

Abstract
Objective
The aim of this study was to compare midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor between pregnant women who subsequently developed preeclampsia and those who did not.
Methods
Midtrimester maternal plasma was collected and stored at -70℃ when genetic amniocentesis was performed. Cases included 37 samples of individual who subsequently developed preeclampsia, and matched controls were from individuals who did not develop preeclampsia. Angiopoietin 1, angiopoietin 2, and placental growth factor concentrations were measured by the enzyme-linked immunosorbent assay method and were compared using the Mann-Whitney U-test. A P-value <0.05 was considered significant.
Results
In pregnant women who subsequently developed preeclampsia, midtrimester maternal plasma concentrations of angiopoietin 1 and angiopoietin 2 were significantly higher and placental growth factor concentrations were significantly lower than in women who did not develop preeclampsia (angiopoietin 1: 10.6 [3.1-19.7] vs. 7.8 [0.9-24.4] ng/mL, P=0.031; angiopoietin 2: 31.0 [4.7-81.2] vs. 18.4 [4.2-49.7] ng/mL, P<0.001; placental growth factor: 87.1 [14.2-774.3] vs. 148.8 [57.2-425.6] pg/mL, P<0.001). Within the case group who subsequently developed preeclampsia, the placental growth factor was significantly lower in those who had fetal growth restrictions than in those who did not (placental growth factor: 72.5 [14.2-774.3] vs. 140.9 [44.2-257.5] pg/mL, P=0.003).
Conclusion
Midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor may be associated with the subsequent development of preeclampsia.
Keywords: Angiopoietin, placental growth factor, preeclampsia, pregnancy, maternal plasma
Introduction
Preeclampsia complicates approximately 5% of pregnancies and constitutes a major cause of maternal and neonatal morbidity and mortality. Preeclampsia is diagnosed as the occurrence of hypertension and proteinuria after 20 weeks of gestation. It causes endothelial dysfunction (characterized by vasospasm and increased vascular permeability) that affects almost all organ systems [1,2].
The etiology of preeclampsia is not well understood. It is known than preeclampsia is associated with poor vascular formation of the placenta and decidua. Currently, some angiogenic factors derived from placental tissue are considered to be candidate molecules that cause preeclampsia [3,4]. Soluble fms-like tyrosine kinase-1 (sFlt-1) is one of these molecules. Its maternal level is elevated in preeclamptic women, and it is known to be elevated well before the onset of the disease [5,6]. The placental growth factor level is known to be reduced in patients who develop preeclampsia [5]. These changes are thought to affect angiogenesis concerning placental development through the alteration of VEGF activity.
Angiopoietin/Tie 2 is another system that is involved in the regulation of angiogenesis [7]. Angiopoietin 1 is a ligand that binds to Tie 2 receptor, leading to the stabilization of the vessel wall and reduction of vascular permeability. Angiopoietin 2 is a competitive inhibitor of angiopoietin 1, and it interferes with the stabilizing action of angiopoietin 1.
The objective of this study was to compare the midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2 and placental growth factor between pregnant women who subsequently developed preeclampsia and those who did not.
Materials and methods
1. Study design
Maternal plasma was obtained from women who underwent midtrimester genetic amniocentesis between October 1998 and November 2005 at Seoul National University Hospital. Samples were collected in ethylene diamine tetraacetic acid tubes, centrifuged, and stored at -70℃ until assayed. The cases consisted of 37 women who subsequently developed preeclampsia. The control subjects who delivered at term without developing preeclampsia were matched for maternal age (≤ 5 years), gestational age at sampling (≤ 2 weeks), and year of sampling (≤ 3 years). Parity (nullipara or not) was matched for most cases. Preeclampsia was diagnosed by hypertension (blood pressure 140/90 mmHg) and proteinuria (300 mg/24 hr or dipstick 1+). Fetal growth restriction (FGR) was defined as a birth weight below the 10th percentile. Preeclampsia was labeled to be severe if one or more of the following criteria were met: diastolic blood pressure ≥110 mmHg, proteinuria ≥2 g/24 hr, persistent headache, visual disturbances, oliguria, convulsion, serum creatinine elevation, thrombocytopenia, marked liver enzyme elevation, FGR, or pulmonary edema. Informed consent was obtained from all patients. The institutional review board of Seoul National University Hospital approved the collection of samples and clinical information for research purposes.
