

Abstract
In the literature on alcohol use and aging, drinking has often been conceptualized as a means of coping with negative feelings, such as stress, yet much of the literature on older adults and drinking has utilized cross-sectional or other data ill-suited for exploring dynamic processes. Experience sampling methods have the ability to measure and analyze dynamic processes in real time, such as relations between alcohol use and mood states. Nonetheless, these approaches are intensive and may burden respondents. Therefore, this study evaluated the feasibility, acceptability, and validity of a modified daily diary to measure alcohol use and explored alternate methods of collecting diary data. Findings suggest that a modified diary was acceptable and not burdensome. Respondents were reluctant to consider technology (e.g., cellphone)-based means of data collection. Measures of alcohol use showed little within-person variation suggesting that for those who drink at all, drinking is a daily habit.
Keywords: alcohol, drinking, experience sampling, older adult, continuing care retirement community
Alcohol use among older adults is often conceptualized as a means of coping with painful life experiences such as losses related to aging and other forms of psychological distress (Blazer & Wu, 2009; Finney & Moos, 1984; Folkman, Bernstein, & Lazarus, 1987; Hunter & Gillen, 2006). The underlying thinking is that alcohol use occurs as a reaction to painful experiences and emotions. Two theories embody this approach to alcohol use: the self-medication hypothesis (Khantzian, 1985) and tension reduction theory (Cappell & Herman, 1972); they have provided a foundation for research on alcohol use among older adults including epidemiology (Platt, Solan, & Costanzo, 2010), treatment (Moos, 2007), and measurement (Blow et al., 1992). Research on the role of negative affective states in drinking is long-standing but has been methodologically limited by cross-sectional or lengthy and burdensome longitudinal study designs.
Experience sampling (ES) methods are intensive longitudinal designs that involve multiple data collection points over hours or days. Methods for ES vary from paper-based diaries completed by research participants to electronic means for capturing data on a moment-to-moment basis (i.e., ecological momentary assessment). ES methods enable researchers to understand dynamic processes that unfold over shorter time frames than traditional longer-term longitudinal surveys. We sought to explore and test the feasibility of ES using a modified daily diary approach.
Background: Alcohol Use and Older Adults
Unhealthy alcohol use is a significant public health concern (Bartels, Blow, Brockmann, & Van Citters, 2005) for older adults. Heavy drinking among older adults is associated with increased risk of mortality (Holahan et al., 2010), stroke (Bazzano et al., 2007), injury (Sorock, Chen, Gonzalgo, & Baker, 2006), and memory impairment (Hendrie, Gao, Hall, Hui, & Unverzagt, 1996; Perreira & Sloan, 2001). Even moderate use of alcohol and certain medications may put older adults at risk (Moore, Whiteman, & Ward, 2007). Moreover, older adults may have medical conditions where the use of alcohol is contraindicated (Moore, Beck, Babor, Hays, & Reuben, 2002) Still, it is unclear the extent to which alcohol and medication co-use leads to clinically significant effects among low-risk drinkers who take medications as prescribed (Mallet, Spinewine, & Huang, 2007).
In a recent national survey, of those age 65 and older, 13% of men and 8% of women reported at-risk alcohol consumption and 14% of men and 3% of women reported binge drinking (Blazer & Wu, 2009). Rates of substance use disorders (Han, Gfroerer, Colliver, & Penne, 2009), past-year treatment (Sacco, Kuerbis, Goge, & Bucholz, 2013), and need for treatment (Gfroerer, Penne, Pemberton, & Folsom, 2003) among older adults are projected to increase in coming years as well. A plurality of approaches to treating older adults with alcohol-related problems has shown positive outcomes (Kuerbis & Sacco, 2013; Outlaw et al., 2012; Schonfeld et al., 2010).
There are, however, many older adults who consume alcohol regularly at a moderate level without experiencing negative effects (Sacco, Bucholz, & Spitznagel, 2009). In fact, moderate alcohol consumption may be associated with better health (Balsa, Homer, Fleming, & French, 2008; Mukamal, Robbins, Cauley, Kern, & Siscovick, 2007) and lower mortality (Klatsky & Udaltsova, 2007; Lee et al., 2009).
