

Abstract
Objective
To characterize the cohort who may become senior leaders in obstetrics and gynecology by examining the gender and subspecialty of faculty in academic department administrative and educational leadership roles.
Methods
This is an observational study conducted through websites of U.S. obstetrics and gynecology residency programs accredited in 2012-2013.
Results
In obstetrics and gynecology departmental administrative leadership roles, women comprised 20.4% of chairs, 36.1% of vice chairs, and 29.6% of division directors. Among educational leaders, women comprised 31.9% of fellowship directors, 47.3% of residency directors and 66.1% of medical student clerkship directors. Chairs were most likely to be maternal–fetal medicine faculty (38.2%), followed by specialists in general obstetrics and gynecology (21.8%), reproductive endocrinologists (15.6%), and gynecologic oncologists (14.7%). Among chairs, 32.9% are male maternal–fetal medicine specialists. Family planning had the highest representation of women (80.0%) among division directors, while reproductive endocrinology and infertility had the lowest (15.8%).
The largest proportion of women chairs, vice chairs, residency program directors, and medical student clerkship directors were specialists in general obstetrics and gynecology.
Conclusion
Women remained under-represented in the departmental leadership roles of chair, vice chair, division director, and fellowship director. Representation of women was closer to parity among residency program directors, where women held just under half of positions. Nearly one in three department chairs was a male maternal–fetal medicine specialist. Compared to subspecialist leaders, specialist leaders in general obstetrics and gynecology were more likely to be women.
Introduction
Women comprise nearly half of medical school students and residents and 37% of medical school faculty members (1-3). However, the proportion of women who advance to the senior ranks of academic medicine remains lower than that of men (3,4). Obstetrics and gynecology has the largest proportion of women residents (81%), faculty (54%), and department chairs (20%) compared to other specialties (3,5). Women have comprised more than 50% of obstetrics and gynecology residency graduates for over 20 years (6). If women and men progress to leadership positions at the same rate, after enough time has elapsed, gender distributions in leadership roles should reflect the historical residency cohorts. If one assumes that 20 years is sufficient time for faculty members to advance to career positions at which promotion to leadership positions is common, (7) based on this historical residency cohort we would expect women and men to hold most obstetrics and gynecology departmental leadership roles in similar numbers.
The Association of American Medical Colleges provides data on the overall proportion of women in the leadership roles of department chair (14%), vice chair (22%), and division director (22%), but these data are consolidated across all medical specialties (3). The objective of this study was therefore to describe the cohort of faculty who may become senior leaders in obstetrics and gynecology by examining the gender and subspecialty of faculty in academic department administrative and educational leadership roles.
Materials and Methods
We conducted a cross-sectional observational study of U.S. academic departments of obstetrics and gynecology. A department was included if it had a residency program that was accredited in 2012-2013 by the Accreditation Council for Graduate Medical Education (8). From November 7, 2012 until January 6, 2013, each academic department's website was visited, and information about leaders within the department was collected. The institutional review board at Beth Israel Deaconess Medical Center approved this project.
Each department's website was searched for information about administrative leadership positions, which included chair, vice chair, and division director, as well as educational leadership positions, which included residency and fellowship program directors and medical student clerkship director. The gender of leaders was determined by name and confirmed by image and pronoun use, when available. Subspecialty was determined by documentation of fellowship training on each website, if applicable. Leaders without apparent subspecialty training who were listed within a subspecialty division or were listed as division directors or fellowship directors were categorized as that subspecialty. Leaders who were not assigned a subspecialty category were considered specialists in general obstetrics and gynecology. Titles and degrees were collected as reported on the websites.
For this study, we considered the titles of assistant chair, associate chair, and co-chair to be equivalent to vice chair. Division chief, division head, and chief (of division) were categorized with division director. Vice chairs or directors of research, medical directors, directors of clinical practice or clinical units, and non-physician leaders were not included. Interim or “acting” titles were recorded in the same way as permanent positions; information on emeritus faculty was not collected. If no leadership information was available but faculty biographies were provided, the individual biographies were searched for relevant titles and positions.
