

Abstract
AIM: In the present study, the characteristics of PEI-RFA treatment were further elucidated by analyzing the relationship between the volume of coagulated necrosis and the energy requirement for ablation or the amount of ethanol injected into HCC.
METHODS: The volume of coagulated necrosis, total energy requirement and energy requirement for coagulation of per unit volume were examined in the groups of PEI-RFA and RFA alone using the Cool-tip RF system.
RESULTS: The results showed that the volume of coagulated necrosis induced was significantly larger in PEI-RFA group than in routine RFA group, when the total energy administered was comparable in both groups. In PEI-RFA, enlargement of coagulated necrosis was admitted in 3 dimensions and the amount of energy requirement per unit volume of coagulated necrosis was negatively correlated with the amount of ethanol injected into HCC.
CONCLUSION: These results suggest that, compared to RFA alone, PEI-RFA enables to induce comparable coagulated necrosis with smaller energy requirement, and that PEI-RFA is likely to be less invasive than RFA alone irrespective of inducing enhanced coagulated necrosis. Thus, simple prior injection of ethanol may make RFA treatment more effective and less invasive for the treatment of patients with HCC.
Keywords: Combination therapy, Percutaneous ethanol injection, Radiofrequency ablation, Energy requirement
INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most serious problems worldwide. Although intensive efforts have been made for the treatment of HCC, the mortality of patients with HCC is still high. Tumor ablation technologies such as microwave, laser and radio frequency have been shown to be reliable and effective for inducing thermally-mediated coagulation necrosis for primary HCC[1-4] and metastatic liver cancer[5,6]. Percutaneous ethanol injection (PEI) therapy, more frequently performed in the past, is considered to be effective for the treatment of patients with relatively small-sized encapsulated HCC below 3 cm in the longest diameter. Recently, it has become possible to obtain larger areas of coagulated necrosis by the innovation of radiofrequency (RFA) technologies[7,8]. Much effort has been applied to enhance the therapeutic effects of RFA by the combination of RFA with other modalities. For example, combined use of transcatheter arterial chemoembolization[9-13] or saline injection[14-17] with RFA therapy was shown to be effective to enhance the coagulated necrosis. We also developed a novel combination therapy of PEI and RFA (PEI-RFA) and reported that this combination therapy could induce wider coagulated necrosis without much efforts and adverse effects. Furthermore, this therapy can be applied to the tumors that are difficult to treat with RFA alone[18,19]. Furthermore, this enhancing effect for inducing the coagulated necrosis has been experimentally confirmed using bovine liver[20]. Recently, we have reported that percutaneous ethanol and lipiodol injection therapy (PELIT), considered to be a milder therapy than RFA, was important as a supportive treatment modality for HCCs especially for those lacking the vascularity or for patients with severely impaired hepatic reserve and useful for the treatment of HCCs that were difficult to treat with RFA alone[21]. After developing PEI-RFA treatment, we have experienced so far some cases that were satisfactorily treated by use of relatively low-power output control. Thus, in the present study, PEI-RFA treatment was further characterized from the standpoint of the energy requirement for total and unit volume ablation as well as of the amount of ethanol injected, using the RF system with cool-tip type electrodes.
MATERIALS AND METHODS
Patients
PEI-RFA was performed against 75 cases (53 males and 22 females; mean age of 69 years) with biopsy-proven HCC. The patients were also diagnosed as having HCC by helical dynamic computed tomography (CT). Among the total subjects, RFA alone was done in 15 patients and PEI-RFA was in 60. The characteristics of the subjects are shown in Table 1. All of these studies were conducted with informed consent at the time of the enrollment for this study.
Table 1.
Characteristics of patients enrolled in the present study.
| RFA alone | PEI-RFA | |
| Total number of patient | 15 | 60 |
| Male/Female | 10/5 | 45/15 |
| Age (yr) | ||
| Mean | 63 | 69 |
| Range | 47-74 | 44-86 |
| Tumor size (cm) | ||
| Mean | 2.5 | 3 |
| Range | 1.5-3.5 | 1.0- 8.0 |
| Injected ethanol (mL) | ||
| Mean | 0 | 7.1 |
| Range | 0-0 | 0-37 |
| Child-Pugh grade | ||
| A | 7 | 38 |
| B | 7 | 21 |
| C | 1 | 1 |
Equipments and RFA procedures
PEI-RFA was performed under the real-time ultrasonography (US) guidance with a 3.5-MHz sector probe (Power Vision 5000; Toshiba Medical, Tokyo, Japan). RFA was performed by Cool-tip RF System (RADIONICS, Burlington, USA)[22] according to the method described in our previous manuscripts[18,19]. Briefly, a 17-gauge RFA needle with an electrode of 3 cm in length was first inserted into the tumor, and then a 21-gauge PEI needle was inserted into the tumor in the liver through the same hole of the attachment beside the echo probe, and then pure ethanol was slowly injected into the tumor till the whole area of tumor was filled with the ethanol (Figure 1). Ethanol injection into the tumor was ceased when resistance to the injection was felt. The volume of injected ethanol was always kept below the double of estimated tumor volume. The ablation was performed under the impedance control and the power output was increased stepwise and the ablation was terminated after the high echoic shadow sufficiently covered the tumor margin.