2. Measurement of angiopoietin 1, angiopoietin 2, and placental growth factor
Concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor were measured by commercially available enzyme-linked immunosorbent assay kits (R&D Systems, Minneapolis, MN, USA). The minimum detectable dose was <10.3 pg/mL (for angiopoietin 1), <21.3 pg/mL (for angiopoietin 2), <7 pg/mL (for placental growth factor), respectively. The intra- and inter-assay coefficients of variation were <3.4% and <6.8% (for angiopoietin 1), <6.9% and <10.4% (for angiopoietin 2), and <7.0% and <11.8% (for placental growth factor).
3. Statistical analysis
The Mann-Whitney U-test was used to compare continuous variables, and Fisher's exact test was used for proportions. A P-value <0.05 was considered significant.
Results
Table 1 shows the clinical characteristics of the study population. There were no statistically significant differences in the maternal age, parity, and gestational age at sampling. The gestational age at the time of sampling ranged from 15.9 to 23.1 weeks of gestation. The gestational age at birth and birth weight were significantly lower in the preeclampsia group than in the control group. The proportion of FGR was higher in the preeclampsia group than in the control group (19/37 [51%] vs 1/37 [3%], P<0.001).
Table 1.
Characteristics and midtrimester maternal plasma concentrations
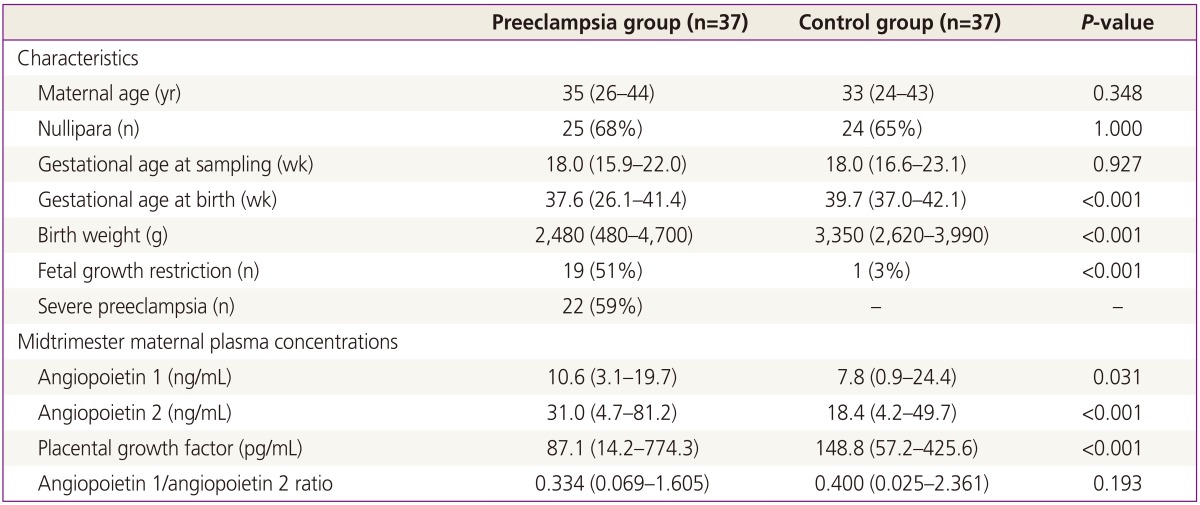
Data were represented as median and range or number (%).
