

Abstract
Non-Hodgkin lymphoma usually presents with generalized lymphadenopathy, but it can also involve any part of the human body. Lymphomatous involvement of muscles is a rare presentation and has been reported to occur in only 1.1% in non-Hodgkin lymphoma. Here we, present a 32 year-old Iranian man with primary involvement of spleen, bone, bone marrow and muscle, mimicking soft tissue sarcoma; core needle biopsy of the gluteal muscle showed diffuse large B cell lymphoma.
Keywords: Non-Hodgkin lymphoma, Diffuse large B-cell lymphoma, Extranodal lymphoma
INTRODUCTION
Extranodal manifestations of lymphomas are well recognized and occur in 20-30% of these patients. Involvement of the skeletal muscles by non-Hodgkin lymphoma (NHL) is unusual. The most commonly affected muscles are those of the extremities, pelvis, and gluteal regions,1 occurring as a result of metastatic hematogenous or lymphatic spread or contiguous spread from adjacent involved lymph nodes or bone.2 Primary skeletal muscle lymphoma is a rare disease accounting for only 0.5% of all extranodal lymphomas which mainly (>95%) consists of B-cell and non-Hodgkin type lymphomas (NHL).3
CASE REPORT
A 32-year-old man was admitted to the general ward of Imam Khomeini Hospital Complex on March 2013 with low back pain, anorexia, and significant weight-loss (15 kg) initiated about 8 months before his admission. Low back pain was constant with worsening effect during the night. The patient also reported fever, sweating, and numbness in the right lower part of his face 1 month before his admission. He gave no history of smoking, alcohol consumption or drug abuse.
On physical examination, the patient was feverish but appeared well. Conjunctiva was pale. There were no cervical masses or peripheral lymphadenopathy. Lungs and heart examinations were normal. Abdominal examination showed splenomegaly. There was no point tenderness on vertebrae or pelvic area. Muscle strength and deep tendon reflexes were symmetric and normal. Loss of sensation to light touch was present in the right lower part of the face. Laboratory findings are presented in Table 1.
Table 1.
Laboratory findings of the patient on admission
| Laboratory test | Patient’s value | Reference value |
|---|---|---|
| CBC | ||
| WBC | 2300/mm3 | 4000-10000/mm3 |
| Hemoglobin | 10.3 g/dL | 12-16 g/dL |
| MCV | 87.5 fL | 80-99 fL |
| Plt | 67000/mm3 | 150000-400000/mm3 |
| ESR | 3 mm/hr | < 20 mm/hr |
| CRP | 22.4mg/L | < 10 mg/L |
| LDH | 787 IU/L | 105-333IU/L |
| Serum Creatinine | 0.8 mg/dL | 0.7-1.3 mg/dL |
| Blood Urea Nitrogen | 19 mg/dl | 8-25 mg/dL |
| AST | 14 IU/L | 10-34 IU/L |
| ALT | 19 IU/L | 10-40 IU/L |
| AlkP | 186 IU/L | 44-147 IU/L |
| RF | 7.6 IU/mL | < 20 IU/mL |
| ANA | 1IU/ml | < 10IU/ml |
| HIV Ab | negative | - |
| HBs Ag | negative | - |
| HCV Ab | negative | - |
Abdominal ultrasound revealed normal parenchymal echo of the liver and there was no space occupying lesion. Spleen had normal parenchymal echo and its size was 167×65mm. Para aortic lymphadenopathy was not detected.
Abdominal Computerized Tomography (CT) scan demonstrated multiple hypodense lesions in the spleen (Fig.1). Diffuse enlargement of left paraspinal, iliopsoas and gluteal muscles were also reported (Fig.2). Thoracic CT scan showed one lymph node (12mm in size) in the posterior mediastinum.
Figure 1.

Abdominal Computerized Tomography showing multiple hypodense lesions in the spleen
Figure 2.