If a department's website did not provide information about its leadership, the department chair was identified on the Association of Professors of Gynecology and Obstetrics website (9) and confirmed via web search: “[name of program] obstetrics gynecology chair”. A similar strategy was used for vice chair and division director. Residency program director information was verified using the Accreditation Council for Graduate Medical Education website (8). If these strategies were unsuccessful, no further search was attempted.
Residency programs were categorized according to the classification used in the American Medical Association's FREIDA Online residency program database as university-based, community-based university-affiliated, community-based, or military (10). Military-based programs and programs outside the 50 U.S. states were excluded because we assumed the pool of potential leaders differed from the general U.S. obstetrician–gynecologist population.
All statistical analyses were performed using SAS 9.3 (SAS Institute, Cary, NC). All tests were two sided, and P values <0.05 were considered statistically significant. Categorical variables were presented as frequency and proportion and compared using the chi-square or Fisher's exact test.
Results
The Accreditation Council for Graduate Medical Education lists 233 non-military U.S. academic departments of obstetrics and gynecology (8). Residency programs in academic departments were university-based (47.6%), community-based with a university affiliation (41.6%), or based in community hospitals (10.7%) (10). A total of 1,575 faculty leaders from these 233 departments were identified. Department websites containing faculty names were available for 231 departments (99.1%). Six websites did not contain information about the department chair.
In obstetrics and gynecology departmental administrative leadership roles, women comprised 20.4% of department chairs, 36.1% of vice chairs, and 29.6% of division directors. In educational leadership roles, women comprised 66.1% of medical student clerkship directors, 47.3% of residency program directors, and 31.9% of fellowship directors. The proportions of leaders who were women did not differ when comparing university-based and community-based departments with or without university affiliations (all P≥0.10) with the exception of residency program directors, where women comprised a higher proportion in university-based departments (P<0.001).
Department chairs who were men were significantly more likely to have subspecialty training (81.6%) compared with department chairs who were women (65.2%; P=0.02). Among obstetrics and gynecology subspecialties, the greatest proportion of department chairs was maternal–fetal medicine faculty (38.2%), followed by specialists in general obstetrics and gynecology (21.8%), reproductive endocrinologists (15.6%), and gynecologic oncologists (14.7%). Nearly 1 in 3 (32.7%) general obstetrics and gynecology specialist department chairs was a woman (Table 1). In contrast, among maternal–fetal medicine specialists serving as chairs, only 12 (14.0%) were women—the lowest among all accredited subspecialties. Nearly one-third of all department chairs was a male maternal– fetal medicine specialist. Among university-based departments, women department chairs were significantly more likely to be subspecialists (81.5%) than women department chairs at community-based departments (42.1%; P=0.01). A similar pattern was seen among chairs who were men, with 91.6% in university-based departments being subspecialists compared with 73.4% in community-based departments (P=0.004).