Figure 1.
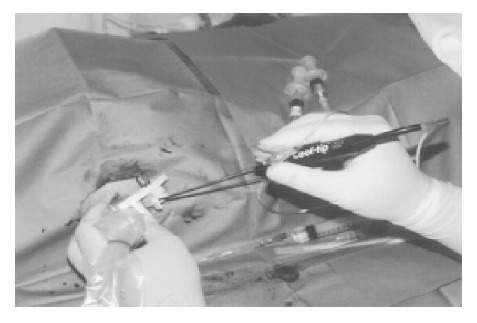
Appearance of PEI-RFA treatment. A 17-gauge RFA needle with 2 or 3 cm electrode was first inserted into the tumor through the hole of the attachment beside the echo probe, and then 21-gauge PEI needle was inserted through the same hole. RFA was performed immediately after injecting the ethanol into the tumor. The ablation was performed under the impedance control. The amount of ethanol injected into the tumors was always kept below the double of the estimated tumor volume and the injection of ethanol was ceased if resistance to the injection was felt.
Evaluation of therapeutic efficacy
The efficacy of the RFA was assessed by using helical dynamic contrast-enhanced CT five to seven days after the treatment. Tumor necrosis was considered to be complete if no enhancing areas were observed based on images obtained during early and late phases of dynamic contrast-enhanced CT.
Evaluation of energy requirement for ablation
Energy requirement needed for ablation was calculated as follows: energy (J) = Watt (W) × duration of ablation (s). The length of coagulated necrosis of the lesion was measured from the late phase of helical dynamic CT. Approximation volume of whole coagulated necrosis area and energy requirement for ablation per unit volume were calculated as follows: whole coagulated volume (cm3) = 4/3 × r1(cm) × r2(cm) × r3(cm); (r1 = longest diameter/2; r2 = shortest diameter/2; r3 = height/2) and energy requirement for coagulation per unit volume (J/cm3 ) = energy/whole coagulated necrosis.
Statistical analysis
Statistical analysis was performed using Macintosh software StatView II (Version 5.0). Regression analysis was used to calculate the correlation coefficients and P values. Statistical significance was accepted when P<0.05.
RESULTS
Comparison of the volume of coagulated area, and energy requirement and the energy requirement for total and unit volume coagulation in the groups of PEI-RFA and RFA alone
Seventy-five patients were divided randomly into two groups. One group (60 patients) received PEI-RFA, while the other (15 patients) RFA alone. All of these patients underwent RFA therapy by means of the Cool-tip RF system. No major complications or adverse effects were observed in both groups. The volume of coagulated necrosis areas, the total amount of energy requirement and the energy requirement for inducing coagulation of per unit volume in the groups of PEI-RFA and RFA alone are shown in Table 2. The longest and shortest diameters as well as the height of the coagulated necrosis areas and the coagulated volume evaluated by dynamic contrast-enhanced CT scan were significantly larger in cases treated with PEI-RFA than in those treated with RFA alone. By contrast, the total amount of energy requirement was comparable between groups. Thus, the energy requirement for coagulation of per unit volume was significantly smaller in PEI-RFA group compared to the group of RFA alone. The energy requirement for coagulation of per unit volume in PEI-RFA was approximately three-fourths of that in RFA alone.
Table 2.
Comparison of the volume of coagulated necrosis, total energy requirement and the energy requirement for inducing coagulation of per unit volume in the groups of PEI-RFA and RFA alone.
| EtOH (mL) | L (cm) | S (cm) | H (cm) | V (cm3) | T-ENE (J) | T-ENE/V (J/cm3) | |
| RFA alone (n = 15) | 0±0 | 2.3±0.6 | 2.1±0.6 | 2.4±0.4 | 6.5±3.6 | 38700±12549 | 10010±11124 |
| PEI-RFA (n = 60) | 6.9±6.6 | 4.2±1.2 | 3.5±1.0 | 4.0±1.1 | 34.0±29.3 | 53828±28144 | 2355±1690 |
| P | <0.0001 | <0.0001 | <0.0001 | 0.0002 | <0.0001 | 0.73 | <0.0001 |
Sixty patients with HCC were treated with PEI-RFA by Cool-tip RF System, while 15 patients were treated with RFA alone using the same system. After the treatment, the longest and shortest diameters and the height of the coagulated necrosis were estimated by the contrast-enhanced CT scan. Each abbreviation in the table is expressing as follows: EtOH, the amount of ethanol; L, longest diameter; S, shortest diameter; H, height; V, the volume of coagulated necrosis; T-ENE, total energy requirement; T-ENE/V, the energy requirement for inducing coagulation of per unit volume. The coagulated necrosis in PEI-RFA group was enlarged in 3 dimensions compared with the group of RFA alone, although the total energy requirement was comparable between groups.
