

Abstract
Individuals with a history of foster care (FC) are at elevated risk for emotion regulation-related mental illness. The purpose of the current study was to characterize regulatory function in a group of adults with a history of FC (N = 26) relative to those without a history of FC (N = 27) and how regulatory function moderates adverse caregiving-related outcomes (daily cortisol production and trait anxiety). Self-report items (anxiety, emotion regulation strategies, inhibitory control, caregiving history) were collected along with more objective measures (computerized task and salivary cortisol). Inhibitory control was assessed via self-report and a computerized task (emotional face go/nogo). Results showed that for adults with a history of FC, higher levels of inhibitory control were associated with higher accuracy on the emotional face go/nogo task and greater reported use of the emotion regulation strategy cognitive reappraisal. Greater use of cognitive reappraisal in turn was associated with healthier stress-related outcomes (decreased trait anxiety and steeper sloped cortisol production throughout the day). Dose-response associations were observed between self-reported regulatory skills and FC experiences (i.e., number of placements and age when exited foster care). These findings suggest that adverse caregiving can have long-term influences on mental health that extend into adulthood; however, individual differences in regulatory skills moderate these outcomes and may be an important target for intervention following caregiving adversity. © 2014 The Authors. Developmental Psychobiology published by Wiley Periodicals, Inc. Dev Psychobiol 57: 1–16, 2015.
Keywords: emotion, foster care, HPA axis, regulation, stress, human
INTRODUCTION
The purpose of the current study was to characterize regulatory skills in a group of adults with a history of foster care (FC) and examine whether regulatory skills moderated stress-related outcomes. Individuals with a history of FC may have experienced significant maltreatment, neglect, exposure to prenatal alcohol/drugs, and separation from the birth home all during development (Dozier, Albus, Fisher, & Sepulveda, 2002). In the United States, children placed in foster care, which is intended to be a better alternative home, may experience warm and enriching caregiving at its best or abuse and neglect at its worst (Dozier et al., 2002). Even at its best, foster care represents caregiving instability, a potent stressor for the developing human (Fisher, Van Ryzin, & Gunnar, 2011; Lewis, Dozier, Ackerman, & Sepulveda-Kozakowski, 2007; Tottenham, 2012).
Stress-Related Outcomes
A history of FC is associated with increased risk for mental illnesses such as depression, anxiety, and post-traumatic stress disorder (Bruskas, 2008; Jackson, O'Brien, & Pecora, 2011; Lawrence, Carlson, & Egeland, 2006; Neely-Barnes & Whitted, 2011; Rusby & Tasker, 2009; Thompson & Hasid, 2012). Much research examining individuals with a history of FC has been performed during childhood and has shown that children with FC experiences exhibit heightened anxiety and associated internalizing problems (Damnjanovic, Lakic, Stevanovic, & Jovanovic, 2011; Dozier et al., 2002; Fisher, Gunnar, Dozier, Bruce, & Pears, 2006; Sawyer, Carbone, Searle, & Robinson, 2007; Wiik et al., 2011). Additionally, individuals with a history of caregiving adversity tend to be more stress reactive (McLaughlin et al., 2010) and exhibit altered activity of the stress-responsive hypothalamic pituitary adrenal (HPA) axis (e.g., flattened slope for cortisol production throughout the day and/or low cortisol morning levels) (Bernard, Butzin-Dozier, Rittenhouse, & Dozier, 2010; Bruce, Fisher, Pears, & Levine, 2009; Dozier et al., 2006; Fisher, Gunnar, Chamberlain, & Reid, 2000; Fisher et al., 2006; Fisher, Stoolmiller, Gunnar, & Burraston, 2007; Fisher et al., 2011). Although it is challenging to know whether adverse care itself causes such outcomes, randomized intervention designs have provided strong evidence for a causal association between adverse caregiving and these stress-related outcomes (Dozier et al., 2002; Fisher et al., 2000).
Regulatory Skills
Importantly, there is heterogeneity in stress-related outcomes and, despite adverse caregiving histories, some individuals exhibit resilience. Resilience is a process of exhibiting resistance to adverse effects caused by stressors (Masten, 2009; Rutter, 2012) and is a process that may explain divergent outcomes across individuals. The presence of individual differences in stress-related outcomes following caregiving adversity (Lengua, Bush, Long, Kovacs, & Trancik, 2008) begs the question of what factors contribute to the heterogeneity in outcome. Individual differences in emotionality have been largely attributed to cognitive regulation processes (Ochsner & Gross, 2008). Cognitive regulatory skills (which can include related processes such as inhibitory control, effortful control, cognitive control, and other executive functions) are often impaired following caregiving adversity in childhood (Garland et al., 2001; Lewis et al., 2007; Linares et al., 2010; Loman et al., 2013; Merz, McCall, Wright, & Luna, 2013; Pollak et al., 2010; Rogosch, Dackis, & Cicchetti, 2011; Simmel, Brooks, Barth, & Hinshaw, 2001; Steele & Buchi, 2008; Tottenham et al., 2010), in adolescence, and in adulthood (Bos, Fox, Zeanah, & Nelson Iii, 2009; Colvert et al., 2008; Mueller et al., 2010; Navalta, Polcari, Webster, Boghossian, & Teicher, 2006), as documented by both parent/self reports as well as laboratory-based performance (e.g., go/nogo tasks). Despite being highly modifiable by caregiving factors, cognitive regulatory skills are also influenced by factors other than caregiving (e.g., genetic polymorphisms, Smith, Kryski, Sheikh, Singh, & Hayden, 2013; reviewed in Barnes, Dean, Nandam, O'Connell, & Bellgrove, 2011). These skills have been shown to be important moderators of stress-related phenotypes (Bardeen & Orcutt, 2011; Lengua et al., 2008), where individuals high on non-affective regulatory skills exhibit lower internalizing problems. Therefore, regulatory skills, which can mitigate high trait anxiety (Bar-Haim & Pine, 2013; Bishop, 2009; Carthy, Horesh, Apter, Edge, & Gross, 2010; Eldar et al., 2012; Etkin & Schatzberg, 2011; Hum, Manassis, & Lewis, ), may contribute to individual differences in affective outcomes following caregiving adversity.
Cognitive regulatory skills may benefit individuals with high anxiety because they contribute to more complex emotion regulation skills, such as cognitive reappraisal. Reappraisal is the process of “mentally transforming, or reappraising, the meaning of the emotion-eliciting situation” (Gross, 2013; Ochsner et al., 2004). It is a complex psychological process that builds on more basic cognitive regulation processes (Ochsner & Gross, 2008), and in the current study, we focused on inhibitory control. Studies have shown that cognitive reappraisal shares features with inhibitory control skills at multiple levels, including both behavioral and neural (Calrlson & Wang, 2007; Eisenberg & Spinrad, 2004). For example, inhibitory control is the ability to regulate undesired thoughts or actions, a critical component of cognitively reappraising distressing thoughts. At the neural level, cognitive reappraisal relies on the same prefrontal and cingulate regions that are recruited for successful inhibitory control (Ochsner, Silvers, & Buhle, 2012; Yarkoni, Poldrack, Nichols, Van Essen, & Wager, 2011), supporting the notion that cognitive reappraisal may build upon fundamental non-affective inhibitory control skills.
Many studies find that by experimentally increasing cognitive reappraisal use, anxiety (including laboratory-induced anxiety, clinical anxiety, and non-clinical trait anxiety) can be reduced (Davey, Burgess, & Rashes, 1995; Moore, Zoellner, & Mollenholt, 2008; Shurick et al., 2012), and these studies are important in demonstrating the causal role of regulatory processes in attenuating anxiety. There are also large differences in spontaneous and routine use of cognitive reappraisal strategies between one individual and another. As observed via laboratory manipulations, greater use of naturally occurring cognitive reappraisal has been associated with decreased anxiety (Egloff, Schmukle, Burns, & Schwerdtfeger, 2006), underscoring the importance of examining spontaneous regular use of cognitive reappraisal in individuals with a history of stress exposure.
Given that regulatory skills have been shown to have significant moderating effects on emotional processes, often acting to mitigate overarousal to emotionally eliciting events and stressors, identifying associations between individual differences in regulatory skills and stress-related phenotypes might provide insight into sources of resilience that buffer against exposure to adverse caregiving environments. We hypothesized that adults with a history of adverse caregiving would show evidence of poor inhibitory control, as measured by both self-report and laboratory-based tasks (emotional face go/nogo task). However, individual differences in inhibitory control would be associated with better mental health. That is, high inhibitory control was predicted to be associated with greater employment of cognitive reappraisal, which in turn would be associated with better stress-related outcomes (i.e., lower trait anxiety and basal salivary cortisol production). The individuals included in this study were adults with a history of FC during development, and at the time of testing, the majority of individuals were either enrolled in a 4-year college or had gained permanent employment. Therefore, this sample provided the opportunity to examine the effects of adverse caregiving in early adulthood, in the absence of current caregiving adversity.
