

Abstract
Much like other racial/ethnic groups, Latinos are facing challenges to provide needed care to aging adults. Older Latinos underutilize nursing homes and home health care services and primarily rely on their families for assistance. While this general trend has been established, little attention has been paid to nativity differentials in patterns of caregiving for this segment of the aging population. The analyses are based on the latest wave (Wave 7) of the Hispanic Established Population for Epidemiologic Studies of the Elderly or H-EPESE (2010/2011) a sample of older Mexican-origin adults and their family caregivers living in the southwestern U.S. We examine 629 child caregiver/parent care recipient dyads using bivariate statistics and multinomial logistic regression analyses. The results reveal that while grown children of Mexican-origin elders play a critical role in providing instrumental and financial supports to their aging parents, the burden that the children of foreign-born parents bear is greater. Despite higher rates of disability, Mexican-born elders are more dependent on a child for help and far less likely to call upon other family members, relatives and community based-providers for help than the U.S. born. Given the recent and future growth in this segment of the aging population, intervention strategies will need to focus on nativity status and acculturative processes in the context of caregiving and caregiver burden.
Keywords: Latinos, Late-Life Family Caregiving, Mexican-origin Population in the United States, Nativity
Introduction
As a result of high immigration and improvements in life expectancy, the older population in the United States is expected to grow more diverse, with the steepest growth in older Latinos. Latinos 65 years and over accounted for 7 percent of the older population in 2010 and will increase to 20 percent over the next thirty years. The number of older Latinos will grow by more than six times, from 3 million to 17.5 million and outnumber older African Americans (Vincent & Velkof, 2010). The oldest and by far the largest segment of the Latino population in the United States are of Mexican heritage, accounting for almost two-thirds of all Latinos. In addition, individuals of Mexican origin represent the largest segment of the elderly Latino population (U.S. Census Bureau, 2012). There are no national data on rates of caregiving by Latino subgroup but it has been suggested that there are higher rates of caregiving among Mexican Americans than in the general population because of higher disability rates and dementia and lower tendency to institutionalize older family members (Gaugler, Kane, A., & Newcomer, 2006; Markides, Eschach, Ray, & Peek, 2007) Villa & Aranda, 2000).
At the same time, Latinos of Mexican-origin enter the later years of life with substantially fewer financial resources, including pensions and housing assets, than non-Latino whites. Approximately one-quarter of Latino elders live below the poverty line, more than double the rate of non-Latino adults 65 and over (DeNavas, Proctor, & Smith, 2011). In 2010, Latinos were half as likely as non-Latino white elderly households to have income from a private retirement plan (39% versus 72%); and rates were especially low among Mexican-origin households (15%). Forty percent of Latinos must rely solely on Social Security for their income support (Ronald J. Angel & Angel, 2009). The fact that many Mexican-origin parents have few economic resources and a high risk of disability represents a serious potential dependency burden for adult children (Gassoumis, Wilber, Baker, & Torres-Gil, 2010).
Mexican-origin elders also tend to underutilize formal caregiving services (Crist, Garcıa-Smith, & Phillips, 2006; A. P. Herrera, Benson, Angel, Markides, & Torres-Gil, 2013), including nursing homes and other long-term private-pay care facilities, even when they suffer a significant decline in functional capacity (Espino, Angel, Wood, Finely, & Ye, 2013). This pattern of remaining in the community even with serious functional limitations may reflect individual and family preferences and culture, or the inability to pay for formal long-term care (J. L. Angel, Angel, McClellan, & Markides, 1996). However, recent shifts in traditional family arrangements and female workforce participation indicate that as older parents become seriously impaired families will require new care arrangements and an increased use of formal services. There is a large body of literature on the emotional and psychological burdens of caregiving (Crist, Woo, & Choi, 2007; Cucciare, Gray, Azar, Jimenez, & Gallagher-Thompson, 2010; A. P. Herrera, Lee, Palos, & Torres-Vigil, 2008; Villa & Aranda, 2000; Werner, Mittelman, Goldstein, & Heinik, 2012; Zarit & Reamy, 2012). Our study adds to a growing understanding of the motivations, rewards, and difficulties faced by the adult children of infirm or incapacitated older Mexican-origin parents. The characterization of this population as traditional, conservative, and familistic may reflect little more than caricature. Below, we first review research on factors that influence support systems in the older Mexican-origin population. Then, we describe our conceptual framework and pay particular attention to the role of nativity status.
Support Systems in the Late Life
Close relationships, such as those between family members and close friends, can vary in terms of intimacy, support, and information and can have a positive effect on the lives of older adults, particularly when they are in their eighties (Umberson & Montez, 2010). When an older person needs money for food or some other immediate assistance, he or she usually calls upon a close family member or friend (Umberson & Montez, 2010). In general, such close relationships are the only sources to which an older adult has access in times of crisis and in the event they need assistance with basic activities of daily living (Dilworth-Anderson, Williams, & Gibson, 2002; Taylor & Chatters, 1986).
For older adults with good health and adequate income, later life can be truly golden, but for those with limited resources who face long periods of disability, old age can represent a serious burden for their families. Older individuals with adequate resources can help educate grandchildren and assist their adult children in buying homes, starting businesses, or weathering financial setbacks. Such an ideal retirement is rarer for Mexican-origin elders than for non-Latino white elders. Many people of Mexican-origin spend their working lives in low-paying jobs that do not allow them to save for retirement (Kochhar, 2005). Only 31.5 percent of Mexican-origin workers participate in an employer-sponsored retirement plan, and very few have substantial retirement savings (Ronald J. Angel & Angel, 2009). Even those who are eligible for Social Security often receive low benefits because of low contributions (Orszag & Rodriguez, 2005). Consequently, among the poor with few assets, the elderly of Mexican ancestry have few options other than to turn to children or Medicaid and Supplemental Security Income (SSI) programs for assistance (Carmel, Morse, & Torres-Gil, 2007).
Mexican-Origin Families, Demographic Shifts, and Caregiving
Latino family members currently provide nearly eighty percent of long-term care that is provided in the home or community, a higher percentage than for African-Americans and non-Latino whites (Torres-Gil, Greenstein, & Kamin, 2005). According to the National Alliance of Caregiving, there are over eight million Latino caregivers in the United States (Evercare, 2008). One out of every three Latino households reports that at least one family member provides care to an older person (Evercare, 2008). Previous research and anecdotal evidence reveal a pattern that is typical of all burdensome responsibilities: the responsibility for supporting and caring for elderly parents is often shared unequally shared among family members (Connidis, 2007; Connidis & Kemp, 2008). In most cases the responsibility for the care of Latino aging parents and parents-in-law falls to daughters (A. Herrera, Angel, Venegas, & Angel, 2012). Such inequity in responsibility and burden can cause serious family strife (Markides & Black, 1995; Markides, Peek, & Angel, 2013).
