephone, a mobile phone, a washing machine, a microwave oven, a car, a motorcycle, a kitchen, a bathroom, a toilet, house ownership, number of rooms per capita (less than one vs. one and more), and area of the house (below the median vs. above the median). In principle component analysis, the first component explains the largest proportion of the total variance, so assets that were more unequally distributed across the sample had a higher weight in the first component. The weights (coefficients) for each asset from this first component were used to generate the wealth scores, with higher score indicating higher wealth status and vice versa. Finally, based on quintiles, the scores converted to five ordered categories, from poorest to richest, to determine each household wealth status.
Sampling method and sample size
A multistage cluster random sampling was used in this study. First stage was stratified by districts. Then 200 clusters were selected randomly in each district and finally eight household were selected in each cluster using systematic random sampling method and all the household persons were selected as primary sampling units. To estimate required sample size for the survey, each district was considered independently to calculate sample size based on Cochrane formula as 1535 households in each district. Then, to facilitate the allocation of sample to the mentioned eight-box table that had to be completed for the individual questionnaires and also to reach higher precision, the sample was expanded to 1600 households, regardless the population size in each district. Therefore, we assigned 200 blocks to each district equally. To allocate samples at neighborhood level, method of the probability proportional to size of each district was used. The total sample size was 34116 households covering 118542 individuals from 22 districts and 368 neighborhoods. After excluding participants aged under 25 and over 65 years (n = 49369). The analysis was performed on data of the remaining 69173 individuals, who were aged 25–64 years.
Statistical analysis
Descriptive statistical measures (including measures of central tendency, dispersion, the weighted prevalence and incidence rates) were used to describe the data. Principle component analysis was used to construct the wealth index. Chi-square and Odds ratio were used to assess associations in univariate analysis. In multivariate analysis, Odds Ratios from Logistic Regression model were used as the measures of association between the study variables. All reported p-values are based on two-sided tests and compared to a significance level of 0.05. STSTA version 12.0 software was used for all the statistical calculations.
Results
A total of 69173 subjects consisting 33884 (49%) men and 35289 (51%) women, were included in this analysis. The mean age ± standard deviation (SD) of the participants was 41.5±11.37 years. The overall weighted prevalence of self-reported hypertension was 5.27%; significantly higher in women (6.64%) than men (3.83%) (p<0.001). Age group of 25-34 years had the minimum prevalence (0.56%) and age group of 55-64 years had the maximum prevalence (15.32%). Overall trend for prevalence of self-reported hypertension increased considerably as age increased (p for trend<0.001) (Table 1).
Table 1 . Prevalence rates of Hypertension by sex and age groups.
| Age group | Male | Female | Total | p-value | ||||||
| n | HTN | Weighted Prevalence (%) (95% CI) | n | HTN | Weighted Prevalence (%) (95% CI) | n | HTN | Weighted Prevalence (%) (95% CI) | ||
| 25-34 | 11991 | 76 | 0.66 (0.49-0.83) | 12267 | 59 | 0.45 (0.33 – 0.57) | 24258 | 135 | 0.56 (0.46 – 0.65) | 0.11 |
| 35-44 | 8108 | 144 | 1.87 (1.52-2.23) | 8668 | 258 | 2.87 (2.43 – 3.30) | 16776 | 402 | 2.39 | <0.001 |
| 45-54 | 7822 | 436 | 5.51 (4.95-6.10) | 8576 | 835 | 9.84 (9.01 – 10.67) | 16398 | 1271 | 7.80 (7.23 – 8.37) | <0.001 |
| 55-64 | 5963 | 625 | 10.51 (9.57-11.46) | 5778 | 1160 | 20.32 (18.79 – 21.85) | 11741 | 1785 | 15.32 (14.31 – 16.32) | <0.001 |
| Total | 33884 | 1281 | 3.83 (3.56 – 4.10) | 35289 | 2312 | 6.64 (6.21 – 7.07) | 69173 | 3593 | 5.27 (4.96-5.57) | <0.001 |
The annual weighted incidence rate of self-reported hypertension was 6.87 per 1000; 5.26 in men and 8.43 in women. Age group of 25-34 years had the lowest incidence rate (1.09 per 1000) and age group of 55-64 years had the highest incidence rate (14.94 per 1000). The estimated female to male risk ratio for incidence rate of self-reported hypertension was 1.61 (1.34 – 1.93). Risk ratios and their 95% confidence intervals presented in Table 2 indicates that incidence rates of self-reported hypertension in men was significantly higher than women in age groups of 45-54 and 55-64 years, but no significant difference in age groups of 25-34 and 35-44 years was observed. The overall trend for incidence rates of self-reported hypertension increased considerably as age increased (p for trend<0.001).