Table 1 and Fig. 1 shows the midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor in the preeclampsia group and control group. Midtrimester maternal plasma concentrations of angiopoietin 1 and angiopoietin 2 were significantly higher in patients who subsequently developed preeclampsia than those who did not, while placental growth factor concentrations were significantly lower in the preeclampsia group than in the control group (angiopoietin 1: 10.6 [3.1-19.7] vs. 7.8 [0.9-24.4] ng/mL, P=0.031; angiopoietin 2: 31.0 [4.7-81.2] vs. 18.4 [4.2-49.7] ng/mL, P<0.001; placental growth factor: 87.1 [14.2-774.3] vs. 148.8 [57.2-425.6] pg/mL, P<0.001). The angiopoietin 1/angiopoietin 2 ratio was not significantly different between the preeclampsia and control groups (0.334 [0.069-1.605] vs. 0.400 [0.025-2.361], P=0.193).
Fig. 1.

Midtrimester maternal plasma concentrations of angiopoietin 1 (A), angiopoietin 2 (B), placental growth factor (C), and angiopoietin 1/angiopoietin 2 ratio (D) in patients who subsequently developed preeclampsia and controls. In pregnant women who subsequently developed preeclampsia, midtrimester maternal plasma concentrations of angiopoietin 1 and angiopoietin 2 were significantly higher and placental growth factor concentrations were significantly lower than those who did not develop preeclampsia. NS, non-significant.
Table 2 shows the subgroup data according to the presence of FGR at birth within the case group of women who subsequently developed preeclampsia. Midtrimester maternal plasma concentrations of placental growth factor were significantly lower in the FGR group than in the no FGR group (placental growth factor: 72.5 [14.2-774.3] vs. 140.9 [44.2-257.5] pg/mL, P=0.003). Angiopoietin 1 and angiopoietin 2 concentrations and the angiopoietin 1/angiopoietin 2 ratio were not significantly different between the two groups, but there was a tendency of higher concentrations of angiopoietin 2 in the no FGR group (P=0.078).
Table 2.
Subgroup data according to the presence of fetal growth restriction at birth within the preeclampsia
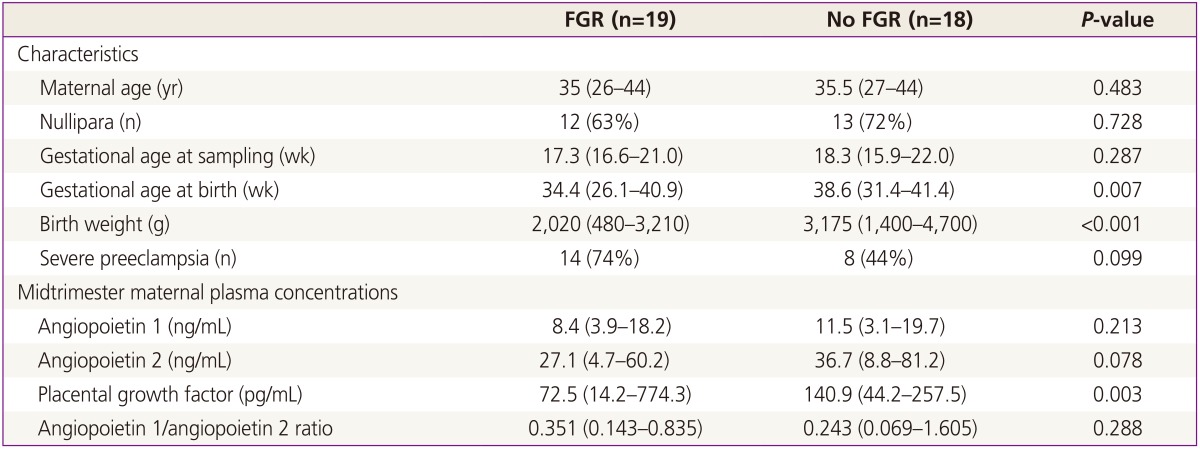
Data were represented as median and range or number (%).
FGR, fetal growth restriction.