Additionally, Mexican-origin families are undergoing changes that will affect their ability to continue providing emotional and instrumental support to elderly functionally impaired parents. The movement away from traditional family arrangements that results from smaller families, the need for women to enter the labor force, international migration, and other socio-demographic forces invariably alters the norms and practices that surround intergenerational relations and intra-familial exchanges (Lee & Mason, 2011). For example, the protracted economic recession that began in 2008 undoubtedly has exacerbated the problems that families face in their attempts to care for dependent parents. This is perhaps especially true for Mexican-origin families that suffered disproportionately high levels of unemployment, foreclosures, and the depletion of savings (Tavernise, 2011). These factors have the potential to disrupt traditional support networks and undermine their support capacity (Massey, 2011; Wong & Espinoza, 2007), and make caring for aging parents more difficult (United States Department of Labor, 2012). Financial uncertainty, in addition to other institutionalized disadvantages, including the responsibility for children and adult children's own living expenses, means that older Mexican-origin adults often have no choice but to turn to their families in order to age in the community with some degree of dignity and comfort.
Previous research on racial/ethnic differences in caregiving finds that Latinos tend to report more demanding care situations than non-Latino white and African American caregivers (Evercare, 2008). Most research has focused on caregiver burden and psychological distress or the role of cultural factors like familism (Aranda & Knight 1999; Crist et al. 2007; Hernandez & Bigatti 2010; Hahn et al. 2011; Sayegh & Knight 2011). A recent study using this sample found that lower income Mexican-origin caregivers report more psychological distress than their higher income counterparts (blind citation).
The Current Study
This study will describe the role of nativity status on types of assistance (self-care, household, and financial) that adult children provide to their infirm older Mexican-origin parents. We employ data from the most recent wave of a 17-year cohort study of elderly Mexican-origin adults eighty-five years and older. We focus on various family, cultural, social, and economic factors that allow functionally impaired older Mexican-origin adults to remain in the community.
Although individuals from traditional cultures may retain a cultural orientation that increases the likelihood that they will assume a major role in the care of older parents, our model is based on the assumption that basic economic and material factors are equally, if not more, important. More specifically, the immigration experience is likely to be associated with structural factors such as residential location, family demographics, and the local availability of formal care. Figure 1 displays a conceptual model delineating some of the material and cultural factors that are hypothesized to mediate the association between nativity status and dependency on one caregiver among older Mexican origin adults. The first three steps (i.e., paths “a” “b”) are mostly descriptive and the focus of the current investigation. If supported, we also test whether path “a,” nativity status differences in dependency are attenuated when controlling for the proposed mediators. This conceptual model was created to guide future explanatory research on nativity status and caregiving.
Figure 1. A Heuristic Schematic of the Potential Associations Among Exogenous and Endogenous Variables.
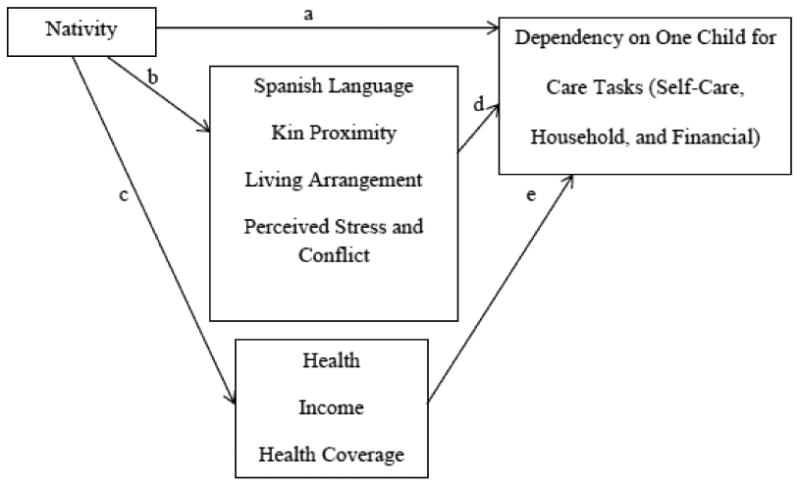
Earlier work using these data indicates foreign-born elderly individuals of Mexican origin often have greater difficulty adapting to the host culture and are less likely than the U.S. born to become self-sufficient (Ronald J Angel, Angel, Lee, & Markides, 1999). Mexican-born elderly are more likely than the U.S. born to lack English language proficiency, more likely to reside with their caregiver, more likely to suffer from disability and cognitive impairment, and less likely to have access to Medicare-supported home health care, private-pay personal care services, and to possess the skills necessary to navigate the spectrum of available care. Given the fact that Mexican-born parents are also less likely to have been able to save for retirement, they are likely to have little choice but to rely on a focal adult child for care and support (Ronald J. Angel & Angel, 2009). The U.S. born, on the other hand, are more likely than the Mexican-born elders to be culturally assimilated and they may be able to rely on other family members and professional or formal services, such as home-health care agency or an accountant for assistance with taxes and money management, and, therefore, are less likely to report high levels of perceived stress and conflict. Given greater resources and perhaps a greater familiarity among adult children with those options, U.S-born adults with serious impairments may be more likely than Mexican born impaired adults to call upon these sources of care and support.
These considerations lead us to the following expectations:
Mexican-born care recipients will be more dependent on an adult child than U.S. born care recipients. They will be more likely to live with children and to receive material and instrumental support from them.
Mexican born care recipients and their families are more likely than their U.S.-born counterparts to experience stressful life circumstances, lack health care coverage and financial resources, and suffer from disease and disability.
Subjects and Methods
Data come from the Hispanic Established Population for Epidemiologic Studies of the Elderly or H-EPESE) (Markides, Rudkin, Angel, et al., 1997). The H-EPESE is the first longitudinal investigation of the health and care experiences of a large multi-stage, probability sample of older individuals of Mexican origin in five states: Texas, California, New Mexico, Arizona, and Colorado. This sampling strategy makes it possible to generalize the results to the population 65 and older of Mexican-origin residing in the Southwest (J. L. Angel & Angel, 1998). The baseline cohort of 3,050, aged 65 and older were surveyed in their homes in 1993-94 by raters who received 20 hours of training and reinterviewed in 1995-96, 1998–99, 2000–01, 2004–05, 2006-07, and in 2010-11 for a total of seven observation waves. The baseline response rate was 86%, and respondents had the option of taking the interviews in Spanish or English. At wave five, 902 new subjects aged 75 and older were added to the cohort.