Table 2 . Weighted incidence rates of hypertension by sex and age groups .
| Age group | Male | Female | Total | Risk Ratio (95% CI) Female / Male | ||||||
| At Risk | New case | Incidence (per 1000) | At Risk | New case | Incidence (per 1000) | At Risk | New case | Incidence (per 1000) | ||
| 25-34 | 11915 | 17 | 1.56 | 12208 | 8 | 0.63 | 24123 | 25 | 1.09 | 0.46(0.20 – 1.06) |
| 35-44 | 7964 | 35 | 4.35 | 8410 | 56 | 5.88 | 16374 | 91 | 5.14 | 1.52(0.99 – 2.31) |
| 45-54 | 7386 | 69 | 7.81 | 7741 | 125 | 14.42 | 15127 | 194 | 11.30 | 1.73(1.29 – 2.32) |
| 55-64 | 5338 | 62 | 10.50 | 4618 | 108 | 19.57 | 9956 | 170 | 14.94 | 2.01(1.48– 2.74) |
| Total | 32603 | 183 | 5.26 | 32977 | 297 | 8.43 6 | 5580 | 480 | 6.87 | 1.61(1.34 – 1.93) |
Figure 1 indicates that as age increased, prevalence and incidence rates of self-reported hypertension in both sex increased. Moreover, both reported prevalence and incidence rates tend to be higher in women in relation to men as age increased so that in age group of 55-64 years, the two rates have been reached almost twice for females in relation to males.
Fig. 1 .
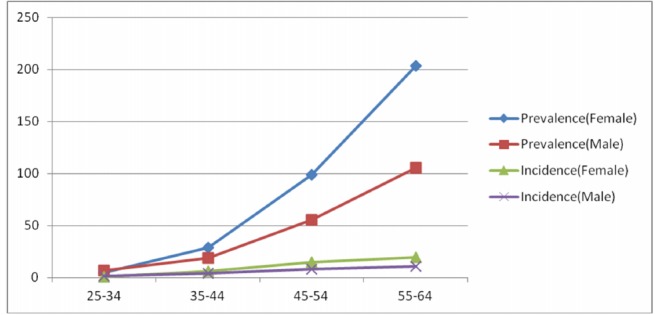
Prevalence and Incidence rates of self-reported hypertension by sex and age groups (per 1000)
Table 3 shows the prevalence and incidence rates of self-reported hypertension by district. The two rates obviously vary across the districts. The lowest prevalence occurred in district 17 (2.3%) and the highest in 8 (7.0%). On the other hand, the lowest incidence rate was in district 17 (2.15 per 1000) and the highest in 9 (10.07 per 1000).
Table 3 . Prevalence and Incidence rates of self-reported hypertension by district .