Comparative study of the coagulated necrosis and the energy requirement for coagulation of per unit volume between PEI-RFA and RFA groups
As shown in Table 3, the mean volume of ethanol injected in PEI-RFA group was 6.9 mL. Therefore, 60 patients treated with PEI-RFA were divided into two groups according to the amount of ethanol injected. One group (high-EtOH group) consisted of 19 cases administered with 6.9 mL and more ethanol and the other (low-EtOH group) of 41 cases less than 6.9 mL ethanol. Between these two groups, the total energy requirement was also comparable as shown in Table 1. However, the volume of coagulated necrosis was significantly larger in the high-EtOH group than in the low-EtOH group. The volume of coagulated necrosis in the high-EtOH group was 2.6 times larger than that in the low-EtOH group. Accordingly, the energy requirement for coagulation per unit volume in the high-EtOH group was significantly lower in the high-EtOH group than in the low-EtOH group.
Table 3.
Comparative study of coagulated necrosis in the groups classified according to the amount of ethanol injected in PEI-RFA.
| EtOH (mL) | L (cm) | S (cm) | H (cm) | V (cm3) | T-ENE (J) | T-ENE/V (J/cm3) | |
| EtOH <6.9 mL | 3.1±1.6 | 3.8±0.9 | 3.0±0.6 | 3.6±0.9 | 22.3±14.3 | 48 901±23219 | 2796±1752 |
| (n = 41) | -1 | ||||||
| EtOH >6.9 mL | 14.9±6.1 | 5.1±1.3 | 4.3±1.2 | 4.8±1.1 | 57.6±38.2 | 63 931±34744 | 1460±1016 |
| (n = 19) | -2.6 | ||||||
| P | <0.0001 | 0.0002 | <0.0001 | 0.0003 | <0.0001 | 0.11 | 0.0014 |
The mean volume of ethanol injected in PEI-RFA was 6.9 mL. Therefore, 60 patients treated with PEI-RFA were divided into two groups according to the amount of ethanol injected. One group (high EtOH group) consisted of 19 cases administered with 6.9 mL and more ethanol, and the other (low EtOH group) of 41 cases less than 6.9 mLethanol. Each abbreviation in the table is expressing as follows: EtOH, the amount of ethanol; L, longest diameter; S, shortest diameter; H, height; V, the volume of coagulated necrosis; T-ENE, total energy requirement; T-ENE/V, the energy requirement for inducing coagulation of per unit volume. The volume of coagulated necrosis in the high EtOH group was 2.6 times larger than that in the low EtOH group, although the total energy requirement was comparable between groups.
All cases treated with PEI-RFA were divided into two groups. One was high-energy group and the other low-energy group according to the mean amount of total energy requirement (53828 J). As shown in Table 4, in this classification, the amount of ethanol injected was statistically comparable in both groups. The volume of coagulated necrosis in the high-energy group was 1.8 times larger than that in the low-energy group. The degree of the enhancing effect was smaller compared to that in cases classified by the mean amount of ethanol injected as shown in Table 2. Furthermore, the energy requirement for coagulation of per unit volume was comparable between groups.
Table 4.
Comparative study of coagulated necrosis in the groups classified according to the total energy requirement in PEI-RFA.
| EtOH (mL) | L (cm) | S (cm) | H (cm) | V (cm3) | T-ENE (J) | T-ENE/V(J/cm3) | |
| T-ENE <53828J | 5.8±5.8 | 3.6±0.8 | 3.2±0.8 | 3.6±1.0 | 24.6±17.3 | 32003±12743 | 2038±1638 |
| (n = 32) | -1 | ||||||
| T-ENE >53828 J | 8.1±7.3 | 4.8±1.2 | 3.8±1.2 | 4.4±1.2 | 44.0±36.4 | 77884±19567 | 2727±1687 |
| (n = 28) | -1.8 | ||||||
| P | 0.23 | 0.0002 | 0.04 | 0.0028 | 0.014 | <0.0001 | 0.052 |
All cases treated with PEI-RFA were divided into two groups. One was high energy group and the other low energy group according to the mean amount of total energy requirement (53828 Joule). Each abbreviation in the table is expressing as follows: EtOH, the amount of ethanol; L, longest diameter; S, shortest diameter; H, height; V, the volume of coagulated necrosis; T-ENE, total energy requirement; T-ENE/V, the energy requirement for inducing coagulation of per unit volume. The amount of ethanol injected was statistically comparable in both groups. The volume of coagulated necrosis in the high energy group was 1.8 times larger than that in the low energy group. The degree of the enhancing effect was smaller compared with that in cases classified by the mean amount of injected ethanol as shown in Table 3. Furthermore, the energy requirement for coagulation of per unit volume was comparable between groups.