The 2010/2011 survey (Wave 7) includes data on 1,078 respondents ages 82 and over. Interviewers asked the older adult to provide the name and contact information of a person close to them that they could rely on for help and 925 individuals (i.e., informants) familiar with the elderly respondent's caregiving needs were interviewed. Informant interviews were not conducted for a few elderly respondents (n = 153, 14.2%). Informant interviews are specific to Wave 7 and, therefore, the data is cross-sectional.
We restrict our sample to adult child/parent dyads based theoretical and empirical considerations. Among informants in the sample 629 (58.4%) are children and 221 (20.5%) other family members, or in a small number of cases paid employees (75, 7%). Preliminary analyses (not reported) indicate that caregivers who are not the care recipients' children have higher incomes and are more likely to receive money from the older person than caregivers who are the care recipient's child. Those who are not children of the elderly adult tend to be older, female, and married and are more likely to have taken the interview in Spanish. In addition, care recipients differ depending on who provides care. Individuals who are cared for by children tend to be older, female, and have more serious IADL disability and cognitive impairment than older individuals who are cared for by others.
Theoretically and empirically, then, caregiving by children and others reflect very different arrangements and expectations. Adult children are also more apt to provide accurate information about the elderly respondents' socio-economic situation and caregiving needs than other individuals (Phillips, Torres de Ardon, Komnenich, Killeen, & Rusinak, 2000). Since the caregiving context and the relationship between caregiver and care recipient is likely to be very different for adult child/parent dyads than for others/older care recipient dyads we restrict our analytic sample to adult child/parent dyads. To simplify our discussion, we refer to the elderly respondents as “parents” and the adult child informants/caregivers as “children.” Appendix A includes additional information concerning the demographic composition of our sample.
Dependent Variable
Sources of Assistance
The child was asked about his/her parent's ability to perform activities of daily life across three domains: personal care, household (instrumental) tasks, and managing financial affairs. We examine four possible sources of care: 1) parent does not need any help, 2) parent needs some help from others, 3) parent is dependent solely on the focal child, 4) parent is dependent on others, including the family. These categories are mutually exclusive and exhaustive. Parents were considered self-sufficient (reference group) if they could care for themselves most of the time without assistance from anyone else.
Independent Variables
Nativity Status
Our primary independent variable is parents' nativity status. Nativity status (0 = U.S. born, 1 = Mexican born) was self-reported by parents when they were first interviewed (i.e., either wave 1 or wave 5).
Child Characteristics
Child sociodemographic characteristics and health status include age (in years), gender (1=female, 0=male), language of interview including Spanish (coded 1) or English (coded 0), education in completed years, marital status (married, divorced/separated, widowed, or never married), proximity to parent including four mutually exclusive categories: co-resident, one mile or less, another city/state/Mexico, and other (unspecified), household income including the following categories: less than $15,000, $15,000 to $29,999, $30,000 or more, and missing, whether the child receives income from the parent, and self-rated health (poor, fair, good, or excellent).
Parent Characteristics
Parent socio-demographic characteristics include age in years ranging from 82 to 102 years (M = 86.0), gender (coded 1 for female and 0 for male), language of interview including Spanish (coded 1) or English (coded 0), education in completed years was reported by respondents at their initial H-EPESE interview (M = 5.0 years). and living arrangements including three mutually exclusive categories: parent lives alone (26.1%), parent lives with his/her spouse only (16.2%), or parent lives with someone other than their spouse (57.7%).
Financial Situation of Parent
Children were asked to indicate whether the parent's income was “adequate enough to cover [their] monthly expenses” (1 = inadequate income, 0 = adequate income). We include a dummy variable indicating whether or not the parent received any financial support from his/her children (1 = received financial support, 0 = received no financial support). Relatively few individuals were missing on the economic hardship (n = 5, 0.8%) and child financial support (n = 27, 4.3%) measures. We created a variable with the following categories for parents' current insurance coverage status: Medicare only (18.4%), Medicare and Medicaid (52.9%), Medicare and any private insurance coverage (19.1%), or unknown (9.5%).
Health of Parent
Children provided information about their elderly parents' ability to perform basic and instrumental activities of daily living. We summed their responses to these questions to create two indices that measure ADL (range: 0-7; M = 2.0) and IADL limitations (range: 0-6; M = 3.6). Higher scores on the ADL and IADL scales indicate greater levels of disablement. Most individuals missing all seven IADL items (n = 27) had proxy interviews due to mental impairment (e.g., diagnosed dementia, confusion while taking the survey, etc.) and/or physical impairment (e.g., paralysis, blindness, etc.). These individuals were assigned a seven on the IADL scale under the assumption that they had severe disablement.
Interviewers also administered the Performance-Oriented Mobility Assessment (POMA) (Guaralnik et al., 1994) to the parent. The POMA includes four items that objectively measure balance and gait: balance (semi-tandem, full tandem, and single leg), stands (repeated chair stands), and gait assessment (inability to walk approximately 10 feet across a room or taking more than 13 seconds to complete such a walk). We summed the POMA items to create a 13-point scale (range 0-12; M = 4.0), with lower scores indicating poorer performance (Tinetti, 1986). Individuals who were unable to complete all the POMA items because they were bedridden, unable to stand with support, only able to stand with support, or restricted to a wheelchair were considered severely impaired and assigned a zero. The analyses exclude a few respondents with missing POMA scores (n = 10, 1.6%).
The parents also completed the Mini Mental Status Exam (MMSE). The MMSE measures cognitive function by assessing orientation, attention, immediate and short-term memory recall, language, and the ability to follow simple verbal and written commands (Nguyen et al., 2003). Higher scores indicate better cognitive functioning (Folstein et al., 1975). The mean is 18.30 and range is 0 to 30. Parents who did not complete the MMSE (n = 77, 8.3%) were considered “definitely impaired” and assigned a “0” on the scale in situations where proxy interviews were necessary due to “mental incapacitation” or an informant stated that respondent currently received care because s/he had dementia. Imputation allowed us to retain most individuals with missing MMSE scores (nmissing = 16, 2.5%).