To determine drinking patterns, most studies in this area have used retrospective measurement that has numerous limitations. Those who drink infrequently may overreport their consumption, and heavy drinkers tend to underreport their consumption (Leigh, Gillmore, & Morrison, 1998; O’Hare, 1991; Townshend & Duka, 2002). When asked to recall affective states and thoughts, participant responses may involve recall bias influenced by their current emotional state (Ready, Weinberger, & Jones, 2007). Among older adults, the presence of cognitive impairments may also contribute to problems with recall that may impact the reliability of data.
ES methods offer an alternative approach to measuring drinking patterns; often described as intensive longitudinal design, in ES studies, a single construct (e.g., mood) is measured repeatedly either at regular time intervals or random times. ES methods move beyond simply testing the association between major depression and drinking because they capture within-person variation (e.g., does being lonely on a given day lead to consumption on that day) and allow investigators to assess between-person variation, in essence adjusting for within-person variation (e.g., does loneliness account for the variation in drinking between people).
Experience Sampling Methods
ES has been used extensively in studies of alcohol use among younger age groups (Leigh, 2000) and has been shown to be feasible among older adults (Cain, Depp, & Jeste, 2009). Nonetheless, ES approaches can be burdensome to research participants depending on the method. For example, older adults may find it difficult to respond to daily interactive voice response systems over the telephone. Paper diaries are inexpensive but present compliance issues with the requirement of completing multiple forms each day. This burden may lead participants to complete their responses at one time—either at the beginning or the end of the study (Litcher-Kelly, Kellerman, Hanauer, & Stone, 2007). Electronic means of collecting daily diary data, such as use of personal data assistants (PDAs), may outperform paper-based approaches in health-related studies for the general population (Dale & Hagen, 2007) but have challenges including the cost of electronic tools and data management (e.g., data loss due to hardware or software problems; Dale & Hagen, 2007).
Research suggests that respondents prefer to use electronic means over paper and pencil diaries, but the use of electronic diaries with older adult populations is an emerging approach and is relatively uncommon in studies with individuals over 75 (Cain et al., 2009). Although ES methods are a potentially powerful approach to research on drinking among older adults, the acceptability and feasibility of these approaches are relatively unexamined. In this study, we sought to explore one ES approach with three specific aims: (1) to evaluate the feasibility and acceptability of using a modified daily diary to measure alcohol use and daily variation in stress and mood, (2) to assess the concurrent validity of a modified diary method with a retrospective risk measure and measures of at-risk drinking, and (3) to explore the perceived acceptability of electronic means of data collection in a sample of older adults.
Method
Study Site
This study was conducted at a Continuing Care Retirement Community (CCRC) located in Maryland. This site was selected because the social context of drinking among the residents of the CCRC was fairly consistent as was the level of resident functioning. Similarly, we were aware that a plurality of residents identified as current drinkers. It was also appropriate because we were interested in the relationship between alcohol use, stress, and daily living in the context of a CCRC. The study was approved by a university Institutional Review Board.
Sample
We collaborated with the CCRC to recruit residents who consumed at least one drink in the past 2 weeks. Study personnel contacted residents, invited them to participate, obtained consent, and enrolled them into the study. Inclusion criteria included residing in independent living, ability to speak and hear over the phone, English proficiency, and lack of significant dementia. Dementia was assessed using the Mini-Cog screen (Borson, Scanlan, Chen, & Ganguli, 2003).
A total of 65 individuals were contacted by a licensed social worker with extensive experience as an interviewer. Under a Health Insurance Portability and Accountability Act (HIPAA) waiver, names of participants were identified by the primary care provider (PCP) as likely to be eligible. Among these individuals, 20 were not eligible to participate as they were nondrinkers (n = 14; 22%), could not hear or speak over the phone (n = 2; 3%), were not currently residing within independent living (n = 3; 5%), or were residing with a study participant (n = 1; 2%). Of the 45 eligible participants, 25 (56%) consented to participate, 11 individuals (25%) were not interested in participating, and 9 (24%) were unreachable by phone.
The demographic profile of the sample reflected that of CCRC residents (see Table 1). The average age of residents was 86 (SD = 6.0), and all the respondents had a college education or more. More than half of individuals were currently married and almost a third were widowed. These demographic characteristics approximate those of CCRC residents nationally but differ in certain respects. The average age of CCRC residents nationally is 84 years, 21% of residents are married and 23% of residents are male (Coe & Boyle, 2013). The difference may be a result of distinct profiles for current drinkers versus the overall population of CCRCs. For example, older men are more likely than women to be past-year consumers of alcohol (Moore et al., 2009). Of the 25 people in the study, 12% displayed significant depressive symptoms and a very small percentage (4%) were hazardous drinkers based on the Alcohol Use Disorders Identification Test (AUDIT) screening instrument.
