

Abstract
Purpose:
To estimate test-retest reliability, inter-rater reliability and validation of a method for measuring balance by stepping over four squares, four square step test (FSST) in children with Down syndrome (DS).
Methods:
A sample of 13 children with DS was recruited for the cross-sectional study. They were asked to perform FSST and the time taken was noted. For estimating test-retest reliability, FSST was done by principal investigator twice and Inter-rater reliability was assessed by principal investigator and second investigator with an interval of 7 days. FRT was used as the criterion dynamic balance measure to validate FSST. The data was tabulated and analysed statistically.
Results:
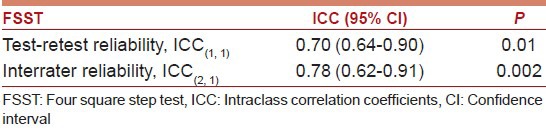
The test-retest reliability and inter-rater reliability of FSST are ICC(1,1) = 0.70 (0.64-0.90) and ICC(2,1) = 0.78 (0.62-0.91) respectively. The Bland-Altman limits of agreement were also satisfied. Concurrent validity between FRT and FSST with Spearman's ρ = −0.58 (−0.86 to −0.13).
Conclusion:
FSST has moderate to good concurrent validity and good reliability among the children with Down syndrome.
Keywords: Down syndrome, dynamic balance, functional reach test, inter-rater reliability, test-retest reliability, validity
Introduction and Purpose
According to World Health Organization (WHO) the estimated incidence of Down syndrome (DS) is between 1 in 1,000 and 1 in 1,100 live births worldwide. Each year approximately 3,000–5,000 children are born with this chromosome disorder.[1] Children with DS have problems in the gross motor development, cognitive development, body balance, functional balance and problems with fine motor skills such as coordination.[2,3] They have hypotonia, increased reaction time in performing voluntary activities, muscle weakness due to inadequate co-contraction and improper sensory integration.[2] Many researchers have proven that the individual with DS has difficulty in maintaining their line of gravity (LOG) within the base of support (BOS) and have worse balance compared to their counterparts.[3,4] Thus children with DS have difficulty in maintaining balance. Most equipment used for measuring balance is costly, highly technical and not portable. So, there is a need to validate the cheap and feasible balance test for the children with DS. Four square step test (FSST) is one among them that needs to be validated.
FSST is a dynamic standing balance test.[5] It is designed to assess the ability to rapidly cross over obstacle and change direction in a clinical setting. It requires minimal space, equipment and time. The FSST is easy to score, and quick to administer. It involves stepping over low objects and movement in four directions. Dite and Temple[6] had performed FSST on older adults to identify multiple falls. FSST was carried out for 15 s and subjects with score greater than 15 s are considered multiple fallers and those with score <15 as non-multiple fallers. Similarly, FSST was performed on patients with unilateral trans-tibial amputations by Dite et al.[7] to examine functional mobility which could discriminate between multiple falling and non-multiple falling people. Here, the time taken by each subject for FSST was ≥24 s which helped to identify multiple fall risks. The same test was performed in patients with vestibular disorders by Whitney et al.[8] who frequently report falling and they have difficulty in changing the direction and test performed was for >12 s. Also in people with multiple sclerosis FSST was performed by Nilsagård et al.[9] with respect to their clinical variables and predictive values to measure the accidental falls and near falls incidents.
Blennerhassett et al.[10] has performed FSST on stroke patients to investigate whether clinical test score at discharge predicts falls or limited community mobility after stroke and also to check walking and dynamic standing balance change after discharge. On chronic stroke patients Goh et al.[5] performed FSST. In recent, the study was done with people with Parkinson's disease (PD) by Duncan and Earhart.[11] He stated FSST, as a quick and simple test of multidirectional stepping which may be useful in predicting falls in people with PD. Salis and Samuel[12] established the test-retest (ICC = 0.85) and inter-rater reliability (ICC = 0.88) of FSST among the children with typical development (CTD).
Most of the above mentioned studies have explained about the role of FSST in the neurological disorders found in adults and not much in children. Till now as far as to our knowledge, there is one study available in children using FSST to estimate their dynamic balance in CTD[12] but not in special children group. In DS, child has difficulty in maintaining their line LOG within BOS. Thus children with DS have difficulty in maintaining balance. As there is a dearth of literature in FSST's validity and reliability in children with DS, we intend to explore it.