Relationship between the amount of ethanol and the volume of coagulated necrosis or the energy requirement for coagulation of per unit volume
Relationship between the amount of ethanol injected and the volume of coagulated necrosis or the energy requirement for coagulation of per unit volume was analyzed in the total subjects treated with PEI-RFA (60 cases). As shown in Figure 2, the amount of ethanol injected into tumor significantly and positively correlated with the volume of coagulated necrosis with high correlation coefficient (r = 0.71, P<0.0001). Then, the amount of ethanol injected negatively, although weak, correlated with the energy requirement for coagulation of per unit volume (r = -0.41, P = 0.014). These results suggest that, according to the amount of ethanol injected into tumor, larger coagulated necrosis can be obtained and less amount of energy is required for coagulation of per unit volume.
Figure 2.
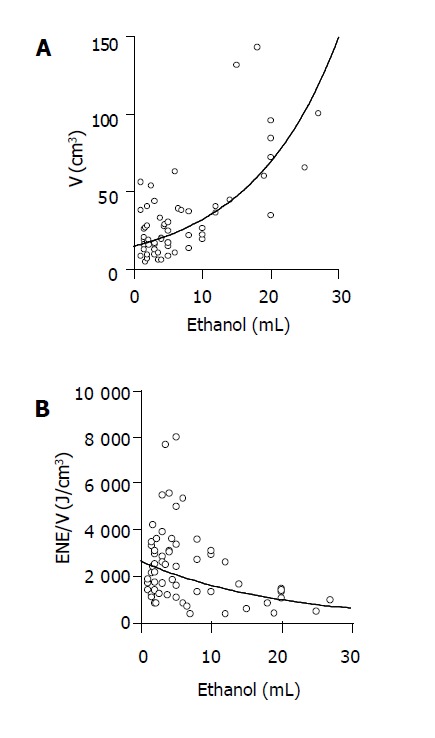
Relationship between the amount of ethanol injected and the volume of coagulated necrosis or the energy requirement for inducing per unit volume of coagulated necrosis in PEI-RFA. PEI-RFA was performed on 60 patients with HCC. The ablation was done by using the Cool-tip RF system. The amount of ethanol injected into tumors positively correlated with the volume of coagulated necrosis (A: r = 0.71, P<0.0001) and it negatively correlated with the energy requirement for inducing per unit volume of coagulated necrosis (B: r = -0.41, 0.014).
Relationship between the total required energy for ablation and the volume of coagulated necrosis or the energy requirement for coagulation of per unit volume
Relationship between the total required energy and the volume of the coagulated necrosis or the energy requirement for coagulation of per unit volume was analyzed in the total subjects treated with PEI-RFA (60 cases). As shown in Figure 3, the total required energy significantly and positively correlated with the volume of coagulated necrosis (r = 0.47, P = 0.0013). However, this correlation coefficient was smaller than that between the amount of ethanol injected and the volume of coagulated necrosis. Moreover, the total required energy and the energy requirement for coagulation of per unit volume did not show significant correlation (r = 0.35, P = 0.13).
Figure 3.
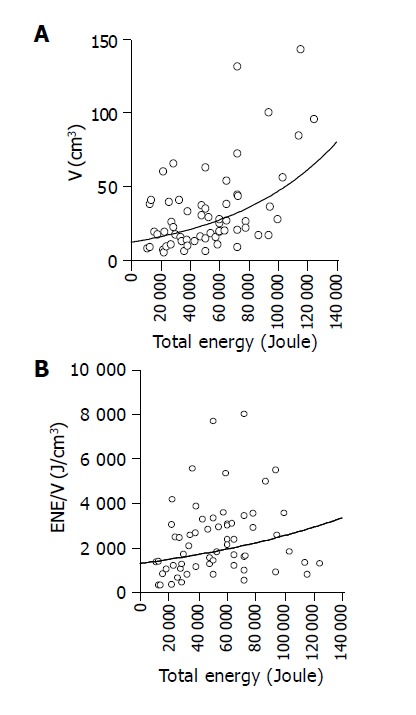
Relationship between the amount of total energy requirement and the volume of coagulated necrosis or the energy requirement for inducing per unit volume of coagulated necrosis in PEI-RFA. PEI-RFA was performed on 60 patients with HCC. The ablation was done by using the Cool-tip RF system. The amount of total energy requirement positively correlated with the volume of coagulated necrosis (r = 0.47, P = 0.0013), whereas no significant correlation was admitted between the total amount of energy requirement and the energy requirement for inducing per unit volume of coagulated necrosis (r = 0.35, P = 0.13) in PEI-RFA.
Representative cases with HCC treated with PEI-RFA
By analyzing the relationship between the energy requirement and the amount of ethanol injected in PEI-RFA, two characteristic points have been turned out: (1) PEI-RFA enables to induce wider coagulated necrosis by increasing the amount of ethanol injected into tumor; (2) PEI-RFA is able to obtain comparative therapeutic effects by means of lower energy compared to RFA alone.
