

Abstract
Objective
This study evaluated effects of nonlinear frequency compression (NLFC) processing in children with hearing loss for consonant identification in quiet and for spondee identification in competing noise or speech. It was predicted that participants would benefit from NLFC for consonant identification in quiet when access to high-frequency information was critical, but that NLFC would be less beneficial, or even detrimental, when identification relied on mid-frequency cues. Further, it was hypothesized that NLFC could result in greater susceptibility to masking in the spondee task. The rationale for these predictions is that improved access to high-frequency information comes at the cost of decreased spectral resolution.
Design
A repeated-measures design compared speech perception outcomes in 17 pediatric hearing aid users (9-17 years) wearing Naida V SP “laboratory” hearing aids with NLFC on and off. Data were also collected in an initial baseline session in which children wore their personal hearing aids. Children with a wide range of audiometric configurations were included, but all participants were full-time users of hearing aids with active NLFC. For each hearing aid condition, speech perception was assessed in the sound field using a closed-set 12-alternative consonant-vowel identification measure in quiet, and a closed-set 4-alternative spondee identification measure in a speech-shaped noise or in a two-talker speech masker.
Results
No significant differences in performance were observed between laboratory hearing aid conditions with NLFC activated or deactivated for either speech perception measure. An unexpected finding was that the majority of participants had no difficulty identifying the high-frequency consonant /s/, even when NLFC was deactivated. Investigation into individual differences revealed that subjects with a greater difference in audible bandwidth with NLFC on versus NLFC off were less likely to demonstrate improvements in high-frequency consonant identification in quiet, but were more likely to demonstrate improvements in spondee identification in speech-shaped noise. Group results observed in the initial baseline assessment using personal aids fitted with more aggressive NLFC settings than used in laboratory aids indicated better consonant identification accuracy in quiet. However spondee identification in the two-talker masker was poorer with personal compared with laboratory hearing aids. Comparisons across personal and laboratory hearing aids are tempered, however, by the potential of an order effect.
Conclusions
The observation of comparable performance with NLFC on and off in the laboratory aids provides evidence that NLFC is neither detrimental nor advantageous when modest in strength. Results with personal hearing aids fitted with stronger compression settings than laboratory aids (NLFC on) highlight the critical need for further research to determine the impact of NLFC processing on speech perception for a wider range of speech perception measures and compression settings.
Keywords: children, hearing aids, hearing loss, speech perception
INTRODUCTION
Despite ongoing advances in hearing aid technology, many contemporary hearing aids are unable to provide sufficient gain to achieve audibility for frequencies above 5000 – 6000 Hz (Ricketts et al. 2008), a frequency region in which thresholds are typically quite poor (Pittman & Stelmachowicz 2003). Bandwidth restrictions due to gain limitations may be exacerbated in children relative to adults due to tubing resonance effects in behind-the-ear versus in-the-ear products (Killion, 1980), and increased susceptibility to acoustic feedback due to reamplification of leaked sound from tubing or poorly fitted earmolds in growing ears (Hellgren et al. 1999; Stelmachowicz et al. 2001). The impact of bandwidth restrictions on speech perception has been investigated in both children and adults with hearing loss, but findings appear to differ across these age groups. In adults, some work shows that increased high-frequency audibility fails to improve, and in some cases degrades, speech perception performance in individuals with considerable high-frequency hearing loss (Skinner 1980; Rankovic 1991; Ching et al. 1998; Hogan & Turner 1998; Turner & Cummings 1999). However, evidence is also available to support stable or improved speech recognition performance for adults with increased bandwidth (Stelmachowicz et al. 2001; Turner & Henry 2002; Simpson et al. 2005). It has been speculated that the presence of dead regions (i.e., non-stimulable areas in the cochlea) may partly explain decreased benefit with increased bandwidth (Vickers et al. 2001; Baer et al. 2002). Some studies report that adults with hearing loss who do not have dead regions show improved speech perception with increased bandwidth, but that adults with high-frequency dead regions tend not to benefit from increased high-frequency amplification within dead regions (Vickers et al. 2001; Baer et al. 2002, but also see Cox et al. 2011).
While results across adult studies describing the effects of high-frequency audibility on speech perception have been mixed, more consistent improvements have been observed in studies involving children. Work by Stelmachowicz and colleagues (2001) showed that children with mild to moderately severe hearing loss demonstrated improved speech perception with increased bandwidth. Pronounced improvements in fricative (i.e., /s, z/) identification were revealed with increased high-frequency audibility (Stelmachowicz et al. 2001). Children with hearing loss demonstrated an average improvement of 40 percentage points for stimuli produced by a female talker that were low-pass filtered at 9000 versus 6000 Hz (Stelmachowicz et al. 2001). The bandwidth effects observed for speech perception measures may have consequences for aspects of communication development in addition to speech perception. Hearing aid bandwidth limitations have been implicated as a contributing factor in delays in fricative and affricate production in early-identified children with hearing loss (Stelmachowicz et al. 2004; Moeller et al. 2007), and may contribute to articulation errors and grammar deficits (e.g., errors with plural and possessive forms of nouns; Elfenbein et al. 1994). High-frequency speech cues may be more beneficial for children than for adults with hearing loss due to the fact that children are still developing linguistic knowledge, which is shaped by auditory exposure and is therefore critically dependent upon consistent and adequate audibility (Stelmachowicz et al. 2004). Limited exposure to language could result in more stringent cue requirements, such that children require access to high-frequency speech cues that would be redundant for an adult.
Given the importance of high-frequency speech cues for children’s communication development and the bandwidth restrictions imposed by high-frequency gain limitations of most hearing aids, frequency-lowering algorithms have been developed to try to improve access to high-frequency information. A number of different signal processing methods exist, but the common goal of these technologies is to deliver high-frequency spectral information to a lower frequency region, where hearing thresholds are potentially better, and where more gain can be applied. Several frequency-lowering algorithms are available in contemporary, commercially available hearing aids, including nonlinear frequency compression (NLFC), dynamic speech recoding, and frequency transposition, with and without bandwidth restriction (reviewed by: Simpson 2009, McCreery et al. 2013). Reflecting the local clinical population, the present study focused specifically on NLFC. This technology acts on information above a specified start frequency by lowering it according to a pre-determined compression ratio.
Recent studies evaluating the effects of NLFC algorithms on speech perception and sound quality are relatively sparse and reveal variability in benefit. Work by Simpson et al. (2005) indicated that the overall performance of a group of adults with sloping high-frequency hearing loss on a word recognition test was improved when subjects wore an experimental NLFC aid versus conventional frequency processing. Single-subject data indicated that seven adults improved with NLFC, seven showed no change, and one exhibited poorer performance. In a follow-up experiment, researchers reported that the group benefit observed with the NLFC device also exceeded that achieved with an experimental, non-compressing device offering added high-frequency gain, although it was not apparent whether gain was equalized across the two devices (Simpson et al. 2005). Subsequent work by Simpson et al. (2006) revealed no improvements in speech recognition scores in quiet or noise with the experimental NLFC device in adults with more steeply sloping hearing losses. Results of the latter study imply reduced benefit from NLFC in participants with greater high-frequency hearing losses. However, conclusions are tenuous given that verification of improved high-frequency audibility with NLFC was not provided, and that some of the start frequencies for compression were lower than those available in contemporary, commercially available products.
Simulation studies have also provided insight into the potential impact of frequency compression on speech understanding and the variables contributing to success with NLFC. McCreery et al. (2013) compared the performance of 25 normal-hearing adults on a consonant-vowel-consonant, non-word identification task in quiet using hearing loss and hearing aid simulations. Three different audiometric configurations that varied in the amount of high-frequency hearing loss were used for simulations. The non-word stimuli were digitally processed to mimic standard hearing aid processing, and were presented in one of three formats: 1) conventional processing without NLFC (low-pass filtered at 5000 Hz), 2) NLFC processing using manufacturer default start frequency and compression ratio parameters, and 3) NLFC processing using “optimized” start frequency and compression ratio settings. The optimized settings were determined using the SoundRecover Fitting Assistant (Alexander 2009), which uses the audible bandwidth of the hearing aid with NLFC deactivated to assign compression recommendations. Analysis of group-average responses indicated that performance was best for the NLFC optimized fitting method, and that there was a positive relationship between bandwidth (compression on or off) and performance. There was no difference between the conventional and NLFC default conditions, however. These findings raise the possibility that differences in the benefit of NLFC across studies involving adults with hearing loss may be due, in part, to differences in the approach used to adjust compression prescriptions for individual subjects.
Although individual variability in NLFC benefit has also been observed in children, results of studies with children investigating the influence of NLFC on speech perception are generally more decisive than those of adults. Glista et al. (2009) analyzed the performance of children and adults with moderately-severe to profound high-frequency hearing loss on speech recognition, /s, ∫/ discrimination, and plural detection measures, administered with and without NLFC. Compression settings in NLFC aids were selected to optimize audibility of mid- and high-frequency sounds (e.g., live voice productions of /s, ∫/) while preserving participants’ ability to discriminate between these sounds (Glista et al. 2009). Results of testing indicated that the group-average detection thresholds were lower with NLFC compared to conventional processing, and scores on consonant and plural identification tasks were higher with NLFC. No significant difference was observed in vowel identification. Single-subject analyses indicated that most children benefitted or did no worse with NLFC processing than conventional amplification. Results of a multiple linear regression model suggested that participants with more hearing loss generally derived greater NLFC benefit.