Emotional Well-Being of Parents and Adult Children
We also examine the child's perceived level of stress and reported levels of interpersonal conflict with their parent. Child informants' perceived stress was measured via a four-item scale asking informants to indicate “how often [they] felt” each of the following: 1) “unable to control things in your life,” 2) “confident about your ability to handle your personal problems,” 3) “things were going your way,” and 4) “difficulties were piling up so high that you could not overcome them.” Possible responses included “never,” “almost never,” “sometimes,” “fairly often,” or “very often.” The responses to the second and third items were reverse coded and answers were summed to create a 16-point scale (M = 3.7, range: 0-16). The scale was highly positively skewed and therefore dichotomized so that individuals with scores between 0 and 3 (n = 279, 44.4%) were assigned a zero (“low to mild stress”) and individuals with scores between 4 and 16 (n = 350, 55.6%) were assigned a one (“moderate to high stress”). Finally, interpersonal (i.e., parent-child) conflict was assessed by a question asking informants how well they generally got along with the parent. Possible responses included “not well/not at all,” “not too well,” “somewhat,” “well,” “very well,” or “extremely well.” One informant was excluded due to missing information. To measure informants' perceptions of parent-child conflict, we created a variable signifying “moderate to high” (“not well” to “well,” n = 137, 21.8%), “low” (“very well,” n = 309, 49.2%), and “very low” (“extremely well,” n = 182, 29.0%) conflict.
Analyses
First, we assessed the extent to which parents born in the U.S. and Mexico differed with respect to their socio-demographic characteristics, financial situation, health insurance coverage, functional capabilities, and cognitive and physiological impairment levels (Tables 1 and 2). We conducted t-tests to evaluate whether any differences observed by nativity status were statistically significant. Second, we conducted bivariate analyses to evaluate whether the person(s) responsible for assisting the elderly parents with their personal care, household tasks, and financial affairs differs between U.S.-born and Mexican-born parents (Table 3). We then estimated three multinomial logistic regression models that evaluate the extent to which the person(s) responsible for assisting the parents with their personal care, household tasks, and financial affairs differs by parental nativity status once the parents' socio-demographic factors, socio-economic factors, and cognitive/physical functioning is taken into account (Table 4). Finally, we assessed nativity differences in perceived level of stress and parent-child conflict (Table 5).
Table 1. Child Informants' Characteristics By Parents' Nativity Status, H-EPESE Wave 7.
| Overall (n = 629) |
U.S. born (n = 341) |
Mexican Born (n = 288) |
||||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| n | % (Mean) | n | % (Mean) | n | % (Mean) | |
| Age (mean) | 628 | 55.0 | 341 | 55.4 | 287 | 54.7 |
| Female (%) | 437 | 69.5 | 237 | 69.5 | 200 | 69.4 |
| Spanish Interview (%) | 364 | 57.9 | 172 | 50.4 | 192 | 66.7* |
| Education (years, mean) | 619 | 11.6 | 334 | 12.3 | 285 | 10.7* |
| Marital Status (%) | ||||||
| Married | 326 | 52.2 | 178 | 52.5 | 148 | 51.8 |
| Divorced/Separated | 159 | 25.4 | 93 | 27.4 | 66 | 23.1 |
| Widowed | 34 | 5.4 | 18 | 5.3 | 16 | 5.6 |
| Never Married | 106 | 17.0 | 50 | 14.8 | 56 | 19.6 |
| Proximity to Parent | ||||||
| Co-Resident | 292 | 46.9 | 145 | 42.9 | 147 | 51.6* |
| One Mile or Less | 198 | 31.8 | 112 | 33.1 | 86 | 30.2 |
| Another City/State/Mexico | 87 | 14.0 | 49 | 14.5 | 38 | 13.3 |
| Other (Unspecified) | 46 | 7.4 | 32 | 9.5 | 14 | 4.9* |
| Household Income (%) | ||||||
| < $15,000 | 174 | 27.7 | 90 | 26.4 | 84 | 29.2 |
| $15,000 to $29,999 | 157 | 25.0 | 77 | 22.6 | 80 | 27.8 |
| $30,000+ | 235 | 37.4 | 141 | 41.4 | 94 | 32.6* |
| Missing | 63 | 10.0 | 33 | 9.7 | 30 | 10.4 |
| Receives Income from Parent (%) | 89 | 14.2 | 56 | 16.4 | 33 | 11.6 |
| Self-Rated Health (%) | ||||||
| Poor | 32 | 5.1 | 15 | 4.4 | 17 | 5.9 |
| Fair | 226 | 36.1 | 122 | 36.0 | 104 | 36.2 |
| Good | 255 | 40.7 | 135 | 39.8 | 120 | 41.8 |
| Excellent | 113 | 18.1 | 67 | 19.8 | 46 | 16.0 |
Notes: The Sample is restricted to Respondents whose child served the Informant. The sample is not restricted to Informants with complete information on the characteristics presented in the table.
p ≤ 0.05
Table 2. Parents' Characteristics By Nativity Status, H-EPESE Wave 7.
| Overall (n = 629) |
U.S. born (n = 341) |
Mexican Born (n = 288) |
||||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| n | % (Mean) | n | % (Mean) | n | % (Mean) | |
| Age (mean)b | 629 | 86.0 | 341 | 85.7 | 288 | 86.3 |
| Female (%)b | 423 | 67.3 | 231 | 67.7 | 192 | 66.7 |
| Spanish Interview (%)a | 523 | 83.2 | 255 | 74.8 | 268 | 93.1* |
| Education (mean)b | 618 | 5.0 | 335 | 6.2 | 283 | 3.6* |
| Living Arrangements (%)a | ||||||
| Spouse Only | 101 | 16.2 | 59 | 17.5 | 42 | 14.7 |
| Lives Alone | 162 | 26.1 | 91 | 27.0 | 71 | 24.9 |
| Others Present | 359 | 57.7 | 187 | 55.5 | 172 | 60.4 |
| Inadequate Income (%) | 126 | 20.2 | 55 | 16.2 | 71 | 24.9* |
| Receives Income from Child (%) | 131 | 21.8 | 78 | 23.6 | 53 | 19.6 |
| Health Insurance Coverage (%) | ||||||
| Medicare Only | 116 | 18.4 | 65 | 19.1 | 51 | 17.7 |
| Medicare & Medicaid | 333 | 52.9 | 160 | 46.9 | 173 | 60.1* |
| Any Private Insurance | 120 | 19.1 | 91 | 26.7 | 29 | 10.1* |
| Informant Did Not Know | 60 | 9.5 | 25 | 7.3 | 35 | 12.2* |
| ADL (mean) | 625 | 2.0 | 339 | 2.0 | 286 | 2.1 |
| IADL (mean) | 629 | 5.3 | 341 | 4.9 | 288 | 5.7* |
| MMSE (mean, range: 0-30)a | 613 | 18.3 | 334 | 18.9 | 279 | 17.3 |
| POMA (mean, range: 0 - 12)b | 619 | 4.0 | 335 | 4.2 | 284 | 3.8 |
Notes: The sample is restricted to Respondents whose child served the Informant. Observations with missing information are not listwise deleted. Consequently, while the overall analytic sample contains n = 629 observations, the statistics presented in the table often are based on fewer observations. Missing IADL items (n=39), MMSE scores (n=62), and POMA scores (n=62) were imputed in the analytic sample.
