

Abstract
A 42-year-old woman was referred to our hospital with a chief complaint of asymptomatic gross hematuria. Computed tomography revealed a 4-cm tumour in the left kidney and radical nephrectomy was performed. Microscopically, the tumour was completely necrotic and consisted of nests of cells with abundant cytoplasm and large nuclei. Immunohistochemical analysis indicated complete infarction of the chromophobe renal cell carcinoma. Two years after surgery, the patient remained recurrence-free.
Introduction
Spontaneous regression of cancer was first defined by Everson and Cole in 1959 as the partial or complete disappearance of a malignant tumour without any treatment.1 Spontaneous regression of renal cell carcinoma (RCC) was first reported by Bumpus2 in 1928 and has occasionally been reported since then. Almost all reported cases concern the regression of metastases, and regression of the primary tumour is extremely rare. We report a case of spontaneous necrosis of a primary chromophobe RCC.
Case report
A 42-year-old woman was referred to our hospital with a chief complaint of asymptomatic gross hematuria. Her medical history was unremarkable, and she was not under any oral medication. Physical examination did not reveal any abnormal findings. Serum laboratory data indicated slight anemia (hemoglobin level 9.2 g/dL). Computed tomography (CT) revealed a hypovascular mass in the left kidney, measuring 4 cm in diameter (Fig. 1).
Fig. 1.
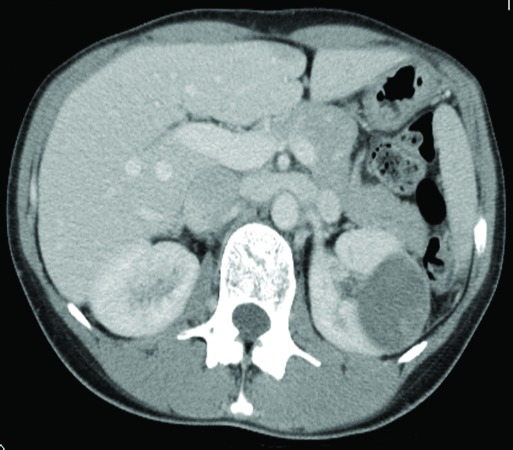
Computed tomography scan showing a hypovascular mass in the left kidney, measuring 4 cm in diameter.
RCC (cT1aN0M0) was diagnosed, and radical nephrectomy was performed. The excised tumour was an encapsulated dark-reddish mass (Fig. 2).
Fig. 2.

The excised tumour as an encapsulated dark-reddish mass.
Microscopically, the tumour was completely necrotic. It consisted of nests of cells with abundant cytoplasm and large nuclei. For the most part, the tumour structure was intact (Fig. 3, part A). Immunohistochemically, the tumour cells stained positive for cytokeratin (AE1/AE3), cytokeratin 7, and c-kit (weak staining) and negative for vimentin and CD10 (Fig. 3, part B).
Fig. 3.
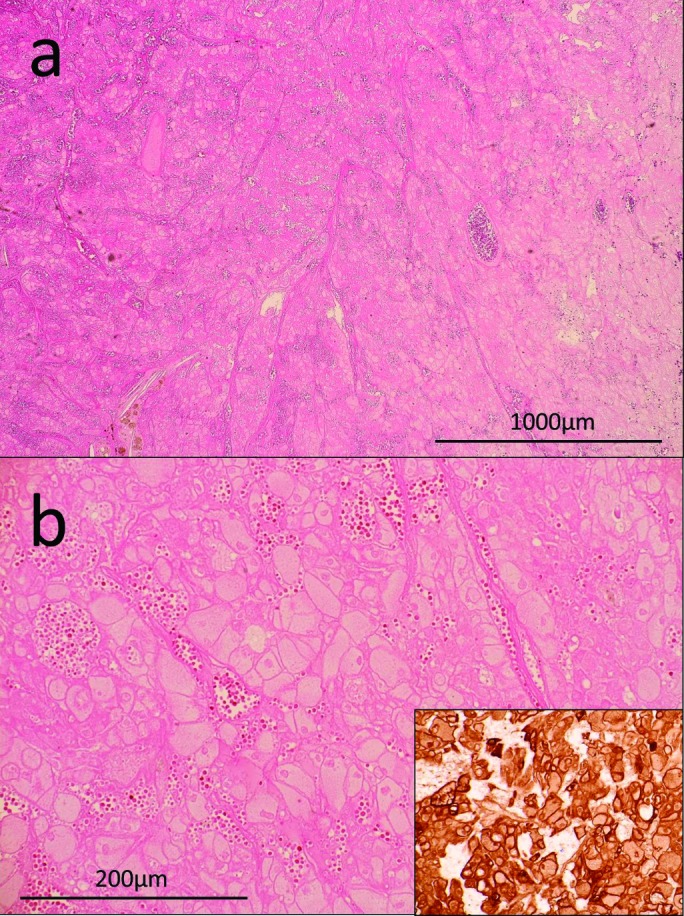
A: Hematoxilin-eosin (H&E) staining of the tumour tissue (×20). B: H&E staining (×100) and cytokeratin 7 staining (lower right) of the tumour tissue. The tumour was completely necrotic. Tumour cells with abundant cytoplasm and large nuclei formed nests. Tumour structure was intact.
On the basis of these findings, the tumour was diagnosed as a completely infarcted chromophobe RCC. Two years after surgery, the patient was recurrence-free.