METHOD
Participants
Fifty-three adult participants, 26 individuals with a history of foster care (FC group), 27 typical individuals without a history of foster care or any disrupted caregiving (comparison group) were recruited from college campuses and surrounding neighborhoods in the greater Los Angeles metropolitan area through ads posted in the Psychology department (for course credit) and on local bulletin boards. Demographic data are presented in Tables 1 and 2. The 27 comparison participants (mean (SD) age = 21(3) years old; 16F/11M), that are those without a history of FC, were a racially/ethnically diverse group (19% Black/African-, 19% Asian-, 33% European-, 11% Latino-American, 19% other/missing). All were physically and psychiatrically/neurologically healthy as determined by self-report during phone screening, all had very low trait anxiety scores (as measured by the Spielberger et al (1983) State/Trait Anxiety Inventory), and all were undergraduate students enrolled in a 4-year college. The 26 participants with a history of FC (mean(SD) age = 21(3) years old; 18F/8M), were also a racially/ethnically diverse group (35% Black/African-, 8% European-, 15% Asian-, 23% Latino-American, 8% mixed (African/European-American), 4% American Indian/Pacific Islander; 8% other/missing). The reasons for removal from birth home are provided in Table 1. Individuals had spent a mean (SD) of 6.4 (4.8) years in foster care (range: .5–18).
Table 1a.
Characteristics for the Foster Care (FC) and Comparison Participants
| FC (n = 26) | Comparison (n = 27) | |
|---|---|---|
| Participant sex | 18 female; 8 male | 16 female; 11 malea |
| Mean age in years (SD); range | 21 (3.1); 18–28 | 21 (3.23)b; 18–33 |
| Mean (SD) age in years when placed in first foster home; range | 8 (4.8); .1–16 | — |
| Mean (SD) time in years with biological parent(s); range | 9.1 (5.4); .1–18 | |
| Mean (SD) total time in years in foster care; range | 6.5 (4.7); .5–18 | — |
| Total number of foster care placements; range | 4.1 (7); 1–36 | — |
| % in Kinship foster care | 15.4% | |
| Mean (SD) self-reported overall quality of foster care/treatment (1 = poor/maltreatment, 10 = high/stable caregiving); range | 7 (2.6); 3–10 | — |
| Mean (SD) self-reported overall foster care experience (1 = poor/very negative, 10 = excellent/very positive); range | 6.1 (2.3); 1–10 | — |
| Percentage (SD) of life spent in care; range | 33% (23%); 3–89% | — |
| Mean (SD) self-reported quality of care with birth parents (1 = poor/maltreatment, 10 = high/stable caregiving); range | 4.7 (3.3); 1–10 | — |
| Mean (SD) self-reported overall experience living with birth parents (1 = poor/very negative, 10 = excellent/very positive); range | 4.4 (3.2); 1–10 | — |
| Reasons for removal from birth home (% of FC participants) (note: could be more than 1 reason) | Parent drug abuse (30%), physical abuse (17%), mother unfit (17%), domestic violence (13%), neglect/malnutrition (13%), emotional abuse (13%), sexual abuse (4%), death of parent (4%), mother involved in prostitution (4%), and truancy (4%) | — |
| Transition from foster care currently (% of FC participants) | Emancipated/aged-out of system or still formally in foster care (35%), returned to parent(s) (23%), living with a relative (15%), adopted or foster parents transitioned to legal guardianship (19%), and no response (7%) | — |
No significant group difference (X2 = .57, p = .45).
No significant group difference (t = .34, p = .73).
Table 1b.
Correlations Between Foster Care Related Variables
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Age placed in foster care | 1 | |||||
| 2. Age left foster care | .515** | 1 | ||||
| 3. Time in foster care | −.49* | .50* | 1 | |||
| 4. Time with biological parent | .81*** | .22 | −.62** | 1 | ||
| 5. Number of placements (1–2 vs. >3) | .04 | .28 | .25 | −.05 | 1 | |
| 6. Quality of foster caregiving (low vs. high) | −.11 | −.24 | −.12 | −.03 | −.48* | 1 |
p < .05.
p < .001.
p < .0001.
All participants were either students enrolled in a 4-year college/university in Southern California (comparison = 27/27; FC = 22/26) or were successfully employed (FC = 4/26). For participants in the FC group, there were no group differences between those enrolled in colleges versus those employed in caregiving-related variables (i.e., time in FC (p = .15), age removed from FC (p = .54), number of placements (p = .82), reported quality of foster care (p = .62)) or in the psychological characteristics measured within this study (i.e., Inhibitory control (p = .38), Cognitive Reappraisal Use (p = .49), Trait Anxiety (p = .58)). However, we did observe that those who were employed rather than in college were more likely to be placed in foster care at an earlier age (college mean (SD) = 8.9 years old (4.7), employed mean (SD) = 3.5 years old (1.3); t = 2.3, p < .05). Participants provided informed consent and received either $20 or course credit for their participation. The protocol was approved by the Institutional Review Board at the University of California, Los Angeles.
Self-Report Measures
Adult Temperament Questionnaire—Short Form (ATQ) (Evans & Rothbart, 2007)
This 77 item self-report measure of temperament produces five general factors of temperament. Likert-scale ratings ranging from 1 (extremely untrue) to 7 (extremely true) were obtained on each item, and subscales were composed of the mean of relevant items. For the present study we examined the three Effortful Control subscales: Activational (“Capacity to perform an action when there is a strong tendency to avoid it.” Example item: “I can keep performing a task even when I would rather not do it.”), Attentional (“Capacity to focus attention as well as to shift attention when desired.” Example item: “When interrupted or distracted, I usually can easily shift my attention back to whatever I was doing before.”), and Inhibitory control (“Capacity to suppress inappropriate approach behavior.” Example item: “It is easy for me to hold back my laughter in a situation when laughter wouldn't be appropriate.”). Previous work has found that the ATQ has good internal consistency and is correlated with individual difference traits measured using other well-validated instruments (Evans & Rothbart, 2007). All participants completed the ATQ.
Emotion Regulation Questionnaire (ERQ) (Gross & John, 2003)
This 10 item self-report measure is designed to assess individual differences in the habitual use of two emotion regulation strategies: cognitive reappraisal and expressive suppression. Reappraisal is a “form of cognitive change that involves construing a potentially emotion-eliciting situation in a way that changes its emotional impact” (example item: “I control my emotions by changing the way I think about the situation I'm in”). Suppression is a “form of response modulation that involves inhibiting ongoing emotion-expressive behavior” (example item: “I control my emotions by not expressing them”). Participants responded on a 7-point Likert-scale ranging from strongly disagree to strongly agree. Higher scores indicate greater use of a particular strategy. This measure has been shown to have good convergent and discriminant validity (Gross & John, 2003). Values on individual items were transformed to percent of maximum possible scores, which range from 0 to 100. Thus, percent of maximum possible scores (POMP transformation) for suppression and reappraisal were computed for each participant (Cohen, Cohen, Aiken, & West, 1999; McRae, Heller, John, & Gross, 2011) and then exponent transformed to account for non-normality of the data. All but two participants completed the ERQ.
State/Trait Anxiety Inventory (STAI) (Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983)
This 40-item self-report measure assesses the intensity of feelings of anxiety using a 4-point likert-scale ranging from almost never to almost always and distinguishes between state anxiety (i.e., a temporary condition experienced in specific situations) and trait anxiety (i.e., a general tendency to perceive situations as threatening). Higher scores indicate greater anxiety. This measure has been shown to have good reliability and consistency (Spielberger et al., 1983). All but one participant completed the STAI.
Life Events Questionnaire (Coddington, 1972, 1973)
This 40-item self-report measure assesses the presence or absence of major life events (e.g., move to a new home; death of a family member) within the past 12 months. The dependent measure of interest was the number of these life events that occurred within the past 12 months. This measure has been used in adolescents from multiple socioeconomic backgrounds (Coddington, 1972) showing significant correlations with emotional adjustment and personality variables (Compas, 1987).