Table 1.
Sample Characteristics (n = 25).
| Categorical measures | % |
|---|---|
| Demographic | |
| Male gender | 56% |
| Marital status | |
| Married | 56% |
| Widowed | 28% |
| Never married | 16% |
| Education level | |
| College | 40% |
| Graduate or Prof. school | 60% |
| Alcohol-related | |
| AUDIT score >8 (hazardous drinking) | 4% |
| Health and mental health | |
| GDS (>4) | 12% |
| Continuous measures | M (SD) |
|---|---|
| Demographic | |
| Mean age | 85.9 (6.0) |
| Alcohol-related | |
| Mean daily alcohol cons. | .99 (.87) |
| Mean weekly alcohol cons. | 6.9 (6.1) |
| AUDIT score | 3.4 (1.5) |
| Health and mental health | |
| GDS (M) | 2.0 (1.9) |
| SF-12 (Mental component) | 53.9 (6.6) |
| SF-12 (Physical component) | 45.0 (11.2) |
Note. AUDIT = Alcohol Use Disorders Identification Test; GDS = Geriatric Depression Scale.
Procedure
The study was conducted in three parts (see Figure 1). An initial in-person survey was completed that included sociodemographic information, the SF-12 Health Survey (Ware, Kosinski, & Keller, 1996), AUDIT (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001), and the Geriatric Depression Scale (GDS; Brink et al., 1982). Next, for 7 days, participants were surveyed via telephone about their alcohol consumption from the previous day including type of alcohol consumed, number of drinks, whether they were alone, when they drank, and the setting for alcohol consumption (i.e., at home, somewhere in the facility, or in the community).
Figure 1.
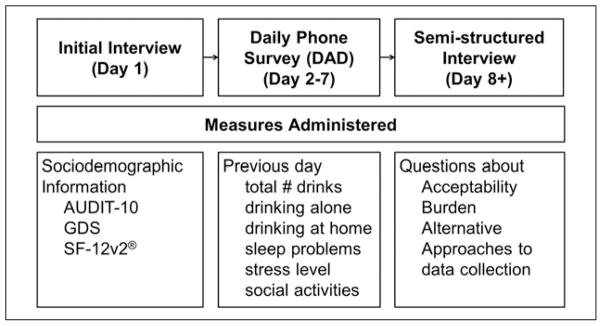
Data collection procedure.
Members of the research team, including MSW and PhD student trainees, conducted the phone interviews. In most cases, the same caller would contact the respondent each day. During the initial interview, a convenient time for the phone call was arranged with the participant, typically in the midmorning. If the interviewer was unable to contact the resident on the first call attempt, a phone message was left with a follow-up time. A total of three attempts were made to reach the participant on a given day. If the interviewer was unable to contact after three attempts, no further attempts were made. During the daily phone calls, five-point Likert-scaled items were administered that focused on mood, stress level, and sleep problems during the previous day. After seven days of daily diary reports, participants took part in an open-ended qualitative interview focused on the acceptability and burden of the protocol as well as potential alternative approaches for data collection (e.g., interactive voice response and mobile devices).
Analysis
Univariate analysis of daily mood items and alcohol consumption were calculated to assess variation across the 7 days. Interclass correlation coefficients (ICC) were computed to assess the relationship of within- to between-person variation on constructs of interest. To assess the concurrent validity of retrospective data with daily diary reports, we conducted bivariate analysis of time-varying measures (e.g., Likert-scaled mood items) with retrospective measures (e.g., GDS) and alcohol consumption with AUDIT scores. To achieve this, we used multilevel models with a single predictor (e.g., each mood item predicting GDS score) to explore relations between time-varying daily diary items and invariant measures of related constructs. Quantitative data analysis was conducted using SAS 9.2 (SAS Institute, 2008) and STATA (Statacorp, 2011). Qualitative data were recorded, transcribed, and analyzed separately by two researchers. Major themes were identified independently, compared, and reconciled by the study team.