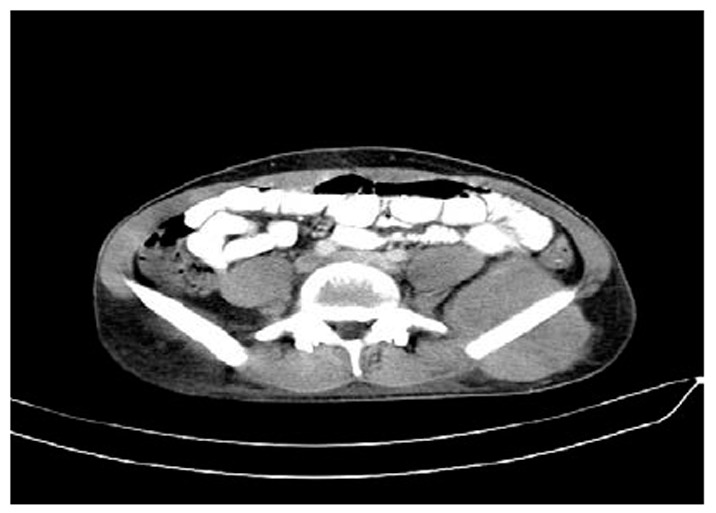
Pelvic Computerized Tomography showing diffuse enlargement of left Paraspinal,iliopsoas and gluteal muscles
Thoracic and lumbar Magnetic Resonance Imaging (MRI) revealed multiple signal intensity lesions in dorsal and lumbar vertebrae with heterogeneous enhancement after contrast injection. There was not any intervertebral disk involvement. There was also significant contrast enhancement in the left paraspinal muscles, mainly on the left iliopsoas and iliacus.
Brain MRI showed right trigeminal nerve (cranial nerve V) schwannomas that explained anesthesia of the right lower part of his face.
Whole body bone scintigraphy showed increased uptake in the spine, ribs, and left sacroiliac joints (Fig.3).
Figure 3.
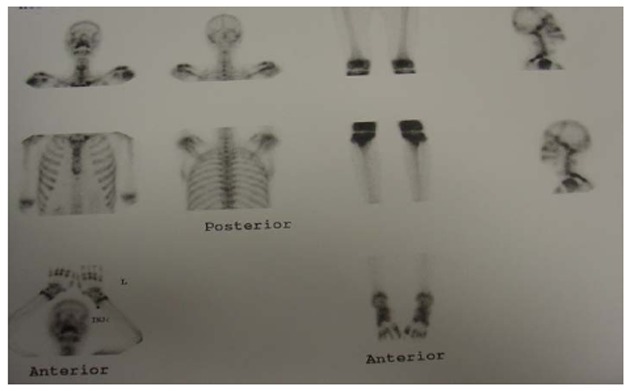
Whole body bone scintigraphy showingincreased uptake inspines and ribs
Bone marrow biopsy with immunohistochemical analysis was positive for leukocyte common antigen; CD20, Ki67 and CD3which were consistent with malignant diffuse large B-cell lymphoma.
CT-guided core needle biopsyof the gluteal muscle revealed malignant lymphoma, diffuse large B-cell with degrees of fibrosis. The large cells were positive for CD20. The small lymphoid cells were positive for CD3 and negative for CD15 or CD30. Proliferative activity was 45-50%.