Methods
Participants
The 5 girls and 8 boys with DS were included for the cross section study. Their mean age was 12.76 ± 2.9 years, ranging from 8 to 17 years. The above sample was estimated from the online sample size estimation software for correlation program http://www.statstodo.com/SSizCorr_Pgm.php. The study protocol obtained ethical clearance (ACP/OP/2013/OL 03) from Alva's College of Physiotherapy Ethics Committee. Children who were able to comprehend and follow the instructions (as recent IQ data for individual children was not available, the former was adopted), independence in stance or ambulation, absence of congenital heart defects and with functional vision and hearing were recruited. Children with DS who had musculoskeletal injury within past 6 months, under medications or part of physiotherapy programme (may act as confounder in estimating reliability) and other health conditions which might prevent them from enrolling in the test were excluded. A simple random sampling was made by listing of children with DS from recognized special school by the software application tool, the random number generator. All the parents of the children were informed about the study and their consent was obtained. To avoid any bias, proper demonstration was given to each child and purpose, procedures, risks and benefits of the study was explained to them before data collection. It was ensured to them that the data collected would be confidential and it would be properly maintained. The test was conducted bare foot to avoid any possible error. Anthropometric measure was taken prior to the test.
Procedure
The subjects were asked to step in a pre-determined sequence over four 90 cm long sticks with flat base, placed in a cross configuration on the ground. The subject's starting position is in 1st square facing the 2nd square. The subjects were then asked to step forward to the right, backward to the left in to each square in the clockwise direction. Then the subjects were asked to do the same in anti-clockwise direction, as the sequence of stepping shown in Figure 1. Subjects both feet must make contact in each quadrant. The subjects were asked to complete the test as fast as possible without touching any sticks. The video illustrating the procedure can be accessed from http://youtube/v6JqJCo6e0k.
Figure 1.
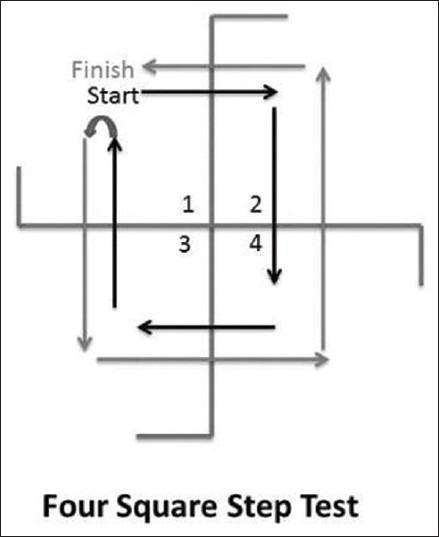
FSST sequence
The time taken to complete the test was recorded. The trial was considered a failure and repeated if the test was not completed correctly, that is, if the subject lost his or her balance, or a foot touched a stick. All the participants underwent practice trial until they became familiar with the procedure. The standardized assessment protocol with standardized instructions was followed to minimize bias between the investigators. The tests were only repeated to a maximum of twice if the participant failed during the 2nd and 3rd trials. Each subject performed 3 trials, as shown in Figure 2, with 1 min rest between trials to avoid fatigue. The test score were noted and mean of all the three trials were taken and used as the final score.
Figure 2.
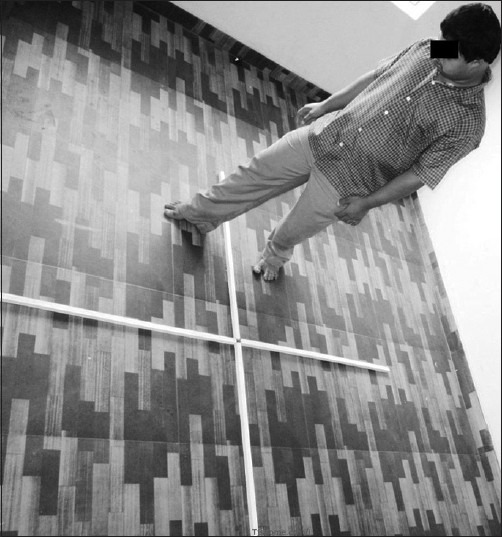
A children with Down's syndrome undergoing FSST. The sticks with 90 cm length are placed perpendicular to each other
Inter-rater reliability
The children with DS were asked to perform the second session with an interval of 7 days (as weekly once, the review of treatments were made in the special school) to estimate test-retest reliability by the second investigator. The second investigator is a registered qualified physiotherapist who had minimum 3 years’ experience in handling children.