Ascertained from the respondent at Wave 7.
Ascertained from the respondent at first interview (Wave 1 or 5).
p ≤ 0.05, (U.S. born ≠ Mexican Born)
Table 3. The Distribution of Sources and Types of Caregiving Assistance By Nativity Status (n = 629), H-EPESE Wave 7.
| Overall (n = 629) | U.S. born (n = 341) | Mexican Born (n = 288) | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| n | % | n | % | n | % | |
| Parents' Personal Care | ||||||
| Parent Only | 354 | 56.3 | 201 | 58.9 | 153 | 53.1 |
| Parent & Others | 107 | 17.0 | 55 | 16.1 | 52 | 18.1 |
| Child Only | 80 | 12.7 | 35 | 10.3 | 45 | 15.6 |
| Child & Others | 88 | 14.0 | 50 | 14.7 | 38 | 13.2 |
| χ2 = 5.049, df = 3, p = 0.168 | ||||||
| Parents' Household Tasks | ||||||
| Parent Only | 141 | 22.4 | 79 | 23.2 | 62 | 21.5 |
| Parent & Others | 115 | 18.3 | 76 | 22.3 | 39 | 13.5 |
| Child Only | 180 | 28.6 | 87 | 25.5 | 93 | 32.3 |
| Child & Others | 193 | 30.7 | 99 | 29.0 | 94 | 32.6 |
| χ2 = 9.888, df = 3, p = 0.020 | ||||||
| Parents' Financial Affairs | ||||||
| Parent Only | 246 | 39.1 | 145 | 42.5 | 101 | 35.1 |
| Parent & Others | 52 | 8.3 | 35 | 10.3 | 17 | 5.9 |
| Child Only | 234 | 37.2 | 107 | 31.4 | 127 | 44.1 |
| Child & Others | 97 | 15.4 | 54 | 15.8 | 43 | 14.9 |
| χ2 = 12.682, df = 3, p = 0.005 | ||||||
Notes: The Sample is restricted to Respondents whose child served the Informant. The analyses are not weighted. Caregiving roles were reported by Informants. Nativity status was reported by Respondents at their first interview (i.e., Wave 1 or 5). The table displays cell frequencies and column percentages.
Table 4. Multinomial Logistic Regression Models Predicting Parental Caregiving Responsibilities, H-EPESE (Wave 7).
| Personal Care | Household Tasks | Financial Affairs | |||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||
| Parent/Others | Child Only | Child/Others | Parent/Others | Child Only | Child/Others | Parent/Others | Child Only | Child/Others | |
| vs. Parent Only | vs. Parent Only | vs. Parent Only | vs. Parent Only | vs. Parent Only | vs. Parent Only | vs. Parent Only | vs. Parent Only | vs. Parent Only | |
|
|
|
|
|||||||
| Mexican Born | 0.943 | 0.954 | 0.983 | 0.516* | 0.780 | 0.904 | 0.543 | 1.113 | 0.826 |
| N | 560 | 560 | 560 | ||||||
| Pseudo R2 | 0.284 | 0.151 | 0.163 | ||||||
Notes. The table displays relative risk ratios. The models control for age, gender, education, co-residence, MMSE, POMA, income adequacy, receipt of income from their child, and health coverage.
p<.05;
p<.01;
p<.001
Table 5. Distribution of Factors Contributing to Role Strain Among Child Informants By Parents' Nativity Status, H-EPESE Wave 7.
| Overall (n = 629) | U.S. born (n = 341) | Mexican born (n = 288) | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| n | % | n | % | n | % | |
| Informants' Perceived Level of Stress | ||||||
| Low to Mild | 423 | 67.3 | 233 | 68.3 | 190 | 68.3 |
| Moderate to High | 206 | 32.8 | 108 | 31.7 | 98 | 31.7 |
| Total | 629 | 100.0 | 341 | 100.0 | 288 | 100.0 |
| χ2 = 0.394, df = 1, p = 0.530 | ||||||
| Informants' Perceived Parent-Child Conflict | ||||||
| Moderate to High | 137 | 21.8 | 64 | 18.8 | 73 | 25.4 |
| Low | 309 | 49.2 | 166 | 48.7 | 143 | 49.8 |
| Very Low | 182 | 29.0 | 111 | 32.6 | 71 | 24.7 |
| Total | 628 | 100.0 | 341 | 100.0 | 287 | 100.0 |
| χ2 = 6.499, df = 2, p = 0.039 | ||||||
Notes: The Sample is restricted to Respondents whose child served the Informant. The analyses are not weighted. Caregiving roles were reported by Child Informants. Nativity status was reported by Respondents at their first interview (i.e., Wave 1 or 5). The table displays cell frequencies and column percentages.
Results
Table 1 shows that most caregivers are female (69.5%), married (52.2%), rated their health as either good or excellent (58.8%). The mean age was 55 years old. As one might expect, Spanish interviews were much more common among children whose parents were immigrants (66.7%) in comparison to those whose parents were U.S. born (50.4%). Residential proximity and socioeconomic status also varied by parental nativity status. Specifically, immigrant parents were more apt to co-reside with their children compared to parents who were U.S. born (42.9% vs. 52.6%; p < 0.05). Additionally, children whose parents were born in Mexico had fewer years of schooling and lower household incomes when compared to children whose parents were U.S. born. A lower percentage of immigrant children (11.6%) than the children of U.S. born (16.4%) reported that they received financial support from their parent within the last year, but these differences were only marginally significant (x2 = 2.927; p = 0.087).