DISCUSSION
Lymphoma comprises a histologically heterogeneous group of neoplasms derived from the cells of the immune system, representing approximately 5% of all cancers in the United States.4 The hallmark of the disease is the enlargement and proliferation of lymph nodes or secondary lymphoid tissues. NHL may arise from or may involve almost any organ of the human body. The term extranodal has been used to describe an uncommon form of lymphoid malignancy, in which there is neoplastic proliferation at sites other than the expected native lymph nodes or lymphoid tissues.5 A retrospective review of 3556 cases of NHL revealed that nearly one-third of all cases were extranodal in origin, giving an incidence of 1.9/105 new cases per year.6 The most common extranodal sites of involvement were stomach, spleen, Waldeyer ring, central nervous system, lungs, bones, and skin.5, 6
Lymphomatous involvement of muscles has been reported to occur in only 1.4%of cases, with 0.3% occurring in Hodgkin lymphoma and 1.1% in Non Hodgkin lymphoma.1 The most common route of muscle involvement is metastatic spread from adjacent lymph nodes or other primary sources such as bone.2, 7 Lymphoma spreads by infiltration of malignant cells that lack extracellular stroma and intercellular junctions, resulting in diffuse enlargement of involved structures and passing fascial boundaries. Thus, the involvement of more than one muscle compartment is typical. CT and MR images show diffuse enlargement in the involved organs. Attenuation on CT is similar or slightly decreased compared with uninvolved muscles; enhancement after IV contrast injection may be unapparent.7, 8
Primary skeletal muscle lymphoma is very rare, accounting for approximately 1.5% of NHLs. In a large retrospective study from the Mayo Clinic, Travis et al. reported primary muscle lymphoma in only 8 of 7000 cases of malignant lymphomas. Primary lymphoma of the muscle has been associated with a poor prognosis and usually has diffused large cell histologic feature.3
Our patient presented with involvement of spleen, bone, bone marrow and muscles without lymphadenopathy at any site. Soft tissue sarcoma and extranodal lymphoma were important differential diagnoses at presentation. For confirmatory diagnosis, core needle biopsy of gluteal muscle was performed. Biopsy showed diffuse large B-cell lymphoma. This case is a rare presentation of extranodal lymphoma with involvement of muscles. The muscle involvement was probably secondary to bone involvement. The patient was transferred to hematology-oncology ward where chemotherapy was started using R-CHOP protocol. A follow-up CT-scan and bone marrow biopsy showed complete regression of the lymphoma.
References
- 1.Chong June, Som Peter M, Silvers Adam R, Dalton Jack F. Extranodal Non-Hodgkin lymphoma involving the muscles of mastication. AJNR Am J Neuroradial. 1998;19:1849–1851. [PMC free article] [PubMed] [Google Scholar]
- 2.Suresh S, Saifuddin A, O’Donnell P. Lymphoma presenting as a musculoskeletal soft tissue mass. Eur Radiol. 2008;18:2628–2634. doi: 10.1007/s00330-008-1014-x. [DOI] [PubMed] [Google Scholar]
- 3.O’Neil JK, Devaraj V, Silver DAT, sarsfield P, Stone CA. Extranodal lymphoma presenting as soft tissue sarcoma. Journal of Plastic, Reconstructive Surgery. 2007;60:646–654. doi: 10.1016/j.bjps.2006.03.040. [DOI] [PubMed] [Google Scholar]
- 4.Newton R, Ferlay J, Beral V, et al. The epidemiology of non-Hodgkin’s lymphoma: comparison of nodal and extra-nodal sites. Int J Cancer. 1997;72:923–930. doi: 10.1002/(sici)1097-0215(19970917)72:6<923::aid-ijc1>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 5.Paes Fabio M, Kalknis Dimitrios G, Siders Panagiotis A, et al. FDG PET/CT ofextra nodal involvement in Non-Hodgkin Lymphoma and Hodgkin Disease. Radiogrphics. 2010;30:269–291. doi: 10.1148/rg.301095088. [DOI] [PubMed] [Google Scholar]
- 6.Gumey KA, Cartwright RA. Increasing incidence and descriptive epidemiology of extra nodal Non Hodgkin lymphoma in parts of England and Wales. Hematol J. 2002;3(2):95–104. doi: 10.1038/sj.thj.6200154. [DOI] [PubMed] [Google Scholar]
- 7.Chun ChangoWoo, Jee Won-Hee, Park Hye Jung, et al. MRI features of skeletal muscle lymphoma. AJR. 2010;195:1355–1360. doi: 10.2214/AJR.09.3904. [DOI] [PubMed] [Google Scholar]
- 8.Chew Felix S, Schellingerhout David, Keel Suzanne B. Primary lymphoma of skeletal muscle. AJR. 1999;172:1370. doi: 10.2214/ajr.172.5.10227519. [DOI] [PubMed] [Google Scholar]