Positive effects of NLFC in quiet have also been reported by Wolfe et al. (2010), who compared aided detection thresholds and performance on speech recognition measures in children with mild/moderate to moderately-severe hearing loss using hearing aids with conventional and NLFC processing. Consistent with earlier studies, a longitudinal design with NLFC on and off was employed, allowing for potential technology acclimatization. The NLFC settings were adjusted from manufacturer default values based on electroacoustic analysis of filtered speech sounds and participant feedback, an approach generally consistent with the recommended protocol developed by researchers at the University of Western Ontario (Glista & Scollie 2009). Testing performed after 6 weeks of device experience, with conventional and NLFC processing, revealed improved detection thresholds for warble tones and /s, ∫/ speech sounds, as well as increased accuracy of plural identification with NLFC. Results of a phoneme discrimination test (Logatom Test; Phonak 2009) revealed significant improvements in the accuracy of identification of two of the six consonants sampled (i.e., /d, s/). No improvement was observed in sentence recognition in multi-talker babble with NLFC over conventional processing. Wolfe et al. (2010) posited that the lack of improvement for sentences could reflect an increase in the audibility of high-frequency babble with compression (as well as target speech), or the need for an extended acclimatization period with NLFC for successful speech processing in the presence of a competing background sound. The benefits that were observed with NLFC after 6 weeks of acclimatization were comparable or greater after 6 months of device use (Wolfe et al. 2011).
Overall, research to date suggests that NLFC can improve high-frequency speech recognition in quiet for at least some children with hearing loss, and that the magnitude of gains may be dependent on the compression setting, and degree and configuration of hearing loss. However, a number of important questions surrounding NLFC technology and its application in pediatric hearing aid fittings remain unanswered. It is unclear how to configure compression for optimal performance in quiet, and even less is known about the influence of NLFC settings on speech perception in the presence of competing background sounds. The goal of the present study was to address this gap by investigating the influence of NLFC processing on children’s speech perception abilities in quiet, in competing noise, and in competing speech using hearing aids fitted according to a theory-driven fitting method known as the SoundRecover Fitting Assistant. Its approach is designed to optimize NLFC settings for listeners by maximizing the audible bandwidth (Alexander 2009). A secondary goal was to evaluate the influence of NLFC settings on speech perception by comparing outcomes for children wearing their personal hearing aids fitted using a more widespread clinical approach developed at the University of Western Ontario (Glista & Scollie 2009) versus performance for children wearing laboratory aids fitted using the approach based on maximizing audible bandwidth (Alexander 2009).
Previous studies showing improved /s, ∫/ discrimination, detection of final pluralization, and consonant identification with NLFC have primarily focused on recognition of a circumscribed set of predominantly high-frequency sounds (Glista et al. 2009; Wolfe et al. 2010; Wolfe et al. 2011). In contrast, effects of NLFC in children were evaluated in the present study using a broader range of speech stimuli and measures. The hypothesis is that NLFC may benefit children with hearing loss when the task requires access to high-frequency information in regions where hearing aids cannot adequately amplify sound (e.g., identification of the phoneme /s/; Glista et al. 2009; Wolfe et al. 2010), but may compromise the ability to use mid-frequency speech cues (e.g., Alexander 2012). Such impairment might be expected if the compression of high-frequency information reduces the resolution of speech cues. Support for this idea is provided by recent findings reported by Perreau et al. (2013) as part of a larger study investigating outcomes for adults using a cochlear implant in one ear and a hearing aid in the opposite ear (bimodal). Results indicated relatively poorer performance using NLFC compared to conventional hearing aid processing in the ear with acoustic amplification for both spondee identification in competing speech and vowel identification in quiet, but not for consonant identification in quiet. It was hypothesized that aggressive compression settings can cause spectral smearing and alter formant spacing, potentially decreasing speech understanding (see also Alexander 2009). Thus, the influence of NLFC on consonant identification in quiet in the present study was evaluated separately for high-frequency (i.e., / s, z, d, t/) and mid-frequency (i.e., /k, ∫, p, h/) consonants. Reductions in spectral resolution associated with NLFC are likely to be compounded by hearing loss and amplification (Glasberg & Moore 1986; Lutman et al. 1991), factors that are known to reduce spectral resolution. Testing in the presence of background noise could exacerbate the challenges associated with frequency resolution due to the fact that noise effectively reduces the spectral modulation depth of the speech signal. A complex masker, such as two-talker speech, could introduce additional challenges related to perceptually segregating the speech signal from the masker (e.g., Oxenham 2008). Spondee identification performance was therefore evaluated in both a speech-shaped noise and a two-talker speech masker to capture these effects.
MATERIALS AND METHODS
Participants
Seventeen children (6 males, 11 females) with bilateral sensorineural hearing loss participated in this study. The children ranged in age from 9 yr 5 mo to 17 yr 1 mo (mean age = 12 yr 3 mo). All participants were identified through the University of North Carolina Pediatric Audiology Clinic, where they receive ongoing audiological services. Participant recruitment and testing was completed in accordance with the rules and regulations of the University of North Carolina Institutional Review Board.
All participants were native English speakers with no known history of neurological problems (including Auditory Neuropathy Spectrum Disorder) or other medical issues (including recurrent or persistent middle ear infection). Age of hearing loss identification ranged from 2 mo to 6 yr (mean age = 2 yr 9 mo). The age of the children’s first hearing aid fitting was within 3 months of the time of identification for all but two participants, who were fitted 7 mo and 22 mo after their hearing loss was identified. Participants varied with respect to degree and configuration of hearing loss, ranging from mild to profound (Table 1). Reflecting the diverse population of children fitted with hearing aids that incorporate NLFC processing, this recruitment approach enabled investigation into individual differences influencing benefit from NLFC technology.
Table 1.
Participants’ thresholds at octave frequencies from 250 -8000 Hz ordered based on the difference in audible bandwidth with NLFC on versus off for the better hearing ear (logarithmic units). Points associated with missing data (*) and no response at the limits of the audiometer (nr) were omitted from calculations of mean threshold.
| Participant | Ear | 250 | 500 | 1000 | 2000 | 4000 | 8000 |
|---|---|---|---|---|---|---|---|
| 1 | R | 30 | 45 | 55 | 60 | 50 | 30 |
| L | 35 | 40 | 55 | 60 | 55 | 30 | |
| 2 | R | 35 | 35 | 40 | 35 | 10 | 30 |
| L | 30 | 30 | 35 | 40 | 10 | 0 | |
| 3 | R | 35 | 60 | 65 | 55 | 50 | 60 |
| L | 35 | 60 | 65 | 55 | 50 | 65 | |
| 4 | R | 55 | 60 | 70 | 70 | 65 | 65 |
| L | 50 | 55 | 65 | 65 | 60 | 65 | |
| 5 | R | 65 | 70 | 75 | 75 | 75 | 65 |
| L | 55 | 65 | 65 | 70 | 70 | 70 | |
| 6 | R | 10 | 15 | 60 | 65 | 60 | 60 |
| L | 10 | 10 | 50 | 65 | 60 | 60 | |
| 7 | R | 35 | 45 | 55 | 50 | 50 | 65 |
| L | 35 | 40 | 55 | 50 | 50 | 65 | |
| 8 | R | 60 | 70 | 85 | 75 | 70 | 65 |
| L | 85 | 85 | 85 | 90 | 80 | 90 | |
| 9 | R | 10 | 10 | 10 | 55 | 90 | 75 |
| L | 15 | 10 | 10 | 55 | 80 | 80 | |
| 10 | R | 25 | 35 | 65 | 95 | 110 | nr |
| L | 25 | 40 | 55 | 70 | 65 | 70 | |
| 11 | R | 50 | 70 | 90 | 90 | 85 | nr |
| L | 50 | 65 | 95 | 100 | 115 | nr | |
| 12 | R | 45 | 70 | 90 | 95 | 95 | * |
| L | 40 | 65 | 80 | 90 | 90 | * | |
| 13 | R | 0 | 5 | 5 | 90 | 95 | 75 |
| L | 5 | 10 | 20 | 95 | 95 | 80 | |
| 14 | R | 50 | 55 | 70 | 80 | 95 | * |
| L | 60 | 65 | 80 | 95 | 100 | * | |
| 15 | R | 30 | 40 | 45 | 75 | 85 | nr |
| L | 30 | 40 | 60 | 90 | 100 | nr | |
| 16 | R | 15 | 25 | 75 | 115 | 110 | * |
| L | 10 | 25 | 60 | 105 | 110 | nr | |
| 17 | R | 15 | 35 | 75 | 115 | 115 | 95 |
| L | 15 | 20 | 85 | 105 | 105 | nr | |
| Mean | R | 33.2 | 43.8 | 60.6 | 76.2 | 77.1 | 62.3 |
| L | 34.4 | 42.6 | 60.0 | 76.5 | 76.2 | 61.4 |
threshold unavailable;
nr = no response at audiometer limits
Participants were all consistent, full-time hearing aid users who wore Phonak products with NLFC activated. Duration of NLFC use at the time of testing with laboratory aids ranged from 1 mo to 3 yr (mean = 1 yr 6 mo). Participants’ personal hearing aids were fitted by their managing audiologist according to DSL v5.0 targets using probe microphone measurements (Bagatto et al. 2005; Scollie et al. 2005). The NLFC settings were established and verified using an approach developed at the University of Western Ontario (Glista & Scollie 2009), where Phonak default NLFC settings are adjusted as needed to maximize audibility of filtered speech bands and accommodate patient feedback. Further information on personal hearing aids and participants can be found in Table 2.