Table 3 shows the subgroup data according to the severity of preeclampsia within the case group of women who subsequently developed preeclampsia. Midtrimester maternal plasma concentrations of placental growth factor were significantly lower in the severe preeclampsia group than in the mild preeclampsia group (placental growth factor: 70.2 [14.2-257.5] vs 122.4 [57.9-774.3] pg/mL, P=0.033). This difference may be linked to a tendency of a higher proportion of FGR in the severe preeclampsia group. Angiopoietin 1 and angiopoietin 2 concentrations, and the angiopoietin 1/angiopoietin 2 ratio were not significantly different between the two groups.
Table 3.
Subgroup data according to the severity of preeclampsia within the preeclampsia
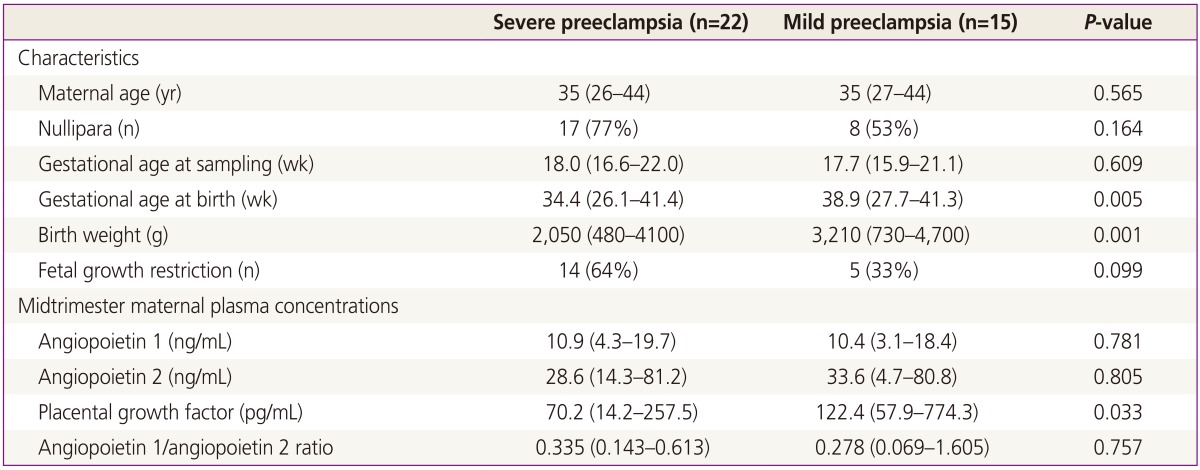
Data were represented as median and range or number (%).
Discussion
This study shows that, in pregnant women who subsequently developed preeclampsia, midtrimester maternal plasma concentrations of angiopoietin 1 and angiopoietin 2 were significantly higher and placental growth factor concentrations were significantly lower than in women who did not develop preeclampsia.
The change of placental growth factor level seems to agree with the previous reports [5,8], but it appears that the change of angiopoietin levels is not well established yet. It has been reported that patients with clinical manifestations of preeclampsia had an increased concentration of maternal plasma angiopoietin 1 [9]. Leinonen et al. [10] examined angiopoietin levels before the onset of the clinical manifestation of preeclampsia. They reported that at 12 to 15 weeks of gestation, maternal serum concentrations of angiopoietin 1 were higher in women who later developed preeclampsia with concomitant intrauterine growth restriction compared with control subjects, but they did not show a statistically significant increase at 16 to 20 weeks of gestation. Our data showed that at approximately 16 to 23 weeks, maternal plasma concentrations of angiopoietin 1 were significantly higher in patients who subsequently developed preeclampsia than in control subjects.
Placental mRNA expression of angiopoietin 2 is high during the first trimester, but decreases as gestation advances [11,12]. Placental angiopoietin 2 expression is decreased in preeclamptic women. The placenta is considered to be the main source of maternal circulating angiopoietin 2. Hirokoshi et al. [13] and Hirokoshi et al. [14] reported significantly lower levels of serum angiopoietin 2 in women with clinical manifestations of preeclampsia than in healthy pregnant women. Our data shows higher levels of midtrimester maternal plasma angiopoietin 2 in women who subsequently develop preeclampsia than in those who did not. Hirokoshi's data were from 3rd trimester samples after the onset of preeclampsia, while our data were from 2nd trimester samples from women who did not yet show the clinical features of preeclampsia. Leinonen et al. [10] reported that at 16 to 20 weeks, angiopoietin 2 concentrations were higher in women with subsequent preeclampsia than in control subjects, which is in agreement with our data.