Test-retest reliability
To evaluate test-retest reliability, the children were asked to perform one more session of FSST by the same principal investigator on the day of estimating inter-rater reliability. None of the children were absent for the second session after 7 days due to any discomfort or lack of interest. The time taken was noted by the principal investigator for analysis.
Concurrent validity
The performance of FSST was compared with the functional reach test (FRT) to establish the concurrent validity. All 13 children with DS were asked to undergo FRT. FRT was performed by using a measuring tape placed on the wall, parallel to the floor, at the height of the acromion of the subjects. The dominant arm was made closer to the wall at 90° of shoulder flexion with a closed fist. The subjects were asked to stand with feet apart. Then the subjects were asked to make a fist and flex forward with the dominant arm up to 90° and asked to reach forward as much as possible without taking a step or touching the wall. The head of the metacarpal of the third finger was used as the reference point. The start point and the end point were marked and the distance between these two points was measured. The scores of FRT was used as the criterion dynamic balance measure to determine validity with FSST.
Data analysis
The data were analysed by using statistical package for social sciences, version-20 (SPSS® 20.0 IBM®). To gain sufficient power for the data analysis we obtained sample of 13 children with DS with 0.05 alpha level and 80% power to detect minimum reliability coefficient of 0.75.[13] The normality of the collected data was established using Shapiro-Wilk Test and it was found to be that the data doesn’t follow normal distribution. Hence, we used non-parametric test. Descriptive statistics are reported as mean (95% CI) and range. Test-retest and inter-rater reliability were established using intra-class correlation coefficient (ICC). For test retest reliability, an ICC(1,1) (one-way random effect model) was used and for inter-rater analysis, an ICC(2,1) (two-way random effect model) was used in accordance with Shrout and Fleiss. According to them ICC interpretation <0.4 - poor, 0.4 to <0.75 - moderate, 0.75 to <0.9 - good, ≥0.9 - excellent.[14] The limits of agreement (LOA) were established as described by Bland and Altman. The Bland-Altman plots were used to display the level of agreement between repeated measures.[15] To find out the association between FSST and FRT, the Sperman rank correlation test was used.
Results
13 children with DS took part in the reliability study. None of them complained of pain or discomfort during the test. Demographics of the children recruited are displayed in Table 1. Here both males and females do not show any significant difference (P > 0.05) among their demographics. So, we can say that the boys and girls were matched in their age height and weight and this matching improves the quality of the study.
Table 1.
Demographic characteristics of male and female recruited and their characteristics were expressed as mean (95% CI)

Figures 3 and 4 shows test-retest and inter-rater variability of FSST scores among the children with DS. The ICC value of the repeated measures by the same investigator and inter-rater reliability of FSST are displayed in Table 2. According to Shrout and Fleiss criteria in estimating reliability, there is good reliability between them.
Figure 3.
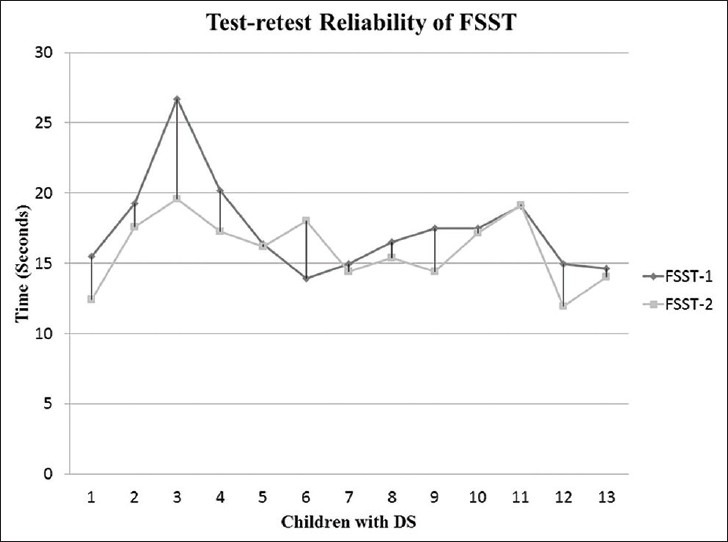
Test-retest agreement for the children with DS who participated in FSST
Figure 4.