Laboratory-Based Task
Emotional Face Go/Nogo (Hare et al., 2008; Tottenham, Hare, & Casey, 2011)
This computerized task, which is a standard go/nogo task using facial expressions as the stimuli, was administered to measure inhibitory control in affective contexts. We administered this task in addition to the ATQ measure of inhibitory control as a means of providing additional validity for the ATQ self-report measure. This task provides a measure of inhibitory control in both positive and in negative contexts; therefore, using this task allows us to observe whether poor inhibitory control is more evident in one emotional context versus another. The task required participants to press a button when a given facial expression (e.g., neutral) was displayed and withhold pressing for other expressions (e.g., fear). Face stimuli were presented singly in the center of the screen. Face stimuli were selected from a standardized set (Ekman & Friesen, 1976), and consisted of grayscale images of 10 adults (five males and five females) posing five different expressions (happy, fearful, angry, sad, and neutral). Visual angle of the face stimuli was approximately 12°. Participants were instructed to press a button as fast as they could when a named expression (e.g., neutral) was presented. These “go” trials occurred frequently (70% of the trials) in order to create a prepotent tendency for the participant to respond. Participants were instructed to withhold pressing a button for a “nogo” facial expression stimulus (e.g., fear), and these “nogo” trials occurred infrequently (30% of the trials). Participants were not told what the “nogo” faces were, but were instructed to withhold pressing for “any face other than the ‘go’ expression.” In each block, an emotional expression (either positive (happy) or negative (fear, angry, or sad)) was always paired with a neutral expression, and depending on the block, either the emotional expression served as the “go” stimulus (when neutral was the “nogo” stimulus) or as the “nogo” stimulus (when neutral was the “go” stimulus). Therefore, eight randomized blocks of “go–nogo” pairs (happy–neutral, neutral–happy, fear–neutral, neutral–fear, angry–neutral, neutral–angry, sad–neutral, and neutral–sad) with 30 randomized trials for each condition were administered to participants. Stimulus duration was 500 ms with 1,000 ms between trials to ensure that participants had enough time to respond. Practice trials were administered to ensure that participants understood the task and could execute the responses. Stimulus presentation and response collection was programmed using E-Prime software. Participants' data on the emotional face go/nogo task were only included if correct hit rate exceeded 75%, which resulted in the exclusion of one participant from the FC group.
The primary dependent measure of interest from the emotional face go/nogo task was accuracy, which was calculated as total trials minus errors [false alarms (i.e., errors of commission) + misses (i.e., errors of ommission)], which approximates a d-prime index (Tottenham et al., 2011). We calculated accuracy for four conditions: positive “go” block (the happy “go” with neutral “nogo” block); positive “nogo” block (the neutral “go” with happy “nogo” block); negative “go” blocks (mean across negative expression “go” with neutral “nogo” blocks); and negative “nogo” blocks (mean across neutral “go” with negative expression “nogo” blocks). Post hoc analyses were also included that examined false alarm rate versus miss rate (1–hit rate). Reaction times were computed for each of these four block types.
Basal Salivary Cortisol
Participants were provided with six salivettes (http://www.sarstedt.com) for home saliva collection. They were instructed to collect samples at three time points across 2 days: upon wake-up; 45 min following wake-up; and 5 PM. These times were selected to provide values of cortisol production throughout the day. Participants were instructed not to eat or brush their teeth before collection and to choose a day of average activity when they were feeling healthy, and they recorded daily journals on health and activity levels for confirmation. Participants were instructed to return their samples to the laboratory upon collection completion. When samples were received by the laboratory, they were placed in a freezer (−20°C) until assay. Eighty-seven percent of participants (46/53) returned complete salivary samples. Samples were shipped on dry ice to the laboratory of Dr. Clemens Kirschbaum (Technical University of Dresden) for assay. Since cortisol values are typically skewed, they were natural log transformed for statistical analyses.
Procedure
Participants visited the laboratory and completed the self-report measures. They were then seated in a quiet dark room approximately 55 cm away from the computer screen, where they were administered the emotional face go/nogo task. Following administration of the computerized tasks, participants were instructed on home salivary collection.
RESULTS
Descriptives From Self-Report Measures
Effortful Control Subscales (ATQ)
Individuals with a history of FC experience reported lower Inhibitory Control (t(51) = 2.44, p < .025) than the comparison group (Fig. 1), but there were no group differences for the other two Effortful Control subscales of the ATQ, Activational Control (t(51) = .43, ns) and Attentional Control (t(51) = .71, ns).
FIGURE 1.
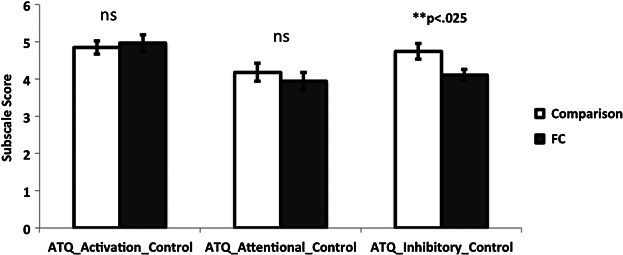
Group differences in Self-Reported Subscales of the Adult Temperament Questionnaire (ATQ). Individuals with a history of foster care (FC) reported lower levels of inhibitory control than the comparison group.
Emotion Regulation (ERQ)
There were no group differences in reporting of Reappraisal (t(49) = .75, ns, comparison mean(SD) = 2.00(.25) [raw average = 4.79], FC mean(SD) = 2.06(.32) [raw average = 4.97]) or Suppression scores (t(49) = 1.03, ns, comparison mean(SD) = 1.69(.30) [raw average = 3.55], FC mean (SD) = 1.77(.28) [raw average = 3.90]).
State/Trait Anxiety (Spielberger)
(Trait) Individuals with a history of FC experience reported higher trait anxiety (mean(SD) = 44(13)) than the comparison group mean(SD) = 37(8); t(50) = 2.25, p < .05 (Fig. 4A). (State) There were no group differences in state anxiety (t(50) = .38, ns; comparison mean(SD) = 36(8), FC mean(SD) = 35(11)).
FIGURE 4.
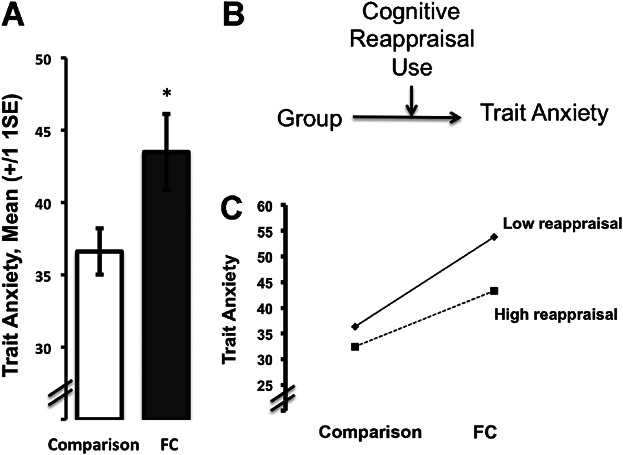
(A) Trait anxiety was higher in individuals in the foster care (FC) group. p < .05. (B) Reappraisal is an important moderator of the association between FC and trait anxiety. (C) The results of a regression analysis are plotted and show that individuals in the FC group with higher reappraisal skills had lower trait anxiety scores than those with lower reappraisal skills.
Life Events Questionnaire
There were no group differences in the number of major life events in the past 12 months, F(1,51) = .52, ns; comparison mean (SD) = 4.0 (2.9), FC mean (SD) = 4.5 (2.9). These values are within the range (mean = 4.71) previously reported in similarly aged participants (Coddington, 1972).
Laboratory-Based measure of Inhibitory Control (Emotional Face Go/Nogo Task)
The emotional face go/nogo task provided additional confidence in the validity of the participants' self-report of inhibitory control. We tested the hypothesis that individuals in the FC group would show lower accuracy (poorer inhibitory control), particularly in the context of negatively valenced emotional stimuli. Separate 2 (emotion: positive, negative) × 2 (stimulus type: go, nogo) × 2 (group) repeated measures ANOVAs were performed on the dependent measures of accuracy and reaction time on correct trials. For accuracy, there were main effects of emotion (F(1,49) = 39.39, p < 10−6, partial η2 = .45) and stimulus type (F(1,49) = 532.79, p < 10−6, partial η2 = .40), and an Emotion X Stimulus Type interaction (F(1,49) = 4.48, p < .05, partial η2 = .08). These effects were all qualified by an Emotion × Stimulus Type × Group interaction (F(1,49) = 4.15, p < .05, partial η2 = .08). As shown in Figure 2A, post hoc t-tests showed that a history of FC was associated significantly lower accuracy for the condition where negative facial expressions were the “nogo” stimulus relative to the comparison group (p < .05). For reaction time, there were main effects of emotion (F(1,49) = 4.11, p < .05, partial η2 = .08), which were qualified by an Emotion × Stimulus Type interaction (F(1,49) = 12.25, p < .001, partial η2 = .20) (Table 3). Post hoc t-tests showed that reaction time was slowest for the condition when a negative expression was the go stimulus (p < .001). There were no other main effects or interactions.