Four cases with HCC treated with PEI-RFA expressing these characteristic points are shown in Figures 4, 5. The large-sized HCCs (5 cm in diameter) of the first and second cases were located in S7 (Figure 4A) and S1 regions (Figure 4C) respectively. In the first case, RFA was performed at 30-100 W for 10 min after injecting 10 mL of ethanol homogeneously into the tumor. The RFA electrode was reinserted into the tumor and the RFA was performed for further 10 min. Contrast-enhanced CT after the treatment showed the achievement of coagulated necrosis of 8 cm in diameter and the ablated region covered the entire region of the tumor including the safety margin (Figure 4B). In the second case, contrast-enhanced CT showed the enhancement in the early vascular phase of dynamic CT (Figure 4C). It was likely to be difficult to treat with RFA under high power output, because the tumor was surrounded by inferior vena cava, portal tract and aorta. Therefore, PEI-RFA under a relatively low power output after injecting high amount of ethanol was chosen as a treatment modality. After injecting 19 mL of ethanol into the tumor, one session of RFA was performed at 30 W for 12 min. Contrast-enhanced CT after the treatment showed that the ablated region reached the most of the entire region of the tumor in this case as well (Figure 4D).
Figure 4.
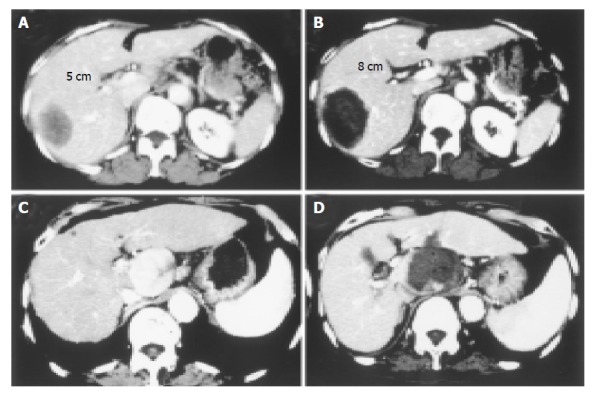
Two cases with large-sized HCC treated with PEI-RFA are shown. Contrast-enhanced CT before (A: delay phase, C: early vascular phase) and after (B: delay phase, D: delay phase) PEI-RFA. Massive HCCs of 5 cm in the longest diameter were located in the right lobe of the liver in both cases. In the first case (A and B), RFA was started at 30 W and the power output was increased stepwise to 100 W every two min and the ablation was performed for 20 min. In the second case (C and D), because the tumor was located close by blood vessel such as inferior vena cava, portal tract and aorta, it was likely to be difficult to treat with RFA under high power control. After injecting 19 mL of ethanol into the tumor, one session of RFA was performed at 30 W for 12 min. The massive tumor was completely eliminated by PEI-RFA.
Figure 5.
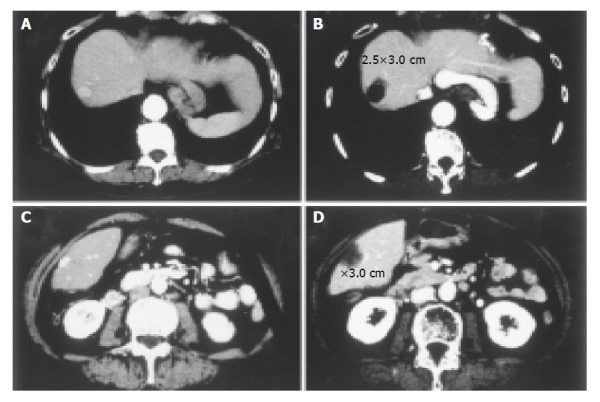
Two cases with small-sized HCCs treated with PEI-RFA under low power output control are shown. Contrast-enhanced CT before (A, C) and after (B, D) PEI-RFA. Small HCCs of 1.5 cm in the longest diameter were located in the S8 region of the liver in both cases. In both cases, RFA was performed at 40 W for 5 min. Though the ablation was performed at relatively low power output for short duration, the coagulated necrosis larger than 2.5 cm was induced after the treatment.
The HCCs of the third and fourth cases are located in S8 (Figure 5A) and S6 (Figure 5C) respectively and the size of both HCCs was 1.5 cm in diameter. To obtain over 0.5 cm of the safety margin area from the edge of the tumor, the coagulated necrosis wider than 2.5 cm in diameter was required for the ablation. In both cases, after injecting 2 mL of ethanol into the tumors, RFA was performed at 40 W for 5 min. Although RFA was performed under a relatively low power output and for a short time period, dynamic CT after PEI-RFA in both cases indicated the induction of coagulated necrosis larger than 2.5 cm in diameter (Figure 5B, D). In the third case, the energy requirement for coagulation of per unit volume was an extremely low level of 1244 (J/cm3), a half-value of the mean in PEI-RFA group as shown in the Table 2.