Table 2 focuses on parent characteristics by nativity status. Approximately 46 percent were born in Mexico. The U.S.-born and Mexican-born populations had comparable age structures and gender compositions. While about 75% of the U.S. born was interviewed in Spanish, about 93% of the Mexican-born were interviewed in Spanish. Living in households with someone other than a spouse was more common among Mexican-born parents (60.4%) than U.S. born (55.5%), but these differences were not statistically significant. Table 2 also shows that, as expected, Mexican-born parents are much more socioeconomically disadvantaged in comparison to parents who are U.S. born. The sample had low levels of educational attainment overall (M = 5.0 years), but U.S.-born parents (M = 6.2 years) completed considerably more schooling than Mexican-born parents (M = 3.6 years). More U.S. born (23.6%) than Mexican born (19.6%) parents received financial support from their adult children, but these differences were not statistically significant. Mexican-born parents were more apt to experience economic hardship than their U.S-born parents (24.9% vs. 16.2%), and these differences were statistically significant. Health insurance coverage and, to a lesser extent, physical and cognitive impairment also significantly varies by nativity status. Compared to U.S-born parents, more Mexican-born parents were covered by Medicaid (60.1% vs. 40.9%), and fewer Mexican-born parents were covered by private insurance (10.1% vs. 26.7%). These results are not surprising given the rather large differences in economic hardship between U.S. and Mexican-born parents.
Table 3 presents the distribution and type of caregiving received by parents by nativity status. The results show that most parents do not receive assistance in performing tasks related to self-care (56.3%). A slightly higher percentage of U.S. born (58.9%) than Mexican born (53.1%) parents did not have any assistance performing self-care activities, but these differences were not statistically significant (x2 = 5.049, p = 0.168). In contrast, elderly parents were more apt to rely on others for assistance with various household tasks. The results demonstrate that this trend is particularly the case among Mexican-born parents who were more likely than U.S. born parents to receive assistance with household tasks from their adult children and/or other relatives (x2 = 9.888, p = .02). In addition, the results indicate that parents born in Mexico were more likely to rely on one child to assist them with their financial affairs than were U.S-born parents (x2 = 12.682, p = 0.005).
Table 4 presents relative risk ratios from multinomial logistic regression models predicting nativity differences in caregiving arrangements. The results suggest that elderly parents' prospects of being completely self-reliant vs. receiving some assistance from others with household tasks was about 50 percent lower (RRR = 0.516, p ≤ 05.)for Mexican-born parents than U.S-born parents. Additionally, when controlling for parental socio-demographic characteristics, health insurance coverage status, economic hardship, and physical and cognitive functioning, the coefficient for Mexican Born in the model for financial affairs only attained marginal significance (RRR = 0.543; p ≤ 0.10). This suggests that the high rates of dependency on one focal child for financial tasks by Mexican-born parents relative to U.S-born parents is reflective of the significant nativity differences in these control variables. Not surprisingly, results suggest that elderly Latino individuals who are female, socioeconomically disadvantaged, and physically and/or cognitively impaired are more likely to rely on others for assistance with personal care and financial affairs net of nativity status and the other controls (not presented).
Table 5 provides information about the focal child's emotional wellbeing. While levels of perceived stress did not significantly differ between children whose parents were born in Mexico and the United States, the results imply that the children of immigrants experience more conflict with their parents than children whose parents were U.S. born.
Discussion
Despite economic disadvantage, the long life expectancy of the Mexican-origin population, or the so-called “Latino Paradox,” presents formidable challenges in providing late-life family caregiving (Markides & Eschbach, 2011). Since the first wave of the H-EPESE, which occurred almost two decades ago, the study has documented a persistent low use of nursing homes, reflecting the observation that families are the primary source of care for older individuals of Mexican origin. This is the first and to our knowledge largest caregiving study that helps to answer the question of who is caring for aging Mexican-origin Latinos at a period in the life course in which disability, dependency, and vulnerability are most common. This paper extended previous research on Latino aging by examining the role of the children of Mexican-origin Latino elders in providing assistance with daily activities, including household tasks and finances.
The preference to care for aging parents at home may be undermined by the demands of serious illness and disability at a time when adult children find it necessary to work and care for their own children. In this wave of the H-EPESE, the average age of the survivors was 86 years old, many had a high level of ADL and IADL dependence and poor performance on physical mobility tests, and the vast majority of them still lived in the community, many with their grown children. The child caregivers reported high levels of material hardship, financial strain, and low rates of private insurance coverage for their aging parents. This study also highlights the significance of nativity as an independent source of variation in caregiving roles as they relate to living arrangements.
Our findings build on qualitative studies that examine how changing cultural traditions in the Mexican-origin family relate to parental care (Crist, Garcia-Smith, & Phillips, 2006; Crist et al., 2007; A. P. Herrera et al., 2008; Mausbach et al., 2004; Radina, 2007). We demonstrate that children of U.S. born parents show a greater willingness than children of the Mexican-born parents to seek assistance for household tasks and financial affairs from both within and outside the family network, including social service agencies.
At the initial wave of the H-EPESE, the Mexican born were more likely than the U.S. born to co-reside with their children. At the 17-year follow up the data reveal that cultural preferences in living arrangements may give way to increasing pressures to care for elderly parents as the result of the onset of physical and cognitive frailty, as well as disability. Adult children, in general, reported a high level of caregiver stress and conflict, providing compelling evidence that the demands faced by the Mexican-origin family are significant (Aranda and Knight (1999). The analysis identified a potential source of conflict in immigrant families. Mexican-born elders were far more likely to report cognitive impairment, mobility limitations, ADL and IADL disability than the U.S. born, suggesting that Mexican-born parents have more complex needs that create caregiver role strain.
In light of the historically low levels of nursing home care and other private pay care service utilization within Latino immigrant communities, keeping aging parents at home may be an unrealistic objective, especially for dementia care (Apesoa-Varano, Barker, & Hinton, 2012; Hinton, Haan, Geller, & Mungas, 2003). Taking a closer look at the H-EPESE cohort demonstrates the need for policies aimed at maximizing cost-effective and culturally sensitive options in long-term care. Local, state, and federal governments are faced with increasing challenges related to Medicaid-funded elder care. Some of the most promising programs are designed to help Latino families keep their aging parents in the community by providing home-based assistance to the older person and his or her caregiver (Aranda, Villa, Trejo, Ramirez, & Ranney, 2003).
In conclusion, the lesson we come away with from the present investigation is that the Latino community, like every other community, is changing in ways that will affect its ability to provide all of the care older members need (Stone, 2011). While we establish differences in parental support based on nativity status, numerous questions remain as to the motivation and consequences of the need to care for aging parents. Identifying the numerous and complex financial, cultural, and social constraints involved in providing partial or complete support for aging parents, especially among the Mexican-origin population, is needed. In addition, a deeper understanding of the psychological and economic consequences of the burden of caregiving on younger generations merits attention. Such knowledge would better inform the development of public policies and support system for adult child caregivers and help coordinate informal and formal care delivery.