Bolin et al. [15] showed that the angiopoietin 1/angiopoietin 2 ratio was significantly lower during gestational weeks 25 and 28 in women who later developed preeclampsia than in normal pregnant women. Our data showed a similar tendency, but did not reach statistical significance.
Wang et al. [16] reported that the maternal serum concentrations of angiopoietin-2 during 10 to 13 weeks of gestation were lower in patients who subsequently developed severe intrauterine growth restriction compared with normal pregnant control subjects. The gestational age at sampling of their study was earlier than that of ours. In addition, they examined the women who subsequently developed a FGR, but we should also pay attention to their study because fetal growth restriction and preeclampsia might share some common etiology with respect to placental development and angiogenesis [8]. However, when we subdivided our preeclampsia group into FGR and no FGR groups (Table 2), our data showed that angiopoietin 2 levels were elevated in both groups, especially in the no FGR group. This discrepancy may be due to the presence of preeclampsia in our study and the difference of gestational age at sampling.
Our study has several limitations. First, it has a small study population. Some of the analyses may not have enough power to demonstrate the statistical significance. Second, there was a lack of information on some confounding factors. Schneuer et al. [17] showed that maternal age, weight, country of birth, and socioeconomic status significantly affected angiopoietin 1, angiopoietin 2, and the angiopoietin1/angiopoietin 2 ratio, but our matching parameters could not include all of these points.
The role of angiopoietins in the development of preeclampsia is not well known. Multiple systems might be interconnected with respect to the development of preeclampsia. Indeed, the action of angiopoietin 2 is different depending on the presence of VEGF. In the absence of VEGF, angiopoietin 2 causes vascular regression, but in the presence of VEGF, angiopoietin 2 can stimulate angiogenesis [18].
In conclusion, the midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor may be associated with the subsequent development of preeclampsia. We expect that further studies on the angiogenic factors may result in better understanding of the etiology of preeclampsia.
Acknowledgments
This work was supported by grant no. 03-2006-0250 from Seoul National University Hospital Research Fund.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.ACOG Committee on Obstetric Practice. ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 2002;77:67–75. [PubMed] [Google Scholar]
- 2.Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365:785–799. doi: 10.1016/S0140-6736(05)17987-2. [DOI] [PubMed] [Google Scholar]
- 3.Erez O, Romero R, Espinoza J, Fu W, Todem D, Kusanovic JP, et al. The change in concentrations of angiogenic and antiangiogenic factors in maternal plasma between the first and second trimesters in risk assessment for the subsequent development of preeclampsia and small-for-gestational age. J Matern Fetal Neonatal Med. 2008;21:279–287. doi: 10.1080/14767050802034545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, et al. Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003;111:649–658. doi: 10.1172/JCI17189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350:672–683. doi: 10.1056/NEJMoa031884. [DOI] [PubMed] [Google Scholar]