DISCUSSION
RFA is a promising technique for local control of liver malignancy such as primary hepatocellular carcinoma[4,23,24] and metastatic liver cancers[25]. This technique has become the main stream of the treatment of non-surgical treatment modalities in clinical settings[3]. In contrast to its efficacy, the region of coagulated necrosis induced by RFA is still limited and tumors within 3 cm in diameter are thought to be the good application sites of RFA therapy. Underestimated complication was sometimes observed after RFA treatment. To enhance the therapeutic effect of RFA, several treatment modalities have been applied as additional treatments on local treatment. It has been reported that combined use of transcatheter arterial chemoembolization or saline injection therapy with RFA enhanced the extent of induced coagulation[11-14,17,26,27]. Recently, Pawlik et al have reported that resection combined with RFA provides a surgical option to a group of patients with unresectable liver metastases[28]. As one of the optional combination therapies, we have shown that the injection of ethanol prior to RFA markedly increased the induced coagulated necrosis in human[18,19] and bovine livers[20]. In the present study, we further evaluated the usefulness of PEI-RFA using the system equipped with a cool-tip type electrode, instead of the system with an expandable type electrode. Especially, the characteristics of PEI-RFA were assessed from the standpoint of energy requirement for inducing the coagulated necrosis and the amount of ethanol injected. In our previous manuscript, we have shown that the longest and the shortest diameters as well as the height of the coagulated necrosis areas, and the coagulated volume evaluated by dynamic contrast-enhanced CT scan were significantly larger in cases treated with PEI-RFA than in those treated with RFA alone using the system equipped with an expandable type of electrode (RITA-500PA)[18]. Similar enhancing effects of ethanol injection were observed in the present study using the Cool-tip RF system. The volume of coagulated necrosis in PEI-RFA was approximately four times larger than that in RFA alone in the Cool-tip RF system. This degree of enhancement of coagulated necrosis area was quite similar to that detected in the system with the expandable type of electrode in our previous manuscript[18]. These results suggest that injection of ethanol prior to RFA therapy may equally enhance the volume of coagulated necrosis in 3 dimensions to the same extent regardless of types of RFA instruments.
More importantly and interestingly, it should be noted that the volume and diameters of coagulated necrosis were significantly larger in PEI-RFA than in RFA alone, although the amount of total energy requirement was comparable between groups. Thus, the energy requirement for coagulation of per unit volume was significantly lower in PEI-RFA than in RFA alone. The degree of enhancement of coagulated necrosis was higher between the groups classified according to the amount of injected ethanol than between those classified according to the amount of total energy requirement. The former was 2.6-times enhancement and the latter was 1.8 times. Furthermore, the volume of coagulated necrosis showed a stronger correlation with the amount of ethanol injected than the total energy requirement (r = 0.71 vs 0.47) respectively. While the amount of injected ethanol, negatively correlated with the energy requirement for coagulation of per unit volume, the total required energy did not show negative correlation with the energy requirement for coagulation of per unit volume. Taken together, these results clearly indicate that smaller energy is required in PEI-RFA to induce comparable coagulated necrosis to RFA alone, and the use of ethanol injection prior to RFA is likely to alter the RFA therapy to a milder one for the treatment of patients with HCC. These results may be one of the explanations that PEI-RFA is able to induce wider coagulated necrosis compared to RFA alone under the same power output condition.
Although it is possible to say that RFA is less invasive compared to surgical treatment, we have experienced some patients whose liver function tests declined after RFA treatment. Furthermore, RFA treatment has sometimes been obliged to be ceased due to the pain complained by patients during the treatment[29]. Therefore, it is very important to develop less invasive treatments than those currently used. It is needless to say that less invasive and more effective treatment is desirable for local control of HCC in patients treated with RFA.
When thinking of the medical treatment, it should be important to take both efficacy and the adverse reactions into consideration. In this regard, PEI-RFA is thought to be a less invasive and more effective treatment modality for local control of hepatic malignancies than RFA alone. PEI-RFA is expected to contribute to the local treatment of patients with hepatic malignancy from the standpoint of not only the effectiveness but also the reduction of adverse events.