Table 1.
Subspecialty and Gender for Obstetrics and Gynecology Leadership Roles
| Title | General Obstetrics and Gynecology | Maternal-Fetal Medicine | Gynecologic Oncology | Reproductive Endocrinology and Infertility | Female Pelvic Medicine and Reconstructive Surgery | Minimally-Invasive Gynecologic Surgery | Family Planning | Other |
|---|---|---|---|---|---|---|---|---|
| Department Chair, n | 49 | 86 | 33 | 35 | 12 | 3 | 1 | 6 |
| Women, n (%) | 16 (32.7) | 12 (14.0) | 7 (21.2) | 5 (14.3) | 3 (25.0) | 0 (0.0) | 0 (0.0) | 3 (50.0) |
| Men, n (%) | 33 (67.4) | 74 (86.1) | 26 (78.8) | 30 (85.7) | 9 (75.0) | 3 (100.0) | 1 (100.0) | 3 (50.0) |
| Department Vice Chair, n |
56 | 44 | 17 | 12 | 4 | 2 | 1 | 11 |
| Women, n (%) | 21 (37.5) | 15 (34.1) | 4 (23.5) | 3 (25.0) | 4 (100.0) | 0 (0.0) | 0 (0.0) | 6 (54.6) |
| Men, n (%) | 35 (62.5) | 29 (65.9) | 13 (76.5) | 9 (75.0) | 0 (0.0) | 2 (100.0) | 1 (100.0) | 5 (45.5) |
| Division Director, n | 104 | 135 | 106 | 114 | 66 | 20 | 10 | 29 |
| Women, n (%) | 44 (42.3) | 35 (25.9) | 23 (21.7) | 18 (15.8) | 24 (36.4) | 5 (25.0) | 8 (80.0) | 16 (55.2) |
| Men, n (%) | 60 (57.7) | 100 (74.1) | 83 (78.3) | 96 (84.2) | 42 (63.6) | 15 (75.0) | 2 (20.0) | 13 (44.8) |
| Fellowship Director, n | 0 | 58 | 36 | 27 | 28 | 15 | 12 | 15 |
| Women, n (%) | -- | 17 (29.3) | 8 (22.2) | 4 (14.8) | 12 (42.9) | 1 (6.7) | 9 (75.0) | 10 (66.7) |
| Men, n (%) | -- | 41 (70.0) | 28 (77.8) | 23 (85.2) | 16 (57.1) | 14 (93.3) | 3 (25.0) | 5 (33.3) |
| Residency Program Director, n |
130 | 43 | 11 | 20 | 26 | 3 | 3 | 3 |
| Women, n (%) | 71 (54.6) | 16 (37.2) | 3 (27.3) | 8 (40.0) | 10 (38.5) | 1 (33.3) | 2 (66.7) | 2 (66.7) |
| Men, n (%) | 59 (45.4) | 27 (62.8) | 8 (72.7) | 12 (60.0) | 16 (61.5) | 2 (66.7) | 1 (33.3) | 1 (33.3) |
| Clerkship Director, n | 92 | 15 | 1 | 3 | 2 | 0 | 1 | 1 |
| Women, n (%) | 64 (69.6) | 9 (60.0) | 0 (0.0) | 0 (0.0) | 1 (50.0) | -- | 1 (100.0) | 1 (100.0) |
| Men, n (%) | 28 (30.4) | 6 (40.0) | 1 (100.0) | 3 (100.0) | 1 (50.0) | -- | 0 (0.0) | 0 (0.0) |
Specialists in general obstetrics and gynecology comprised the greatest proportion of vice chairs (38.1%), followed by maternal-fetal medicine specialists (29.9%) (Table 1). Among division directors, family planning had the highest proportion of women (80.0%), although we only identified 10 family planning division directors. This was followed by general obstetrics and gynecology divisions, for which women comprised 42.3% of division directors. The divisions with the lowest proportions of women directors were reproductive endocrinology and infertility (15.8%) and gynecologic oncology (21.7%) (Table 1). Figure 1 shows the numbers of chairs, vice chairs, and division directors stratified by subspecialty and gender.
Figure 1.
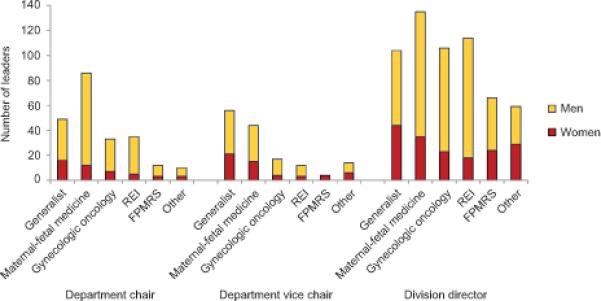
Obstetrics and gynecology administrative leadership by subspecialty and gender. Other includes family planning, minimally-invasive gynecologic surgery, adolescent gynecology, and reproductive infectious diseases. REI, reproductive endocrinology and infertility; FPMRS, female pelvic medicine and reconstructive surgery.
The subspecialty with the highest proportion of fellowship directors who were women (75.0%) was family planning; however, the overall number of family planning fellowship directors identified was small relative to other fellowships. The lowest proportion of women fellowship directors were in the subspecialties of minimally invasive gynecologic surgery (6.7%) and reproductive endocrinology and infertility (14.8%) (Table 1).