Discussion
Spontaneous regression of metastases of RCC is occasionally reported. Most cases of spontaneous regression are associated with kidney resection.3,4 Even if rare, this procedure is supposed to induce the spontaneous regression of metastases due to immune mechanism and elimination of substances secreted by neoplasm.
However, spontaneous regression of primary RCC is extremely rare, and only 4 cases have been reported to date.5–8 However, in these studies, spontaneous regression was diagnosed on the basis of CT and magnetic resonance imaging findings, and regression was not confirmed histologically. In the present case, histologic examination showed that the tumour cells in the resected specimen were almost necrotic, although the tumour structure was intact. Furthermore, immunohistochemical analysis confirmed a precise diagnosis of spontaneously necrotic chromophobe RCC. To the best of our knowledge, this is the first case of spontaneous regression of primary RCC diagnosed on the basis of histological examination of the resected tumour.
The mechanism of spontaneous regression is unclear. Researchers have proposed the involvement of humoral, immunological, vascular, and other factors,7,8 but these hypotheses remain undemonstrated. Spontaneous regression of other types of neoplasms (e.g., hepatocellular carcinoma) has been reported.9,10 There are 2 possible mechanisms to explain this phenomenon: tumour hypoxia and systemic inflammatory activation.10
Adequate blood supply is essential for tumour growth. Necrosis of the tumour tissue and a compromised blood supply are likely factors contributing to spontaneous regression.11 Tumour hypoxia is also a likely explanation, given that this mechanism is exploited in treatment modalities, such as transarterial embolization and antiangiogenic therapy (i.e., vascular endothelial growth factor inhibitors). However, if hypoxia progresses gradually, tumour cells are likely to produce angiogenic factors in response to environmental cues; therefore, tumour necrosis is most likely induced by acute hypoxia.12
Several reports have documented elevated cytokine levels in cases of spontaneous tumour regression, suggesting the involvement of a systemic inflammatory response.10 Induction of cytokines, such as interferon, interleukin (IL)-2, IL-6, and IL-12, can play an important role in cancer cell regression, supported by the fact that immunotherapy is a standard treatment for RCC.
Conclusion
In the current case, no viable cells were observed and the histological findings were similar to those seen after trans-catheter arterial embolization. Accordingly, we speculate that the acute hypoxia theory could explain tumour necrosis in this case. However, given the limited number of reported cases, the exact regression process remains uncertain, and future studies may help elucidate the underlying mechanism.
Footnotes
Competing interests: Authors declare no competing financial or personal interests.
This paper has been peer-reviewed.
References
- 1.Everson T, Cole W. Spontaneous regression of cancer. Ann Surg. 1956;144:366–80. doi: 10.1097/00000658-195609000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bumpus HC. The apparent disappearance of pulmonary metastasis in a case of hypernephroma following nephrectomy. J Urol. 1928;20:185–91. [Google Scholar]
- 3.de Reijke TM1, Bellmunt J, van Poppel H, et al. EORTC-GU group expert opinion on metastatic renal cell cancer. Eur J Cancer. 2009;45:765–73. doi: 10.1016/j.ejca.2008.12.010. [DOI] [PubMed] [Google Scholar]
- 4.Janiszewska AD, Poletajew S, Wasiutyński A. Spontaneous regression of renal cell carcinoma. Contemp Oncol (Pozn) 2013;17:123–7. doi: 10.5114/wo.2013.34613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Choi SK, Chang SK, Lee JM, et al. Spontaneous regression of primary renal cell carcinoma-a case report. Yonsei Med J. 1986;27:314–7. doi: 10.3349/ymj.1986.27.4.314. [DOI] [PubMed] [Google Scholar]
- 6.Edwards MJ, Anderson JA, Angel JR, et al. Spontaneous regression of primary and metastatic renal cell carcinoma. J Urol. 1996;155:1385. doi: 10.1016/S0022-5347(01)66275-X. [DOI] [PubMed] [Google Scholar]
- 7.Kobayashi K, Sato T, Sunaoshi K, et al. Spontaneous regression of primary renal cell carcinoma with inferior vena caval tumor thrombus. J Urol. 2002;167:242–3. doi: 10.1016/S0022-5347(05)65424-9. [DOI] [PubMed] [Google Scholar]
- 8.Jawanda GG, Drachenberg D. Spontaneous regression of biopsy proven primary renal cell carcinoma: A case study. Can Urol Assoc J. 2012;6:203–5. doi: 10.5489/cuaj.11035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Storey RE, Huerta AL, Khan A, et al. Spontaneous complete regression of hepatocellular carcinoma. Med Oncol. 2011;28:948–50. doi: 10.1007/s12032-010-9562-8. [DOI] [PubMed] [Google Scholar]
- 10.Huz JI, Melis M, Sarpel U. Spontaneous regression of hepatocellular carcinoma is most often associated with tumour hypoxia or a systemic inflammatory response. HPB (Oxford) 2012;14:500–5. doi: 10.1111/j.1477-2574.2012.00478.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Papac RJ. Spontaneous regression of cancer: Possible mechanisms. In Vivo. 1998;12:571–8. [PubMed] [Google Scholar]
- 12.Hemmerlein B, Kugler A, Ozisik R, et al. Vascular endothelial growth factor expression, angiogenesis, and necrosis in renal cell carcinomas. Virchows Arch. 2001;439:645–52. doi: 10.1007/s004280100464. [DOI] [PubMed] [Google Scholar]