Table 2.
List of factors related to the participants and their personal hearing aids.
| Participant | Age (yrs) |
Age of HL identification (yrs) |
Duration of hearing aid use (yrs) |
Duration of NFC use (yrs) |
Current Amplification |
|---|---|---|---|---|---|
| 1 | 10.13 | 5.00 | 4.88 | 0.75 | Exelia micro |
| 2 | 10.82 | 5.52 | 5.20 | 1.99 | Naida V SP |
| 3 | 9.70 | 3.58 | 5.55 | 0.10 | Solana micro P |
| 4 | 17.09 | 1.16 | 14.00 | 2.31 | Naida V SP |
| 5 | 9.41 | 1.73 | 7.44 | 1.71 | Naida V SP |
| 6 | 15.50 | 6.00 | 9.50 | 2.12 | Naida V SP |
| 7 | 13.19 | 4.01 | 8.93 | 1.55 | Naida V SP |
| 8 | 11.23 | 0.41 | 10.73 | 0.66 | Nios V micro |
| 9 | 13.31 | 5.00 | 8.31 | 0.56 | Exelia Art M |
| 10 | 10.28 | 0.12 | 10.12 | 2.44 | Naida IX SP |
| 11 | 9.57 | 0.25 | 9.16 | 1.43 | Exelia Art SP |
| 12 | 11.18 | 3.00 | 7.93 | 1.94 | Naida IX SP |
| 13 | 15.77 | 2.55 | 12.95 | 1.73 | Naida V SP |
| 14 | 10.44 | 0.25 | 10.12 | 1.55 | Nios V micro |
| 15 | 13.96 | 4.00 | 9.86 | 0.60 | Nios micro V |
| 16 | 15.68 | 2.90 | 12.68 | 2.99 | Naida IX SP |
| 17 | 10.94 | 0.16 | 10.69 | 2.18 | Naida V SP |
|
| |||||
| Mean | 12.25 | 2.68 | 9.30 | 1.56 | |
Laboratory Hearing Aid Fitting and Verification
For testing with laboratory hearing aids, children were fitted with Phonak Naida V SP behind-the-ear hearing instruments coupled to their personal earmolds. Laboratory hearing aids were programmed in advance of the session for children with a recent audiogram (within six months) and measured real-ear-to-coupler differences (within one year) from the UNC Pediatric Audiology Clinic. For all other participants, these measurements were obtained by an audiologist in the laboratory on the day of the evaluation prior to testing. Hearing aids were programmed using Phonak IPFG Fitting software according to DSL v. 5.0 targets (Bagatto et al. 2005; Scollie et al. 2005) using simulated real-ear measures and real-ear-to-coupler differences. Hearing aid verification was performed in a 2-cc coupler using the Audioscan Verifit. The feedback cancellation feature was activated for all participants, but all other advanced and automatic technologies were deactivated during testing with the laboratory aids.
Two listening programs were created and saved in the laboratory aids: 1) NLFC on and 2) NLFC off. During programming, the NLFC feature in the hearing aids (i.e., SoundRecover) was initially turned off while the aided response to a standard speech passage was measured for soft, medium and loud inputs (55, 65, and 75 dB SPL, respectively). The maximum power output of the hearing aids was verified using a swept pure tone. Gain adjustments were made to match targets where possible; accurate fits to targets (within 5 dB) could not be achieved in all participants for all mid-to-high frequencies. After fine-tuning was completed with NLFC off, this program was duplicated to create the NLFC on program. The amount of NLFC applied in laboratory aids was determined using the SoundRecover Fitting Assistant, a free web-based application (Alexander 2009). This method for assigning NLFC settings was used because: 1) it provides an objective, reproducible means of assigning compression parameters, 2) it yields an estimate of audible bandwidth with compression that could potentially inform subsequent analyses, and 3) it has a reasonable, theoretically-driven underlying rationale – to maximize audible bandwidth with minimal compression (to achieve audibility with the least cost to frequency resolution). Unlike other fitting approaches, SoundRecover Fitting Assistant does not rely on patient feedback, /s, ∫/ discriminability, or interpretation of verification tracings with filtered bands to select compression settings. Instead, it uses the maximum audible output of the hearing aid without NLFC, defined as the intersection point between the aided speech spectrum and audiometric thresholds, to determine ideal start frequency and compression ratio settings from those available to each individual patient in the fitting software. Here, the intersection of the average line of an aided standard speech passage played at 65 dB SPL was used to determine the intersection point, although this fitting method also supports use of the peak line of the aided spectrum for determining the maximum output.
After compression settings were established, NLFC processing was verified using modified versions of the standard speech passage (i.e., filtered speech bands) that allow for visualization of compression effects. The filtered speech bands have a 30-dB reduction in gain for frequencies above 1000 Hz, except for a 1/3 octave-wide band of energy centered at 3150, 4000, 5000 or 6300 Hz. The introduction of NLFC is intended to increase access to high-frequency stimuli, effectively increasing the bandwidth of audibility. The predicted increase in audible bandwidth with NLFC can be estimated using the SoundRecover Fitting Assistant (Table 3). For the present work, this difference was further quantified for individual listeners as the difference in audible bandwidth for laboratory aids with NLFC on and NLFC off, with bandwidth in logarithmic units. Compression settings were verified at 55, 65, 70, and 75 dB SPL, and the number of filtered bands that were audible with compression was documented for each participant (Table 4). Audibility was defined herein as a positive difference, in dB SPL, between the center of a given filtered band (aided, compressed curve) and the audiometric threshold at the corresponding frequency.1 All but two participants demonstrated audibility for two or more filtered bands in at least one ear for an input level of 65 dB SPL. Exceptions were participants 16 and 17, who demonstrated audibility of two or more bands in at least one ear for only the highest input level (75 dB SPL).2 These procedures may underestimate participants’ audibility with compression because the filtered bands are representative of the average energy in a given frequency region, whereas peak energy of natural speech can be substantially higher than the average.
Table 3.
Table displaying audible bandwidth (ABW) for each participant (better hearing ear) wearing laboratory hearing aids with Sound Recover activated (“On”) and without Sound Recover activated (“Off”). Participants are ordered according to the log difference in audible bandwidth with NLFC on and off (from smallest to largest). (Note: The audible bandwidth of two participants is reported as 8500Hz, which reflects the last frequency visibly audible on the Verifit.)
| ID | ABW - Off | ABW - On |
|---|---|---|
| 1 | 8500 | 9520 |
| 2 | 8500 | 9520 |
| 3 | 7360 | 8880 |
| 4 | 7529 | 9190 |
| 5 | 8000 | 9840 |
| 6 | 7218 | 8880 |
| 7 | 6979 | 8880 |
| 8 | 6372 | 8340 |
| 9 | 5907 | 8560 |
| 10 | 5416 | 8102 |
| 11 | 4360 | 7600 |
| 12 | 3473 | 7280 |
| 13 | 3053 | 6640 |
| 14 | 2808 | 6640 |
| 15 | 2649 | 6320 |
| 16 | 1879 | 4600 |
| 17 | 1500 | 4600 |
Table 4.
Summary of the number of filtered bands audible with NLFC active for soft (55 dB SPL), average (65 dB SPL), loud (70 dB SPL), and very loud (75 dB SPL) input levels. Cases of shoulder audibility, indicated with asterisks, were not included in the total count.