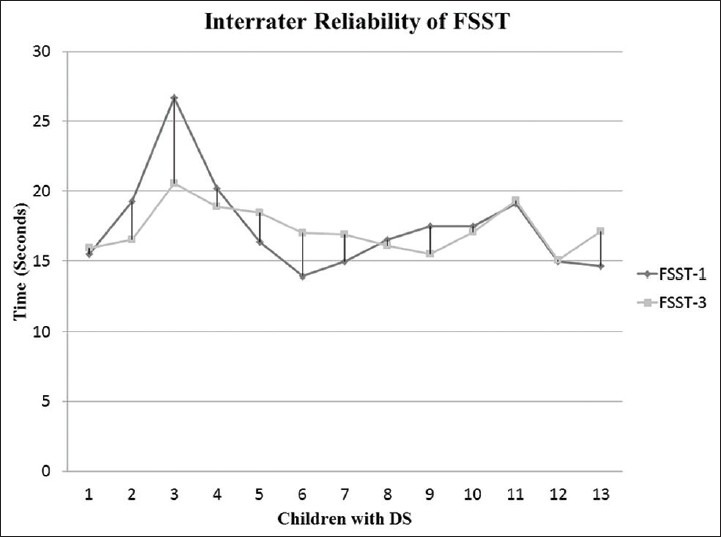
Inter-rater agreement for the children with DS who participated in FSST
Table 2.
Test-retest and interrater reliability of FSST and their intraclass correlation coefficients were expressed as mean (95% CI)
The Bland-Altman limits of agreement plots are included in Figures 5 and 6. The LOA between repeated measurement fall well within 2 SD. In both the figures, there is one outlier. Thus the agreement between measurements was satisfied.
Figure 5.
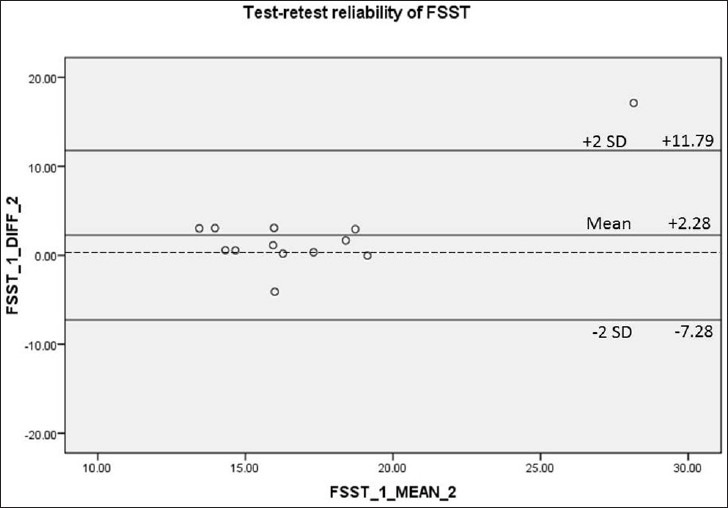
The Bland-Altman graph shows LOA of repeated measurements by the same investigator
Figure 6.
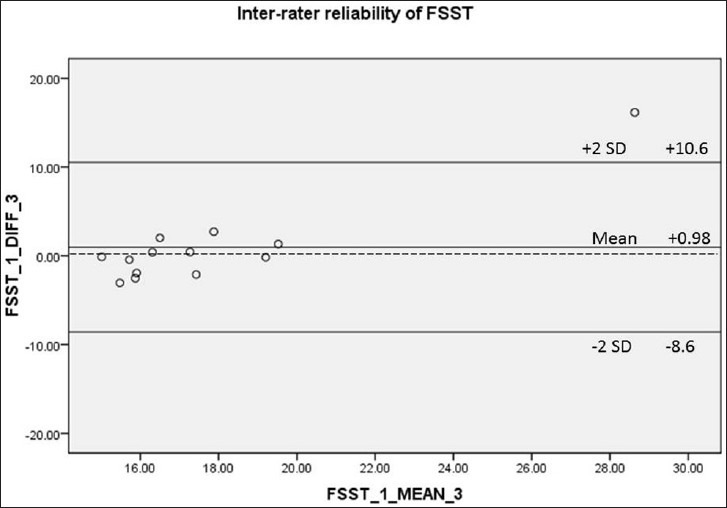
The Bland-Altman graph shows LOA of repeated measurements by the principal investigator and second investigator
The concurrent validity of FSST with the dynamic balance measure is displayed in Figure 7. According to Porteney and Watkins criteria in judging the relationship, there is moderate degree of inverse association between FRT and FSST with Mean Spearman's ρ −0.58 (P = 0.03).