Appendix A. The Distribution of Key Respondent Demographics in 2010-11 (Wave 7)
|
|
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All Respondents | Informant Caregiver Dyads | |||||||||
|
|
|
|||||||||
| Total | No Informant | Total | Child | Non-Child | ||||||
|
|
|
|
|
|
||||||
| n | % | n | % | n | % | n | % | n | % | |
| Overall | ||||||||||
| Female | 700 | 64.9 | 98 | 64.1 | 602 | 65.1 | 423 | 67.3 | 179 | 60.5 |
| Education (mean) | 1,066 | 5.1 | 153 | 6.2 | 913 | 4.9 | 618 | 5.0 | 295 | 4.6 |
| Financially | ||||||||||
| Strained | 189 | 19.4 | 18 | 12.3 | 171 | 20.7 | 113 | 20.4 | 58 | 21.3 |
| Mexican Born | 490 | 45.5 | 67 | 43.8 | 423 | 45.7 | 288 | 45.8 | 135 | 45.6 |
| Total N | 1,078 | 153 | 925 | 629 | 296 | |||||
| U.S. Born | ||||||||||
| Female | 391 | 66.5 | 60 | 69.8 | 331 | 65.9 | 231 | 67.7 | 100 | 62.1 |
| Education (mean) | 581 | 6.3 | 86 | 7.3 | 495 | 6.1 | 335 | 6.2 | 160 | 5.9 |
| Financially | ||||||||||
| Strained | 85 | 16.1 | 10 | 12.4 | 75 | 16.8 | 48 | 16.0 | 27 | 18.6 |
| Total N | 588 | 86 | 502 | 341 | 161 | |||||
| Mexican Born | ||||||||||
| Female | 309 | 63.1 | 38 | 56.7 | 271 | 64.1 | 192 | 66.7 | 79 | 58.5 |
| Education (mean) | 485 | 3.6 | 67 | 4.8 | 418 | 3.5 | 283 | 3.6 | 135 | 3.1 |
| Financially | ||||||||||
| Strained | 104 | 23.3 | 8 | 12.3 | 96 | 25.2 | 65 | 25.7 | 31 | 24.2 |
| Total N | 490 | 67 | 423 | 288 | 135 | |||||
References
- Angel JL, Angel RJ. Aging Trends: Mexican Americans in the Southwestern USA. Journal of Cross-Cultural Gerontology. 1998;13:281–290. doi: 10.1023/a:1006505814367. [DOI] [PubMed] [Google Scholar]
- Angel JL, Angel RJ, McClellan JL, Markides KS. Nativity, Declining Health, and Preferences in Living Arrangements among Elderly Mexican Americans: Implications for Long term Care. The Gerontologist. 1996;36:464–473. doi: 10.1093/geront/36.4.464. [DOI] [PubMed] [Google Scholar]
- Angel RJ, Angel JL. Hispanic Families at Risk: The New Economy, Work, and the Welfare State. New York, NY: Springer Sciences; 2009. [Google Scholar]
- Angel RJ, Angel JL, Lee GY, Markides KS. Age at Migration and Family Dependency among Older Mexican Immigrants: Recent Evidence from the Mexican American EPESE. The Gerontologist. 1999;39:59–65. doi: 10.1093/geront/39.1.59. [DOI] [PubMed] [Google Scholar]
- Apesoa-Varano EC, Barker JC, Hinton L. Mexican-American Families and Dementia: An Exploration of “Work” in Response to Dementia-Related Aggressive Behavior. In: Angel JL, Torres-Gil F, Markides K, editors. Aging, Health, and Longevity in the Mexican-Origin Population. New York, NY: Springer Science; 2012. pp. 277–289. [Google Scholar]
- Aranda M, Knight BG. The Influence of Ethnicity and Culture on the Caregiver Stress and Coping Process: A Sociocultural Review and Analysis. The Gerontologist. 1999;37(3):342–354. doi: 10.1093/geront/37.3.342. [DOI] [PubMed] [Google Scholar]
- Aranda M, Villa V, Trejo L, Ramirez R, Ranney M. El Portal Latino Alzheimer's Project: Model Program for Latino Caregivers of Alzheimer's Disease-Affected People. Social Work. 2003;48(2):259–271. doi: 10.1093/sw/48.2.259. [DOI] [PubMed] [Google Scholar]
- Carmel S, Morse C, Torres-Gil F, editors. The Art of Caring for Older Adults. Amityville, New York: Baywood Publishing Company, Inc; 2007. [Google Scholar]
- Connidis IA. Negotiating Inequality among Adult Siblings: Two Case Studies. Journal of Marriage and Family. 2007;69(2):482–499. [Google Scholar]
- Connidis IA, Kemp C. Negotiating Actual and Anticipated Parental Support: Multiple Sibling Voices in Three-Generation Families. Journal of Aging Studies. 2008;22(3):228–238. [Google Scholar]
- Crist JD, Garcia-Smith D, Phillips L. Accommodating the Stranger en Casa: How Mexican American Elders and Caregivers Decide to Use Formal Care. Research and Theory for Nursing Practice. 2006;20(2):109–126. doi: 10.1891/088971806780641791. [DOI] [PubMed] [Google Scholar]
- Crist JD, Garcıa-Smith D, Phillips LR. Accommodating the Stranger en Casa: How Mexican American Elders and Caregivers Decide to Use Formal Care. Research and Theory for Nursing Practice: An International Journal. 2006;20(2):109–126. doi: 10.1891/rtnp.20.2.109. [DOI] [PubMed] [Google Scholar]
- Crist JD, Woo SH, Choi M. Mexican American and Anglo elders' use of home care services. Journal of Transcultural Nursing. 2007;18:339–348. doi: 10.1177/1043659607305190. [DOI] [PubMed] [Google Scholar]
- Cucciare MA, Gray H, Azar A, Jimenez D, Gallagher-Thompson D. Exploring the relationship between physical health, depressive symptoms, and depression diagnoses in Hispanic dementia caregivers. Journal of Aging and Mental Health. 2010;14(3):274–282. doi: 10.1080/13607860903483128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeNavas C, Proctor BD, Smith JC. Income, Poverty, and Health Insurance Coverage inthe United States: 2010. Washington, DC: U.S. Census Bureau; 2011. [Google Scholar]
- Dilworth-Anderson P, Williams IC, Gibson BE. Issues of Race, Ethnicity, and Culture in Caregiving Research: A Twenty - year Review (1980-2000) The Gerontologist. 2002;42(2):237–272. doi: 10.1093/geront/42.2.237. [DOI] [PubMed] [Google Scholar]
- Espino DV, Angel JL, Wood RC, Finely MR, Ye Y. Characteristics of Mexican American Elders Admitted to Nursing Facilities in the United States: Data from the Hispanic Established Populations for Epidemiologic Studies of the Elderly (EPESE) Dtudy. Journal of the America Director's Association. 2013;14(3):226.e221–224. doi: 10.1016/j.jamda.2012.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evercare. Hispanic Family Caregiving in the US: Findings from a National Study. Bethesda, MD: National Alliance for Caregiving; 2008. [Google Scholar]