| Participant | Ear | 55 | 65 | 70 | 75 |
|---|---|---|---|---|---|
| 1 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 2 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 3 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 4 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 5 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 6 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 7 | R | 4 | 4 | 4 | 4 |
| L | 4 | 4 | 4 | 4 | |
| 8 | R | 4 | 4 | 4 | 4 |
| L | 1 | 4 | 4 | 4 | |
| 9 | R | 0* | 3 | 4 | 4 |
| L | 3 | 4 | 4 | 4 | |
| 10 | R | 0 | 0* | 0* | 3 |
| L | 4 | 4 | 4 | 4 | |
| 11 | R | 0 | 3 | 4 | 4 |
| L | 0 | 0 | 4 | 4 | |
| 12 | R | 0 | 2 | 3 | 3 |
| L | 0 | 3 | 4 | 4 | |
| 13 | R | 0 | 3 | 4 | 4 |
| L | 0 | 2* | 2 | 4 | |
| 14 | R | 0 | 3 | 4 | 4 |
| L | 0 | 2 | 3 | 3 | |
| 15 | R | 0 | 2* | 4 | 4 |
| L | 0 | 0 | 3 | 3 | |
| 16 | R | 0 | 0 | 0* | 0* |
| L | 0 | 0 | 0* | 2 | |
| 17 | R | 0 | 0 | 0 | 0* |
| L | 0 | 0 | 0 | 2 | |
| Mean | R | 1.88 | 2.82 | 3.24 | 3.41 |
| L | 2.12 | 2.76 | 3.29 | 3.65 |
Experimental Procedures
The primary motivation underlying this study was to compare speech perception performance with the same participants using laboratory hearing aids with NLFC on and off. However, baseline measures (testing with participants’ personal hearing aids) were also obtained for a complementary study comparing performance in children with hearing loss and age-matched peers with normal hearing (Leibold et al. 2013). Thus, each participant completed the speech perception measures with their personal hearing aids (NLFC on) and twice with laboratory aids (NLFC on, NLFC off). The order of testing with laboratory hearing aids (NLFC on and NLFC off) was counterbalanced across participants, but baseline testing with personal hearing aids was always completed first. Before testing with laboratory aids, children listened in the assigned hearing aid program for a period of 15 minutes. During this time, the children and their parents were instructed to converse with one another naturally, or to engage in games promoting communication (e.g., “I Spy”). In addition to providing designated breaks, this offered participants an opportunity to listen to their own voice as well as the voices of others before testing. No specific questions or discussion points were introduced by study personnel. Additional short breaks (i.e., lasting approximately 5 minutes) were provided throughout the test session as needed to prevent participant fatigue. Testing with personal and laboratory hearing aids was completed in a single, 2 ½ hour session.3 All testing was completed in a double-walled sound proof booth (IAC). Stimuli were presented in the sound field via a loudspeaker located 1 meter directly in front of the participant (0° azimuth, 0° elevation). Test order for the speech perception tasks described below was randomized across participants, but was identical for baseline and both laboratory hearing aid conditions within individual participants.
Closed-Set Speech Perception Tests
Consonant Identification in Quiet
The consonant identification measure is a closed-set, 12 alternative-forced-choice task. The measure is motivated by the Audiovisual Feature Test for Young Children (Tyler et al. 1991).
Stimuli
Stimuli were 12 phonemes produced in isolation by a native English-speaking female. The syllables were comprised of an initial consonant (i.e., /b, s, d, h, k, m, n, p, t, v, z, ∫/) followed by the /i/ vowel. The duration of the tokens ranged from 458 to 620 ms (mean = 523 ms). The average root-mean-square (rms) level of the tokens was equalized, and stimuli were presented in quiet at a fixed level of 70 dB SPL. The center of gravity (i.e. weighted mean frequency) and the standard deviation of the power spectrum were obtained for each consonant using praat (Boersma & Weenink 2009). Each token was first low pass filtered at 300 Hz to reduce the influence of the speaker's fundamental frequency (approximately 270 Hz). Center of gravity values ranged from 445 to 10,067 Hz (Table 5).
Table 5.
The center of gravity (COG) and standard deviation values in Hz were computed for each token from the consonant confusion task. The values represent the frequency place and region containing predominant spectral energy for the excised portion of consonant-vowel utterances (consonant-only, excluding formant transitions) above the frequency of voicing (low-pass filter cut-off = 300 Hz). The four tokens used in the high-frequency subset analysis appear in a darker gray and those in the mid-frequency analysis in lighter gray.
| Consonant | COG | St Dev |
|---|---|---|
| s | 10067 | 1450 |
| z | 8646 | 4029 |
| d | 6909 | 1073 |
| t | 6323 | 1324 |
| k | 4680 | 2255 |
| ʃ | 4620 | 997 |
| p | 3530 | 1849 |
| h | 3318 | 1663 |
| v | 1943 | 3048 |
| b | 788 | 906 |
| n | 450 | 240 |
| m | 445 | 207 |
Procedure
Testing consisted of five blocks of 12 stimulus presentations per block. Each token occurred once per block in random order for a total of 60 trials (5 repetitions per consonant). Pictures representing each of the 12 consonant-vowel stimuli appeared on a single 8 inch x 10 inch laminated card. After each stimulus presentation, participants pointed to the picture that represented the consonant they thought they heard. An experimenter located in the room behind the child entered each response into the computer and initiated trials. No feedback was provided. Stimulus presentation and response logging was controlled using a custom MATLAB program. To achieve the desired presentation level, stimuli were amplified (Techron 5507) and attenuated (TDT PA5) before being routed through a headphone buffer (TDT HB6) to a loudspeaker (Monitor Audio, Monitor 4) located in the sound proof booth. Stimulus presentation level was verified in advance of each session using a Larson Davis (Model 824) sound level meter.
Spondee Identification in Competing Backgrounds
The spondee identification measure was based on a four alternative-forced-choice task developed by Hall et al. (2002). It was applied here to investigate the influence of NLFC processing on spondee identification in two different types of competing maskers: (1) speech-shaped noise, or (2) two-talker speech. Spondees were selected as the target stimuli based on pilot data showing that children with varying degrees and configurations of hearing loss could successfully discriminate these targets in the presence of both maskers.
Stimuli
The target speech tokens were twenty-five spondees, or words with equal stress on each of two syllables. Each spondee word was represented by a unique picture. The spondee words were produced in isolation by a native English-speaking female. The tokens varied in overall duration (range = 845 - 1412 ms, mean = 1126 ms), and were scaled so that the average rms level was equalized across all spondees.
The masker was either two-talker speech or speech-shaped noise. The two-talker speech masker was comprised of separate recordings from different English-speaking females reading popular children’s books. After the two individual streams were recorded and digitized, each recording was manually edited so that silent gaps of 300 ms or greater were removed. One edited sample was 3.1 minutes in length, and the other edited sample was 3.5 minutes in length. Each sample was repeated without discontinuity to create a continuous one-hour speech stream. The rms levels of the two streams were equated, and the streams were digitally mixed to create the two-talker masker. The speech-shaped noise masker was based on the magnitude spectrum of the two-talker speech. For testing, the signal and masker were mixed (TDT SM3), and then routed using the same hardware described above for the consonant identification measure. Stimulus control and presentation was achieved using a custom MATLAB program, and presentation levels of the stimuli were calibrated as described above for the consonant identification measure.
Procedure
Before testing, children were familiarized with the spondees in quiet. An experimenter pointed to each picture on a laminated card and recited the corresponding spondee word aloud. During testing, target words were embedded in either the speech-shaped noise or the two-talker speech masker. Participants were asked to select the picture from a set of four, including the target and three foils, each depicting a different spondee word. Target words were randomly selected from the full set of 25, and foils were randomly selected without replacement from the remaining 24 possibilities. Pictures were displayed on a 7” handheld touch screen monitor (MIMO), with the quadrant positions of the target and foils randomly determined. Responses registered on the handheld device were recorded in MATLAB. Visual feedback was provided after each trial in the form of the correct picture flashing four times on the touchscreen.
The spondee targets were presented at a fixed level of 65 dB SPL throughout testing, and the level of the masker was adapted. The initial presentation levels of the two-talker and speech-shaped noise masker were 50 and 55 dB SPL, respectively. These starting levels were expected to be approximately 10-15 dB below participants’ final masker thresholds. Starting levels differed across the two maskers because pilot work indicated that the two-talker masker was more challenging for children with hearing loss compared to the speech-shaped noise masker. Level changes occurred during inter-stimulus intervals, and a 0.75-second pause was executed after changes in masker level and prior to presentation of the next word. Masker level was determined using a 2-up, 1-down staircase procedure, which estimated the masker level associated with 70.7 % correct spondee identification (Levitt 1971). The initial step size was 4 dB, which decreased to 2 dB after 2 reversals. The track terminated after 8 reversals, and the threshold estimate was calculated as the average masker level on the last 6 reversals. Each participant completed at least two runs in presence of each masker. When threshold estimates differed by more than 5 dB across tracks for a given masker, the task was repeated a third time. The final threshold reflects the average of the two runs with the most similar threshold estimates. The order in which testing was performed with each masker was counterbalanced across participants, but all runs were completed for one masker before testing began with the other.
RESULTS
Effects of NLFC: Laboratory Hearing Aids
Consonant identification in quiet
Overall percent correct consonant identification was computed for each participant (n = 17) on all 12 tokens (60 total responses) for both hearing aid configurations. The range of percent correct scores across participants for the 12-token composite sample ranged from 55.0 to 93.3 % (mean = 76.5 %) with NLFC on, and from 55.0 to 96.7 % (mean = 78.9 %) with NLFC off. Percent correct scores were converted to rationalized arcsine units (RAUs) for statistical analysis (Studebaker 1985). The transformed scores were analyzed using a repeated-measures analysis of variance (ANOVA) with the within-subjects factor of hearing aid condition (NLFC on, NLFC off). The main effect of hearing aid condition was not significant (F 1, 16 = 1.67; p = 0.22), indicating similar performance for participants with and without NLFC activated.