Footnotes
Edited by Guo SY Language Editor Elsevier HK
References
- 1.Nagata Y, Hiraoka M, Akuta K, Abe M, Takahashi M, Jo S, Nishimura Y, Masunaga S, Fukuda M, Imura H. Radiofrequency thermotherapy for malignant liver tumors. Cancer. 1990;65:1730–1736. doi: 10.1002/1097-0142(19900415)65:8<1730::aid-cncr2820650812>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 2.Allgaier HP, Deibert P, Zuber I, Olschewski M, Blum HE. Percutaneous radiofrequency interstitial thermal ablation of small hepatocellular carcinoma. Lancet. 1999;353:1676–1677. doi: 10.1016/S0140-6736(99)00368-2. [DOI] [PubMed] [Google Scholar]
- 3.Goldberg SN, Gazelle GS, Solbiati L, Livraghi T, Tanabe KK, Hahn PF, Mueller PR. Ablation of liver tumors using percutaneous RF therapy. AJR Am J Roentgenol. 1998;170:1023–1028. doi: 10.2214/ajr.170.4.9530053. [DOI] [PubMed] [Google Scholar]
- 4.Curley SA, Izzo F, Ellis LM, Nicolas Vauthey J, Vallone P. Radiofrequency ablation of hepatocellular cancer in 110 patients with cirrhosis. Ann Surg. 2000;232:381–391. doi: 10.1097/00000658-200009000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Solbiati L, Goldberg SN, Ierace T, Livraghi T, Meloni F, Dellanoce M, Sironi S, Gazelle GS. Hepatic metastases: percutaneous radio-frequency ablation with cooled-tip electrodes. Radiology. 1997;205:367–373. doi: 10.1148/radiology.205.2.9356616. [DOI] [PubMed] [Google Scholar]
- 6.Solbiati L, Ierace T, Goldberg SN, Sironi S, Livraghi T, Fiocca R, Servadio G, Rizzatto G, Mueller PR, Del Maschio A, et al. Percutaneous US-guided radio-frequency tissue ablation of liver metastases: treatment and follow-up in 16 patients. Radiology. 1997;202:195–203. doi: 10.1148/radiology.202.1.8988211. [DOI] [PubMed] [Google Scholar]
- 7.Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Solbiati L, Gazelle GS. Small hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injection. Radiology. 1999;210:655–661. doi: 10.1148/radiology.210.3.r99fe40655. [DOI] [PubMed] [Google Scholar]
- 8.Goldberg SN, Gazelle GS, Compton CC, Mueller PR, Tanabe KK. Treatment of intrahepatic malignancy with radiofrequency ablation: radiologic-pathologic correlation. Cancer. 2000;88:2452–2463. [PubMed] [Google Scholar]
- 9.Rossi S, Garbagnati F, Lencioni R, Allgaier HP, Marchianò A, Fornari F, Quaretti P, Tolla GD, Ambrosi C, Mazzaferro V, et al. Percutaneous radio-frequency thermal ablation of nonresectable hepatocellular carcinoma after occlusion of tumor blood supply. Radiology. 2000;217:119–126. doi: 10.1148/radiology.217.1.r00se02119. [DOI] [PubMed] [Google Scholar]
- 10.Buscarini L, Buscarini E, Di Stasi M, Quaretti P, Zangrandi A. Percutaneous radiofrequency thermal ablation combined with transcatheter arterial embolization in the treatment of large hepatocellular carcinoma. Ultraschall Med. 1999;20:47–53. doi: 10.1055/s-1999-14233. [DOI] [PubMed] [Google Scholar]
- 11.Yamasaki T, Kurokawa F, Shirahashi H, Kusano N, Hironaka K, Okita K. Percutaneous radiofrequency ablation therapy with combined angiography and computed tomography assistance for patients with hepatocellular carcinoma. Cancer. 2001;91:1342–1348. doi: 10.1002/1097-0142(20010401)91:7<1342::aid-cncr1137>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 12.Koda M, Murawaki Y, Mitsuda A, Oyama K, Okamoto K, Idobe Y, Suou T, Kawasaki H. Combination therapy with transcatheter arterial chemoembolization and percutaneous ethanol injection compared with percutaneous ethanol injection alone for patients with small hepatocellular carcinoma: a randomized control study. Cancer. 2001;92:1516–1524. doi: 10.1002/1097-0142(20010915)92:6<1516::aid-cncr1477>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- 13.Kitamoto M, Imagawa M, Yamada H, Watanabe C, Sumioka M, Satoh O, Shimamoto M, Kodama M, Kimura S, Kishimoto K, et al. Radiofrequency ablation in the treatment of small hepatocellular carcinomas: comparison of the radiofrequency effect with and without chemoembolization. AJR Am J Roentgenol. 2003;181:997–1003. doi: 10.2214/ajr.181.4.1810997. [DOI] [PubMed] [Google Scholar]
- 14.Livraghi T, Goldberg SN, Monti F, Bizzini A, Lazzaroni S, Meloni F, Pellicanò S, Solbiati L, Gazelle GS. Saline-enhanced radio-frequency tissue ablation in the treatment of liver metastases. Radiology. 1997;202:205–210. doi: 10.1148/radiology.202.1.8988212. [DOI] [PubMed] [Google Scholar]