FIGURE 2.
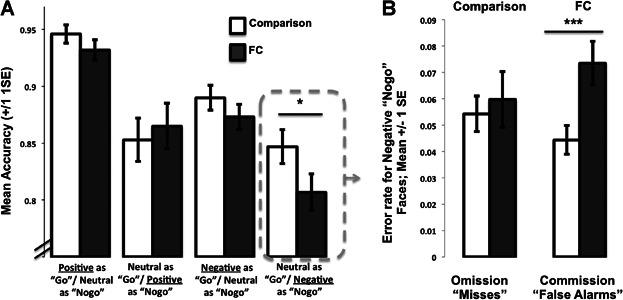
A history of foster care (FC) is associated with poorer inhibitory control in the context of negative information. (A) As assessed by the emotional face go/nogo task, individuals in the FC group exhibited lower accuracy (i.e., hits minus false alarms) during blocks when negative facial expressions served as the “nogo” stimuli. (B) Examination of error type (omission versus commission errors) showed that the source of the group differences was specific to errors of commission (i.e., false alarms) during blocks when negative facial expressions served as the “nogo” stimuli. *Between group p < .05, ***within group p < .005.
Table 2.
Reaction Times on the Laboratory Task (Emotional Face Go/Nogo)
| Group | Emotion | Stimulus Type | Mean (SD) |
|---|---|---|---|
| Comparison | Positive | Go | 401.13 (52.98) |
| Nogo | 407.70 (77.64) | ||
| Negative | Go | 440.38 (66.60) | |
| Nogo | 414.92 (57.85) | ||
| FC | Positive | Go | 387.18 (50.93) |
| Nogo | 407.78 (103.09) | ||
| Negative | Go | 413.63 (59.08) | |
| Nogo | 386.10 (84.12) |
Because our accuracy score combined both errors of omission (misses) and commission (false alarms), we further examined the low accuracy scores for the FC group in the negative expression nogo condition by directly comparing error types. Independent t-tests showed that individuals in the FC group had a significantly higher commission error rate (i.e., false alarm rates; mean(SD) = .07(.04)) than the comparison group (mean(SD) = .04(.03); t(48) = 3.02, p < .005), but the two groups did not differ in omission rates (i.e., miss rates; t(48) = .44, ns; comparison mean(SD) = .05(.03) & FC mean(SD) = .06(.05)) (Fig. 2B). These findings showed that individuals in the FC group had poorer inhibitory control specifically in the negative emotion condition.
Self-Report of Inhibitory Control Is Associated With Laboratory Task
Linear regression that included group, self-report of inhibitory control, and the interaction of the two showed a significant effect of the interaction on accuracy during the laboratory task (beta = 1.41, p < .05). Specifically, as shown in Figure 3A, individuals in the FC group with lower self-reported inhibitory control made more errors during the condition when negative emotions were the “nogo” faces; however, FC individuals with high self-reported inhibitory control made few errors in this condition of the task. These findings showed an association between self-reported inhibitory control and the laboratory-based measure of inhibitory control.
FIGURE 3.
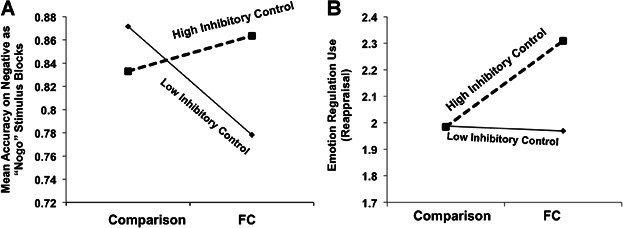
Inhibitory control as a moderator of group differences. (A) Individuals in the foster care (FC) group with high self-reported inhibitory control had high accuracy during the negative “nogo” blocks on the emotional face go/nogo relative to those with low self-reported inhibitory control (plotted here are the results of a regression analysis). (B) Individuals in the foster care group with high self-reported inhibitory control reported greater use of cognitive reappraisal strategies relative to those with low self-reported inhibitory control (plotted here are the results of a regression analysis).
Association Between Self-Report of Inhibitory Control and Emotion Regulation Strategies
These two self-report measures were significantly correlated with each other (comparison: r = −.72, p < .001; FC: r = −.48, p < .025). Linear regression that included group, self-report of inhibitory control, and the interaction of the two showed a significant interaction between group and inhibitory control on the use of cognitive reappraisal (Fig. 3B; Group × Inhibitory Control beta = 1.42, p < .05). A post hoc Pearson correlation test showed that those individuals in the FC group who reported greater inhibitory control also reported greater use of reappraisal strategies (r(24) = .50, p < .015). That is, inhibitory control had a significant association with reappraisal emotion regulation use for those in the FC group. An additional post hoc probe split groups into either low or high inhibitory control groups based on median-splits; post-hoc t-tests showed that within the high inhibitory control group, individuals in the FC group reported higher use of reappraisal strategies than the comparison group (t(21) = 2.28, p < .05). There were no significant associations between inhibitory control and suppression scores (p > .05).
Association Between Emotion Regulation and Trait Anxiety
We then tested the association between emotion regulation strategies and reported trait anxiety. A linear regression test including group (comparison, FC) and the two emotion regulation strategies of reappraisal and suppression as independent variables showed a negative association between reported reappraisal use and trait anxiety (beta = −.35, p < .01); there was no significant association between suppression and trait anxiety (beta = .19, ns). Secondly, we used linear regression to test whether reappraisal moderated the association between group and trait anxiety. This test was significant such that, as Figure 4B shows, those individuals in the FC group who reported greater use of reappraisal strategies also reported lower trait anxiety (Group × Reappraisal beta = −1.29, p < .015).
Basal Salivary Cortisol Production
A 3 (time of day) × 2 (group) × 2 (day) repeated measures ANOVA was performed on home cortisol levels. There was a significant effect of time of day (F(2,88) = 83.88, p < 10−6, partial η2 = .66) and group (F(1,44) = 5.86, p < .02, η2 = .12). As Figure 5A shows, individuals with a history of FC showed elevated cortisol production throughout the day. Although there was no interaction with time of day, planned t-tests were performed to identify the time of day when the largest discrepancy in salivary cortisol occurred. There was no group difference in cortisol levels at wake-up (t(44) = .48, ns), there was a trend towards a group difference 45 min after wake-up (t(44) = 1.92, p = .06), and there was a significant group difference at 5 PM (t(44) = 2.69, p < .01).
FIGURE 5.
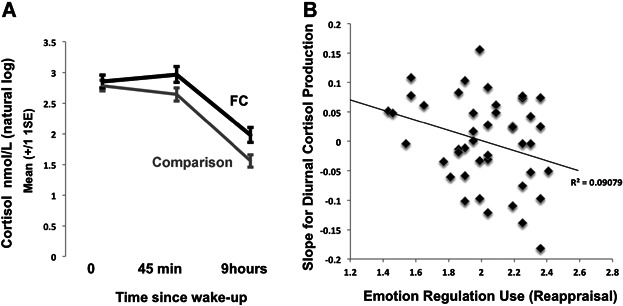
Associations with daily cortisol production. (A) Individuals with a history of foster care (FC) experience exhibit higher levels of daily salivary cortisol. (B) Greater reported use of reappraisal emotion regulation strategies is associated with greater declines in cortisol production throughout the day (more negative slopes).
Association Between Reappraisal Use and Salivary Cortisol
We computed slope throughout the day since our post-hoc tests above suggested that the group differences emerged largely as a function of evening levels. A slope for each participant was computed indexing the change in cortisol production from morning values to evening values with the equation:
Linear regression was used to test the association between reappraisal use (independent variable), with group (comparison, FC) included as a covariate, on cortisol slope throughout the day. Results showed that higher reported use of reappraisal strategies was associated with more negative slopes throughout the day (beta = −.29, p < .05; Figure 5B).