Following Miller and Nicely (1955), an analysis of information transfer for three phonetic features of speech (i.e., manner, place, and voicing) was conducted to uncover the nature of the errors exhibited in the two hearing aid conditions. Information transmitted in each feature category was normalized to a range of 0 – 1, to facilitate comparisons across the three features. Transmission rates did not appear to differ across NLFC on and off conditions within a given feature. However, a difference across features was apparent, with transmission being substantially poorer for place than for manner or voicing, irrespective of hearing aid condition. Statistical analyses were performed to investigate the significance of these trends. A two-way within-subjects ANOVA of normalized transmission showed no significant main effect of hearing aid condition (F 1, 16 = 0.00, p = 1.0), indicating that information transfer was similar with NLFC on and off. There was a significant main effect of feature (F 2, 32 = 60.47, p < 0.001), but the interaction term was not significant (F 1, 16 = 0.00, p = 1.0). Pairwise comparisons (with Bonferroni correction) indicated that information transfer was lower for place than for either manner (p < 0.001) or voicing (p < 0.001). There was no significant difference in information transfer between manner and voicing (p = 1.0).
Surprisingly, few errors in the identification of /s/ and / ∫/ were observed for the majority of participants in either hearing aid condition, sounds for which improved detection and discrimination with NLFC have been previously reported (Glista et al. 2009; Wolfe et al. 2010, Wolfe et al. 2011). Single-token analysis revealed high average identification scores in both hearing aid conditions for /s/ (NLFC on = 88.2%, NLFC off = 87.1%) and /∫/ (NLFC off = 92.9 %, NLFC on = 97.6 %). The most common errors of place were reports of “m” for “n” and “z” for “v”. Responses of “t” for presentations of “k” were also observed, although less frequently.
The a priori prediction for consonant identification performance in quiet was that participants would benefit from NLFC when access to high-frequency information was critical, but not when consonant identification relied on mid-frequency information. Thus, percent correct scores were calculated for two subgroups of tokens: (1) the four consonants with the greatest high-frequency energy, /s, z, d, t/ (6323 – 10,067 Hz), and (2) the four consonants with dominant mid-frequency energy / k, ∫, p, h/ (3318 – 4680 Hz). Individual and group-average percent correct scores are shown in Figure 1 for the high- (top panel) and mid-frequency (bottom panel) subsets. Data are sorted along the x-axis based on the increase in audible bandwidth with NLFC activation (difference in the logarithm of the audible bandwidth with NLFC on versus off) in the better hearing ear; mean scores appear on the far right side of each graph.
Figure 1.
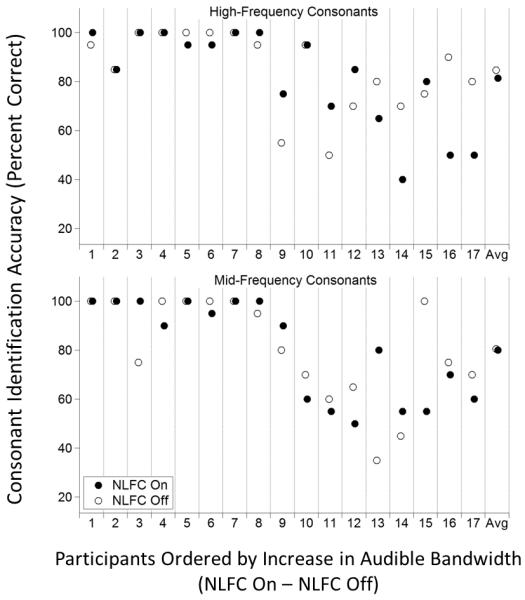
Individual and group-average consonant identification accuracy scores are shown for NLFC on (filled circles) and NLFC off (open circles), both using laboratory hearing aids. The top panel shows results for the four consonants with the greatest high-frequency energy (/s, z, d, t/), and the bottom panel shows results for the four consonants with dominant mid-frequency energy (/k, ∫, p, h/). Participant number, indicated on the abscissa, reflects the change in audible bandwidth with NLFC in the better ear: participant #1 had the smallest change in bandwidth, and participant #17 had the largest.
Visual inspection of the data suggests that consonant identification abilities were generally poorer in individuals with increasing difference in audible bandwidth, which closely corresponds to increasing unaided thresholds. However, no systematic differences in the datasets were evident between NLFC on (filled circles) and NLFC off (open circles) for either the high- or mid-frequency tokens. Average performance was similar with NLFC activated and deactivated for the high-frequency (NLFC on = 81.5 %, NLFC off = 84.7 %) and mid-frequency (NLFC on = 80.0 %, NLFC off = 80.6 %) subsets. A repeated-measures ANOVA on RAU scores was conducted to evaluate the statistical trends in the data shown in Figure 1. This analysis included the within-subjects factors of hearing aid condition (NLFC on, NLFC off) and consonant frequency (high, mid). There was no main effect of hearing aid condition (F 1, 16 = 0.40; p = 0.54) or consonant frequency (F 1, 16 = 0.30; p = 0.59). The hearing aid condition X consonant frequency interaction was also not significant (F 1, 16 = 0.07; p = 0.79). In summary, this pattern of statistical results indicates no effect of NLFC on performance with laboratory hearing aids for either high- or mid-frequency consonants, with similar performance across the two subsets of tokens.
One factor to consider in evaluating the lack of an effect of NLFC on mid-versus high-frequency consonant identification is that fact that participants made relatively few errors overall. For example, percent correct scores were 80 % or better in both hearing aid conditions for 7 of the 17 participants for the full set of 12 tokens. The relatively small number of errors introduces the question of whether the ease of the task and/or the speech perception abilities of the sample of children included in this study limited the ability to observe a benefit of NLFC. To examine the influence of task difficulty and rule out possible ceiling effects, supplemental data were collection from a subset of participants on the consonant identification task in speech-shaped noise. Seven participants returned for testing with laboratory aids (NLFC on and off) in the presence of a speech-shaped noise masker. All returning subjects were “high performers” in quiet, with average consonant identification scores ranging from 85.0 – 91.7 % (NLFC on) and 71.7 – 96.7 % (NLFC off). These participants completed testing in noise an average of 9 months after completion of the initial test battery (range = 5 – 13 mos). The test procedure was the same as that described above, except that a speech-shaped noise masker was played continuously throughout the experiment at a presentation level equal to that of the signal (0 dB SNR). Group-average scores on the 12-token consonant identification measure were reduced from 88.8 % in quiet to 73.1 % in noise using laboratory aids with NLFC on, and from 88.6 % in quiet to 69.5 % in noise using laboratory aids with NLFC off. Despite the increased task difficulty, no systematic differences in performance were observed across the two hearing aid conditions in the presence of the noise masker. A repeated-measures ANOVA of the transformed RAU scores in noise, with hearing aid condition (NLFC on, NLFC off) as a factor, confirmed that the main effect of hearing aid condition was not significant (F 1, 6 = 2.06; p = 0.20). Consistent with data collected in quiet, the most common errors for data collected in noise represented confusions between ‘m’ and ‘n’, and confusions between ‘v’ and ‘z’.
Spondee identification in competing backgrounds
To examine the influence of hearing aid condition on spondee identification in the presence of each competing background, estimates of masker thresholds corresponding to 70.7 % correct spondee identification were compared across masker type (speech-shaped noise, two-talker speech) and hearing aid condition (NLFC on, NLFC off). Figure 2 displays individual and group average masker thresholds for the speech-shaped noise (top panel) and two-talker speech (bottom panel) conditions. Individual data are rank ordered on the abscissa based on the increase in audible bandwidth with NLFC activation in the better hearing ear. Thresholds for the speech-shaped noise condition ranged from 66.3 to 73.0 dB SPL (mean = 70.1 dB SPL) with NLFC on, and from 65.2 to 74.0 dB SPL (mean = 70.1 dB SPL) with NLFC off. Although performance was generally poorer in the two-talker compared to the noise masker, a similar lack of trend was observed with respect to hearing aid condition for the two-talker condition, where thresholds ranged from 62.2 to 72.7 dB SPL (mean = 67.0 dB SPL) with NLFC on, and from 64.0 to 73.0 (mean = 67.0 dB SPL) with NLFC off. Results of a repeated-measures ANOVA on threshold with the within-subjects factors of masker type (speech-shaped noise, two-talker speech) and hearing aid condition (NLFC on, NLFC off) confirmed a significant main effect of masker condition (F 1, 16 = 49.2; p < 0.001; ηp2 = 0.76). There was no main effect of hearing aid condition (F 1, 16 = 0.00; p = 0.998) and no interaction between masker type and hearing aid condition (F 1, 16 = 0.00; p = 0.977), indicating that NLFC did not influence spondee identification in either masker.
Figure 2.
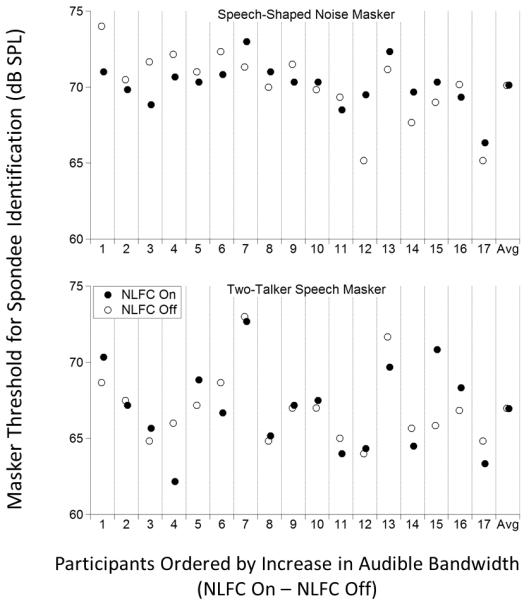
Individual and group-average masker thresholds in dB SPL are shown for the spondee recognition task. As in Figure 1, symbols size indicates NLFC on (filled circles) and NLFC off (open circles), both using laboratory hearing aids, and participant number, indicated on the abscissa, reflects the change in audible bandwidth with NLFC in the better ear. The top panel shows results in the speech-shaped noise masker, and the bottom panel shows results in the two-talker speech masker.