Results
Average alcohol use was approximately one drink per day (see Table 1), but variability was present among the participants in their levels of average consumption over the 7 days (see Figure 2). Across the 7-day ES period, people’s stress level and mood varied but alcohol use was consistent (see Figure 3). ICCs suggest that within-person variability was higher for questions related to affect and mood than for those on drinking (see Table 2). Between 16% (stress) and 47% (loneliness) of the variance was explained by between-person variance in the mood and sleep items. Most of the variation in alcohol consumption and drinking alone was explained by differences between people; older adults drank in consistent ways during the data collection period, with some older adults drinking more than others but little binge drinking.
Figure 2.

Distribution of mean drinking among older adult CCRC residents (n = 25).
Note. CCRC = Continuing Care Retirement Community.
Figure 3.

Means and standard errors of Likert-scaled items across days.
a1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree.
Table 2.
Item ICC Values and Association With Retrospective Measures.
| ICC | Association with GDS Score | Association with AUDIT Score | |
|---|---|---|---|
| “Yesterday was very stressful for me” | .162 | −.060 | .046 |
| “Yesterday I felt lonely” | .473 | .097* | −.096 |
| “Yesterday I felt sad” | .263 | .048 | .223 |
| “Yesterday I had trouble sleeping” | .206 | .033 | −.132 |
| Day distress | .395 | .116 | −.359 |
| Total reported drinks | .757 | .094 | .476** |
| Drinking alone | .918 | .183 | .499** |
Note. ICC = intraclass correlation coefficient; GDS = Geriatric Depression Scale; AUDIT = Alcohol Use Disorders Identification Test.
p = .06.
p < .001.
Concurrent Validity
AUDIT scores were significantly associated with daily reports of total drinks consumed during the day and drinking when alone (see Table 2). Conversely, measures of daily distress were not significantly associated with overall GDS score, but relationships were in the expected direction (e.g., daily loneliness was associated with higher GDS) and significant at p < .10.
Acceptability and Burden
Participants reported that the modified daily diary method was convenient, especially for those with physical limitations. Participants preferred to be called the next day rather than at the end of their day and most reported no associated burden. Electronic daily diary collection, including e-mail or use of a touchscreen device was seen as problematic by participants. Many indicated a lack of familiarity with the technology:
That’s sort of a routine that would be good for younger people, who are computer-oriented. I’m not. I’m oriented to reading the newspapers, reading books, getting news, television …
Participants indicated that daily phone calls are advantageous as they afford an opportunity to develop a rapport. This may allow participants to be more forthcoming:
Well if you use an automated…, where one of these canned voices that we’re now learning to be used to ask questions and gives you alternatives to pick, “press 1,” “press 2” and so forth, that is going to put a damper on any response because then you feel as though you aren’t talking to a person you’re just filling in a blank somewhere.
Discussion
Daily phone call diaries are a feasible method of assessment of alcohol use and emotional states among retired older adults. Participants did not find questions stigmatizing, and they did not report that daily phone calls were burdensome. In addition to reporting acceptability, missed data collection was very rare (3%). The potential for systematic bias with this approach should be noted as daily phone calls about drinking may influence whether individuals endorse drinking due to social desirability.
Based on data from qualitative interviews with respondents, the use of technology may be problematic in collecting daily diary data. This is in contrast to some other studies done with the “young–old,” who may be more familiar with computers and handheld computing devices. In those studies, few concerns with the use of electronic means for ES were raised (Atienza, Oliveira, Fogg, & King, 2006), and authors recommended the use of electronic means as feasible (Cain et al., 2009). Participants in this study were older than those in prior studies; disparate findings may be the result of cohort differences. Someone who is aged 50 years may have greater comfort with technology than someone aged 75 because of exposure to computing in the workplace. Indeed, the study sample is not representative of the general population of older adults, a limitation of this study. Consequently, this modified diary approach may not be transferrable to other populations of older adults.
From a substantive perspective, patterns of alcohol use among CCRC residents are marked by consistency, although variability in mood and affective states was present. The daily phone call ES method performed well in this study and is a promising method for future research with the older–old population.
Acknowledgments
Funding
Support for this research was provided from an internal grant from the University of Maryland, School of Social Work.
Biographies
Paul Sacco is an Assistant Professor at the University of Maryland School of Social Work in Baltimore, Maryland. His research focuses on addictive behaviors with a focus on life course development and aging. Specifically, he has conducted research on the epidemiology of alcohol use and pathological gambling among older adults.