Association Between Caregiving Experiences and Self-Regulation
We examined the association between caregiving experiences for those participants with a history of FC and self-regulation using two separate linear regressions, one for inhibitory control and one for reappraisal. Age placed in FC,1 age when left FC, number of FC placements (binary coding: 1 = 1–2, 2 = 3+) and self-reported quality of FC experiences (binary coding based on median response from a 1 (poor quality)-10 (high quality) scale: 1 = 1–6, 2 = 7–10) were entered as independent variables. We chose to binarize number of FC placements and quality of FC experiences because of the skewed nature of the former and the arbitrary nature of the units in the latter. As shown in Figure 6, results showed that higher inhibitory control was associated with fewer foster care placements (beta = −.43, p < .05), but higher reappraisal use was associated with earlier removal from foster caregiving (beta = −.65, p < .015).
FIGURE 6.
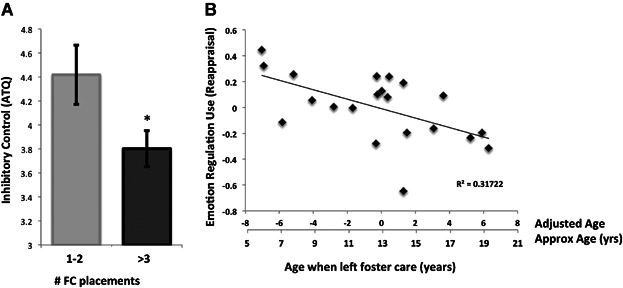
Caregiving Experiences and Regulatory Skills. (A) A higher number of caregiver placements were associated with decreased inhibitory control as measured by the Adult Temperament Questionnaire. p < .05 (B) Older age when exited foster care (FC) was associated with lower reappraisal emotion regulation strategy use as measured by the Emotion Regulation Questionnaire.
DISCUSSION
Individuals with a history of FC have, by definition, unstable caregiving experiences. Stress-related outcomes in this population have largely been examined during childhood and often at the time when children are living in unstable caregiving arrangements. The goal of the current study was to examine long-term stress-related phenotypes that extend into adulthood. We observed group differences in anxiety, inhibitory control, and salivary cortisol. However, the results of this study suggest that individual differences in inhibitory control may be a source of resilience for individuals with a history of FC. Higher inhibitory control in the FC group (relative to low inhibitory control) was associated with fewer negative-affect-related inhibitory control errors in the emotional face go/nogo task and greater reported use of cognitive reappraisal emotion regulation strategies. Therefore, the results of this study suggest that inhibitory control might contribute to better emotion regulation-related skills in adults with a history of FC.
In addition to lower self-reported inhibitory control in the FC group, low inhibitory control was observed during performance on the laboratory-based emotional face go/nogo task, which provided additional confidence for the low scores obtained on the self-report measure of inhibitory control. Specifically, individuals in the FC group exhibited more inhibitory control-related errors in the context of negative emotion as indexed by errors of commission (i.e., false alarms). This pattern of errors in negative emotion contexts has been observed in previous studies of early life caregiving adversity (Tottenham et al., 2010), and has been interpreted as poor inhibitory control in the context of highly emotional contexts. Statistical tests confirmed that individuals in the FC group with more inhibitory control errors also had lower self-reported inhibitory control. Thus, inhibitory control behavior during task was similar to and associated with self-report, thereby validating our reliance on the self-report measure.
Inhibitory control in the FC group was associated with higher reported use of cognitive reappraisal emotion regulation strategies, an association that adds support to the hypothesis that emotion regulation via reappraisal builds on non-affective cognitive regulation skills (Ochsner & Gross, 2008). Reappraisal is a strategy that has been shown to effectively and therapeutically attenuate high anxiety (Davey et al., 1995; Moore et al., 2008; Ochsner et al., 2012; Shurick et al., 2012). In the current study, we observed that although individuals in the FC group reported greater trait anxiety, those who also reported greater use of reappraisal strategies tended to have lower trait anxiety scores, consistent with the notion that cognitive regulation may be a resilience factor within this population. These findings suggest that inhibitory control might mitigate the negative impact of caregiving adversity on anxiety. We did not and could not manipulate regulatory skills in this study, which limits our ability to draw conclusions about causality between regulatory skills and stress-related phenotypes. There are numerous alternative sources of resilience to which individuals could have access (e.g., (epi-)genetic factors, social support, spiritual beliefs) that are not addressable by the current study. Additionally, there would certainly be heterogeneity in the degree of risk exposure, as suggested by participants' reports of caregiving experiences. Rutter (2012) has likened resilience to a “steeling” process, whereby the process of experiencing a stressor may itself be a source of resilience for many individuals such that negative experiences could have a strengthening effect. This conceptualization of resilience may explain why in the current study individuals within the FC group with high inhibitory control reported the highest levels of reappraisal strategy use, even higher than the comparison group. This finding suggests that a history of adversity may elicit greater use of adaptive emotion regulation processes—perhaps because of greater need to recruit emotion regulation strategies relative to a group without caregiving adversity. We had anticipated and observed that inhibitory control would be associated with greater cognitive reappraisal. Although on the surface, inhibitory control might be a process more consistent with the emotion regulation strategy of suppression rather than reappraisal, our findings showed the positive association between inhibitory control and reappraisal. This association suggests that the aspects of inhibitory control processes that allow for flexibly controlling undesired thoughts and actions may facilitate taking effortful control over undesired affective thoughts as well, a critical component of cognitive reappraisal.
Caregiving adversity has been associated with dysregulation of the HPA axis across several (semi) altricial species (e.g., mouse, rat, monkey, human) (reviewed in Gunnar & Quevedo, 2007; Tottenham & Sheridan, 2010). In the current sample, we also observed group differences in diurnal basal levels of salivary cortisol production, such that daily cortisol production in the FC group was significantly higher throughout the day relative to the comparison group. Planned post hoc tests showed that this group differences was largely attributable to higher evening levels. This finding suggests that the differences in caregiving experienced by the two groups not only alter HPA axis in childhood (Bernard et al., 2010; Bruce et al., 2009; Dozier et al., 2006; Fisher et al., 2000, 2006, 2007, 2011; Graham et al., 2012), but also extend into adulthood. In contrast to the blunted morning cortisol levels often observed during childhood, we observed high levels in the current adult sample, which is consistent with other studies that have found hypersecretion of daily cortisol in adults with a history of early life stress (Gonzalez, Jenkins, Steiner, & Fleming, 2009; Nicolson, 2004). These age-related differences may be due to several factors, including age-related differences in evening activity, which can influence evening cortisol levels (Kertes & Gunnar, 2004). Alternatively, they may reflect developmental changes that occur in HPA axis organization after several years (Gunnar & Quevedo, 2007), which have been attributed to temporal adaptations of the HPA axis (e.g., at the level of the adrenal gland) that can occur following early stress exposure (Newport, Heim, Bonsall, Miller, & Nemeroff, 2004) and may be maintained in part by concurrent internalizing behaviors in adulthood (Ruttle et al., 2011). The current study cannot address such alternatives.
The steepness in cortisol slope was inversely associated with the emotion regulation skill of reappraisal. That is, individuals who reported greater use of reappraisal strategies exhibited greater declines in cortisol production throughout the day. This finding suggests that cognitive strategies may have powerful top-down modulatory effects on the physiological activity of systems sensitive to caregiving adversity, and that these influences are apparent during adulthood. A limitation of our cortisol measure is that since we did not use time stamping measures that provide an accurate assessment of collection time (Adam & Kumari, 2009), we cannot be confident that the time of collection was accurate across all individuals. However, the main effect of time of day, that is, all participants showed the typical decline in values across the day, provides some degree of confidence for the obtained values.