Specialists in general obstetrics and gynecology comprised the largest proportion of both the 239 residency program directors (54.4%) and 115 medical student clerkship directors (80.0%). Among residency program directors, general obstetrics and gynecology specialists (54.6%), family planning specialists (66.7%), and other subspecialists (66.7%) had the largest proportion of women. Significantly more department chairs who were women were also residency program directors (26.1%) compared with department chairs who were men (14.0%, P=0.048). The majority (55.7%) of the 115 medical student clerkship directors were women specialists in general obstetrics and gynecology. Figure 2 shows the numbers of fellowship, residency program, and clerkship directors stratified by subspecialty and gender.
Figure 2.
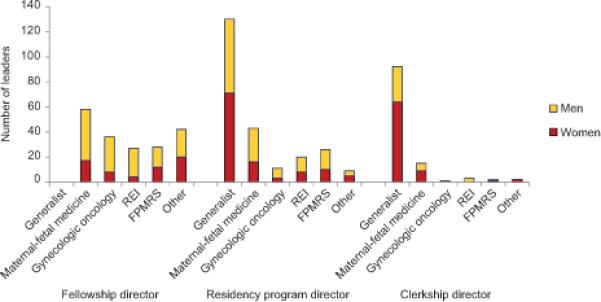
Obstetrics and gynecology educational leadership by subspecialty and gender. Other includes family planning, minimally-invasive gynecologic surgery, adolescent gynecology, and reproductive infectious diseases. REI, reproductive endocrinology and infertility; FPMRS, female pelvic medicine and reconstructive surgery.
Overall, 12.3% of men and 17.6% of women had at least one post-secondary degree in addition to the MD or other doctoral- level clinical degree. For men, the most common additional degree was a PhD (4.2%), and for women the most common additional degree was an MPH or MSPH (8.3%). Among chairs, significantly more women (26.1%) than men (12.9%) had an additional degree (P=0.03).
Discussion
Compared to other medical specialties, obstetrics and gynecology has the highest proportion of women in the department chair role at 20% (3,6); however, our study also finds that men hold more than two-thirds of the department-based leadership positions of chair, vice chair, and division director. With more women than men graduating from obstetrics and gynecology residency programs for over 20 years, clearly women remain underrepresented even in mid-level department leadership roles.
Our study revealed that nearly one-third of obstetrics and gynecology department chairs are male maternal–fetal medicine specialists. Specialists in general obstetrics and gynecology hold a substantial proportion of administrative leadership roles, especially in community-based departments, and the vast majority of residency and medical student program leadership positions. Women pursue subspecialty fellowships less often than men, which may help explain why general obstetrics and gynecology specialist leaders are more likely to be women compared to subspecialist leaders (11). The leadership role of the academic specialist has increased in recent years, further enhanced by support from the Society for Academic Specialists in General Obstetrics and Gynecology (12).
Women are more often found in resident and medical student educational leadership roles than in administrative leadership positions. The reasons for the larger proportion of women in these educational leadership roles are unclear. Perhaps these roles are on a different ‘track’ or are not routes to administrative department leadership; however, we found that 16% of department chairs are also residency program directors. Fulfilling these dual roles is likely challenging due to the Accreditation Council for Graduate Medical Education requirement that obstetrics and gynecology residency program directors devote a minimum of 20 hours weekly to the position (13). Anecdotally, department chairs often ascend from division directors and vice chair positions. Further investigation is required to define the pathways to the chair role, and to what extent, if any, educational leadership roles or subspecialty choice are part of those pathways.
Our data are limited to the information that departments present on the Internet. Over 99% of non-military U.S. residency program websites report faculty information, and our finding for the proportion of women in the chair role was nearly identical to what the Association of American Medical Colleges reports (3). This suggests that, at least for department chairs, our search method was accurate. We used supplemental databases to ensure completeness of department chair and residency program director data, and over 86% of departments had information available for leadership positions beyond these roles. Some of the remaining departments are small and may not have additional faculty leaders. Apparent subspecialty of leaders was determined from websites, which may have led to misclassification due to missing information. While it is difficult to know how up-to-date each website was, data collection occurred over only two months, thus limiting the amount of time for leadership turnover and website changes. Conclusions from our data are limited by our decisions to define academic departments as those with residency programs and to exclude leadership roles such as research positions and medical directors.