Predictor(s) of Individual Differences in Effects of NLFC
No significant effect of NLFC was observed in group data using laboratory hearing aids with NLFC on versus NLFC off for consonant identification in quiet, spondee identification in speech-shaped noise, or spondee identification in two-talker speech. However, considerable individual differences were observed for all three measures. Previous studies have also reported substantial between-subjects variability in outcomes associated with NLFC (e.g., Glista et al. 2009). Thus, multiple linear regression analyses were performed to explore subject-specific factors that might predict the range of effects observed. Stepwise regression analyses were performed on difference scores across hearing aid conditions (NLFC on – off) for high- and mid-frequency consonant identification in quiet, and for spondee identification thresholds obtained in each of the two competing maskers. Significant predictor variables (p < 0.05) were included in the models in a stepped fashion; factors that failed to significantly contribute to the regression equation were excluded. The following two independent variables were considered for each regression model: (1) difference in the logarithm of audible bandwidth with NLFC on versus off in the better hearing ear, and (2) total duration of NLFC use on personal hearing aids. The first variable provided an estimate of the improvement in audible bandwidth with NLFC activated, and the second was included to determine whether prior listening experience with NLFC processing (on personal hearing aids) influenced the extent of NLFC-related changes in performance. A third factor offering gross information regarding participants’ high-frequency hearing status (audiometric threshold at 4000 Hz for the better ear) was originally selected to be included in the analyses, but was excluded because it was strongly correlated with the difference audible bandwidth (r = 0.85, p = 0.001).
For high-frequency consonant identification in quiet, the regression analysis indicated thatone predictor, the logarithm of the difference in audible bandwidth, explained 23% of the variance in the NLFC on versus NLFC off difference (adjusted R2 = 0.230, F 1, 15 = 5.78, p = 0.03). Similarly, the logarithm of the difference in audible bandwidth explained 30% of the variance in the NLFC on versus NLFC off difference in spondee identification performance in the speech-shaped noise masker (adjusted R2 = 0.305, F 1, 15 = 8.02, p = 0.01). The change in audible bandwidth with compression was negatively correlated with the difference in performance across NLFC on and NLFC off conditions for high-frequency consonant identification (ϐ = −0.53), suggesting that children with more aggressive compression settings as the result of greater high-frequency hearing loss were less likely to benefit from NLFC. In contrast, the change in audible bandwidth with compression was positively correlated with the difference in performance across NLFC on and off conditions for spondee identification in the speech-shaped noise masker (ϐ = 0.59), suggesting that children with more aggressive compression settings as the result of greater high-frequency hearing loss were more likely to benefit from NLFC. Neither subject variable predicted performance differences with NLFC on versus off for mid-frequency consonant identification in quiet or for spondee identification in the two-talker masker.
Effects of NLFC Settings: Personal versus Laboratory Hearing Aids
The primary goal of this study was to compare speech perception outcomes within the same individuals using laboratory hearing aids with NLFC on and off. The focus on performance with laboratory aids ensured consistency across participants in terms of both technology and the underlying fitting strategy. Prior to testing with laboratory aids, however, each participant completed the assessment wearing their own hearing aids. Unlike previous studies investigating effects of NLFC in children, all participants wore personal hearing aids with NLFC activated. Moreover, the personal hearing aids worn by nearly half of all participants (7/17) were the same model as the laboratory hearing aids used in the present study. However, one distinguishing feature between the children’s personal hearing aids and the laboratory aids with NLFC activated was the frequency-compression parameters. Thus, comparison of performance with personal aids versus laboratory aids provides an opportunity to investigate the influence of NLFC settings on speech perception outcomes, with the important caveat that baseline testing with participants’ own hearing aids was always completed before testing with laboratory hearing aids.
Comparison of Frequency-Compression Parameters
The mean start frequency for NLFC processing was 2.8 kHz for personal hearing aids, compared to 3.5 kHz for laboratory aids with NLFC on. The results of a paired-samples, two-tailed t-test revealed that mean start frequency values were significantly lower for the baseline than for NLFC on condition (t 16 = −2.62, p = 0.02). On average, more mid-frequency speech was compressed when children wore their personal hearing aids compared to when they were tested with NLFC activated in the laboratory aids. Similarly, mean data showed an average compression ratio of 3.1:1 for personal hearing aids, and 2.8:1 for laboratory hearing aids. However, no significant difference in mean compression ratio values was found between personal and laboratory hearing aids (t 16 =−1.75, p = 0.10).
Consonant identification in quiet
Figure 3 plots average performance (in RAUs) for personal (shaded bars) and laboratory (open bars) hearing aids for high-frequency (left) and mid-frequency (right) consonant identification. Error bars show ± SEM of the average transformed scores. High-frequency consonant identification appeared to be similar with personal (mean = 84.6 RAUs) and laboratory (mean = 85.3 RAUs) hearing aids. However, mid-frequency consonant identification appeared to be more accurate with personal (mean = 96.0 RAUs) than with laboratory (mean = 84.3 RAUs) hearing aids. To test the statistical significance of the trends observed in Figure 3, a repeated-measures ANOVA on RAU score was performed with hearing aid (personal, laboratory) and consonant frequency (high, mid) as within-subjects factors. The main effect of hearing aid was significant (F 1, 16 = 4.60; p = 0.048; ηp2 = 0.22), indicating better consonant identification accuracy with personal compared to laboratory hearing aids. The main effect of consonant frequency did not reach statistical significance (F 1, 16 = 4.28; p = 0.06). The interaction between hearing aid and consonant frequency was not significant (F 1, 16 = 2.57; p = 0.13).
Figure 3.

Transformed group-average consonant accuracy scores (± 1 SEM) are shown for apersonal hearing aids (shaded bars) and for laboratory hearing aids (open bars), both with NLFC activated. Results for the four consonants with the greatest high-frequency energy (/s, z, d, t/) are shown on the left, results for the four consonants with dominant mid-frequency energy (/k, ∫, p, h/) are shown on the left right.
Spondee identification in competing backgrounds
Figure 4 shows average masker levels at threshold for participants wearing personal (shaded bars) and laboratory (open bars) hearing aids. Error bars show ± 1 SEM. For the speech-shaped noise condition, masker thresholds ranged from 66.3 to 72.8 dB SPL (mean = 69.8 dB SPL) with personal hearing aids, and from 66.3 to 73.0 dB SPL (mean = 70.1 dB SPL) with laboratory aids. In contrast to the speech-shaped noise condition, thresholds for the two-talker masker condition appeared to be higher (indicating better performance) with laboratory compared to personal hearing aids. Thresholds ranged from 62.0 to 68.3 dB SPL (mean = 64.9) with personal hearing aids, and from 62.2 to 72.7 dB SPL (mean = 67.0) with laboratory aids. A repeated-measures ANOVA on masker threshold was performed to examine the trends observed in Figure 4. This analysis included the within-subjects factors of hearing aid (personal, laboratory) and masker type (speech-shaped noise, two-talker speech). The ANOVA indicated significant main effects for hearing aid (F 1, 16 = 7.38; p = 0.02; ηp2 = 0.32) and for masker type (F1, 16 = 79.54; p < 0.0001; ηp2 = 0.83), and a significant hearing aid type X masker type interaction (F 1, 16 = 5.55; p = 0.03; ηp2 = 0.26). Follow-up paired samples t-tests on the interaction indicated lower thresholds for the two-talker condition with personal compared to laboratory hearing aids (t 16 = 3.27; p = 0.005), suggesting that participants were more detrimentally affected by the two-talker masker when they wore their personal hearing aids as compared to when they wore their laboratory hearing aids. No significant difference in masker thresholds was observed between personal and laboratory hearing aids for the speech-shaped noise condition (t 16 = 0.65; p = 0.53).
Figure 4.

Group-average masker thresholds in dB SPL (± 1 SEM) are shown for personal hearing aids (shaded bars) and for laboratory hearing aids (open bars), both with NLFC activated. Results in the speech-shaped noise masker are shown on the left, and results in the two-talker speech masker are shown on the right.
To investigate possible practice effects for the spondee identification task in the two-talker masker, thresholds from the first and second threshold estimation track in the baseline condition were compared using a paired-samples t-test. Results indicated that the first threshold estimate (mean = 64.0 dB SPL) was significantly lower than the second (mean = 65.8 dB SPL; t 16 = −3.03, p = 0.008), providing evidence of improvement. In contrast, there was no significant difference between the first (mean = 69.5 dB SPL) and second (mean = 70.0 dB SPL) baseline threshold estimates in the speech-shaped noise masker (t 16 = −0.81, p = 0.43). It is therefore plausible that listeners’ relative better performance for NLFC on and off laboratory conditions in the two-talker masker relative to their baseline performance wearing personal hearing aids reflects some benefit from task familiarity or training.