Figure 7.
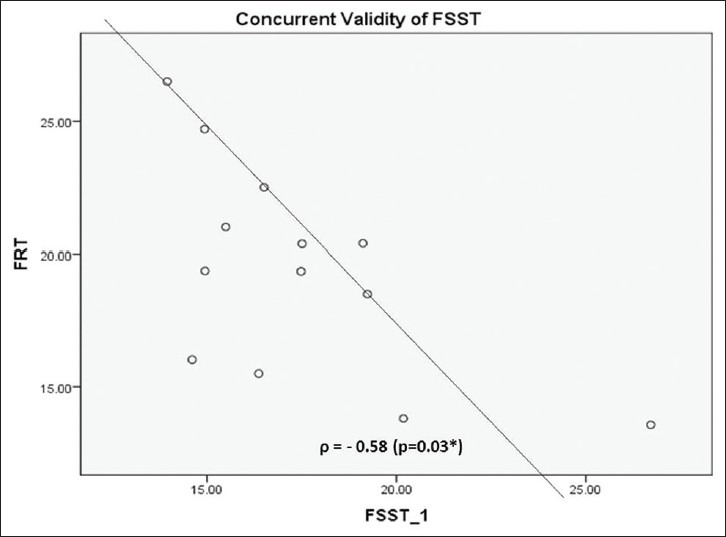
Correlation Scatter block between FRT and FSST. According Shrout and Fleiss JL criteria there is moderate degree of inverse association between FRT and FSST with Spearman's ρ-0.58 (P=0.03)
Discussion
Out of the total of 13 subjects who participated in this study, eight were boys and five were girls. The participants were in comfortable clothing and performed the test bare foot. Comfortable homely environment was provided for all the participants to make the test successful.[5] FSST is a convenient and feasible method to evaluate the dynamic balance in children with DS as the total time taken is <20 s and with easily available material. FSST in older adults was conducted by Dite and Temple[6] and the test was carried out for 15 s. Mean time taken by the participants was 8.70 (7.36–10.01) s. Again Dite along with Connor et al.[5] performed FSST on unilateral transtibial amputation subjects and the minimum time took by the subjects is 24 s.
Whitney et al.[8] performed FSST on people with balance deficits secondary to vestibular disorder and they took time more than 12 s (13.6 ± 4.3) to complete the test. Duncan and Earhart[11] has performed FSST in Parkinson's disease subjects and time taken was 9.52 s. On post stroke subjects, it was carried out in more than 15 s.[16] In CTD the time taken to complete the test is 9.3 ± 1.1 s.[12] But in this study the mean time taken by boys is 17.65 s and by girls is 16.42 s respectively. Hence, time taken were >15 s, the risk of fall is high among the children with DS.
The study by Goh et al.[5] shows good test-retest reliability of FSST with ICC (1,1) = 0.83 and inter-rater reliability ICC (2,1) = 0.99 in persons with chronic stroke subjects. From the data collected, for test-retest reliability, we obtained ICC (1,1) = 0.70 with principal investigator performed FSST twice on the subjects with an interval of 7 days. Similarly, for inter-rater reliability is ICC (2,1) = 0.78 with FSST administered by both, the principal investigator and second investigator on subjects with same interval. Thus FSST has good reliability among the children with DS.
Here we used FRT as the standard criterion measure in estimating the concurrent validity of FSST as it is the most convenient method and easy to perform. Moreover, it does not require large clinical setup and it can be easily demonstrated to the subject. It identifies the maximum distance a subject can reach forward without moving his/her feet and the distance covered correlates well with the dynamic balancing ability of an individual.[17]
According to Norris et al.[18] the normal value of FRT in the age group 3–5 years ranged between 5.2 and 22.7 cm and it was in the range of 19.7–32.2 cm for the normal children in age group 6-12 years from the report of Deshmuk et al.[19] For the children with TBI, the FRT ranged between 13.3 and 31.4 cm from the analysis done by Katz-Leurer et al.[20] But in our study the normal value of FRT for the children with DS ranged from 13.56 to 26.5 cm (19.35 ± 3.93). This is almost in line with the values of other study. We have taken the age group from 8 to 17 years as by this time the CNS of the children would have attained maturity. So, the disparity in balance due to the immaturity of CNS is prevented.