Reasons for the continued gender gap even in mid-level department leadership roles in academic obstetrics and gynecology may include a lack of role models, mentors, and representation in professional networks, as well as expectations and choices regarding work and family (14,15). Increasingly, institutional culture and workplace environments have been shown to impact retention and promotion of women as leaders (16-19). Women perceive that flexible career paths and supportive leadership would improve their success in academic medicine (18-20). Interventions modeled from the business community, including academic sponsorship and Stanford's Academic Biomedical Career Customization model, are currently being explored with promising results (16,21,22).
The proportion of women leaders in obstetrics and gynecology mirrors women's representation in other U.S. professions: women comprise 20% of members of Congress (23), 33% of Supreme Court justices (24), and 26% of college presidents (25). As the providers of health care for women and the specialty with the largest proportion of women in its membership, obstetrics and gynecology should instead lead the way in promoting women as leaders.
This study demonstrates that women are significantly under-represented even in mid-level department leadership roles. This situation is not acceptable. Future efforts should include targeted development of women for leadership roles, identifying best-practice cultures in obstetrics and gynecology departments that have successfully promoted higher proportions of women, and overt recognition that increasing the number of women in leadership is a goal. To date, the specialty of obstetrics and gynecology has celebrated its promotion of women as leaders, but this simple view of the number of women achieving leadership does not tell the full story. Recognition that disparities continue, even in mid-level department leadership, is the first step toward attaining proportionate representation of women as senior leaders.
PRECIS.
Women remain underrepresented among departmental leaders, and non-fellowship trained leaders are more often women; one third of department chairs are male maternal–fetal medicine specialists.
Acknowledgments
This work was conducted with support from Harvard Catalyst | The Harvard Clinical and Translational Science Center (National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health Award 1UL1 TR001102-01) and financial contributions from Harvard University and its affiliated academic health care centers.
Footnotes
Financial Disclosure: The authors did not report any potential conflicts of interest.
Contributor Information
Lisa Hofler, Department of Obstetrics and Gynecology Beth Israel Deaconess Medical Center Harvard Medical School.
Michele R. Hacker, Department of Obstetrics and Gynecology Beth Israel Deaconess Medical Center Harvard Medical School Harvard School of Public Health.
Laura E. Dodge, Department of Obstetrics and Gynecology Beth Israel Deaconess Medical Center.
Hope A. Ricciotti, Department of Obstetrics and Gynecology Beth Israel Deaconess Medical Center Harvard Medical School.
References
- 1.Accreditation Council for Graduate Medical Education . ACGME Data Resource Book, Academic Year 2012-2013. Accreditation Council for Graduate Medical Education; Chicago, IL: 2013. [Google Scholar]
- 2.Castillo-Page L. Diversity in Medical Education: Facts and Figures 2012. Association of American Medical Colleges; Washington, DC: 2012.. [Google Scholar]
- 3.Jolliff L, Leadley J, Coakley E, Sloane RA. Women in U.S. Academic Medicine and Science: Statistics and Benchmarking Report 2011-2012. Association of American Medical Colleges; Washington, DC: 2012. [Google Scholar]
- 4.Nonnemaker L. Women physicians in academic medicine: new insights from cohort studies. New Engl J Med. 2000;342:399–405. doi: 10.1056/NEJM200002103420606. [DOI] [PubMed] [Google Scholar]
- 5.Bickel J, Galbraith A, Quinnie R. Women in U.S. Academic Medicine Statistics 1995. Association of American Medical Colleges; Washington, DC: 1995. [Google Scholar]
- 6.Rayburn WF. The obstetrician-gynecologist workforce in the United States: facts, figures, and implications 2011. American Congress of Obstetricians and Gynecologists; Washington, DC: 2011. [Google Scholar]
- 7.Rayburn WF, Schrader RM, Fullilove AM, Rutledge TL, Phelan ST, Gener Y. Promotion rates for assistant and associate professors in obstetrics and gynecology. Obstet Gynecol. 2012;119:1023–9. doi: 10.1097/AOG.0b013e31824fc980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Accreditation Council for Graduate Medical Education [October 15, 2012];List of programs by specialty: obstetrics and gynecology, year ending. 2013 Jun 30; Available at: http://www.acgme.org/.