| District | n | HTN | Weighted Weighted Prevalence (%) (95% CI) | At Risk | New Case | Weighted Incidence (per 1000) (95% CI) |
| 1 | 3200 | 133 | 4.16(3.15 – 5.16) | 3067 | 17 | 5.31(3.20 – 7.11) |
| 2 | 3295 | 225 | 6.83(5.29 – 8.37) | 3070 | 24 | 7.28(3.71 – 10.86) |
| 3 | 3042 | 153 | 5.03(4.09 – 5.97) | 2889 | 12 | 3.95(1.20 – 6.69) |
| 4 | 3301 | 170 | 5.15(3.91 – 6.39) | 3131 | 25 | 7.57(3.58 – 11.57) |
| 5 | 3363 | 202 | 6.01(5.02 – 6.99) | 3161 | 25 | 7.43(5.28 – 9.59) |
| 6 | 2955 | 168 | 5.69(4.57 – 6.80) | 2787 | 29 | 9.81(4.49 – 15.14) |
| 7 | 3068 | 146 | 4.76(3.63 – 8.89) | 2922 | 20 | 6.52(1.80 – 11.24) |
| 8 | 210 | 7.02(6.02 – 8.02) | 2763 | 19 | 6.35(2.46 – 10.24) | |
| 9 | 2979 | 178 | 5.98(4.76 – 7.19) | 2801 | 30 | 10.07(7.04 – 13.10) |
| 10 | 3011 | 105 | 3.49(1.49 – 5.48) | 2906 | 24 | 7.97(2.04 – 13.90) |
| 11 | 2962 | 142 | 4.80(3.56 – 6.04) | 2819 | 19 | 6.42(4.13 – 8.71) |
| 12 | 3166 | 193 | 6.10(4.42 – 7.78) | 2973 | 25 | 7.90(4.60 – 11.19) |
| 13 | 2764 | 94 | 3.40(2.46 – 4.34) | 2670 | 11 | 3.98(1.94 – 6.03) |
| 14 | 2971 | 140 | 4.71(3.10 – 4.43) | 2831 | 16 | 5.39(2.44 – 8.31) |
| 15 | 3408 | 179 | 5.25(4.37 – 6.14) | 3229 | 26 | 7.63(2.79 – 12.46) |
| 16 | 3055 | 178 | 5.83(4.41 – 7.25) | 2877 | 26 | 8.51(4.02 – 13.0) |
| 17 | 3261 | 75 | 2.30( 1.56 – 3.04) | 3186 | 7 | 2.15(0.37 – 3.93) |
| 18 | 3683 | 155 | 4.21(3.17 – 5.24) | 3528 | 18 | 4.89(3.40 – 6.38) |
| 19 | 3201 | 169 | 5.28(4.33 – 6.23) | 3032 | 29 | 9.06(5.68 – 12.44) |
| 20 | 3424 | 203 | 5.93(4.87 – 6.99) | 3221 | 30 | 8.76(5.31 – 12.22) |
| 21 | 3503 | 240 | 6.85(5.85 – 7.86) | 3263 | 29 | 8.28(5.65 – 10.91) |
| 22 | 2569 | 135 | 5.26(4.39 – 6.14) | 2434 | 19 | 7.40(3.89 – 10.91) |
| Total | 69173 | 3593 | 5.27(4.96 – 5.57) | 65580 | 480 | 6.87(6.02 – 7.73) |
In multivariate analysis, the odds of self-reported hypertension in women was 1.62 times that of men. Among all assessed variables in the survey, age had the strongest association to self-reported hypertension so that the odds of self-reported hypertension rapidly increased as age of participants increased (p for trend<0.001). Overall, as the level of education increased, the odds of self-reported hypertension decreased (p for trend<0.001) so that illiterate respondents had more likely than the +17 college group to report hypertension. Compared with married participants, single participants had 33% higher odds of reporting hypertension whereas widow or divorced participants had less likely to report hypertension [OR = 0.46 (0.36 – 0.58)]. The odds of being hypertensive increased with excess of BMI (p for trend<0.001) so that cmpared with the normal group, over weight and obese participants had more likely to report hypertension (52% and 2.42 times, respectively). Also smokers had 19% more likely to report hypertension than non-smokers. On the other hand, only wealth status was not associated to self-reported hypertension. The Odds ratios and their confidence intervals are presented in Table 4.