Because of the quasi-experimental nature of this study, that is because the caregiving groups were not randomly assigned, we cannot make inferences about causality. While strong evidence for a causal association between adverse caregiving and these stress-related outcomes has been cited (Dozier et al., 2002; Fisher et al., 2000; McDermott et al., 2013; McGoron et al., 2012), many factors may contribute to these outcomes, including separation from primary caregivers, exposure to teratogenic substances (i.e., drugs and alcohol), early neglect and abuse, and traumatic events that lead to separation. Moreover, there are numerous other sources of heterogeneity in this sample (e.g., time in foster care; number of placements; quality of caregiving). On the one hand, this heterogeneity makes it difficult to discuss these participants as a single group. On the other hand, individual differences in FC experiences provide the opportunity to examine associations within the foster care group. For example, the dose-response associations between regulatory skills and caregiving experiences provide support for the notion that caregiving experiences can negatively impact regulatory skills. Better inhibitory control was associated with fewer FC placements, whereas greater reported use of reappraisal strategies was associated with an earlier exit from foster caregiving (which was typically either because of adoption by a family or reunion with birth/extended family). We did not observe associations between individual differences in foster care experiences and performance on the emotional face go/nogo, despite observing significant group differences on the task. It may be that the task was sensitive to group differences within the small sample size used in this article, but not individual differences in caregiving, a characteristic that has previously been observed using this task (Tottenham et al., 2011). That inhibitory control and reappraisal use were influenced by two different aspects of caregiving (two caregiving variables that were not correlated in the current sample) suggests that there are unique contributions of each experience on cognitive development. Although speculative, a high number of caregiving transitions (which has been associated with alterations to the HPA axis during childhood; Fisher et al., 2006) may have different cognitive effects than the experience of exiting the foster care system at older ages. It is of course possible that poorer regulatory ability contributed to longer stays in unstable caregiving (e.g., child-elicited effects; Pardeck, 1983), and the current study cannot address that possibility. Secondly, this association has important policy implications in that it provides empirical evidence that encourages earlier removal from unstable caregiving conditions. These findings support the well-established notion that earlier adoption and fewer transitions are always beneficial, as has been noted by other studies (Dozier et al., 2002).
We used self-report measures of inhibitory control, emotion regulation, and anxiety. We observed significant associations between these factors, which could be indications of important and real associations between these psychological processes but could also be the result of shared variance between self-report measures. We cannot say with certainty from the current results, and the reliance on self-report reduces our ability to infer the causal relationship between early caregiving adversity and these measures. Self-report measures can be very informative indices of psychological processes, like anxiety and temperament (Evans & Rothbart, 2007; Spielberger et al., 1983). Nonetheless, we included additional measures such as laboratory-based tasks and salivary cortisol as a means of characterizing mental health in adults with a history of FC.
The current study was based on a relatively small sample and there was heterogeneity in the FC sample (e.g., some were enrolled in a 4-year college whereas others were employed), in addition to the large heterogeneity in caregiving experiences listed earlier. The sample size and the nature of the samples further limit our ability to make causal inferences about early adverse caregiving. However, the large degree of convergence across several methods provide evidence that a history of caregiving adversity and instability has long-term implications for affect-related regulatory abilities that are observable in a group of high functioning adults (e.g., college enrollment/employment and normative exposure to recent major life events). Despite the caregiving adversity, which in some cases was quite extreme, the level of functioning across participants suggests a high degree of resilience in the FC group. Therefore, group differences in stress-related outcomes may be further pronounced in a more extreme group. Individual differences in regulatory skills were associated with lower trait anxiety and cortisol, suggesting a potential mitigating role for regulatory skills on stress-related outcomes. The results of this study have implications for adult-based interventions. While caregiver-based interventions have proven highly efficacious during development (e.g., Dozier et al., 2002; Fisher et al., 2006), interventions aimed at adult FC populations might benefit from targeting cognitive regulatory skills. This type of intervention (e.g., improving cognitive regulatory skill) has already proven effective in reducing anxiety in individuals with high anxiety (Eldar et al., 2012; Eldar, Ricon, & Bar-Haim, 2008), and the results from the current study suggest the same might be true for individuals with a history of caregiving adversity.
Acknowledgments
This work was supported by NIMH R01MH091864 (NT), the UCLA McNair Research Scholars Program (AJJ), and the American Psychological Association NIGMS Research Fellowship Program (AJJ).
Footnotes
As shown in Table 2, “Time with Biological Family” was highly (inversely) correlated with “Age Placed in FC”, and therefore the two variables would have a high degree of shared variance if included in the same model. Nonetheless, we tested the for the possible effects of “Time with Biological Family” by re-performing these analyses replacing “Age Placed in FC” with “Time with Biological Family”. These analyses showed that “Time with Biological Family” did not account for the variance in either “Inhibitory Control” (p = .20) or “Reappraisal Use” (p < .22).
REFERENCES
- Adam EK. Kumari M. Assessing salivary cortisol in large-scale, epidemiological research. Psychoneuroendocrinology. 2009;34(10):1423–1436. doi: 10.1016/j.psyneuen.2009.06.011. [DOI] [PubMed] [Google Scholar]
- Bar-Haim Y. Pine DS. Cognitive training research and the search for a transformative, translational, developmental cognitive neuroscience. Developmental Cognitive Neuroscience. 2013;4:1–2. doi: 10.1016/j.dcn.2013.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bardeen JR. Orcutt HK. Attentional control as a moderator of the relationship between posttraumatic stress symptoms and attentional threat bias. Journal of Anxiety Disorders. 2011;25(8):1008–1018. doi: 10.1016/j.janxdis.2011.06.009. [DOI] [PubMed] [Google Scholar]
- Barnes JJM, Dean AJ, Nandam LS, O'Connell RG. Bellgrove MA. The molecular genetics of executive function: Role of monoamine system genes. Biological Psychiatry. 2011;69(12):e127–e143. doi: 10.1016/j.biopsych.2010.12.040. [DOI] [PubMed] [Google Scholar]
- Bernard K, Butzin-Dozier Z, Rittenhouse J. Dozier M. Cortisol production patterns in young children living with birth parents vs children placed in foster care following involvement of Child Protective Services. Archives of Pediatrics & Adolescent Medicine. 2010;164(5):438–443. doi: 10.1001/archpediatrics.2010.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bishop SJ. Trait anxiety and impoverished prefrontal control of attention. Nature Neuroscience. 2009;12(1):92–98. doi: 10.1038/nn.2242. [DOI] [PubMed] [Google Scholar]
- Bos KJ, Fox N, Zeanah CH. Nelson Iii CA. Effects of early psychosocial deprivation on the development of memory and executive function. Frontiers in Behavioral Neuroscience. 2009;3:16. doi: 10.3389/neuro.08.016.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruce J, Fisher PA, Pears KC. Levine S. Morning cortisol levels in preschool-aged foster children: Differential effects of maltreatment type. Developmental Psychobiology. 2009;51(1):14–23. doi: 10.1002/dev.20333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruskas D. Children in foster care: A vulnerable population at risk. Journal of Child and Adolescent Psychiatric Nursing. 2008;21(2):70–77. doi: 10.1111/j.1744-6171.2008.00134.x. [DOI] [PubMed] [Google Scholar]
- Calrlson SM. Wang TS. Inhibitory control and emotion regulation in preschool children. Cognitive Development. 2007;22(4):489–510. [Google Scholar]