Cristan A. Smith, MA, is a doctoral candidate in the intercampus program in Gerontology at the University of Maryland Baltimore and University of Maryland, Baltimore County. Her research interests focus on long-term effects of substance abuse, including later life physical, psychological and social functioning.
Donna Harrington, PhD, is professor and associate dean for doctoral and post-doctoral education in the University of Maryland, Baltimore School of Social Work. Dr. Harrington teaches doctoral courses in advanced data analysis and the integration of theory and research methods. Her research focuses on measurement, ethics, and older adults.
Deborah V. Svoboda is an assistant professor in the School of Social Work and an affiliated faculty member of Women’s and Gender Studies at Eastern Washington University. Her teaching and research interests are women’s organizations, community development, and justice seeking policy construction in response to gender based violence and economic disparities.
Barbara Resnick, PhD, CRNP is a Professor in the Department of Organizational Systems and Adult Health at the University of Maryland School of Nursing, co-directs the Adult/Gerontological nurse Practitioner Program, Co-Directs the Biology and Behavior Across the Lifespan Research Center of Excellence, holds the Sonya Ziporkin Gershowitz Chair in Gerontology at the School of Nursing, and does clinical work at Roland Park Place, a Lifecare community.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Atienza AA, Oliveira B, Fogg BJ, King AC. Using electronic diaries to examine physical activity and other health behaviors of adults age 50+ Journal of Aging and Physical Activity. 2006;14:192–202. doi: 10.1123/japa.14.2.192. [DOI] [PubMed] [Google Scholar]
- Babor TF, Higgins-Biddle J, Saunders JB, Monteiro MG. The Alcohol Use Disorders Identification Test: Guidelines for use in primary care. 2. Geneva, Switzerland: World Health Organization; 2001. [Google Scholar]
- Balsa AI, Homer JF, Fleming MF, French MT. Alcohol consumption and health among elders. Gerontologist. 2008;48:622–636. doi: 10.1093/geront/48.5.622. [DOI] [PubMed] [Google Scholar]
- Bartels SJ, Blow FC, Brockmann LM, Van Citters AD. Substance abuse and mental health among older Americans: The state of the knowledge and future directions. Rockville, MD: WESTAT; 2005. [Google Scholar]
- Bazzano LA, Gu D, Reynolds K, Wu X, Chen CS, Duan X, He J. Alcohol consumption and risk for stroke among Chinese men. Annals of Neurology. 2007;62:569–578. doi: 10.1002/ana.21194. [DOI] [PubMed] [Google Scholar]
- Blazer DG, Wu LT. The epidemiology of at-risk and binge drinking among middle-aged and elderly community adults: National Survey on Drug Use and Health. American Journal of Psychiatry. 2009;166:1162–1169. doi: 10.1176/appi.ajp.2009.09010016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blow FC, Brower KJ, Schulenberg JE, Demo-Dananberg LM, Young KJ, Beresford TP. The Michigan Alcohol Screening Test: Geriatric Version (MAST-G): A new elderly specific screening instrument. Alcoholism: Clinical and Experimental Research. 1992;16:172. [Google Scholar]
- Borson S, Scanlan JM, Chen P, Ganguli M. The Mini-Cog as a screen for dementia: Validation in a population-based sample. Journal of the American Geriatrics Society. 2003;51:1451–1454. doi: 10.1046/j.1532-5415.2003.51465.x. [DOI] [PubMed] [Google Scholar]
- Brink TL, Yesavage JA, Lum O, Heersema PH, Adey M, Rose TL. Screening Tests for Geriatric Depression. Clinical Gerontologist. 1982;1(1):37–43. [Google Scholar]
- Cain AE, Depp CA, Jeste DV. Ecological momentary assessment in aging research: A critical review. Journal of Psychiatric Research. 2009;43:987–996. doi: 10.1016/j.jpsychires.2009.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cappell H, Herman CP. Alcohol and tension reduction: A review. Quarterly Journal of Studies on Alcohol. 1972;33:33–64. [PubMed] [Google Scholar]