Table 4 . Multivariate analysis results using logistic regression model.
| Characteristics | N | HTN | Weighted Prevalence (%) (95% CI) | Odds Ratio (95% CI) | p-value | p-value for trend | |
| Total | 69173 | 3593 | 5.27(4.96-5.57) | ||||
| Sex | male | 33884 | 1281 | 3.83(3.56 – 4.10) | 1 | ||
| Female | 35289 | 2312 | 6.64(6.21 – 7.07) | 1.62(1.48 - 1.77) | <0.001 | ||
| Age group | 25-34 | 24258 | 135 | 0.56(0.46 – 0.65) | 1 | ||
| 35-44 | 16776 | 402 | 2.39(2.08 – 2.70) | 2.86 (2.25 - 3.63) | <0.001 | ||
| 45-54 | 16398 | 1271 | 7.80(7.23 – 8.37) | 8.71(7.10 – 10.75) | <0.001 | ||
| 55-64 | 11741 | 1785 | 15.32(14.31 – 16.32) | 18.22(14.74 – 22.53) | <0.001 | <0.001 | |
| Marital Status | Married | 50118 | 3057 | 6.19(5.79 – 6.59) | 1 | ||
| Single | 3436 | 428 | 12.84(11.48 – 14.19) | 1.33(1.18 – 1.50) | <0.001 | ||
| Widow or Divorced | 14497 | 83 | 0.57(0.42 – 0.72) | 0.46(0.36 – 0.58) | <0.001 | ||
| Literacy | Illiterate | 3566 | 513 | 14.53(13.02 – 16.04) | 1.66(1.26 – 2.19) | <0.001 | |
| 1-5 Schooling | 5788 | 558 | 9.86(8.88 – 10.84) | 1.27(0.97 – 1.67) | 0.07 | ||
| 6-8 Schooling | 8832 | 618 | 7.20(6.49 – 7.92) | 1.29(0.99 – 1.68) | 0.06 | ||
| 9-12 Schooling | 30392 | 1341 | 4.55(4.13 – 4.97) | 1.20(0.93 – 1.54) | 0.16 | <0.001 | |
| 13-16 College | 16850 | 458 | 2.77(2.40 – 3.14) | 1.04(0.80 – 1.36) | 0.75 | ||
| +17 College | 3398 | 85 | 2.65(2.07 – 3.23) | 1 | |||
| BMI | Under Weight | 1677 | 19 | 1.21(0.65 – 1.78) | 0.64(0.40 – 1.03) | 0.065 | |
| Normal | 29026 | 850 | 2.94(2.70 – 3.19) | 1 | |||
| Over Weight | 25427 | 1519 | 6.04(5.62 – 6.45) | 1.52(1.38 – 1.66) | <0.001 | <0.001 | |
| Obese | 10067 | 1095 | 11.17(10.29 – 12.05) | 2.42(2.19 – 2.68) | <0.001 | ||
| Smoking | No Smoker | 62996 | 3258 | 5.25(4.94 – 5.56) | 1 | ||
| Smoker | 6177 | 335 | 5.44(4.80 – 6.07) | 1.19(1.04-1.35) | 0.01 | ||
| Wealth Status | Poorest | 12889 | 614 | 4.75(4.24 – 5.26) | 1 | ||
| Poor | 12444 | 657 | 5.28(4.79 – 5.76) | 0.99(0.86 – 1.14) | 0.85 | ||
| Moderate | 9211 | 504 | 5.43(4.85 – 6.02) | 1.03(0.87 – 1.21) | 0.72 | ||
| Rich | 16768 | 923 | 5.63(5.15 – 6.11) | 1.10(0.96 – 1.26) | 0.17 | 0.33 | |
| Richest | 13306 | 700 | 5.51(4.92 – 6.10) | 1.13(0.95 – 1.33) | 0.16 | ||
Discussion
There is a wide range of hypertension prevalence in previous reports. Worldwide estimates for the adult population ranges from 3.4 to 72.5% (4).The present study estimated overall prevalence of self-reported hypertension as 5.27%, which is much lower than the data provided by other clinically assessed (1, 6, 10-13) and even self-reported studies (3, 15, 23-27). This difference is probably due to different study populations, methods and sample sizes. In self-reported studies, moreover, public awareness of hypertension status plays an important role, so that the less public awareness, the more underestimation may occur.