- 9.Association of Professors of Gynecology and Obstetrics [January 6, 2013];Residency directory listing. Available at: https:/www.apgo.org/component/residencydirectory/.
- 10.American Medical Association [January 31, 2013];FREIDA Online® residency fellowship training program search. Available at: https://freida.ama-assn.org/Freida/user/search/programSearch.do/.
- 11.Gerber SE, Lo Sasso AT. The evolving gender gap in general obstetrics and gynecology. Am J Obstet Gynecol. 2006;195:1427–30. doi: 10.1016/j.ajog.2006.07.043. [DOI] [PubMed] [Google Scholar]
- 12. [July 24, 2014];SASGOG – the Society for Academic Specialists in General Obstetrics and Gynecology. Available at: http://www.sasgog.org.
- 13.Accreditation Council for Graduate Medical Education [November 1, 2014];ACGME program requirements for graduate medical education in obstetrics and gynecology. Available at: http://www.acgme.org.
- 14.Cain JM, Schulkin J, Parisi V, Power ML, Holzman GB, Williams S. Effects of perceptions and mentorship on pursuing a career in academic medicine in obstetrics and gynecology. Acad Med. 2001;76:628–34. doi: 10.1097/00001888-200106000-00015. [DOI] [PubMed] [Google Scholar]
- 15.Pololi LH, Civian JT, Brennan RT, Dottolo AL, Krupat E. Experiencing the culture of academic medicine: gender matters, a national study. J Gen Int Med. 2013;28:201–7. doi: 10.1007/s11606-012-2207-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Valantine HA, Grewal D, Ku MC, Moseley J, Shih M- C, Stevenson D, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89:904–911. doi: 10.1097/ACM.0000000000000245. [DOI] [PubMed] [Google Scholar]
- 17.Westring AF, Speck RM, Sammel MD, Scott P, Tuton LW, Grisso JA, et al. A culture conducive to women's academic success: development of a measure. Acad Med. 2012;87:1622–31. doi: 10.1097/ACM.0b013e31826dbfd1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bunton SA. Analysis in Brief. 7. Vol. 8. Association of American Medical Colleges; Washington, DC: 2008. Differences in U.S. medical school faculty job satisfaction by gender. [Google Scholar]
- 19.Westring AF, Speck RM, Sammel MD, Scott P, Conant EF, Tuton LW, et al. Culture matters: the pivotal role of culture for women's careers in academic medicine. Acad Med. 2014;89:658–63. doi: 10.1097/ACM.0000000000000173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.McGuire LK, Bergen MR, Polan ML. Career advancement for women faculty in a U.S. school of medicine: perceived needs. Acad Med. 2004;79:319–25. doi: 10.1097/00001888-200404000-00007. [DOI] [PubMed] [Google Scholar]
- 21.Travis EL, Doti L, Helitzer DL. Sponsorship: a path to the academic medicine C-suite for women faculty? Acad Med. 2013;88:1414–7. doi: 10.1097/ACM.0b013e3182a35456. [DOI] [PubMed] [Google Scholar]
- 22.Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88:1411–3. doi: 10.1097/ACM.0b013e3182a34952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.History, Art & Archives [July 24, 2014];U.S. House of Representatives, Office of the Historian. Women Representatives and Senators by Congress, 1917-Present. Available at: http://history.house.gov/Exhibitions-and-Publications/WIC/Historical-Data/Women-Representatives-and-Senators-by-Congress/.
- 24.Supreme Court of the United States [July 24, 2014];Members of the Supreme Court of the United States. Available at: http://www.supremecourt.gov/about/members.aspx.
- 25.Cook Bryan J., Kim Young. The American College President. American Council on Education; Washington, DC: 2012. 2012. [Google Scholar]