- 6.Park CW, Park JS, Shim SS, Jun JK, Yoon BH, Romero R. An elevated maternal plasma, but not amniotic fluid, soluble fms-like tyrosine kinase-1 (sFlt-1) at the time of mid-trimester genetic amniocentesis is a risk factor for preeclampsia. Am J Obstet Gynecol. 2005;193(3 Pt 2):984–989. doi: 10.1016/j.ajog.2005.06.033. [DOI] [PubMed] [Google Scholar]
- 7.Karamysheva AF. Mechanisms of angiogenesis. Biochemistry (Mosc) 2008;73:751–762. doi: 10.1134/s0006297908070031. [DOI] [PubMed] [Google Scholar]
- 8.Romero R, Nien JK, Espinoza J, Todem D, Fu W, Chung H, et al. A longitudinal study of angiogenic (placental growth factor) and anti-angiogenic (soluble endoglin and soluble vascular endothelial growth factor receptor-1) factors in normal pregnancy and patients destined to develop preeclampsia and deliver a small for gestational age neonate. J Matern Fetal Neonatal Med. 2008;21:9–23. doi: 10.1080/14767050701830480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nadar SK, Karalis I, Al Yemeni E, Blann AD, Lip GY. Plasma markers of angiogenesis in pregnancy induced hypertension. Thromb Haemost. 2005;94:1071–1076. doi: 10.1160/TH05-03-0167. [DOI] [PubMed] [Google Scholar]
- 10.Leinonen E, Wathen KA, Alfthan H, Ylikorkala O, Andersson S, Stenman UH, et al. Maternal serum angiopoietin-1 and -2 and tie-2 in early pregnancy ending in preeclampsia or intrauterine growth retardation. J Clin Endocrinol Metab. 2010;95:126–133. doi: 10.1210/jc.2009-0715. [DOI] [PubMed] [Google Scholar]
- 11.Geva E, Ginzinger DG, Zaloudek CJ, Moore DH, Byrne A, Jaffe RB. Human placental vascular development: vasculogenic and angiogenic (branching and nonbranching) transformation is regulated by vascular endothelial growth factor-A, angiopoietin-1, and angiopoietin-2. J Clin Endocrinol Metab. 2002;87:4213–4224. doi: 10.1210/jc.2002-020195. [DOI] [PubMed] [Google Scholar]
- 12.Zhang EG, Smith SK, Baker PN, Charnock-Jones DS. The regulation and localization of angiopoietin-1, -2, and their receptor Tie2 in normal and pathologic human placentae. Mol Med. 2001;7:624–635. [PMC free article] [PubMed] [Google Scholar]
- 13.Hirokoshi K, Maeshima Y, Kobayashi K, Matsuura E, Sugiyama H, Yamasaki Y, et al. Increase of serum angiopoietin-2 during pregnancy is suppressed in women with preeclampsia. Am J Hypertens. 2005;18(9 Pt 1):1181–1188. doi: 10.1016/j.amjhyper.2005.03.745. [DOI] [PubMed] [Google Scholar]
- 14.Hirokoshi K, Maeshima Y, Kobayashi K, Matsuura E, Sugiyama H, Yamasaki Y, et al. Elevated serum sFlt-1/Ang-2 ratio in women with preeclampsia. Nephron Clin Pract. 2007;106:c43–c50. doi: 10.1159/000101483. [DOI] [PubMed] [Google Scholar]
- 15.Bolin M, Wiberg-Itzel E, Wikstrom AK, Goop M, Larsson A, Olovsson M, et al. Angiopoietin-1/angiopoietin-2 ratio for prediction of preeclampsia. Am J Hypertens. 2009;22:891–895. doi: 10.1038/ajh.2009.97. [DOI] [PubMed] [Google Scholar]
- 16.Wang Y, Tasevski V, Wallace EM, Gallery ED, Morris JM. Reduced maternal serum concentrations of angiopoietin-2 in the first trimester precede intrauterine growth restriction associated with placental insufficiency. BJOG. 2007;114:1427–1431. doi: 10.1111/j.1471-0528.2007.01511.x. [DOI] [PubMed] [Google Scholar]
- 17.Schneuer FJ, Roberts CL, Ashton AW, Guilbert C, Tasevski V, Morris JM, et al. Angiopoietin 1 and 2 serum concentrations in first trimester of pregnancy as biomarkers of adverse pregnancy outcomes. Am J Obstet Gynecol. 2014;210:345.e1–345.e9. doi: 10.1016/j.ajog.2013.11.012. [DOI] [PubMed] [Google Scholar]
- 18.Maisonpierre PC, Suri C, Jones PF, Bartunkova S, Wiegand SJ, Radziejewski C, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science. 1997;277:55–60. doi: 10.1126/science.277.5322.55. [DOI] [PubMed] [Google Scholar]