- Carthy T, Horesh N, Apter A, Edge MD. Gross JJ. Emotional reactivity and cognitive regulation in anxious children. Behaviour Research and Therapy. 2010;48(5):384–393. doi: 10.1016/j.brat.2009.12.013. [DOI] [PubMed] [Google Scholar]
- Coddington RD. The significance of life events as etiologic factors in the diseases of children. II. A study of a normal population. Journal of Psychosomatic Research. 1972;16(3):205–213. doi: 10.1016/0022-3999(72)90045-1. [DOI] [PubMed] [Google Scholar]
- Cohen P, Cohen J, Aiken LS. West SG. The problem of units and the circumstance for POMP. Multivariate Behavioral Research. 1999;34:315–346. [Google Scholar]
- Colvert E, Rutter M, Kreppner J, Beckett C, Castle J, Groothues C. Sonuga-Barke EJ. Do theory of mind and executive function deficits underlie the adverse outcomes associated with profound early deprivation? Findings from the English and Romanian adoptees study. Journal of Abnormal Child Psychology. 2008;36(7):1057–1068. doi: 10.1007/s10802-008-9232-x. [DOI] [PubMed] [Google Scholar]
- Compas BE. Coping with stress during childhood and adolescence. Psychological Bulletin. 1987;101(3):393–403. [PubMed] [Google Scholar]
- Damnjanovic M, Lakic A, Stevanovic D. Jovanovic A. Effects of mental health on quality of life in children and adolescents living in residential and foster care: A cross-sectional study. Epidemiology and Psychiatric Sciences. 2011;20(3):257–262. doi: 10.1017/s2045796011000291. [DOI] [PubMed] [Google Scholar]
- Davey GC, Burgess I. Rashes R. Coping strategies and phobias: The relationship between fears, phobias and methods of coping with stressors. The British Journal of Clinical Psychology. 1995;34(Pt 3):423–434. doi: 10.1111/j.2044-8260.1995.tb01477.x. [DOI] [PubMed] [Google Scholar]
- Dozier M, Albus K, Fisher PA. Sepulveda S. Interventions for foster parents: Implications for developmental theory. Development and Psychopathology. 2002;14(4):843–860. doi: 10.1017/s0954579402004091. [DOI] [PubMed] [Google Scholar]
- Dozier M, Manni M, Gordon MK, Peloso E, Gunnar MR, Stovall-McClough KC. Levine S. Foster children's diurnal production of cortisol: An exploratory study. Child Maltreatment. 2006;11(2):189–197. doi: 10.1177/1077559505285779. [DOI] [PubMed] [Google Scholar]
- Egloff B, Schmukle SC, Burns LR. Schwerdtfeger A. Spontaneous emotion regulation during evaluated speaking tasks: Associations with negative affect, anxiety expression, memory, and physiological responding. Emotion. 2006;6(3):356–366. doi: 10.1037/1528-3542.6.3.356. [DOI] [PubMed] [Google Scholar]
- Eisenberg N. Spinrad TL. Emotion-related regulation: Sharpening the definition. Child Development. 2004;75(2):334–339. doi: 10.1111/j.1467-8624.2004.00674.x. [DOI] [PubMed] [Google Scholar]
- Ekman P. Friesen WV. Pictures of facial affect. Palo Alto, CA: Consulting Psychologists Press; 1976. [Google Scholar]
- Eldar S, Apter A, Lotan D, Edgar KP, Naim R, Fox NA. Bar-Haim Y. Attention bias modification treatment for pediatric anxiety disorders: A randomized controlled trial. The American Journal of Psychiatry. 2012;169(2):213–220. doi: 10.1176/appi.ajp.2011.11060886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eldar S, Ricon T. Bar-Haim Y. Plasticity in attention: Implications for stress response in children. Behaviour Research and Therapy. 2008;46(4):450–461. doi: 10.1016/j.brat.2008.01.012. [DOI] [PubMed] [Google Scholar]
- Etkin A. Schatzberg AF. Common abnormalities and disorder-specific compensation during implicit regulation of emotional processing in generalized anxiety and major depressive disorders. The American Journal of Psychiatry. 2011;168(9):968–978. doi: 10.1176/appi.ajp.2011.10091290. [DOI] [PubMed] [Google Scholar]
- Evans DE. Rothbart MK. Development of a model for adult temperament. Journal of Research in Personality. 2007;41:868–888. [Google Scholar]
- Fisher PA, Gunnar MR, Chamberlain P. Reid JB. Preventive intervention for maltreated preschool children: Impact on children's behavior, neuroendocrine activity, and foster parent functioning. Journal of the American Academy of Child and Adolescent Psychiatry. 2000;39(11):1356–1364. doi: 10.1097/00004583-200011000-00009. [DOI] [PubMed] [Google Scholar]
- Fisher PA, Gunnar MR, Dozier M, Bruce J. Pears KC. Effects of therapeutic interventions for foster children on behavioral problems, caregiver attachment, and stress regulatory neural systems. Annals of the New York Academy of Sciences. 2006;1094:215–225. doi: 10.1196/annals.1376.023. [DOI] [PubMed] [Google Scholar]
- Fisher PA, Stoolmiller M, Gunnar MR. Burraston BO. Effects of a therapeutic intervention for foster preschoolers on diurnal cortisol activity. Psychoneuroendocrinology. 2007;32(8–10):892–905. doi: 10.1016/j.psyneuen.2007.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher PA, Van Ryzin MJ. Gunnar MR. Mitigating HPA axis dysregulation associated with placement changes in foster care. Psychoneuroendocrinology. 2011;36(4):531–539. doi: 10.1016/j.psyneuen.2010.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garland AF, Hough RL, McCabe KM, Yeh M, Wood PA. Aarons GA. Prevalence of psychiatric disorders in youths across five sectors of care. Journal of the American Academy of Child and Adolescent Psychiatry. 2001;40(4):409–418. doi: 10.1097/00004583-200104000-00009. [DOI] [PubMed] [Google Scholar]
- Gonzalez A, Jenkins JM, Steiner M. Fleming AS. The relation between early life adversity, cortisol awakening response and diurnal salivary cortisol levels in postpartum women. Psychoneuroendocrinology. 2009;34(1):76–86. doi: 10.1016/j.psyneuen.2008.08.012. [DOI] [PubMed] [Google Scholar]
- Graham AM, Yockelson M, Kim HK, Bruce J, Pears KC. Fisher PA. Effects of maltreatment and early intervention on diurnal cortisol slope across the start of school: A pilot study. Child Abuse & Neglect. 2012;36(9):666–670. doi: 10.1016/j.chiabu.2012.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross JJ. Emotion regulation: Taking stock and moving forward. Emotion. 2013;13(3):359–365. doi: 10.1037/a0032135. [DOI] [PubMed] [Google Scholar]
- Gross JJ. John OP. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology. 2003;85(2):348–362. doi: 10.1037/0022-3514.85.2.348. [DOI] [PubMed] [Google Scholar]
- Gunnar MR. Quevedo K. The neurobiology of stress and development. Annual Review of Psychology. 2007;58:145–173. doi: 10.1146/annurev.psych.58.110405.085605. [DOI] [PubMed] [Google Scholar]
- Hare TA, Tottenham N, Galvan A, Voss HU, Glover GH. Casey BJ. Biological substrates of emotional reactivity and regulation in adolescence during an emotional go-nogo task. Biological Psychiatry. 2008;63(10):927–934. doi: 10.1016/j.biopsych.2008.03.015015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hum KM, Manassis K. Lewis MD. Neurophysiological markers that predict and track treatment outcomes in childhood anxiety. Journal of Abnormal Child Psychology. 2013;41:1243–1255. doi: 10.1007/s10802-013-9755-7. [DOI] [PubMed] [Google Scholar]
- Jackson LJ, O'Brien K. Pecora PJ. Posttraumatic stress disorder among foster care alumni: The role of race, gender, and foster care context. Child Welfare. 2011;90(5):71–93. [PubMed] [Google Scholar]
- Kertes DA. Gunnar MR. Evening activities as a potential confound in research on the adrenocortical system in children. Child Development. 2004;75(1):193–204. doi: 10.1111/j.1467-8624.2004.00663.x. [DOI] [PubMed] [Google Scholar]
- Lawrence CR, Carlson EA. Egeland B. The impact of foster care on development. Development and Psychopathology. 2006;18(1):57–76. doi: 10.1017/S0954579406060044. [DOI] [PubMed] [Google Scholar]
- Lengua LJ, Bush NR, Long AC, Kovacs EA. Trancik AM. Effortful control as a moderator of the relation between contextual risk factors and growth in adjustment problems. Development and Psychopathology. 2008;20(2):509–528. doi: 10.1017/S0954579408000254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis EE, Dozier M, Ackerman J. Sepulveda-Kozakowski S. The effect of placement instability on adopted children's inhibitory control abilities and oppositional behavior. Development and Psychopathology. 2007;43(6):1415–1427. doi: 10.1037/0012-1649.43.6.1415. [DOI] [PubMed] [Google Scholar]
- Linares LO, Li M, Shrout PE, Ramirez-Gaite M, Hope S, Albert A. Castellanos FX. The course of inattention and hyperactivity/impulsivity symptoms after foster placement. Pediatrics. 2010;125(3):e489–e498. doi: 10.1542/peds.2009-1285. [DOI] [PubMed] [Google Scholar]
- Loman MM, Johnson AE, Westerlund A, Pollak SD, Nelson CA. Gunnar MR. The effect of early deprivation on executive attention in middle childhood. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 2013;54(1):37–45. doi: 10.1111/j.1469-7610.2012.02602.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS. Ordinary magic: Lessons from research on resilience in human development. Education Canada. 2009;49(3):28–32. [Google Scholar]