DISCUSSION
Effects of NLFC: Laboratory Hearing Aids
Consonant Identification in Quiet
No effect of NLFC was observed with laboratory hearing aids on overall, high-frequency, or mid-frequency consonant identification. The lack of a significant effect of NLFC was evident in the data obtained from the group of 17 participants tested in quiet, and also in the subset of data obtained from participants (n = 7) who returned to the laboratory for testing in the presence of speech-shaped noise. The lack of a significant effect of frequency-compression processing for the consonant identification measure with laboratory hearing aids is somewhat unexpected, given reports in the literature showing improved /s, ∫/ discrimination, plural identification, and high-frequency consonant recognition with NLFC (Glista et al. 2009; Wolfe et al. 2011). Several factors may contribute to differences between the present study and earlier work. For example, the children enrolled in the study by Glista et al. (2009) had mean better-ear pure tone thresholds of approximately 90 dB SPL at 4000 and 6000 Hz (estimated from Figure 1, p. 634), whereas our participants had a mean better-ear threshold of 72 dB SPL at 4000 Hz. It is also possible that the relatively favorable presentation level (70 dB SPL) precluded measurement of NLFC effects; gain limitations are less likely at high levels, and the need for NLFC is likewise reduced. Hence, further investigation into benefits with soft or average speech may be worthwhile. Nonetheless, the observation that most of the children with hearing loss included in the present study were capable of successful high-frequency consonant identification of loud conversational level speech in the absence of NLFC processing provides evidence that NLFC may not be uniformly required to provide access to high-frequency speech information. Contrary to our hypothesis, however, modestly applied compression did not impair mid-frequency consonant identification. This finding may influence future candidacy for NLFC processing, and its applications in hearing aid fitting.
Spondee Identification in Competing Backgrounds
No apparent benefit of NLFC using laboratory hearing aids was observed for spondee identification in the presence of either speech-shaped noise or a two-talker speech masker. This null result may be at least partly attributed to the type of stimuli used in the task. While spondees contain energy across a broad range of frequencies, an experiment with normal-hearing adults suggests that low-pass filtered spondees are readily recognizable even without mid- to high-frequency information (Van Tasell & Yanz 1987). It is reasonable to expect that the children with hearing loss would require a larger bandwidth than normal-hearing adults for masked spondee identification, given prior research showing effects of age and hearing status on bandwidth needs for nonsense syllable perception (Stelmachowicz et al. 2001). However, the present results with laboratory hearing aids do not support the hypothesis that NLFC has a negative effect on spondee identification in either a steady-state noise or a fluctuating speech masker, at least for the relatively modest compression settings applied to the laboratory hearing aids.
Effects of NLFC Settings: Personal versus Laboratory Hearing Aids
Consonant Identification in Quiet
Overall consonant identification accuracy was greater than 75 % for most children with both personal and laboratory hearing aids, but identification of mid-frequency consonants appeared to be more accurate with personal compared to laboratory hearing aids. In contrast, high-frequency consonant identification performance was similar across personal and laboratory hearing aids. Recall that compression settings in personal hearing aids were determined by each child’s managing audiologist, using a clinical approach described by Glista & Scollie (2009). This fitting procedure is largely based on maximizing the audibility of filtered bands during electroacoustic analyses (Glista & Scollie 2009), with compression settings matched across the two ears. In contrast to the compression settings employed in participant’s personal hearing aids, NLFC parameters for laboratory hearing aids with NLFC on were based on the maximum auditory bandwidth of the hearing aid without compression and were ear specific (SoundRecover Fitting Assistant; Alexander 2009). Thus, differences in fitting procedure may be the basis for the differences in performance observed using laboratory compared to personal hearing aids in the present study. However, the potential influence of technology differences between personal and laboratory aids in the 10 children not fitted with the Naida V SP, or differences in the amount of listening experience cannot be ruled out.
Spondee Identification in Competing Backgrounds
One intriguing finding of the present study was the improved spondee identification performance in the two-talker masker using laboratory (NLFC on) compared to personal hearing aids. Given the more aggressive NLFC settings employed in personal compared to laboratory hearing aids, this difference in performance suggests that NLFC has the potential to detrimentally affect the ability to hear out target speech in a complex masker such as competing speech. Interpretation of this finding is tempered due to potential test order effects and potential technology differences, however.
Limitations
There were a number of potential limitations with the present study, one being the short-term acclimatization schedule. A longitudinal study with extended, at-home acclimatization may have revealed differences in speech recognition performance across hearing aid conditions. However, at the current time, evidence supporting the need for extended acclimatization to NLFC is extremely limited (Wolfe et al. 2011). Wolfe and his colleagues (2011) reported improvements in speech perception associated with NLFC after 6 weeks of listening experience, which either stayed the same or increased after 6 months of listening experience. These results were interpreted as suggesting that acclimatization to device programming influences some aspects of speech understanding. However, abrupt changes in speech understanding related to NLFC have also been reported (McCreery et al. 2013). A simulation experiment with normal-hearing adults reported immediate improvements in speech perception when stimuli were digitally treated to mimic “optimized” NLFC parameters as compared to manufacturer default NLFC settings and conventional hearing aid processing with limited bandwidth and without NLFC (McCreery et al. 2013), although it is possible that the linguistic experience of normal-hearing adults played a role in these results. It remains to be seen whether the time-course of acclimatization differs for individuals with and without hearing loss, or for younger and older listeners. The lack of an NLFC-related effect on speech recognition measures with laboratory hearing aids may also be related to the effectiveness of the listeners’ compression prescriptions. Additional research is needed to further investigate how to optimize NLFC settings, and to thoroughly vet the potential benefits and consequences of compression to speech perception in children.
Conclusions
Although use of NLFC processing has become increasingly prevalent in pediatric hearing aid fittings, only limited outcome data are available describing its effect on the speech recognition abilities of children. The present study assessed NLFC in a group of children with mild to profound hearing loss, listening in either quiet or competing backgrounds. While all participants used symmetric NLFC in their personal hearing aids, laboratory hearing aids were fitted using an ear-specific approach that used settings that were typically more conservative than those of the personal hearing aids; participants were provided with a short-term acclimatization to these novel NLFC fittings. In contrast to previous work, findings from the present study show no consistent benefit or detriment of NLFC. There was some indication of participant-specific effects, however, with the speech identification abilities of children with more significant hearing loss and more aggressive compression settings being more likely to be altered by the introduction of NLFC. The manner of this effect was variable, with NLFC negatively impacting high-frequency consonant identification, but improving spondee recognition in speech-shaped noise. Ongoing work is needed to further elaborate the role of compression strength and listening experience on children’s speech perception abilities, and to further inform candidacy and determine the best fitting approach.
Short Summary.
The influence of nonlinear frequency compression (NLFC) processing was examined in children with hearing loss for phoneme identification in quiet, and spondee identification in competing noise or speech. Outcomes were assessed using laboratory hearing aids with NLFC on and off, and personal hearing aids with NLFC on. Results showed no consistent effect of NLFC on speech perception abilities for either measure, although performance differences were greater for children with stronger NLFC settings. Findings from measurements using personal and laboratory aids indicated a need for continued research on the influence of listening experience and NLFC settings on speech perception abilities.
ACKNOWLEDGMENTS
This work was supported by the March of Dimes Foundation (#5-FY10-28) and from the National Institute of Deafness and Other Communication Disorders (R01 DC011038). We are grateful to the members of the Human Auditory Development Laboratory for their assistance with data collection. Adam Jacks and Katarina Haley provided expertise regarding acoustic measurements. Joshua Alexander provided helpful information that was instrumental to the success of this work. We also thank Ryan McCreery for helpful discussions and suggestions.
Footnotes
In some cases there was a positive difference between the left edge of a filtered band and corresponding audiometric threshold, but no audibility at the center of the band. This configuration is described here as ‘shoulder audibility’.
All of the statistical analyses were repeated without the data from the two participants who did not have audibility at 70 dB SPL (participants 16 and 17). The findings described below did not differ between the subset of 15 participants and the full group of 17 participants. Thus, results using the full dataset are reported throughout the manuscript.
Data collection was generally completed in one, 2 ½ hour session, although four participants completed baseline measures during a separate session, 2 – 4 months before testing with laboratory aids.