- Coe NB, Boyle MA. The asset and income profiles of residents in seniors housing and care communities: What can be learned from existing data sets. Research on Aging. 2013;35:50–77. [Google Scholar]
- Dale O, Hagen KB. Despite technical problems personal digital assistants outperform pen and paper when collecting patient diary data. Journal of Clinical Epidemiology. 2007;60:8–17. doi: 10.1016/j.jclinepi.2006.04.005. [DOI] [PubMed] [Google Scholar]
- Finney JW, Moos RH. Life stressors and problem drinking among older adults. Recent Developments in Alcoholism. 1984;2:267–288. doi: 10.1007/978-1-4684-4661-6_15. [DOI] [PubMed] [Google Scholar]
- Folkman S, Bernstein L, Lazarus RS. Stress processes and the misuse of drugs in older adults. Psychology and Aging. 1987;2:366–374. doi: 10.1037//0882-7974.2.4.366. [DOI] [PubMed] [Google Scholar]
- Gfroerer J, Penne M, Pemberton M, Folsom R. Substance abuse treatment need among older adults in 2020: The impact of the baby-boom cohort. Drug and Alcohol Dependence. 2003;69:127–135. doi: 10.1016/s0376-8716(02)00307-1. [DOI] [PubMed] [Google Scholar]
- Han B, Gfroerer J, Colliver JD, Penne MA. Substance use disorder among older adults in the United States in 2020. Addiction. 2009;104:88–96. doi: 10.1111/j.1360-0443.2008.02411.x. [DOI] [PubMed] [Google Scholar]
- Hendrie HC, Gao S, Hall KS, Hui SL, Unverzagt FW. The relationship between alcohol consumption, cognitive performance, and daily functioning in an urban sample of older black Americans. Journal of the American Geriatrics Society. 1996;44:1158–1165. doi: 10.1111/j.1532-5415.1996.tb01364.x. [DOI] [PubMed] [Google Scholar]
- Holahan CJ, Schutte KK, Brennan PL, Holahan CK, Moos BS, Moos RH. Late-life alcohol consumption and 20-year mortality. Alcoholism: Clinical and Experimental Research. 2010;34:1961–1971. doi: 10.1111/j.1530-0277.2010.01286.x. [DOI] [PubMed] [Google Scholar]
- Hunter IR, Gillen MC. Alcohol as a response to stress in older adults: A counseling perspective. Adultspan. 2006;5:114–126. [Google Scholar]
- Khantzian EJ. The self-medication hypothesis of addictive disorders: Focus on heroin and cocaine dependence. American Journal of Psychiatry. 1985;142:1259–1264. doi: 10.1176/ajp.142.11.1259. [DOI] [PubMed] [Google Scholar]
- Klatsky AL, Udaltsova N. Alcohol drinking and total mortality risk. Annals of Epidemiology. 2007;17(5 Suppl 1):S63–S67. [Google Scholar]
- Kuerbis A, Sacco P. A review of existing treatments for substance abuse among the elderly and recommendations for future directions. Substance Abuse: Research and Treatment. 2013;7:13. doi: 10.4137/SART.S7865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee SJ, Sudore RL, Williams BA, Lindquist K, Chen HL, Covinsky KE. Functional limitations, socioeconomic status, and all-cause mortality in moderate alcohol drinkers. Journal of the American Geriatrics Society. 2009;57:955–962. doi: 10.1111/j.1532-5415.2009.02184.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leigh BC. Using daily reports to measure drinking and drinking patterns. Journal of Substance Abuse. 2000;12:51–65. doi: 10.1016/s0899-3289(00)00040-7. [DOI] [PubMed] [Google Scholar]
- Leigh BC, Gillmore MR, Morrison DM. Comparison of diary and retrospective measures for recording alcohol consumption and sexual activity. Journal of Clinical Epidemiology. 1998;51:119–127. doi: 10.1016/s0895-4356(97)00262-x. [DOI] [PubMed] [Google Scholar]
- Litcher-Kelly L, Kellerman Q, Hanauer SB, Stone AA. Feasibility and utility of an electronic diary to assess self-report symptoms in patients with inflammatory bowel disease. Annals of Behavioral Medicine. 2007;33:207–212. doi: 10.1007/BF02879902. [DOI] [PubMed] [Google Scholar]
- Mallet L, Spinewine A, Huang A. The challenge of managing drug interactions in elderly people. Lancet. 2007;370:185–191. doi: 10.1016/S0140-6736(07)61092-7. [DOI] [PubMed] [Google Scholar]
- Moore AA, Beck JC, Babor TF, Hays RD, Reuben DB. Beyond alcoholism: Identifying older, at-risk drinkers in primary care. Journal of Studies on Alcohol. 2002;63:316–325. doi: 10.15288/jsa.2002.63.316. [DOI] [PubMed] [Google Scholar]