- 15.Honda N, Guo Q, Uchida H, Ohishi H, Hiasa Y. Percutaneous hot saline injection therapy for hepatic tumors: an alternative to percutaneous ethanol injection therapy. Radiology. 1994;190:53–57. doi: 10.1148/radiology.190.1.8259428. [DOI] [PubMed] [Google Scholar]
- 16.Burdío F, Güemes A, Burdío JM, Navarro A, Sousa R, Castiella T, Cruz I, Burzaco O, Guirao X, Lozano R. Large hepatic ablation with bipolar saline-enhanced radiofrequency: an experimental study in in vivo porcine liver with a novel approach. J Surg Res. 2003;110:193–201. doi: 10.1016/s0022-4804(02)00091-4. [DOI] [PubMed] [Google Scholar]
- 17.Hänsler J, Frieser M, Schaber S, Kutschall C, Bernatik T, Müller W, Becker D, Hahn EG, Strobel D. Radiofrequency ablation of hepatocellular carcinoma with a saline solution perfusion device: a pilot study. J Vasc Interv Radiol. 2003;14:575–580. doi: 10.1097/01.rvi.0000071096.76348.3b. [DOI] [PubMed] [Google Scholar]
- 18.Kurokohchi K, Watanabe S, Masaki T, Hosomi N, Funaki T, Arima K, Yoshida S, Miyauchi Y, Kuriyama S. Combined use of percutaneous ethanol injection and radiofrequency ablation for the effective treatment of hepatocelluar carcinoma. Int J Oncol. 2002;21:841–846. doi: 10.3892/ijo.21.4.841. [DOI] [PubMed] [Google Scholar]
- 19.Kurokohchi K, Watanabe S, Masaki T, Hosomi N, Funaki T, Arima K, Yoshida S, Nakai S, Murota M, Miyauchi Y, et al. Combination therapy of percutaneous ethanol injection and radiofrequency ablation against hepatocellular carcinomas difficult to treat. Int J Oncol. 2002;21:611–615. [PubMed] [Google Scholar]
- 20.Watanabe S, Kurokohchi K, Masaki T, Miyauchi Y, Funaki T, Inoue H, Himoto T, Kita Y, Uchida N, Touge T, et al. Enlargement of thermal ablation zone by the combination of ethanol injection and radiofrequency ablation in excised bovine liver. Int J Oncol. 2004;24:279–284. [PubMed] [Google Scholar]
- 21.Kurokohchi K, Masaki T, Miyauchi Y, Funaki T, Yoneyama H, Miyoshi H, Yoshida S, Himoto T, Morishita A, Uchida N, et al. Percutaneous ethanol and lipiodol injection therapy for hepatocellular carcinoma. Int J Oncol. 2004;24:381–387. [PubMed] [Google Scholar]
- 22.Francica G, Marone G. Ultrasound-guided percutaneous treatment of hepatocellular carcinoma by radiofrequency hyperthermia with a 'cooled-tip needle'. A preliminary clinical experience. Eur J Ultrasound. 1999;9:145–153. doi: 10.1016/s0929-8266(99)00022-1. [DOI] [PubMed] [Google Scholar]
- 23.Goldberg SN, Gazelle GS, Compton CC, Mueller PR, Tanabe KK. Treatment of intrahepatic malignancy with radiofrequency ablation: radiologic-pathologic correlation. Cancer. 2000;88:2452–2463. [PubMed] [Google Scholar]
- 24.Jiang HC, Liu LX, Piao DX, Xu J, Zheng M, Zhu AL, Qi SY, Zhang WH, Wu LF. Clinical short-term results of radiofrequency ablation in liver cancers. World J Gastroenterol. 2002;8:624–630. doi: 10.3748/wjg.v8.i4.624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Curley SA, Izzo F, Delrio P, Ellis LM, Granchi J, Vallone P, Fiore F, Pignata S, Daniele B, Cremona F. Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg. 1999;230:1–8. doi: 10.1097/00000658-199907000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yasuda S, Ito H, Yoshikawa M, Shinozaki M, Goto N, Fujimoto H, Nasu K, Uno T, Itami J, Isobe K, et al. Radiotherapy for large hepatocellular carcinoma combined with transcatheter arterial embolization and percutaneous ethanol injection therapy. Int J Oncol. 1999;15:467–473. [PubMed] [Google Scholar]
- 27.Okano H, Shiraki K, Inoue H, Ito T, Yamanaka T, Deguchi M, Sugimoto K, Sakai T, Ohmori S, Murata K, et al. Combining transcatheter arterial chemoembolization with percutaneous ethanol injection therapy for small size hepatocellular carcinoma. Int J Oncol. 2001;19:909–912. doi: 10.3892/ijo.19.5.909. [DOI] [PubMed] [Google Scholar]
- 28.Pawlik TM, Izzo F, Cohen DS, Morris JS, Curley SA. Combined resection and radiofrequency ablation for advanced hepatic malignancies: results in 172 patients. Ann Surg Oncol. 2003;10:1059–1069. doi: 10.1245/ASO.2003.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Curley SA, Marra P, Beaty K, Ellis LM, Vauthey JN, Abdalla EK, Scaife C, Raut C, Wolff R, Choi H, et al. Early and late complications after radiofrequency ablation of malignant liver tumors in 608 patients. Ann Surg. 2004;239:450–458. doi: 10.1097/01.sla.0000118373.31781.f2. [DOI] [PMC free article] [PubMed] [Google Scholar]