REFERENCES
- Alexander J. Nonlinear frequency compression: Balancing start frequency and compression ratio. American Auditory Society Annual Meeting; Scottsdale, AZ. 2012. [Google Scholar]
- Alexander JM. Candidacy, selection, and verification of SoundRecover options. 3rd Phonak Virtual Audiology Conference; Omaha, Nebraska. 2009. [Google Scholar]
- Baer T, Moore BC, Kluk K. Effects of low pass filtering on the intelligibility of speech in noise for people with and without dead regions at high frequencies. J Acoust Soc Am. 2002;112:1133–1144. doi: 10.1121/1.1498853. [DOI] [PubMed] [Google Scholar]
- Bagatto M, Moodie S, Scollie S, et al. Clinical protocols for hearing instrument fitting in the Desired Sensation Level method. Trends Amplif. 2005;9:199–226. doi: 10.1177/108471380500900404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boersma P, Weenink D. Praat: doing phonetics by computer (Version 5.1.05) [Computer program] 2009 Retrieved May 1, 2009, from http://www.praat.org/
- Ching TY, Dillon H, Byrne D. Speech recognition of hearing-impaired listeners: predictions from audibility and the limited role of high-frequency amplification. J Acoust Soc Am. 1998;103:1128–1140. doi: 10.1121/1.421224. [DOI] [PubMed] [Google Scholar]
- Cox RM, Alexander GC, Johnson J, et al. Cochlear dead regions in typical hearing aid candidates: prevalence and implications for use of high-frequency speech cues. Ear Hear. 2011;32:339–348. doi: 10.1097/AUD.0b013e318202e982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elfenbein JL, Hardin-Jones MA, Davis JM. Oral communication skills of children who are hard of hearing. J Speech Hear Res. 1994;37:216–226. doi: 10.1044/jshr.3701.216. [DOI] [PubMed] [Google Scholar]
- Glasberg BR, Moore BC. Auditory filter shapes in subjects with unilateral and bilateral cochlear impairments. J Acoust Soc Am. 1986;79:1020–1033. doi: 10.1121/1.393374. [DOI] [PubMed] [Google Scholar]
- Glista D, Scollie S. Modified verification approaches for frequency lowering devices. 20092012:1–11. Audiology Online. Retrieved from http://www.audiologyonline.com/articles.
- Glista D, Scollie S, Bagatto M, et al. Evaluation of nonlinear frequency compression: Clinical outcomes. Int J Audiol. 2009;48:632–644. doi: 10.1080/14992020902971349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall JW, 3rd, Grose JH, Buss E, et al. Spondee recognition in a two-talker masker and a speech-shaped noise masker in adults and children. Ear Hear. 2002;23:159–165. doi: 10.1097/00003446-200204000-00008. [DOI] [PubMed] [Google Scholar]
- Hellgren J, Lunner T, Arlinger S. System identification of feedback in hearing aids. J Acoust Soc Am. 1999;105:3481–3496. doi: 10.1121/1.424674. [DOI] [PubMed] [Google Scholar]
- Hogan CA, Turner CW. High-frequency audibility: benefits for hearing-impaired listeners. J Acoust Soc Am. 1998;104:432–441. doi: 10.1121/1.423247. [DOI] [PubMed] [Google Scholar]
- Killion MC. Problems in the application of broadband hearing aid earphones. In: Studebaker GA, Hochberg I, editors. Acoustic factors affecting hearing aid performance. University Park Press; Baltimore: 1980. pp. 219–264. [Google Scholar]
- Leibold LJ, Hillock-Dunn A, Duncan N, et al. Influence of hearing loss on children’s identification of spondee words in a speech-shaped noise or a two-talker masker. Ear Hear. 2013 doi: 10.1097/AUD.0b013e3182857742. doi: 10.1097/AUD.0b013e3182857742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levitt H. Transformed up-down methods in psychoacoustics. J Acoust Soc Am. 1971;49:467–477. [PubMed] [Google Scholar]
- Lutman ME, Gatehouse S, Worthington AG. Frequency resolution as a function of hearing threshold level and age. J Acoust Soc Am. 1991;89:320–328. doi: 10.1121/1.400513. [DOI] [PubMed] [Google Scholar]
- McCreery RW, Brennan MA, Kopun J, et al. Maximizing audibility and speech recognition with non-linear frequency compression by estimating audible bandwidth. Ear Hear. 2013;34:e24–e27. doi: 10.1097/AUD.0b013e31826d0beb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller G, Nicely P. An analysis of perceptual confusions among some english consonants. J Acoust Soc Am. 1955;27:338–352. [Google Scholar]
- Moeller MP, Hoover B, Putman C, et al. Vocalizations of infants with hearing loss compared with infants with normal hearing: Part I--phonetic development. Ear Hear. 2007;28:605–627. doi: 10.1097/AUD.0b013e31812564ab. [DOI] [PubMed] [Google Scholar]
- Oxenham AJ. Pitch perception and auditory stream segregation: implications for hearing loss and cochlear implants. Trends Amplif. 2008;12:316–331. doi: 10.1177/1084713808325881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perreau AE, Bentler RA, Tyler RS. The contribution of a frequency-compression hearing aid to contralateral cochlear implant performance. J Am Acad Audiol. 2013;24:105–120. doi: 10.3766/jaaa.24.2.4. [DOI] [PubMed] [Google Scholar]
- Phonak Structure and evaluation of an adaptive logatom test for measuring the identification of consonants. 2009. In Phonak.
- Pittman AL, Stelmachowicz PG. Hearing loss in children and adults: audiometric configuration, asymmetry, and progression. Ear Hear. 2003;24:198–205. doi: 10.1097/01.AUD.0000069226.22983.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rankovic CM. An application of the articulation index to hearing aid fitting. J Speech Hear Res. 1991;34:391–402. doi: 10.1044/jshr.3402.391. [DOI] [PubMed] [Google Scholar]
- Ricketts TA, Dittberner AB, Johnson EE. High-frequency amplification and sound quality in listeners with normal through moderate hearing loss. J Speech Lang Hear Res. 2008;51:160–172. doi: 10.1044/1092-4388(2008/012). [DOI] [PubMed] [Google Scholar]
- Scollie S, Seewald R, Cornelisse L, et al. The Desired Sensation Level multistage input/output algorithm. Trends Amplif. 2005;9:159–197. doi: 10.1177/108471380500900403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson A. Frequency-lowering devices for managing high-frequency hearing loss: a review. Trends Amplif. 2009;13:87–106. doi: 10.1177/1084713809336421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson A, Hersbach AA, McDermott HJ. Frequency-compression outcomes in listeners with steeply sloping audiograms. Int J Audiol. 2006;45:619–629. doi: 10.1080/14992020600825508. [DOI] [PubMed] [Google Scholar]
- Simpson A, McDermott HJ, Dowell RC. Benefits of audibility for listeners with severe high-frequency hearing loss. Hear Res. 2005;210:42–52. doi: 10.1016/j.heares.2005.07.001. [DOI] [PubMed] [Google Scholar]
- Skinner MW. Speech intelligibility in noise-induced hearing loss: effects of high-frequency compensation. J Acoust Soc Am. 1980;67:306–317. doi: 10.1121/1.384463. [DOI] [PubMed] [Google Scholar]
- Stelmachowicz PG, Lewis DE, Choi S, et al. Effect of stimulus bandwidth on auditory skills in normal-hearing and hearing-impaired children. Ear Hear. 2007;28:483–494. doi: 10.1097/AUD.0b013e31806dc265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stelmachowicz PG, Pittman AL, Hoover BM, et al. Effect of stimulus bandwidth on the perception of /s/ in normal- and hearing-impaired children and adults. J Acoust Soc Am. 2001;110:2183–2190. doi: 10.1121/1.1400757. [DOI] [PubMed] [Google Scholar]
- Stelmachowicz PG, Pittman AL, Hoover BM, et al. The importance of high-frequency audibility in the speech and language development of children with hearing loss. Arch Otolaryngol Head Neck Surg. 2004;130:556–562. doi: 10.1001/archotol.130.5.556. [DOI] [PubMed] [Google Scholar]
- Studebaker GA. A "rationalized" arcsine transform. J Speech, Lang, Hear Res. 1985;28:455. doi: 10.1044/jshr.2803.455. [DOI] [PubMed] [Google Scholar]
- Turner CW, Cummings KJ. Speech audibility for listeners with high-frequency hearing loss. Am J Audiol. 1999;8:47–56. doi: 10.1044/1059-0889(1999/002). [DOI] [PubMed] [Google Scholar]
- Turner CW, Henry BA. Benefits of amplification for speech recognition in background noise. J Acoust Soc Am. 2002;112:1675–1680. doi: 10.1121/1.1506158. [DOI] [PubMed] [Google Scholar]
- Tyler RS, Fryauf-Bertschy H, Kelsay D. Audiovisual feature test for young children. University of Iowa; Iowa City, Iowa: 1991. [Google Scholar]
- Van Tasell DJ, Yanz JL. Speech recognition threshold in noise: effects of hearing loss, frequency response, and speech materials. J Speech Hear Res. 1987;30:377–386. [PubMed] [Google Scholar]
- Vickers DA, Moore BC, Baer T. Effects of low-pass filtering on the intelligibility of speech in quiet for people with and without dead regions at high frequencies. J Acoust Soc Am. 2001;110:1164–1175. doi: 10.1121/1.1381534. [DOI] [PubMed] [Google Scholar]
- Wolfe J, John A, Schafer E, et al. Evaluation of nonlinear frequency compression for school-age children with moderate to moderately severe hearing loss. J Am Acad Audiol. 2010;21:618–628. doi: 10.3766/jaaa.21.10.2. [DOI] [PubMed] [Google Scholar]
- Wolfe J, John A, Schafer E, et al. Long-term effects of non-linear frequency compression for children with moderate hearing loss. Int J Audiol. 2011;50:396–404. doi: 10.3109/14992027.2010.551788. [DOI] [PubMed] [Google Scholar]