Tyson and DeSouza[21] reported that the correlation of FRT with the comparator test, r = 0.32–0.74 (P ≤ 0.05). But according to Volkman et al.[22] for children with typical development in the age group from 7 to 16 years is, r = 0.31. In TBI, Katz-Leurer et al.[20] reported the correlation of FRT was r = 0.71–0.92 (P ≤ 0.05). In our study we established the validity of FSST with the criterion dynamic balance test measure (FRT) to be ρ = −0.58 (P = 0.03). Thus FSST has an inverse moderate to good degree of association with the criterion balance measure. Hence FSST is a valid measure to estimate dynamic balance among the children with DS.
The IQ level of the children with DS and their cognitive ability who took part in the study may not be same. As FSST is cognitively demanding (remembering transfer sequence) the above might have affected their performance. We have not studied the effect of verbal instructions and encouragement provided by the different investigator. All the samples were recruited from one rehabilitation setting but the strength of the study is that samples were recruited by random sampling technique to minimize bias. The other factors which may affect their quality of performance such as muscle strength, level of fear of fall, lower limb proprioception and tactile sensation were not taken into consideration. Only the time taken to complete the test was given importance. The sample size might be small to detect the correlations between FSST and FRT. So, the present results study needs to be interpreted with caution. Future studies should consider the above aspect and should extend the study to the children with cerebral palsy, muscular dystrophy, etc., From our point of view, FSST is simple, feasible, and inexpensive for the rehabilitation of the children with DS in rural set up where advanced clinical measurements are not available.
Conclusion
FSST is a valid and reliable measure in estimating dynamic balance in children with DS aged between 8 and 17 years.
Acknowledgements
The authors are thankful to the children, their parents and the head of Chethana special school, Karkala, South India who gave their time and cooperation.
Footnotes
Source of Support: Transportation to the special school was provided by Alva's College of Physiotherapy, Moodabidri, Karnataka, India and authors were extremely grateful for the support provided. The cost for making four sticks, which were used in the study were sponsored by the first author, Dr. Ajai Verma.
Conflict of Interest: None declared.
References
- 1.WHO. Genes and human Diseases, Genes and Chromosomal Diseases, Down Syndrome. c2013. [Last updated on 2013 Mar 05, Last cited on 2013 Jun 23]. Available from: http://www.who.int/genomics/public/genticdiseases/en/index1.html .
- 2.Carvalho RL, Vasconcelos DA. Motor behavior in Down Syndrome: Atypical Sensoriomotor Control. In: Dey S, editor. Prenatal diagnosis and screening for Down syndrome. Ch. 3. Croatia: INTECH Rijeka; 2001. pp. 33–39. [Google Scholar]
- 3.Malak R, Kotwicka M, Krawczyk-Wasielewska A, Mojs E, Samborski W. Motor skills, cognitive development and balance functions of children with Down syndrome. Ann Agric Environ Med. 2013;20:803–6. [PubMed] [Google Scholar]
- 4.Villarroya MA, González-Agüero A, Moros-García T, de la Flor Marín M, Moreno LA, Casajús JA. Static standing balance in adolescents with Down syndrome. Res Dev Disabil. 2012;33:1294–300. doi: 10.1016/j.ridd.2012.02.017. [DOI] [PubMed] [Google Scholar]
- 5.Goh EY, Chua SY, Hong SJ, Ng SS. Reliability and concurrent validity of Four Square Step Test scores in subjects with chronic stroke: A pilot study. Arch Phys Med Rehabil. 2013;94:1306–11. doi: 10.1016/j.apmr.2013.01.027. [DOI] [PubMed] [Google Scholar]