In this study, hypertension was more prevalent in women (6.64%) than in men (3.83%) similar to most previous studies (9, 12, 14, 23, 28-31), although some contradictory results could be observed (6, 10, 13, 32, 33). This can be explained partly by the fact that women usually used to express more their unwellness and are interested in healthcare services more than men, therefore more likely to have higher awareness of the condition. Also, as we expected, self-reported prevalence of hypertension obviously raised by increasing age in both genders, like most other studies (6, 10-14, 27-30, 32). However with increasing age, a more rapid rise in reported prevalence rates occurred in women compared to men. Furthermore, age and sex patterns of incidence rates of self-reported hypertension were as same as the prevalence rates of self-reported hypertension.
The estimated prevalence and incidence rates of self-reported hypertension by districts ranged from 2.3% to 7.0% and 2.15 to 10.1 respectively. The lowest prevalence and incidence rates of hypertension were reported from district 17 while the highest prevalence and incidence rates of hypertension were reported from districts 8 and 9 respectively. These variations may be explained by different rates of hypertension or different patterns of awareness and reporting the condition among districts residents.
In multivariate analysis using binary logistic regression, we found higher odds of reporting hypertension among women versus men after adjustment for other variables. Also, similar to previous studies, increasing age, BMI, low literacy level and smoking were independent risk factors for self-reported hypertension (6, 7, 10-13, 20, 27, 30). Singles had 33% higher odds of reporting hypertension compared to married persons.Odds of reporting hypertension among widows and divorced was nearly half the married participants, which is probably due to different patterns of utilizing medical services or different self-reporting rates among the three groups. Only wealth status was not significantly associated to self-reported hypertension in multivariate analysis.
A major strength of our study is the larger sample size compared to previous studies in Tehran. This can reduce probability of random error, and can provide more precise estimates as we can see the narrow confidence intervals for the estimated rates. Moreover, using random sample from each district enabled us to achieve better estimates of the rates disaggregated by districts. Our study is subject to several limitations, too: first, because the study design was a cross-sectional survey, the associations are not proof of causality so reverse causality bias could be there. Second, the nature of self-reporting used in the study can cause underestimation of disease rates because always a large fraction of hypertensive cases in any population are not diagnosed and also some participants are probably reluctant to reveal their disease. Third, it was logistically difficult to measure participants’ blood pressure in this survey; hence, we could not present direct estimates of the awareness rates of hypertension in the study population.
Conclusion
Our study findings highlighted low reported rates of hypertension among Tehran adults, which was higher in men and younger people. Hence, we recommend public health strategies to improve health literacy to increase public awareness of hypertension. Moreover, programs to improve the surveillance systems and implementation of community based screening programs to early detection of the cases are urgently needed especially in high risk population subgroups.
Cite this article as: Cheraghian B, Asadi-Lari M, Mansournia M.A, Majdzadeh R, Mohammad K, Nedjat S, Vaez-Mahdavi M.R, Faghihzadeh S. Prevalence and associated factors of self-reported hypertension among Tehran adults in 2011: a population-based study (Urban HEART-2). Med J Islam Repub Iran 2014 (29 September). Vol. 28:105.
References
- 1. World Health Organization. A global brief on hypertension, Silent killer, global public health crisis. 2013.
- 2.Tu K, hen Z, Lipscombe L. Prevalence and incidence of hypertension from 1995 to 2005: a population-based study . CMAJ. May 20 2008;178(11):1429–35. doi: 10.1503/cmaj.071283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Centers for Disease. Self-Reported Hypertension and Use of Antihypertensive Medication Among Adults United States, 2005–2009. MMWR . April 5 2013;62(13) [PMC free article] [PubMed] [Google Scholar]
- 4.Kearney P, Whelton M, Reynolds K, Whelton P, He J. Worldwide prevalence of hypertension: a systematic review. Journal of Hypertension. 2004;22(1):11–9. doi: 10.1097/00004872-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V. et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study. Lancet. 2010 Dec 15;380(9859):2095–128. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sarry El-Din A, Erfan M, Kandeel W, Kamal S, El Banna R, Fouad W. Prevalence of Pre-hypertension and Hypertension in a sample of Egyptian Adults and its Relation to Obesity. Australian Journal of Basic and Applied Sciences. 2012;6(13):481–9. [Google Scholar]
- 7. Mendis S, Puska P, Norrving B. Global Atlas on Cardiovascular Disease Prevention and Control. World Health Organization, Geneva. 2011.