- McDermott JM, Troller-Renfree S, Vanderwert R, Nelson CA, Zeanah CH. Fox NA. Psychosocial deprivation, executive functions, and the emergence of socio-emotional behavior problems. Frontiers in Human Neuroscience. 2013;7:167. doi: 10.3389/fnhum.2013.00167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGoron L, Gleason MM, Smyke AT, Drury SS, Nelson CA, Gregas MC. Zeanah CH. Recovering from early deprivation: Attachment mediates effects of caregiving on psychopathology. Journal of the American Academy of Child and Adolescent Psychiatry. 2012;51(7):683–693. doi: 10.1016/j.jaac.2012.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Kubzansky LD, Dunn EC, Waldinger R, Vaillant G. Koenen KC. Childhood social environment, emotional reactivity to stress, and mood and anxiety disorders across the life course. Depress Anxiety. 2010;27(12):1087–1094. doi: 10.1002/da.20762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McRae K, Heller SM, John OP. Gross JJ. Context-dependent emotion regulation: Suppression and reappraisal at the burning man festival. Basic and Applied Social Psychology. 2011;33:346–350. [Google Scholar]
- Merz EC, McCall RB, Wright AJ. Luna B. Inhibitory control and working memory in post-institutionalized children. J Abnorm Child Psychol. 2013;41:879–890. doi: 10.1007/s10802-013-9737-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore SA, Zoellner LA. Mollenholt N. Are expressive suppression and cognitive reappraisal associated with stress-related symptoms. Behaviour Research and Therapy. 2008;46(9):993–1000. doi: 10.1016/j.brat.2008.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mueller SC, Maheu FS, Dozier M, Peloso E, Mandell D, Leibenluft E. Ernst M. Early-life stress is associated with impairment in cognitive control in adolescence: An fMRI study. Neuropsychologia. 2010;48(10):3037–3044. doi: 10.1016/j.neuropsychologia.2010.06.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Navalta CP, Polcari A, Webster DM, Boghossian A. Teicher MH. Effects of childhood sexual abuse on neuropsychological and cognitive function in college women. The Journal of Neuropsychiatry and Clinical Neurosciences. 2006;18(1):45–53. doi: 10.1176/jnp.18.1.45. [DOI] [PubMed] [Google Scholar]
- Neely-Barnes S. Whitted K. Examining the social, emotional and behavioral needs of youth involved in the child welfare and juvenile justice systems. Journal of Health and Human Services Administration. 2011;34(2):206–238. [PubMed] [Google Scholar]
- Newport DJ, Heim C, Bonsall R, Miller AH. Nemeroff CB. Pituitary-adrenal responses to standard and low-dose dexamethasone suppression tests in adult survivors of child abuse. Biological Psychiatry. 2004;55(1):10–20. doi: 10.1016/s0006-3223(03)00692-9. [DOI] [PubMed] [Google Scholar]
- Nicolson NA. Childhood parental loss and cortisol levels in adult men. Psychoneuroendocrinology. 2004;29(8):1012–1018. doi: 10.1016/j.psyneuen.2003.09.005. [DOI] [PubMed] [Google Scholar]
- Ochsner K. Gross J. Cognitive emotion regulation: Insights from social cognitive and affective neuroscience. Current Directions in Psychological Science. 2008;17(2):153–158. doi: 10.1111/j.1467-8721.2008.00566.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ochsner KN, Ray RD, Cooper JC, Robertson ER, Chopra S, Gabrieli JD. Gross JJ. For better or for worse: Neural systems supporting the cognitive down- and up-regulation of negative emotion. Neuroimage. 2004;23(2):483–499. doi: 10.1016/j.neuroimage.2004.06.030. [DOI] [PubMed] [Google Scholar]
- Ochsner KN, Silvers JA. Buhle JT. Functional imaging studies of emotion regulation: A synthetic review and evolving model of the cognitive control of emotion. Annals of the New York Academy of Sciences. 2012;1251:E1–E24. doi: 10.1111/j.1749-6632.2012.06751.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pardeck JT. An empirical analysis of behavioral and emotional problems of foster children as related to replacement in care. Child Abuse & Neglect. 1983;7(1):75–78. doi: 10.1016/0145-2134(83)90033-9. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Nelson CA, Schlaak MF, Roeber BJ, Wewerka SS, Wiik KL. Gunnar MR. Neurodevelopmental effects of early deprivation in postinstitutionalized children. Child Development. 2010;81(1):224–236. doi: 10.1111/j.1467-8624.2009.01391.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogosch FA, Dackis MN. Cicchetti D. Child maltreatment and allostatic load: Consequences for physical and mental health in children from low-income families. Development and Psychopathology. 2011;23(4):1107–1124. doi: 10.1017/S0954579411000587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rusby JS. Tasker F. Long-term effects of the British evacuation of children during World War 2 on their adult mental health. Aging Ment Health. 2009;13(3):391–404. doi: 10.1080/13607860902867750. [DOI] [PubMed] [Google Scholar]
- Rutter M. Resilience as a dynamic concept. Development and Psychopathology. 2012;24(2):335–344. doi: 10.1017/S0954579412000028. [DOI] [PubMed] [Google Scholar]
- Ruttle PL, Shirtcliff EA, Serbin LA, Fisher DB, Stack DM. Schwartzman AE. Disentangling psychobiological mechanisms underlying internalizing and externalizing behaviors in youth: Longitudinal and concurrent associations with cortisol. Hormones and Behavior. 2011;59(1):123–132. doi: 10.1016/j.yhbeh.2010.10.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sawyer MG, Carbone JA, Searle AK. Robinson P. The mental health and wellbeing of children and adolescents in home-based foster care. The Medical Journal of Australia. 2007;186(4):181–184. doi: 10.5694/j.1326-5377.2007.tb00857.x. [DOI] [PubMed] [Google Scholar]
- Shurick AA, Hamilton JR, Harris LT, Roy AK, Gross JJ. Phelps EA. Durable effects of cognitive restructuring on conditioned fear. Emotion. 2012;12(6):1393–1397. doi: 10.1037/a0029143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simmel C, Brooks D, Barth RP. Hinshaw SP. Externalizing symptomatology among adoptive youth: Prevalence and preadoption risk factors. Journal of Abnormal Child Psychology. 2001;29(1):57–69. doi: 10.1023/a:1005251513130. [DOI] [PubMed] [Google Scholar]
- Smith HJ, Kryski KR, Sheikh HI, Singh SM. Hayden EP. The role of parenting and dopamine D4 receptor gene polymorphisms in children's inhibitory control. Developmental Science. 2013;16(4):515–530. doi: 10.1111/desc.12046. [DOI] [PubMed] [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene R, Vagg PR. Jacobs GA. Manual for the state-trait anxiety inventory. Palo Alto, CA: Consulting Psychologists Press, Inc; 1983. [Google Scholar]
- Steele JS. Buchi KF. Medical and mental health of children entering the utah foster care system. Pediatrics. 2008;122(3):e703–e709. doi: 10.1542/peds.2008-0360. [DOI] [PubMed] [Google Scholar]
- Thompson RG. Hasid D. Psychiatric disorders and treatment among newly homeless young adults with histories of foster care. Psychiatric Services. 2012;63(9):906–912. doi: 10.1176/appi.ps.201100405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N. Human amygdala development in the absence of species-expected caregiving. Developmental Psychobiology. 2012;54(6):598–611. doi: 10.1002/dev.20531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N, Hare TA. Casey BJ. Behavioral assessment of emotion discrimination, emotion regulation, and cognitive control in childhood, adolescence, and adulthood. Frontiers in Psychology. 2011;2:39. doi: 10.3389/fpsyg.2011.00039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N, Hare TA, Millner A, Gilhooly T, Zevin JD. Casey BJ. Elevated amygdala response to faces following early deprivation. Developmental Science. 2011;14(2):190–204. doi: 10.1111/j.1467-7687.2010.00971.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N, Hare TA, Quinn BT, McCarry T, Nurse M, Gilhooly T. Casey BJ. Prolonged institutional rearing is associated with atypically large amygdala volume and difficulties in emotion regulation. Developmental Science. 2010;13(1):46–61. doi: 10.1111/j.1467-7687.2009.00852.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N. Sheridan M. A Review of adversity, the amygdala and the hippocampus: A Consideration of developmental timing. Frontiers in Human Neuroscience. 2010;3:1–18. doi: 10.3389/neuro.09.068.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiik KL, Loman MM, Van Ryzin MJ, Armstrong JM, Essex MJ, Pollak SD. Gunnar MR. Behavioral and emotional symptoms of post-institutionalized children in middle childhood. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 2011;52(1):56–63. doi: 10.1111/j.1469-7610.2010.02294.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yarkoni T, Poldrack RA, Nichols TE, Van Essen DC. Wager TD. Large-scale automated synthesis of human functional neuroimaging data. Nature Methods. 2011;8(8):665–670. doi: 10.1038/nmeth.1635. [DOI] [PMC free article] [PubMed] [Google Scholar]