- Moore AA, Karno MP, Grella CE, Lin JC, Warda U, Liao DH, Hu P. Alcohol, tobacco, and nonmedical drug use in older U.S. adults: Data from the 2001/02 National Epidemiologic Survey of Alcohol and Related Conditions. Journal of the American Geriatrics Society. 2009;57:2275–2281. doi: 10.1111/j.1532-5415.2009.02554.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore AA, Whiteman EJ, Ward KT. Risks of combined alcohol/medication use in older adults. American Journal of Geriatric Pharmacotherapy. 2007;5:64–74. doi: 10.1016/j.amjopharm.2007.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moos RH. Theory-based processes that promote the remission of substance use disorders. Clinical Psychology Review. 2007;27:537–551. doi: 10.1016/j.cpr.2006.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mukamal KJ, Robbins JA, Cauley JA, Kern LM, Siscovick DS. Alcohol consumption, bone density, and hip fracture among older adults: The cardiovascular health study. Osteoporosis International. 2007;18:593–602. doi: 10.1007/s00198-006-0287-7. [DOI] [PubMed] [Google Scholar]
- O’Hare T. Measuring alcohol consumption: A comparison of the retrospective diary and the quantity-frequency methods in a college drinking survey. Journal of Studies on Alcohol. 1991;52:500–502. doi: 10.15288/jsa.1991.52.500. [DOI] [PubMed] [Google Scholar]
- Outlaw FH, Marquart JM, Roy A, Luellen JK, Moran M, Willis A, Doub T. Treatment outcomes for older adults who abuse substances. Journal of Applied Gerontology. 2012;31:78–100. [Google Scholar]
- Perreira KM, Sloan FA. Life events and alcohol consumption among mature adults: A longitudinal analysis. Journal of Studies on Alcohol. 2001;62:501–508. doi: 10.15288/jsa.2001.62.501. [DOI] [PubMed] [Google Scholar]
- Platt A, Solan FA, Costanzo P. Alcohol-consumption trajectories and associated characteristics among adults older than age 50. Journal of Studies on Alcohol and Drugs. 2010;71:169–179. doi: 10.15288/jsad.2010.71.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ready RE, Weinberger MI, Jones KM. How happy have you felt lately? Two diary studies of emotion recall in older and younger adults. Cognition & Emotion. 2007;21:728–757. [Google Scholar]
- Sacco P, Bucholz KK, Spitznagel EL. Alcohol use among older adults in the National Epidemiologic Survey on Alcohol and Related Conditions: A latent class analysis. Journal of Studies on Alcohol and Drugs. 2009;70:829–838. doi: 10.15288/jsad.2009.70.829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sacco P, Kuerbis A, Goge N, Bucholz KK. Help seeking for drug and alcohol problems among adults age 50 and older: A comparison of the NLAES and NESARC surveys. Drug and Alcohol Dependence. 2013;131:157–161. doi: 10.1016/j.drugalcdep.2012.10.008. [DOI] [PubMed] [Google Scholar]
- SAS Institute. SAS 9.2 help and documentation. Cary, NC: Author; 2008. [Google Scholar]
- Schonfeld L, King-Kallimanis BL, Duchene DM, Etheridge RL, Herrera JR, Barry KL, Lynn N. Screening and brief intervention for substance misuse among older adults: The Florida BRITE project. American Journal of Public Health. 2010;100:108. doi: 10.2105/AJPH.2008.149534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sorock GS, Chen LH, Gonzalgo SR, Baker SP. Alcohol-drinking history and fatal injury in older adults. Alcohol. 2006;40:193–199. doi: 10.1016/j.alcohol.2007.01.002. [DOI] [PubMed] [Google Scholar]
- Statacorp. Stata Statistical Software: Release 12. College Station, TX: Author; 2011. [Google Scholar]
- Townshend JM, Duka T. Patterns of alcohol drinking in a population of young social drinkers: A comparison of questionnaire and diary measures. Alcohol and Alcoholism. 2002;37:187–192. doi: 10.1093/alcalc/37.2.187. [DOI] [PubMed] [Google Scholar]
- Ware JE, Kosinski M, Keller S. A 12-item short form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care. 1996;34:220–233. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]