- 8.Haghdoost A, Sadeghirad B, Rezazadehkermani M. Epidemiology and Heterogeneity of Hypertension in Iran:A Systematic Review. Archives of Iranian Medicine. 2008;11(4):444–52. [PubMed] [Google Scholar]
- 9.Veghari G, Sedaghat M, Maghsodlo S, Banihashem S, Moharloei P P, Angizeh A. et al. Impact of Literacy on the Prevalence, Awareness, Treatment andControl of Hypertension in Iran. Journal of Cardiovascular and Thoracic Research. 2012;4(2):37–40. doi: 10.5681/jcvtr.2012.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sahraki M, Mirshekari H, Sahraki A, Mohammadi M, Sahraki E, Khazaei Feizabad A. Hypertension Among 30+ Year-Old People in Zahedan (Southeast of Iran) Shiraz E-Medical Journal . July 2011;12(3):129–34. [Google Scholar]
- 11.Namayandeh S, Sadr S, Rafiei M, Modares-Mosadegh M, Rajaefard M. Hypertension in Iranian Urban Population, Epidemiology, Awareness, Treatment and Control. Iranian J Publ Health. 2011;40(3):63–70. [PMC free article] [PubMed] [Google Scholar]
- 12.Azizi F, Esmaillzadeh A, Mirmiran P. Obesity and cardiovascular disease risk factors in Tehran adults: a population-based study. Eastern Mediterranean Health Journal. 2004;10(6):887–97. [PubMed] [Google Scholar]
- 13.Peymani P, Heydari S, Ahmadi S, Sarikhani Y, Joulaei H, Moghadami M. et al. The Prevalence of High Blood Pressure and Its Relationship with Anthropometric Indicators; a Population Based Study in Fars Province, IR Iran. Int Cardiovasc Res J. 2012;6(2):40–5. [Google Scholar]
- 14.Esteghamati A, Meysamie A, Khalilzadeh O, Rashidi A, Haghazali M, Asgari F. et al. Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. 2009;9(167) doi: 10.1186/1471-2458-9-167. Epub 2003/03/26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Goldman N, Lin IF, Weinstein M, Lin YH. Evaluating the quality of self-reports of hypertension and diabetes. J Clin Epidemiol. 2003;56(2):148–54. doi: 10.1016/s0895-4356(02)00580-2. Epub 2003/03/26. [DOI] [PubMed] [Google Scholar]
- 16.Ayoade A, Oladipo I. Evaluation of the correlation between self-report and electronic monitoring of adherence to hypertension therapy. Blood Press. 21(3):161–6. doi: 10.3109/08037051.2012.679029. Epub 2012/04/20. [DOI] [PubMed] [Google Scholar]
- 17.Sokka T, Pincus T. Poor physical function, pain and limited exercise: risk factors for premature mortality in the range of smoking or hypertension, identified on a simple patient self-report questionnaire for usual care. BMJ Open. 1(1):e000070. doi: 10.1136/bmjopen-2011-000070. Epub 2011/10/25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tsai AC, Chang TL. Quality issues of self-report of hypertension: analysis of a population representative sample of older adults in Taiwan. Arch Gerontol Geriatr. 55(2):338–42. doi: 10.1016/j.archger.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 19.Okura Y, Urban LH, Mahoney DW, Jacobsen SJ, Rodeheffer RJ. Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J Clin Epidemiol. 2004;57(10):1096–103. doi: 10.1016/j.jclinepi.2004.04.005. Epub 2004/11/06. [DOI] [PubMed] [Google Scholar]
- 20.Parker A, Freeman LB, Cantor K, Lynch C. Self-report of smoking, obesity and hypertension history and survival among a cohort of iowa renal cell carcinoma cases. Ann Epidemiol. 2000;10(7):467–8. doi: 10.1016/s1047-2797(00)00158-7. Epub 2000/10/06. [DOI] [PubMed] [Google Scholar]
- 21.Selem S, Castro M, Cesar C, Marchioni L, Fisberg R. Validity of self-reported hypertension is inversely associated with the level of education in Brazilian individuals. Arq Bras Cardiol. 2013;100(1):52–9. doi: 10.1590/s0066-782x2012005000119. [DOI] [PubMed] [Google Scholar]