- Gassoumis Z, Wilber KH, Baker LA, Torres-Gil F. Latino Baby Boomers: A Demographic and Economic Profile Los Angeles. University of California; Los Angeles: 2010. [Google Scholar]
- Gaugler JE, Kane RL, A R, Newcomer R. Predictors of institutionalization in Latinos with dementia. Journal of Cross Cultural Gerontology. 2006;21:139–155. doi: 10.1007/s10823-006-9029-8. [DOI] [PubMed] [Google Scholar]
- Herrera A, Angel JL, Venegas CD, Angel RJ. Estimating the Demand for Long-Term Care Among Aging Mexican Americans: Cultural Preferences Versus Economic Realities. In: Angel JL, Torres-Gil F, Markides K, editors. Aging, Health, and Longevity in the Mexican-Origin Population. New York, NY: Springer Science; 2012. pp. 259–276. [Google Scholar]
- Herrera AP, Benson R, Angel JL, Markides K, Torres-Gil F. Variation in Older Americans Act Caregiver Service Use, Unmet Hours of Care, and Independence Among Hispanics, African Americans, and Whites. Home Health Care Services Quarterly. 2013;32:35–56. doi: 10.1080/01621424.2012.755143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herrera AP, Lee JW, Palos G, Torres-Vigil I. Cultural influences in the patterns of long-term care use among Mexican-American family caregivers. Journal of Applied Gerontology. 2008;27:141–165. [Google Scholar]
- Hinton L, Haan M, Geller S, Mungas D. Neuropsychiatric symptoms in Latino Elders with Dementia or Cognitive Impairment without Dementia and Factors that Modify their Association with Caregiver Depression. The Gerontologist. 2003;43(5):669–677. doi: 10.1093/geront/43.5.669. [DOI] [PubMed] [Google Scholar]
- Kochhar R. The Occupational Status and Mobility of Hispanics. Washington, DC: Pew Hispanic Center; 2005. [Google Scholar]
- Lee R, Mason A, editors. Population Aging and the Generational Economy. Northampton, MA: Edward Elgar Publishing; 2011. [Google Scholar]
- Markides KS, Black SA. Race, Ethnicity, and Aging: The Imapct of Inequality. In: Binstock RH, George LK, editors. Handbook of Aging and the Social Sciences. New York, NY: Academic Press; 1995. pp. 153–170. [Google Scholar]
- Markides KS, Eschach K, Ray LA, Peek MK. Census Disability Rates among Older People by Race/Ethnicity and Type of HIspanic Origin. In: Angel JL, Whitfield KE, editors. The Health of Aging Hispanics: The Mexican-origin Population. New York: Springer; 2007. pp. 26–39. [Google Scholar]
- Markides KS, Eschbach K. Hispanic Paradox and Adult Mortality. In: Rogers R, Crimmins E, editors. International Handbook of Adult Mortality. New York, NY: Springer Sciences; 2011. pp. 227–240. [Google Scholar]
- Markides KS, Peek MK, Angel R. Aging, Health, and Families in the Hispanic Population. In: Silverstein M, Giarusso R, editors. Kinship and Cohort in an Aging Society. Baltimore, MD: Johns Hopkins University; 2013. pp. 314–331. [Google Scholar]
- Massey D. Isolated, Vulnerable And Broke. New York Times. 2011 Jul 26; Retrieved from http://www.nytimes.com/2011/08/05/opinion/hispanic-families-isolated-and-broke.html?_r=0.
- Mausbach BT, Coon DW, Depp C, Rabinowitz YG, Wilson-Arias E, Kraemer HC, Gallagher-Thompson D. Ethnicity and time to institutionalization of dementia patients: A comparison of Latina and Caucasian female family caregivers. Journal of the American Geriatrics Society. 2004;52(7):1077–1084. doi: 10.1111/j.1532-5415.2004.52306.x. [DOI] [PubMed] [Google Scholar]
- Orszag PR, Rodriguez E. Retirement Security for Latinos: Bolstering Coverage, Savings, and Adequacy. Washington DC: The Retirement Security Project, National Council of La Raza; 2005. [Google Scholar]
- Radina EM. Mexican American Siblings Caring for Aging Parents: Processes of Caregiver Selection/Designation. Journal of Comparative Family Studies. 2007;38(1):143–168. [Google Scholar]
- Stone R. Long-Term Care for the Elderly. Washington, DC: Urban Institute press; 2011. [Google Scholar]
- Tavernise S. Recession Study Finds Hispanics Hit the Hardest. 2011 Jul 26; http://www.nytimes.com/2011/07/26/us/26hispanics.html.
- Taylor RJ, Chatters LM. Patterns of Informal Support to Elderly Black Adults: Family, Friends, and Church Members. Social Work. 1986 Nov-Dec;:432–437. [Google Scholar]
- Torres-Gil F, Greenstein R, Kamin D. The Importance of Social Security to the Hispanic Community. Washington DC: Center on Budget and Policy Priorities; 2005. [Google Scholar]
- Umberson D, Montez JK. Social Relationships and Health: A Flashpoint for Public Policy. Journal of Health and Social Behavior. 2010;51:S54–S66. doi: 10.1177/0022146510383501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- United States Department of Labor. The Latino Labor Force in the Recovery. The Latino Labor Force at a Glance. 2012 (Table 1) http://www.dol.gov/_sec/media/reports/hispaniclaborforce/
- Villa VM, Aranda MP. The demographic, economic, and health profile of older Latinos: Implications for health and long-term care policy and the Latino family. Journal of Health and Human Services Administration. 2000;23(2):161–180. [PubMed] [Google Scholar]
- Werner P, Mittelman MS, Goldstein D, Heinik J. Family Stigma and Caregiver Burden in Alzheimer's Disease. The Gerontologist. 2012;52(1):89–97. doi: 10.1093/geront/gnr117. [DOI] [PubMed] [Google Scholar]
- Wong R, Espinoza M, editors. Dynamics of intergenerational assistance in middle-and old-age in Mexico. New York, NY: Springer Sciences; 2007. [Google Scholar]
- Zarit S, Reamy A. Future Directions in Family and Professional Caregiving for the Elderly. Gerontology. 2012;59(2):152–158. doi: 10.1159/000342242. [DOI] [PubMed] [Google Scholar]