- 6.Dite W, Temple VA. A clinical test of stepping and change of direction to identify multiple falling older adults. Arch Phys Med Rehabil. 2002;83:1566–71. doi: 10.1053/apmr.2002.35469. [DOI] [PubMed] [Google Scholar]
- 7.Dite W, Connor HJ, Curtis HC. Clinical identification of multiple fall risk early after unilateral transtibial amputation. Arch Phys Med Rehabil. 2007;88:109–14. doi: 10.1016/j.apmr.2006.10.015. [DOI] [PubMed] [Google Scholar]
- 8.Whitney SL, Marchetti GF, Morris LO, Sparto PJ. The reliability and validity of the Four Square Step Test for people with balance deficits secondary to a vestibular disorder. Arch Phys Med Rehabil. 2007;88:99–104. doi: 10.1016/j.apmr.2006.10.027. [DOI] [PubMed] [Google Scholar]
- 9.Nilsagård Y, Lundholm C, Denison E, Gunnarsson LG. Predicting accidental falls in people with multiple sclerosis – A longitudinal study. Clin Rehabil. 2009;23:259–69. doi: 10.1177/0269215508095087. [DOI] [PubMed] [Google Scholar]
- 10.Blennerhassett JM, Dite W, Ramage ER, Richmond ME. Changes in balance and walking from stroke rehabilitation to the community: A follow-up observational study. Arch Phys Med Rehabil. 2012;93:1782–7. doi: 10.1016/j.apmr.2012.04.005. [DOI] [PubMed] [Google Scholar]
- 11.Duncan RP, Earhart GM. Four square step test performance in people with Parkinson disease. J Neurol Phys Ther. 2013;37:2–8. doi: 10.1097/NPT.0b013e31827f0d7a. [DOI] [PubMed] [Google Scholar]
- 12.Salis JS, Samuel AJ. Paper Presented at: Physioaccord 2014-National Physiotherapy Conference. Bangalore, India: 2014. Jan, Four Square Step Test in Children with Typical Development: Test-Retest and Inter Rater Reliability-A Pilot Study; pp. 17–18. [Google Scholar]
- 13.Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliability studies. Stat Med. 1998;17:101–10. doi: 10.1002/(sici)1097-0258(19980115)17:1<101::aid-sim727>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 14.Shrout PE, Fleiss JL. Intraclass correlations: Uses in assessing rater reliability. Psychol Bull. 1979;86:420–8. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- 15.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–10. [PubMed] [Google Scholar]
- 16.Blennerhassett JM, Jayalath VM. The Four Square Step Test is a feasible and valid clinical test of dynamic standing balance for use in ambulant people poststroke. Arch Phys Med Rehabil. 2008;89:2156–61. doi: 10.1016/j.apmr.2008.05.012. [DOI] [PubMed] [Google Scholar]
- 17.Duncan PW, Weiner DK, Chandler J, Studenski S. Functional reach: A new clinical measure of balance. J Gerontol. 1990;45:M192–7. doi: 10.1093/geronj/45.6.m192. [DOI] [PubMed] [Google Scholar]
- 18.Norris RA, Wilder E, Norton J. The functional reach test in 3- to 5-year-old children without disabilities. Pediatr Phys Ther. 2008;20:47–52. doi: 10.1097/PEP.0b013e31815ce63f. [DOI] [PubMed] [Google Scholar]
- 19.Deshmukh AA, Ganesan S, Tedla JS. Normal values of functional reach and lateral reach tests in Indian school children. Pediatr Phys Ther. 2011;23:23–30. doi: 10.1097/PEP.0b013e3182099192. [DOI] [PubMed] [Google Scholar]
- 20.Katz-Leurer M, Rotem H, Lewitus H, Keren O, Meyer S. Functional balance tests for children with traumatic brain injury: Within-session reliability. Pediatr Phys Ther. 2008;20:254–8. doi: 10.1097/PEP.0b013e3181820dd8. [DOI] [PubMed] [Google Scholar]
- 21.Tyson SF, DeSouza LH. Reliability and validity of functional balance tests post stroke. Clin Rehabil. 2004;18:916–23. doi: 10.1191/0269215504cr821oa. [DOI] [PubMed] [Google Scholar]
- 22.Volkman KG, Stergiou N, Stuberg W, Blanke D, Stoner J. Methods to improve the reliability of the functional reach test in children and adolescents with typical development. Pediatr Phys Ther. 2007;19:20–7. doi: 10.1097/01.pep.0000247173.14969.5a. [DOI] [PubMed] [Google Scholar]