- 22.Mentz G, Schulz A, Mukherjee B, Ragunathan T, Perkins D, Israel B. Hypertension: Development of a prediction model to adjust self-reported hypertension prevalence at the community level. BMC Health Services Research, 12:312. 2012;12(3120) doi: 10.1186/1472-6963-12-312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Asadi-Lari M, Vaez-Mahdavi MR, Faghihzadeh S, Cherghian B, Esteghamati A, Farshad AA. et al. Response-oriented measuring inequalities in Tehran: second round of Urban Health Equity Assessment and Response Tool (Urban HEART-2), concepts and framework. Medical Journal of the Islamic Republic of Iran. 2013;27(4):236–48. [PMC free article] [PubMed] [Google Scholar]
- 24.Pitsavos C, Milias G, Panagiotakos D, Xenaki D, Panagopoulos G, Stefanadis C. Prevalence of self-reported hypertension and its relation to dietary habits, in adults; a nutrition & health survey in Greece. BMC Public Health. 2006;6(206) doi: 10.1186/1471-2458-6-206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rodriguez F, Hicks L, Lopez L. Association of acculturation and country of origin with self-reported hypertension and diabetes in a heterogeneous Hispanic population. BMC Public Health. 2012;12(768) doi: 10.1186/1471-2458-12-768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Estoppey D, Paccaud F, Vollenweider P, Vidal P. Trends in self-reported prevalence and management of hypertension, hypercholesterolemia and diabetes in Swiss adults, 1997-2007. BMC Public Health. 2011;11(114) doi: 10.1186/1471-2458-11-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Valderrama A, Tong X, Carma Ayala, Keenan N. Prevalence of Self-Reported Hypertension, Advice Received From Health Care Professionals, and Actions Taken to Reduce Blood Pressure Among US Adults—HealthStyles, 2008. The Journal of Clinical Hypertension. October 2010;12(10) doi: 10.1111/j.1751-7176.2010.00323.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Azizi F, Ghanbarian A, Madjid M, Rahmani M. Distribution of blood pressure and prevalence of hypertension in Tehran adult population: Tehran Lipid and Glucose Study (TLGS), 1999–2000. Journal of Human Hypertension. 2002;16:305–12. doi: 10.1038/sj.jhh.1001399. [DOI] [PubMed] [Google Scholar]
- 29.Gupta R. Trends in hypertension epidemiology in India. Journal of Human Hypertension. 2004;18:73–8. doi: 10.1038/sj.jhh.1001633. [DOI] [PubMed] [Google Scholar]
- 30.Hatmi Z, Tahvildari S, Gafarzadeh Motlag A, Sabouri Kashani A. Prevalence of coronary artery disease risk factors in Iran: a population based survey. BMC Cardiovascular Disorders. 2007;7(32) doi: 10.1186/1471-2261-7-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Doğan M, Toprak D, Demir S. Hypertension prevalence and risk factors among adult population in Afyonkarahisar region: a cross-sectional research. Anadolu Kardiyol Derg. 2012;12:47–52. doi: 10.5152/akd.2012.009. [DOI] [PubMed] [Google Scholar]
- 32.Shapo L, Pomerleau J, McKee M. Epidemiology of hypertension and associated cardiovascular risk factors in a country in transition: a population based survey in Tirana City, Albania. J Epidemiol Community Health. 2003;57:734–9. doi: 10.1136/jech.57.9.734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Manandhar K, Koju R, Sinha N, Humagain S. Prevalence and associated risk factors of hypertension among people aged 50 years and more in banepa municipality, Nepal. Kathmandu University Medical Journal. Jul- Sep 2012;10(39) doi: 10.3126/kumj.v10i3.8015. [DOI] [PubMed] [Google Scholar]